ACEIs and ARBs
1/121
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
122 Terms
Aldosterone
Stimulates sodium retention
What happens when angiotensin II binds to the AT1 receptor?
- Vasoconstriction
- Cell proliferation/hypertrophy of vascular smooth muscle cells and cardiac myocytes
- Sodium/water retention
- Increases extracellular matrix production
- Increases myocardial stiffness
What happens when angiotensin II binds to the AT2 receptor?
- Vasodilation
- Antiproliferation
- Apoptosis
What is the goal of ACE therapy?
Maximize AT2R effects while minimizing AT1R effects
What are the ACE substrates?
- Angiotensin I
- Bradykinin
How do ACE inhibitors work?
- Competitive inhibitors, inhibiting synthesis of Ang II
- Inhibit bradykinin inactivation, increasing levels (protective)
What are the antihypertensive effects of ACE inhibitors?
- Decrease peripheral vascular resistance
- Decrease aldosterone secretion
- Inhibit breakdown of vasodilatory bradykinins
- Enhance synthesis of vasodilatory prostaglandins
What are the heart-related effects of ACE inhibitors?
- Reduce cardiac myocyte hypertrophy
- Can slow/reverse aspects of cardiac remodeling
- Inhibit collagen deposition in heart and kidneys
- Some may treat HFrEF
What are the renal effects of ACE inhibitors?
- Decrease aldosterone production
- Restore and normalize pressure-natriuresis relationship (sodium excretion)
- Inhibit tubule sodium reabsorption
- Decrease arterial pressure by dilating renal arterioles
- Decrease proteinuria
