Soft Tissue Techniques, Taping, BFR, and Dry Needling
1/66
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
67 Terms
Soft Tissue Mobilization
A systematic manipulation of soft tissues of the body by hands or an instrument with rhythmical pressure and stroking to prevent, develop, maintain, rehabilitate, or augment physical function or relieve pain (Dryden, 2004)
A therapeutic tool used to relieve pain
What is the function of Soft Tissue Mobilization
Effleurage soft tissue mobilization
Gliding or sliding movement over the skin
Petrissage soft tissue mobilization
Lifting, wringing, or squeezing of soft tissues in a kneading motion, or pressing or rolling of tissue
Friction soft tissue mobilization
Penetrating pressure applied through the fingertips
Tapotement soft tissue mobilization
Strike the tissues at a rapid rate
Vibration soft tissue mobilization
Rhythmic oscillation applied to tissue
- Increased neural activity at spinal cord level and subcortical nuclei, which may affect mood and pain perception
- Reduce motor neuron activity at site administered
- Shift physiological response from sympathetic to parasympathetic responses
- Stimulate connective tissue remodeling through resorption of fibrosis, regeneration of collagen secondary to fibroblast recruitment
- Improvement of blood flow (lactate) / lymph flow to tissues
- Building upon framework of therapeutic alliance and patient belief systems
Purported Mechanisms for STM (Soft Tissue Mobilization)
- Reduce pain
- Increase tissue extensibility
- Improve circulation
- Improve overall well-being
- Improve therapeutic alliance / patient expectations
- Complement adjunct techniques
What are indications for the use of STM
- relax muscles
- move body fluids
- promote wellness
What is the intention of relaxation massage
- accomplish specific goals such as releasing muscle spasms
- focus on muscle of fascia
- relieve pain and restricted motion
What is the intention of clinical massage
- induce sense of freedom
- ease and lightness in body
- use movement to enhance posture, body awareness and movement/function
What is the intention of movement re-education
- Swedish massage
- Spa massage
- sport massage
Examples of relaxation massage
- myofascial trigger point therapy
- myofascial release
- strain - counter strain
Examples of clinical massage
- direct pressure
- skin rolling
- resistive stretching
- passive stretching
- cross-fiber friction
What are techniques used in clinical massage
- proprioceptive neuromuscular facilitation
- strain - counter strain
- Trager
Examples of movement re-education
- contract relax
- passive stretching
- resistive stretching
- rocking
What are techniques used in movement re-education
- Phlebitis or varicosity of veins
- Hemophilia
- Lymphangitis
- Tissue integrity loss (remote)
- Sensory damage
- Significant inflammation
- Hematomas
- Irritable Condition
Precautions to keep in mind when approaching STM
- Contagious illnesses
- Skin diseases / lesions
- Malignant tumor
- Aneurysm
- Fragile skin
- Fracture
- Osteomyelitis
Contraindications to keep in mind when approaching STM
- Progressive loading (soft hands!)
- Depth dependent on patient