- Reduce kidney scarring and fibrosis
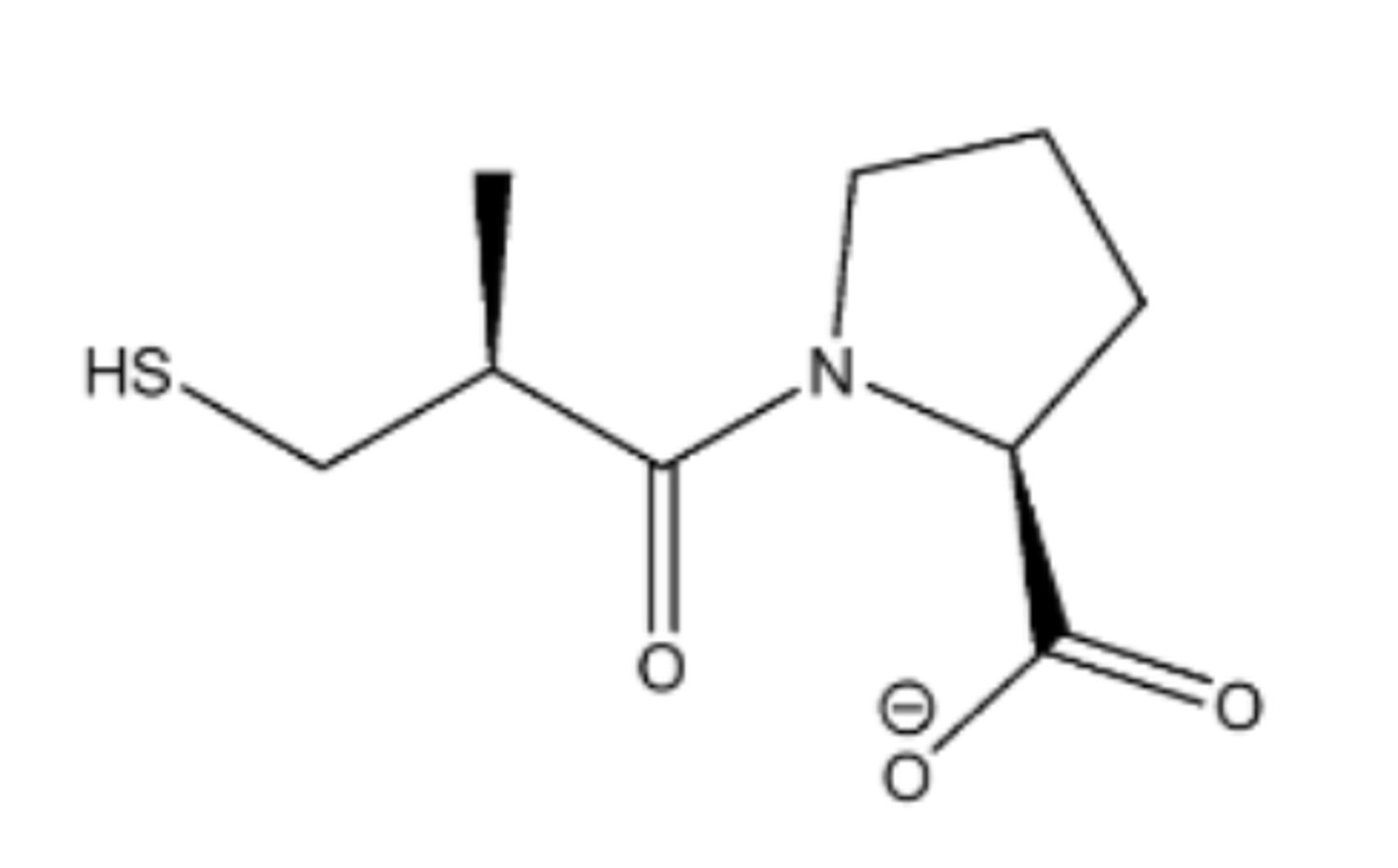
What are the key points of captopril?
- Sulfhydryl
- Synthetic dipeptide analog
- Competitive ACE inhibitor
- Active as administered
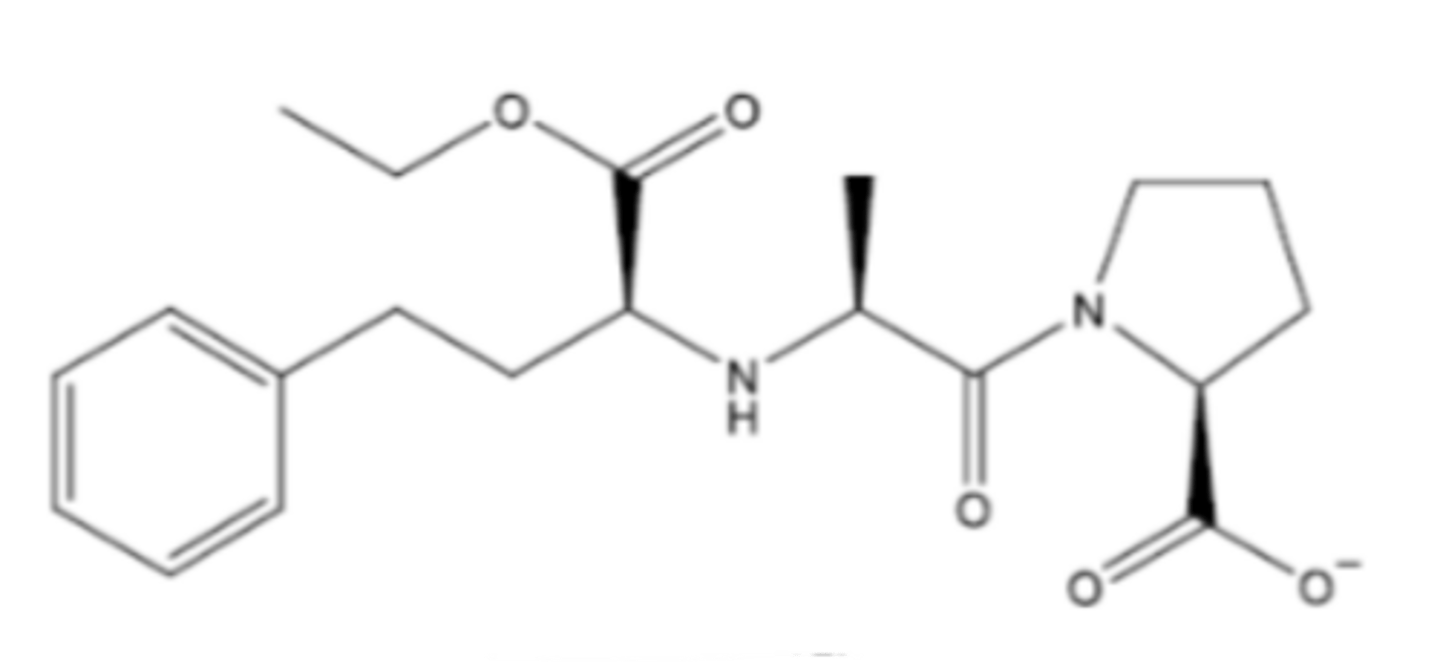
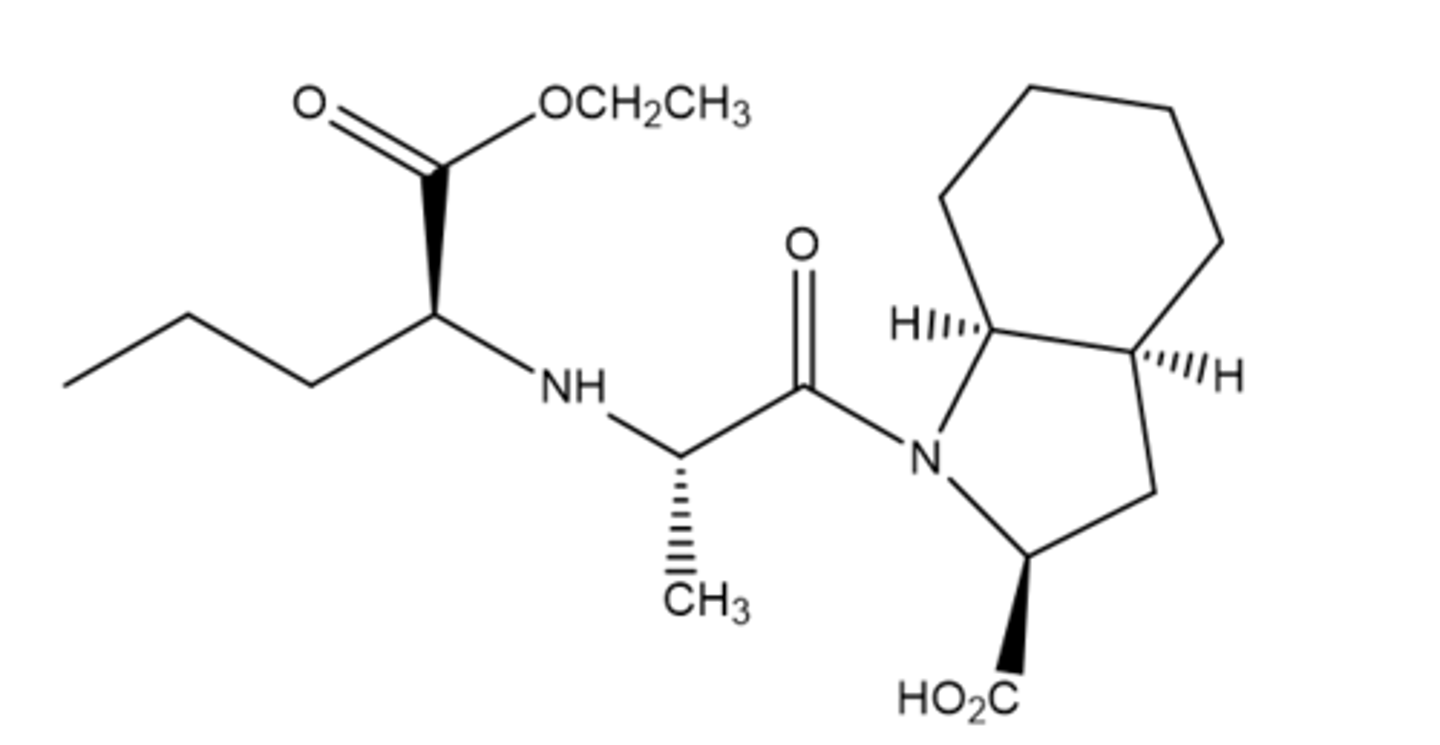
What are the key points of enalapril?
- Carboxyl
- Synthetic tripeptide analog
- Prodrug
- Metabolized to enalaprilat (active)
What are the indications for captopril?
- Hypertension in patients with normal renal function
- Left ventricular dysfunction (LVEF < 40%) after myocardial infarction
- Diabetic nephropathy
What are the indications for enalapril?
- Heart failure
- Hypertension
- Asymptomatic left ventricular dysfunction
What are the key points of lisinopril?
- Carboxyl
- Lysine analog of enalaprilat
- Active as administered
What are the indications for lisinopril?
- Hypertension
- Heart failure
- Acute myocardial infarction (improves survival)
What are the key points of ramipril?
- Carboxyl
- Prodrug
- Metabolized to ramiprilat (active)
- 50 times more potent than captopril
What are the indications for ramipril?
- Hypertension
- Heart failure post-myocardial infarction
- Reduction in risk of major cardiovascular events (MI, stroke, death)
What are the key points of moexipril hydrochloride?
- Prodrug
- Carboxyl
- Metabolized to moexiprilat (active)
What is the indication for moexipril hydrochloride
Hypertension
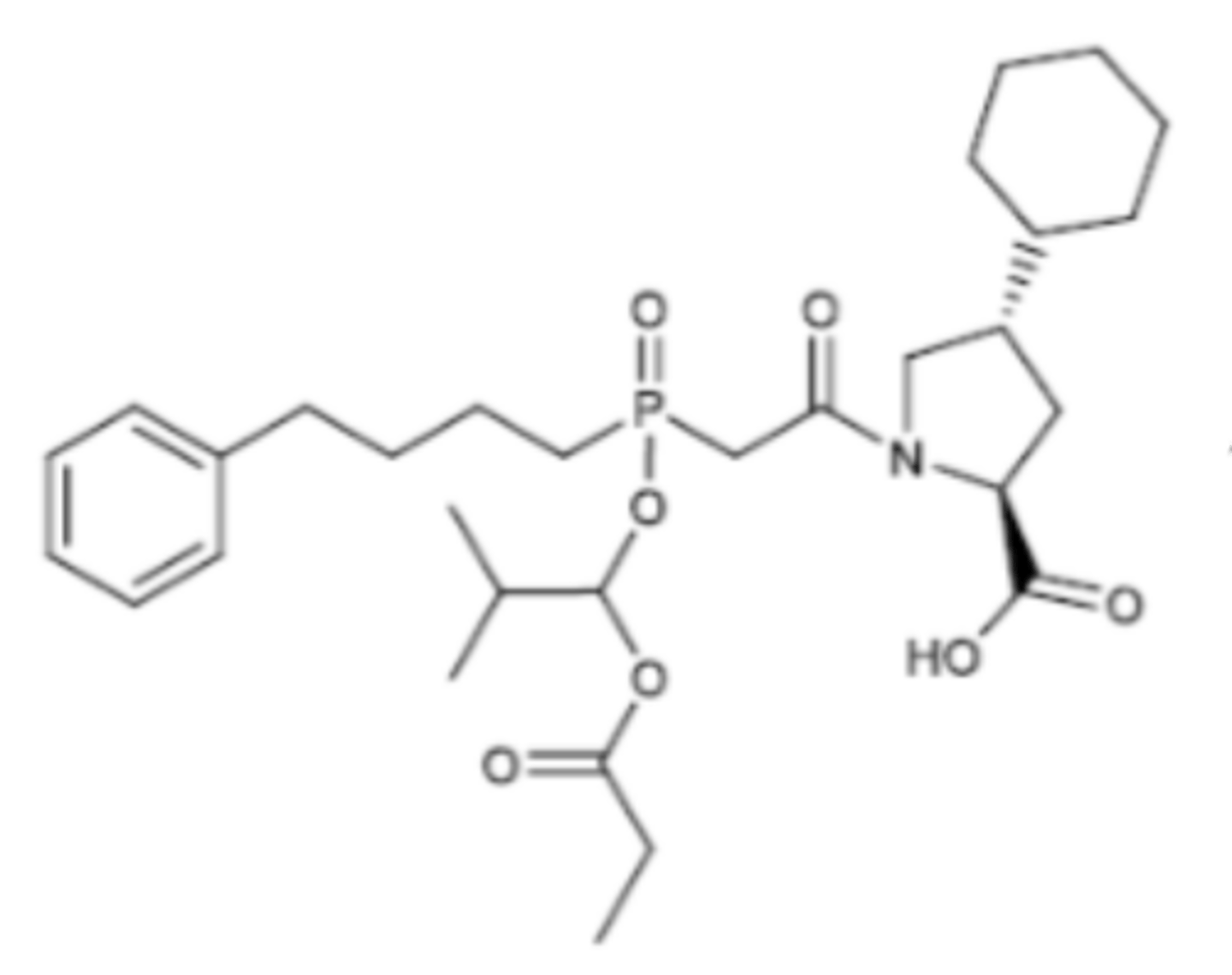
What are the key points of fosinopril?
- Phosphinic acid
- Prodrug
- Metabolized to fosinoprilat (active)
- Effectiveness is not affected by sex, race, or weight
- Binds to zinc group on the ACE active site
What are the indications for fosinopril?
- Hypertension
- Heart failure
What happens if an ACE inhibitor is taken during pregnancy?
- Fetal skull hypoplasia (teratogenic)
- Fetal hypotension
- Increased risk of fetal renal failure and death
What should you do if your patient gets pregnant while on an ACE inhibitor?
Discontinue and switch to an ARB (with caution)
What are the adverse effects of ACE inhibitors (not related to pregnancy)?
- Dry cough
- Angioedema
- Hypotension
- Hyperkalemia/arrhythmias
Why can ACE inhibitors cause dry cough?
Lung accumulation of bradykinin, substance P, and prostaglandins
Patients with what disease states should not take ACE inhibitors?
- Pregnancy
- Angioedema
Angiotensin II binds to MAS receptors.
False
Which of these is the BEST answer? ACE inhibitors:
A) Are active metabolites when administered
B) Are prodrugs that are converted by plasma esterases into the active metabolite
C) Both A and B are correct
D) None of the above
C
Which of the following is contraindicated when prescribing ACE inhibitors?
A) Angioedema
B) Cough
C) Pregnancy
D) Renal impairment from any cause
E) Both A and C
E
Identify the endogenous vasoconstricting agent that can stimulate the release of aldosterone from the renal glands.
Angiotensin II
This ACEI is an analogue of a dipeptide, is active as administered, and is the only US-approved inhibitor with a sulfhydryl group.
Captopril
A patient on the ACE inhibitor ramipril develops angioedema as an adverse effect. Which of the following would be the best recommendation for this patient?
The patient should be given the ARB losartan instead
Angiotensin II activates the AT2 receptors, resulting in all of the following effects except:
Decreased bradykinin metabolism
Which mechanism best explains the antihypertensive effect of ACE inhibitors?
Decreased conversion of angiotensin I to angiotensin II
A patient taking captopril develops a dry cough, which is causing insomnia. The dry cough is due to...
Accumulation of bradykinin and prostaglandins
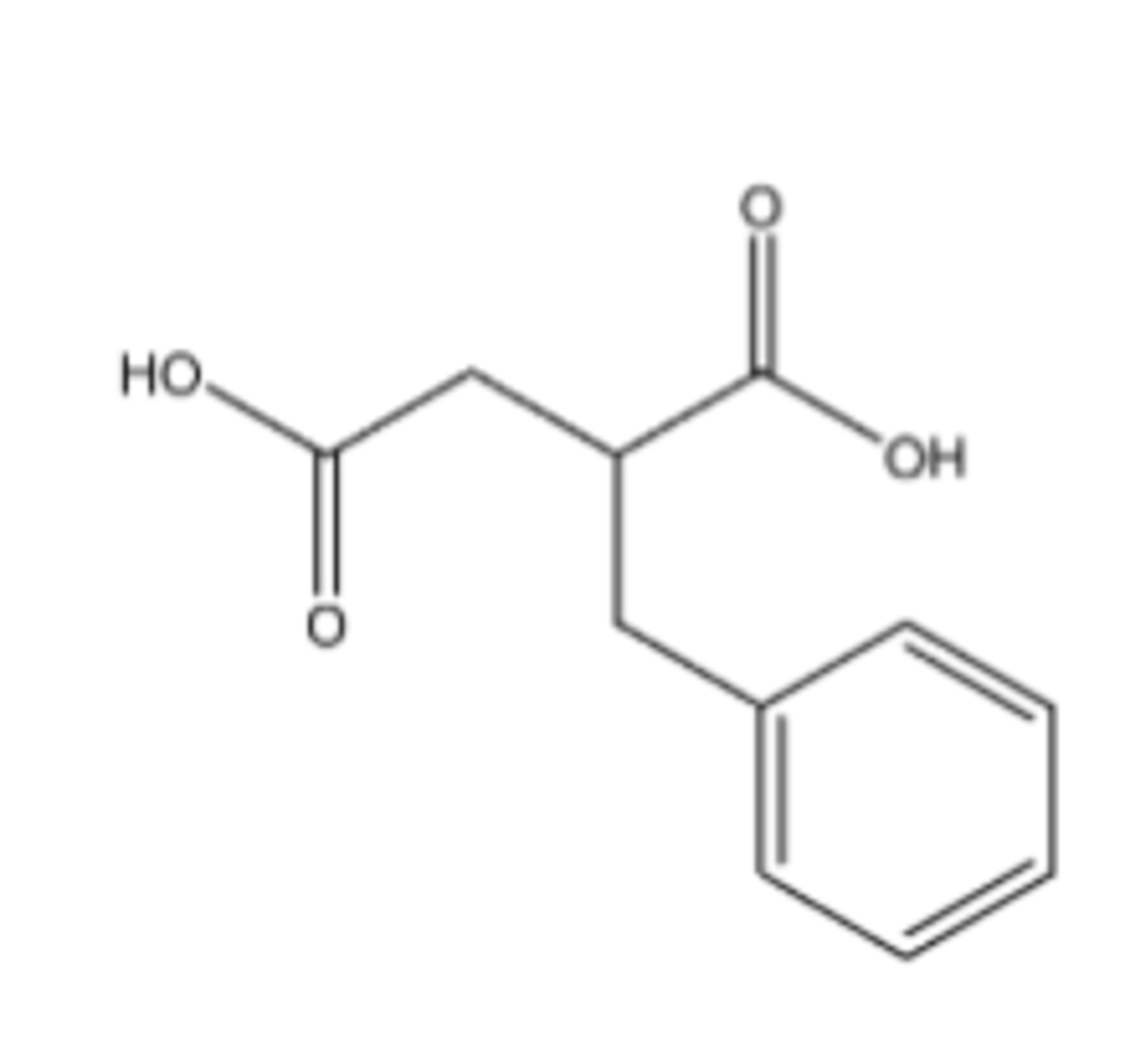
Benzylsuccinic acid
Inhibits carboxypeptidase A
Captopril
Enalapril
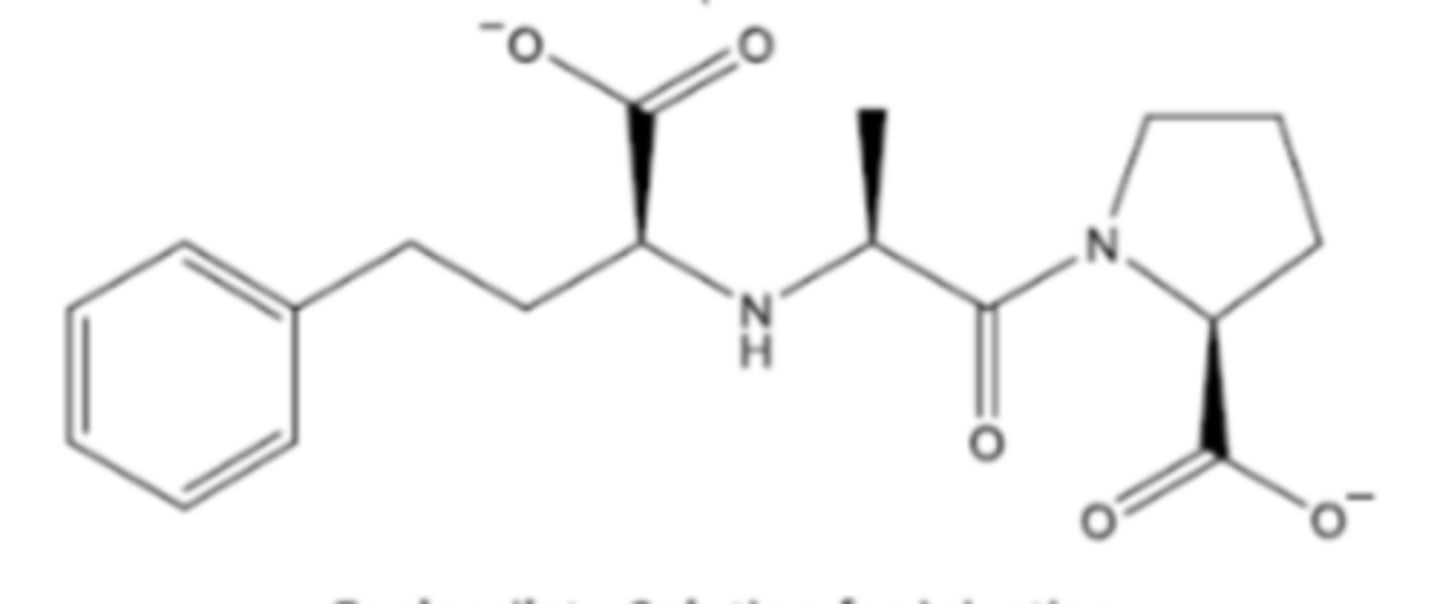
Enalaprilat
Lisinopril
Moexipril
Quinapril
Benazepril
Perindopril
Fosinopril
Fosinoprilat
ACE
Gluzincin metallopeptidase that cleaves the peptide linkages of Ang I and bradykinin with the help of a zinc ion
What happens when Ang II is produced?