Application method considerations for STM
Start distally from target site and work towards it while gauging patient response
When performing STM where should you start the treatment?
- Depth
- Direction
- Frequency/Speed
- Duration
What are the parameters for documentation of STM
Cross friction/Transverse friction massage
What are the techniques used for scar massage
- circular
- vertical
- horizontal
What massage motions are used for scar massage
Cross friction massage not preferred over other techniques
What does the Literature Review of STM conclude
- Low to moderate levels of evidence for the benefits of STM over no treatment
- Low to very low evidence for the lack of benefit of STM over other active treatments
- Benefits suggest short-term improvement re: pain, range of motion
- No evidence in RCTs for IASTM for treating MSK pathologies over other techniques
- Weak evidence for short term improvement
What does the Literature Review of STM conclude on the benefits of STM
a therapeutic alliance approach incorporating other treatment modalities working towards functional activity
What is the best application of STM
- STM may be a useful short-term adjunct as part of a multimodal treatment package
- Can facilitate patient progress to performing more active strategies of patient care
STM as part of a treatment package
Taping
Application of an elastic / semi-elastic / rigid adhesive material to a region of the body to induce therapeutic effect
- Rigid structure
- Readily utilized by a variety of healthcare professionals
- Use in mobility-modified or restricted techniques
- Low dye
- Navicular sling
Athletic tape key points
- Rigid (tan) adhesive with anchor (white) tape
- Requires anchor application, then Leuko
- Use in mobility-modified or restricted techniques
- Patellar
Leuko / McConnell key points
- Elastic adhesive tape
- Capable of stretching 0-100% of resting length
- Accommodates well to body contour
- Capable of being modified into patterns
Kinesio-Tape key points
- Reduction of pain by inhibiting nociceptive stimuli
- Mimics thickness of skin / lifts skin to improve circulation and lymphatic drainage
- Motor control / kinesthetic feedback via cutaneous afferents to joint mechanoreceptors
- Neurofacilitation of alpha motoneurons resulting in improved strength
- Biomechanical correction of over/under facilitation of a given movement
- Placebo effect / patient expectations
What are the Controversial 'Proposed' Mechanisms of taping
- Off-loading of tissues via biomechanical correction
- Symptom modulation via afferent input for motor control
- Patient beliefs
Indication Considerations for taping techniques
- Use beyond 24 hours
- Be on the lookout for rash, signs of contact dermatitis, blistering / bullae formation
- Lack of belief in treatment approach
What are precautions for taping techniques
- Allergy to adhesive
- Use over wound, acute surgical site, and/or tissue warranting a referral to another medical provider
Contraindications for taping
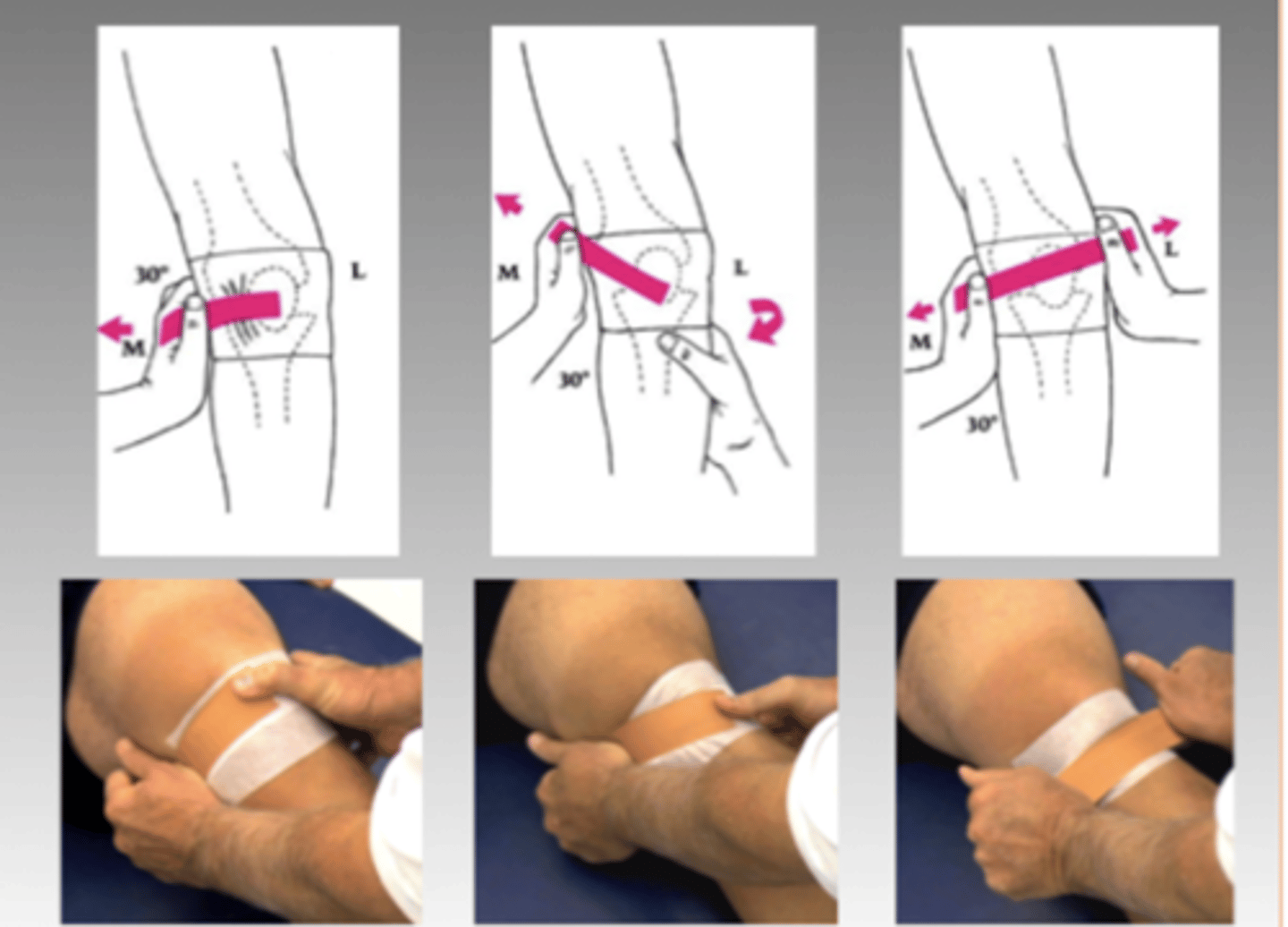
McConnell Taping
Medial tilt, medial glide, internal rotation and fat pad unloading (in order) until the participant's pain reduces by at least 50%.