- Increased blood pressure
- Sodium retention
What is the role of zinc in ACE action?
Forms a tetrahydral intermediate with a negatively-charged molecule (O, S)
What are the key points of captopril?
- Sulfhydryl ACE inhibitor
- Half-life 2 hours, taken 2-3 times daily
- Treats hypertension and heart failure
- Absorbed in the duodenum via passive diffusion, some PepT1
- Take 1 hour before meals
- Reactive, forms disulfide dimers/bonds
What are the adverse effects of captopril?
- Skin rash
- Long-term taste and smell disturbance
What are the key points of enalapril?
- Prodrug, metabolized by carboxylesterases in the liver
- Treats hypertension
- Metabolized to enalaprilat (active)
- Dicarboxylate ACE inhibitor
- Major PepT1 target in the intestines
- Enalaprilat has slow dissociation kinetics (half-life 11 hours)
What are the key points of lisinopril?
- Dicarboxylate ACE inhibitor
- Mainly absorbed through paracellular transport (slow)
- Forms zwitterion in the duodenum (pH = 6)
- Treats hypertension
What are the key points of moexipril?
- Dicarboxylate ACE inhibitor
- Treats hypertension
- Take 1 hour before meals
What are the key points of quinapril?
- Dicarboxylate ACE inhibitor
- Treats hypertension
- Used as adjunctive treatment for heart failure
What are the key points of ramipril?
- Dicarboxylate ACE inhibitor
- Treats hypertension and heart failure
- Very slow dissociation (half-life 50 hours)
- Mostly renally excreted
What are the key points of trandolapril?
- Dicarboxylate ACE inhibitor
- Treats hypertension and heart failure
- Very slow dissociation (half-life 24 hours)
- Less renally excreted than ramipril
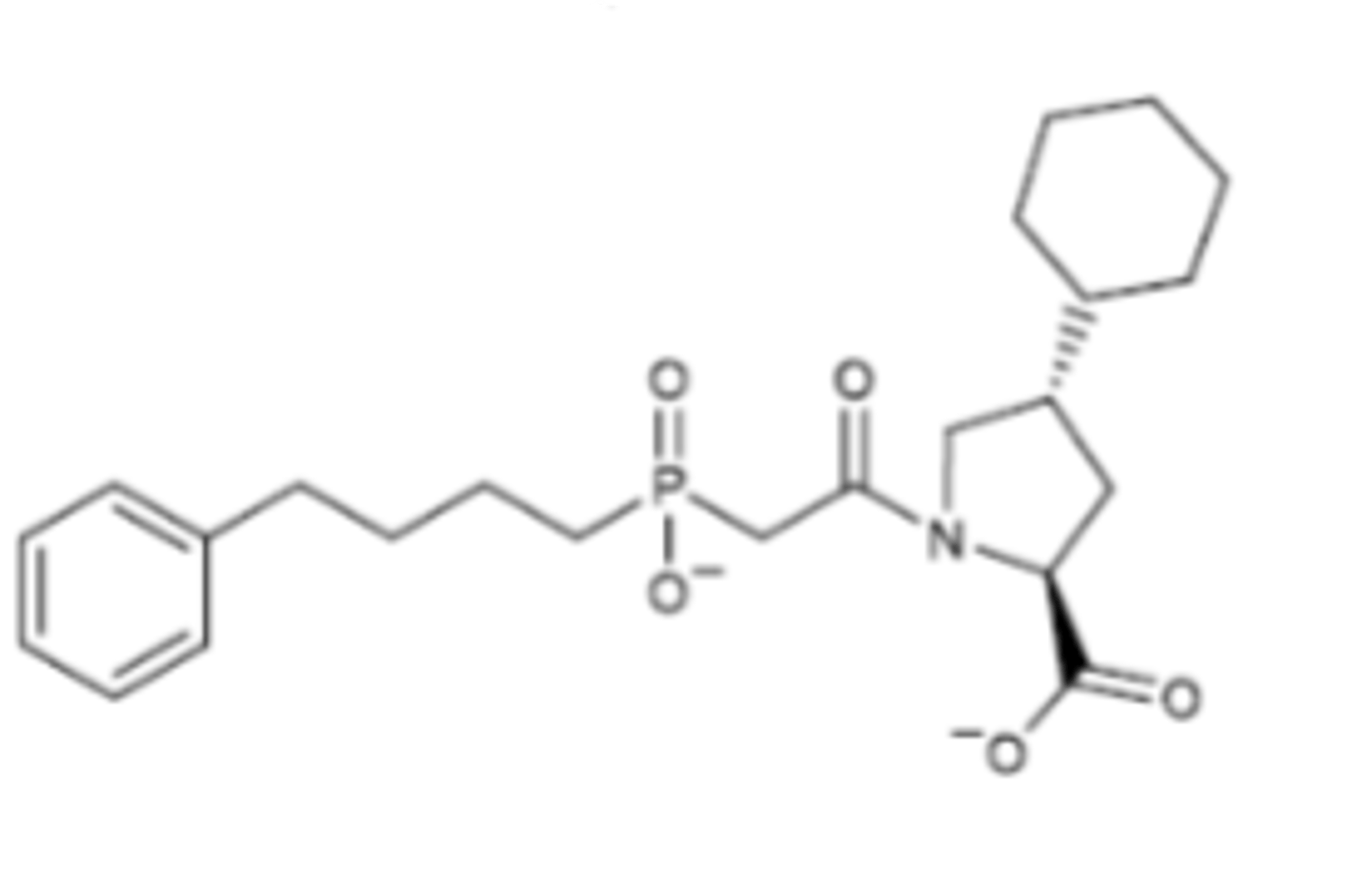
What are the key points of fosinopril?
- Phosphonate ACE inhibitor
- Prodrug, metabolized by hydrolysis
- Metabolized to fosinoprilat
- Binds in hydrophobic site and hydrophobic pocket of ACE
- Do not take with magnesium antacids
Saralasin
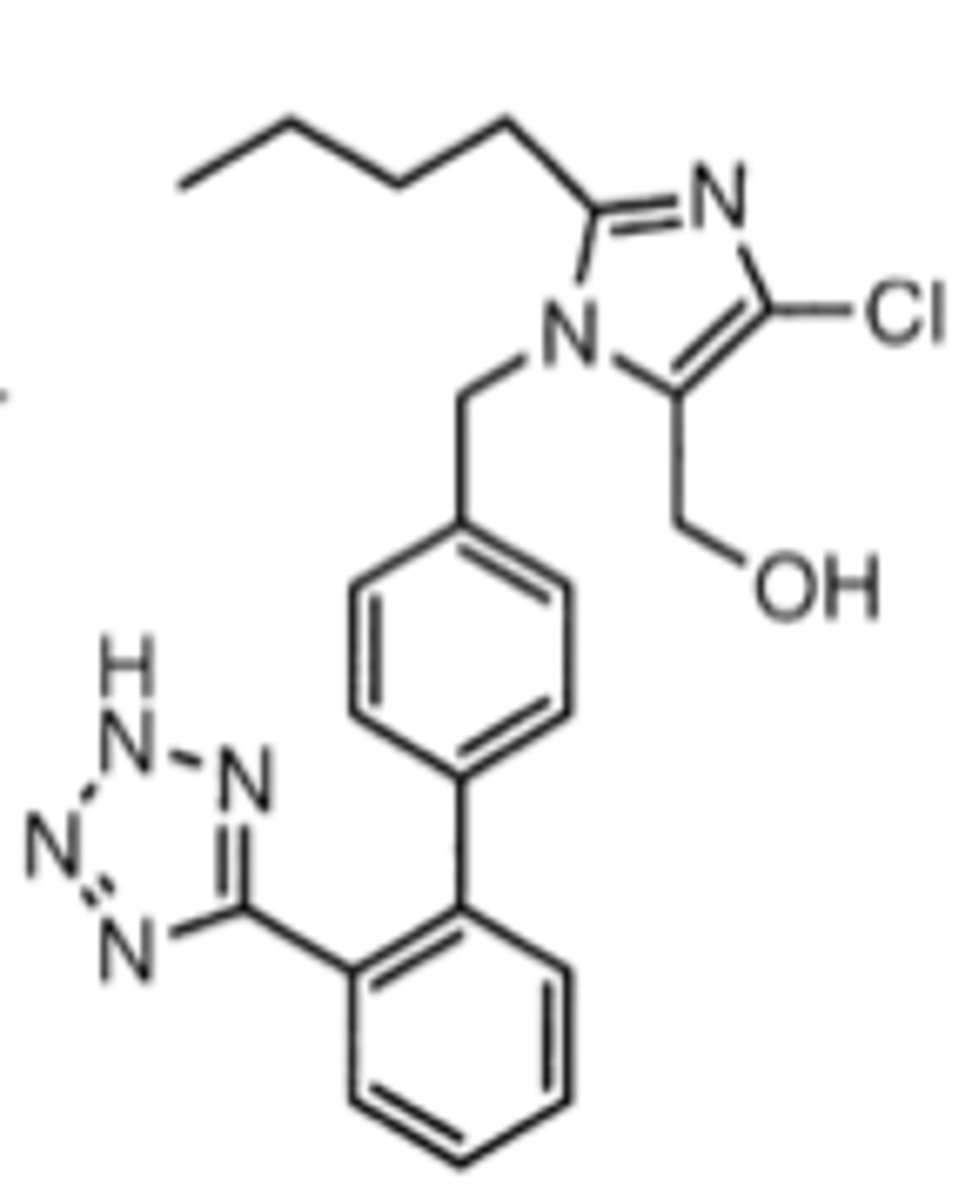
Losartan
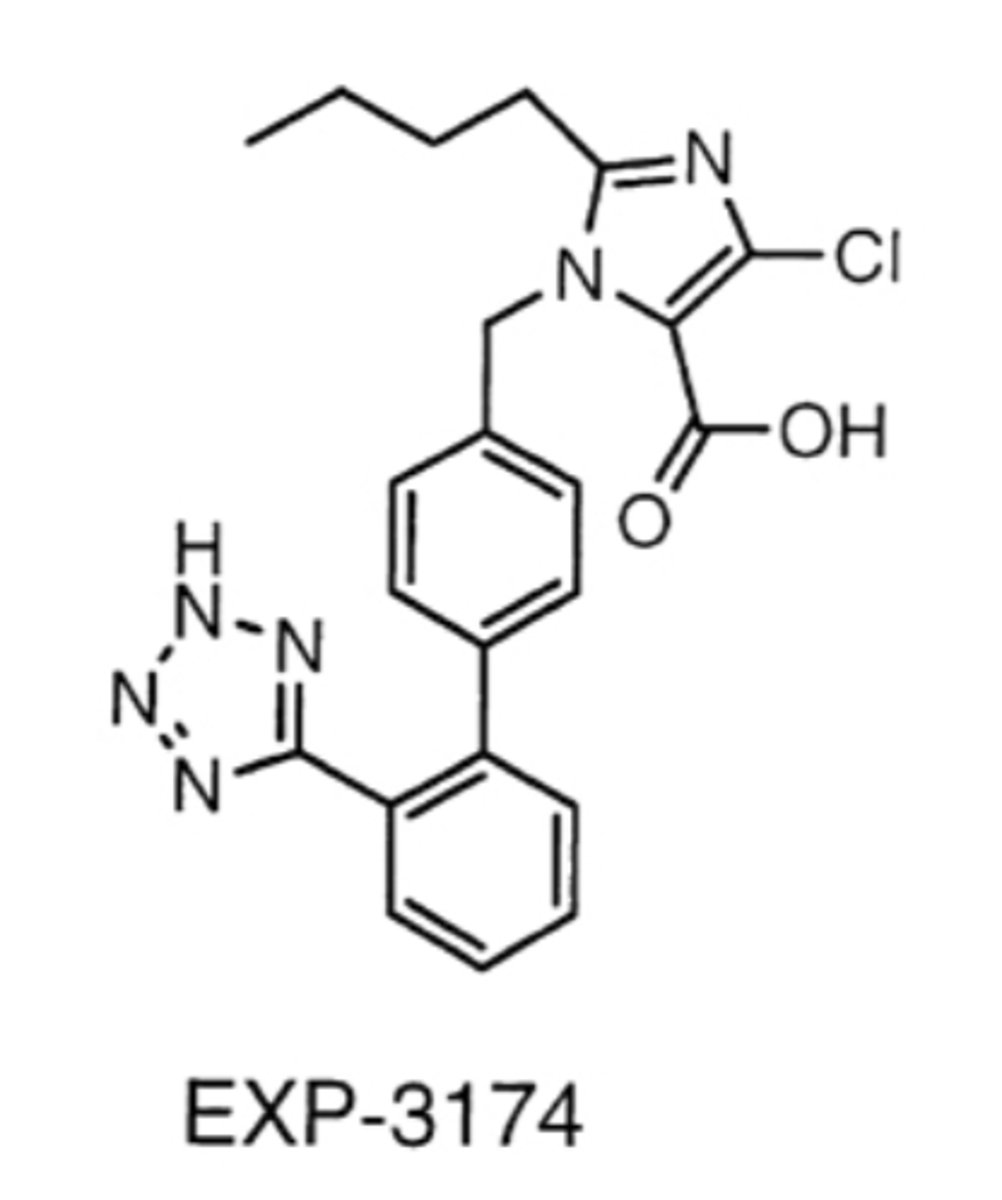
Losartan's more active metabolite
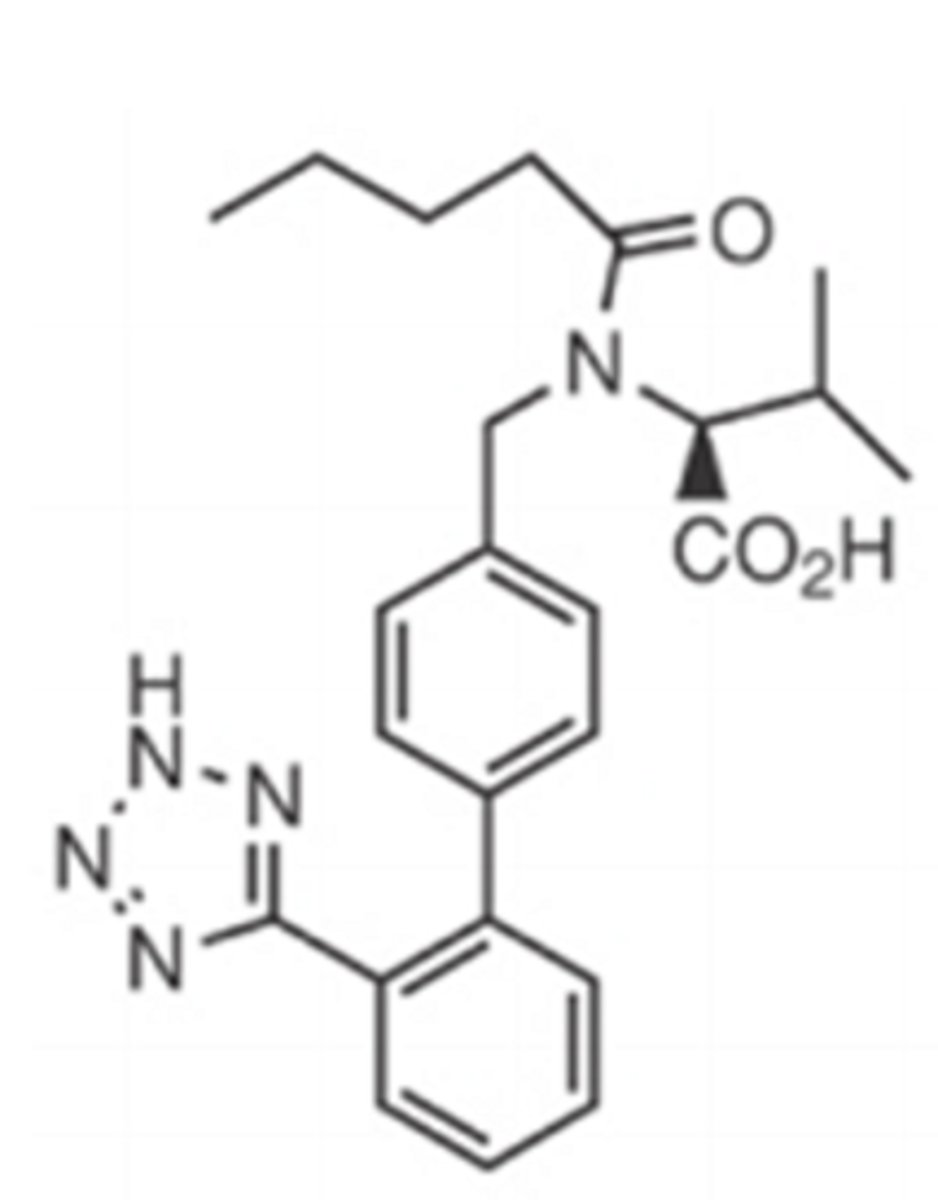
Valsartan
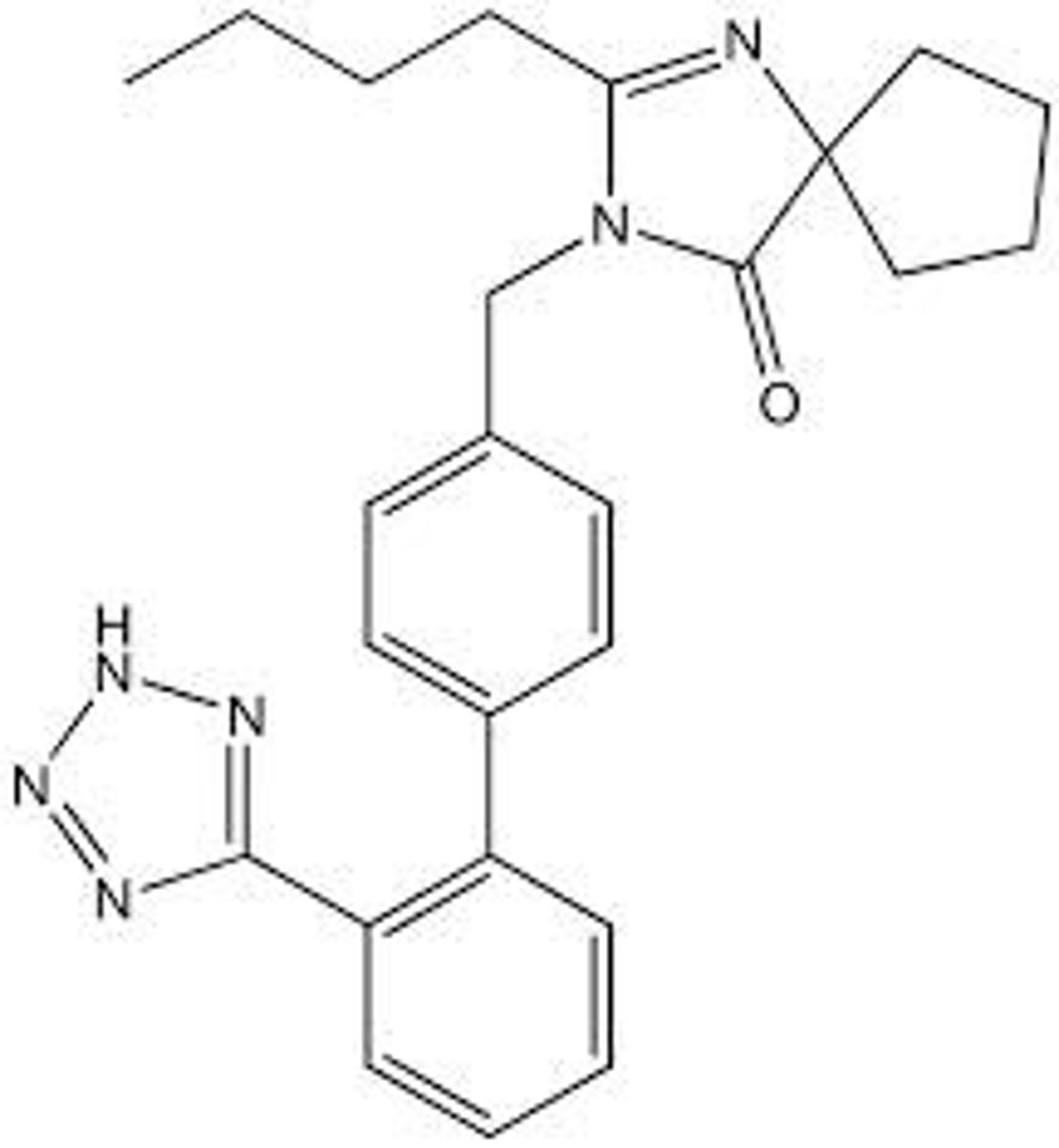
Irbesartan
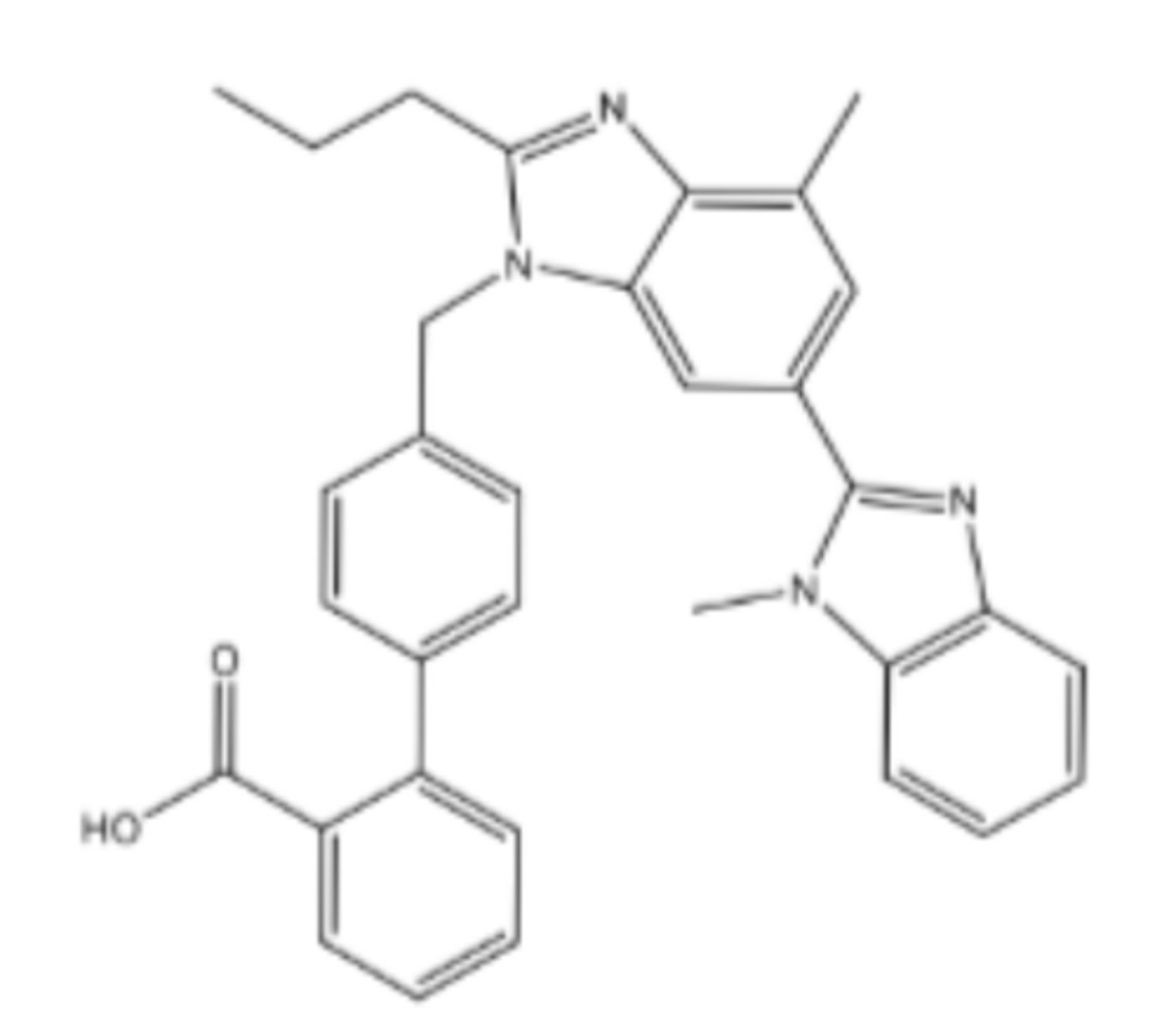
Telmisartan
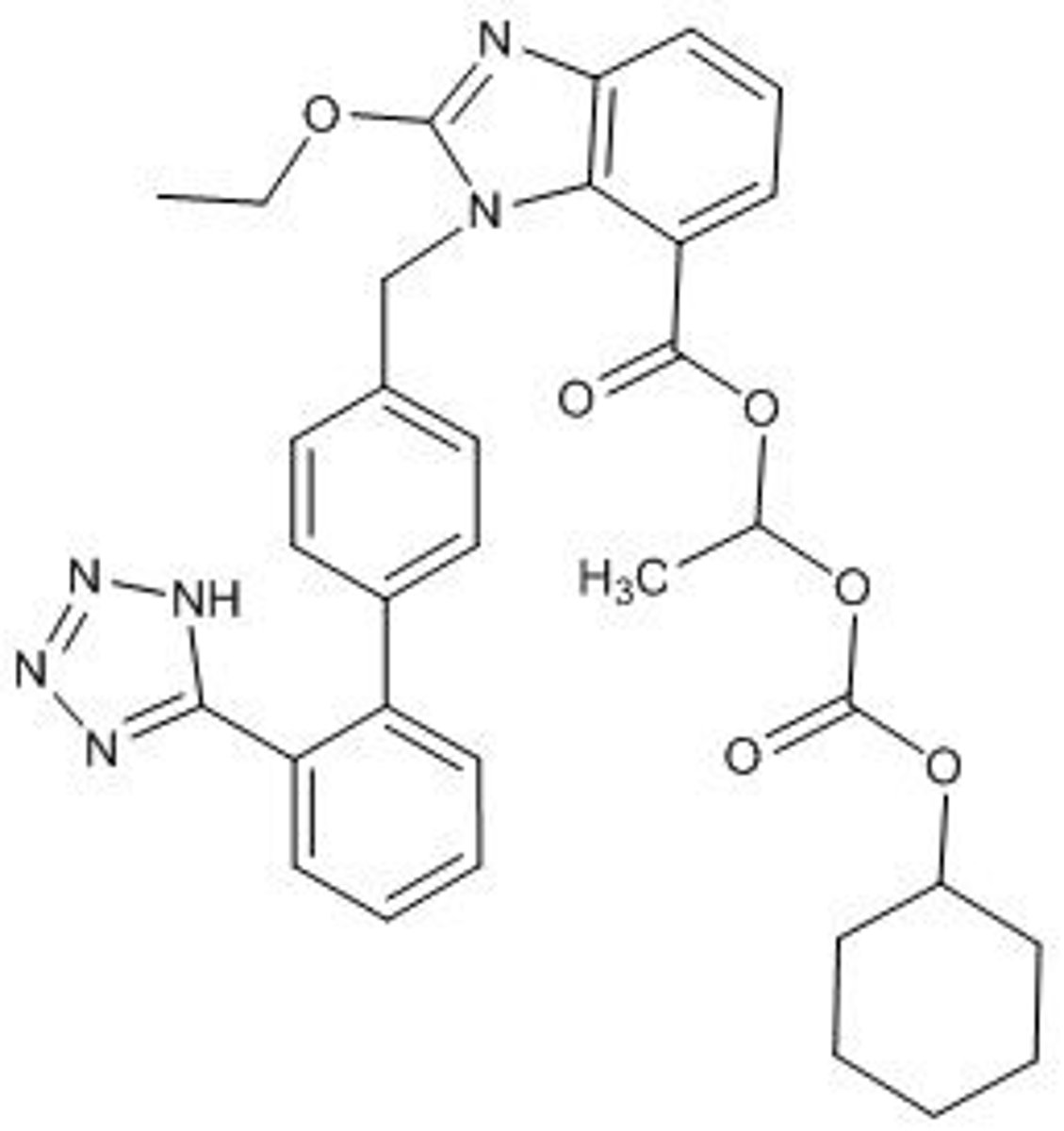
Candesartan cilexetil
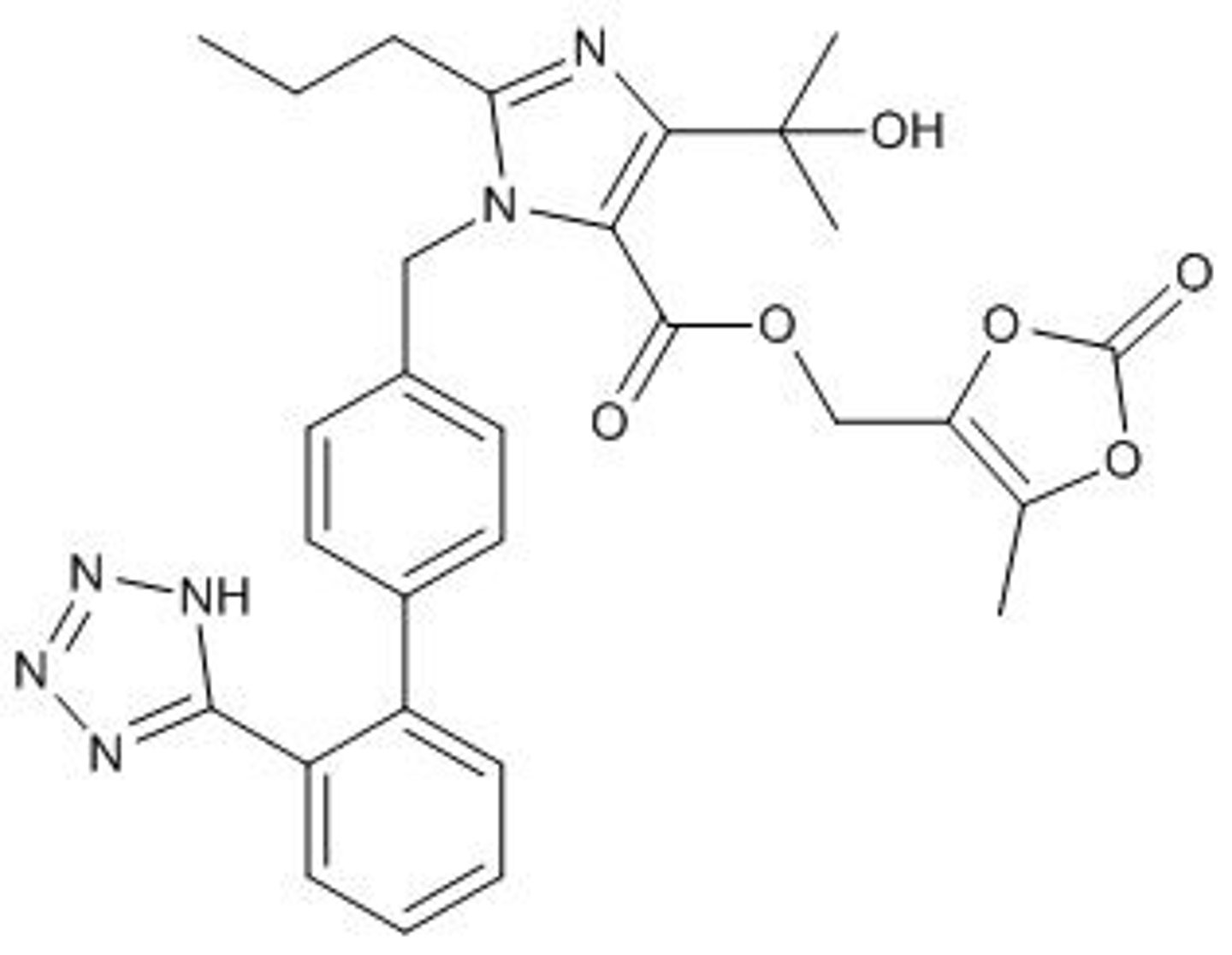
Olmesartan medoxomil
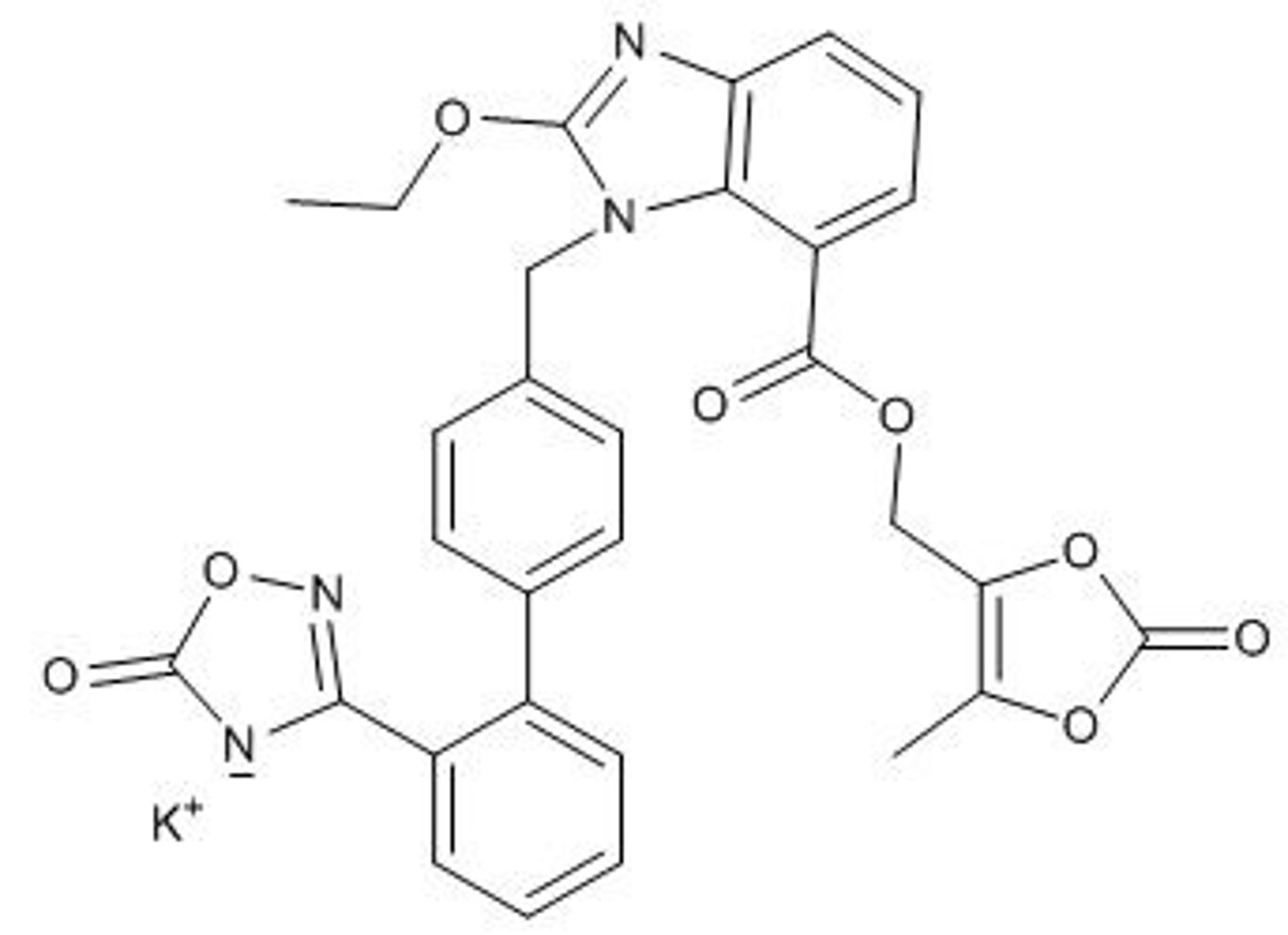
Azilsartan medoxomil
Sacubitril
Aliskiren
Baxdrostat
How do ARBs work?
- Bind to AT1R, blocking Ang II
- Cause vasodilation
- Decrease aldosterone secretion
What are the key points of saralasin?
- First known ARB
- Not orally active
- Short half-life
- Partial agonist
Why might a carboxylic acid be converted to a tetrazole on an ARB?
- Improved oral absorption
- Improved receptor binding
- Improved stability
- Decreased metabolism