McConnell Taping
Calcaneal or low-Dye taping for Plantar Fascia

- Level A evidence for short term (3 weeks or less) pain reduction and improved function for anti-pronation taping for PHP (Martin et al, 2014, CPG)
- Improvement in pain management and peak plantar pressure of hindfoot (Chae et al 2017)
- Improvement in pain, but equivocal for strength, range of motion, and function (Jiao et al, 2025)
- Meaningful gain in pain with medial glide McConnell technique over control, but limited data to calculate effect size (Wilson et al, 2003)
- Significant pooled standard mean difference in pain for KT tape vs. minimal intervention / no treatment (Lim et al 2015)
What is the literature consensus on the benefits of taping
- If best-practice doesn't hit the mark, and taping assists the patient, consider this a road worth traveling
- Ultimate goal is to remove tape and prevent reliance on external equipment
How should we apply taping to PT
Blood Flow Restriction (BFR)
- Training method that involves the use of cuffs placed proximally around a limb, with the aim of maintaining arterial inflow while occluding venous return during exercise
- Used in combination with exercise, most notably low-load resistance exercise
inducing skeletal muscle hypertrophy (strength gains) through pain tolerated loading amount and maximizing physiological processes for muscle growth
What is the goal of BFR
High-load resistance training
What is BFR an alternative to?
Relative ischemic and hypoxic muscular environment created by BFR creates high levels of metabolic stress → metabolic stress + mechanical tension drive hypertrophy and set off a metabolic cascade
- Elevated hormone production (GH, IGF-1, testosterone)
- Cell signaling pathways (Akt/mTOR pathway)
- Cell swelling
What are the proposed physiological metabolic effects of BFR
- stimulation of protein synthesis
- proliferation of myogenic satellite cells
- preferential activation and increased type II muscle fiber recruitment
The Relative ischemic and hypoxic muscular environment created by BFR creates high levels of metabolic stress → metabolic stress + mechanical tension drive hypertrophy and set off a metabolic cascade resulting in:
- BP cuff inflated until flow of blood is no longer detected (systolic)
- 40-80% of limb occlusion pressure used for exercise
- Modified as needed due to exercise
- Self reported means (pain, perceived occlusion) likely under LOP
Blood Flow Restriction Parameters for pressure
- Determine 1RM; train at 20-50% 1RM
- Application of exercise principles
- Duration variable
Blood Flow Restriction Parameters for exercise loading
Proximally at axilla, groin/thigh
Where are BFR devices typically placed?
- Strength/endurance training to compact atrophy, deconditioning
- Poor load tolerance
- Population specific considerations
BFR Indications
- RM performance
- CSA
- aerobic capacity
What are indications to use BFR for strength/endurance training to compact atrophy, deconditioning
- Higher severity and/or irritability
- Post-operative considerations
What are indications to use BFR for poor loading tolerance
- abnormal clotting
- age
- arterial calcification
- diabetes
- CVD
- acute fractures/open wounds
- immobility
- pregnancy
What are some contraindications for BFR
Trigger Point Dry Needling (TrDN)
Technique whereby a fine needle is used to penetrate the skin, subcutaneous tissues and muscle, with the intent to mechanically disrupt tissue without the use of an anesthetic
- 0.30mm x 40 mm for thinner muscles
- 0.30mm x 60 mm for thicker proposed
Trigger Point Dry Needling (TrDN) needle sizes
Often used to treat "myofascial trigger points"
What is Trigger Point Dry Needling (TrDN) typically used to treat
trigger points
Localized hypersensitive spots in a palpable taut band of muscle
active trigger points
produce spontaneous pain and reproduce patient's familiar pain when palpated
latent trigger points
do not produce spontaneous pain, reproduction of patient's pain with palpation
- Descending pain modulation
- Increase in pain pressure threshold
- Decreased muscle tone
- Decrease in pain
The Effects of TrDN based in theory, but largely focuses on local and central nervous responses at site of trigger point for:
25-30 seconds at 1 Hz; 2-3 mm vertical motions; 1-3 bouts
How should Manipulation of needle occur with goal of eliciting local twitch response
- Needle focused on local and neighboring areas
- Discontinued when decreased frequency of trigger response, decreased resistance to palpation, or patient intolerance
- Can consider superficial vs deeper DN
- Reassess for continued use
DN Technique
- Presence of myofascial trigger points
- Muscle contracture or taut bands
- Scar tissue
Dry needling indication
- Patient selection regarding needle phobia
- Cognitive impairment
- Local lymphedema
- 1st trimester of pregnancy
- Severe hyperalgesia or allodynia
Dry needling precaution
- Patients opting out for DN
- Children younger than 12
- Local skin lesion
- Local or systemic infection
- Allergy to material
- Vascular disease
- Abnormal bleeding tendency
- Compromised immune system
- Inability to communicate directly
Dry needling contraindication
TrDN Caveats
- Specialized training using this treatment is a must
- Although not considered an entry-level skill, you may have exposure to this during CEs