- More hydrophobic
What are the key points of losartan?
- First ARB approved for clinical use
- Half-life 1.5-2 hours
- Metabolized by CYP2C9 and CYP3A4
- Metabolite is 10-40x more active, half-life 6-9 hours
- Treats hypertension, heart failure, and slows diabetic nephropathy
- Bioavailability 33%
What are the key points of valsartan?
- ARB
- Half-life 6-9 hours
- Bioavailability 25-35%
- Minimal metabolism
What are the key points of irbesartan?
- ARB
- Half-life 11-15 hours
- Bioavailability 60-80%
- Metabolized by CYP2C9
What are the key points of telmisartan?
- ARB
- Half-life 24 hours
- Bioavailability 40-58%
- Glucuronidated by UGT1A3
What are the key points of candesartan?
- ARB
- May be formulated as a prodrug
- Half-life 9-12 hours
- Bioavailability 15%
- Minimal metabolism
What are the key points of olmesartan?
- ARB
- May be formulated as a prodrug
- Half-life 10-15 hours
- Bioavailability 25-60%
- Minimal metabolism
What are the key points of azilsartan?
- ARB
- Half-life 11 hours
- Bioavailability 60-90%
- Minimal metabolism
- May be formulated as a prodrug
Which ARBs have major metabolic pathways?
- Losartan
- Irbesartan
- Telmisartan
What are the natriuretic peptides targeted by neprilysin (NEP)?
- Atrial natriuretic peptide (ANP)
- B-type natriuretic peptide (BNP)
- C-type natriuretic peptide (CNP)
What does B-type natriuretic peptide (BNP) do?
- Vasodilation
- Natriuresis (sodium excretion)
- Diuresis
- Inhibits RAAS
- Inhibits fibrosis
What does C-type natriuretic peptide (CNP) do?
- Vasorelaxant
- Cell proliferation inhibitor
What does ARNi stand for?
Angiotensin receptor-neprilysin inhibitor
What are the key points of sacubitril/valsartan (Entresto)?
- ARNi
- Neprilysin inhibitor prodrug (sacubitril)
- 1:1 molar ratio
- Treats chronic heart failure
How do direct renin inhibitors work?
Prevent conversion of angiotensinogen to Ang I
What are the key points of baxdrostat?
- Treats treatment-resistant hypertension
- Inhibits selective aldosterone synthase (CYP11B2)
- Little effects on cortisol synthesis
- Improved side effect profile
- Causes less stress to kidneys
What is aliskiren?
Direct renin inhibitor
How do ACEIs impact RAAS?
- Increase plasma renin concentration
- Increase plasma renin activity
- Increase Ang I concentration
- Decrease Ang II concentration
- Increase bradykinin concentration
- Decrease aldosterone concentration
How do ARBs impact RAAS?
- Increase plasma renin concentration
- Increase plasma renin activity
- Increase Ang I concentration
- Increase Ang II concentration
- No change in bradykinin concentration
- Decrease aldosterone concentration
How do DRIs impact RAAS?
- Increase plasma renin concentration
- Decrease plasma renin activity
- Decrease Ang I concentration
- Decrease Ang II concentration
- No change in bradykinin concentration
- Decrease aldosterone concentration
How does aliskiren work?
- Direct renin inhibitor
- Blocks conversion of renin to Ang I
How do ARBs work?
- Competitive AT1R inhibitors
- Block Ang II from binding to AT1R
What does Ang II activate?
- AT1R
- AT2R
What does Ang (1-7) activate?
- AT2R
- MasR
What is the preferred substrate for ACE2?
Ang II
What happens with chronic ACE inhibitor use?
Reduced efficacy
How do ACE inhibitors and ARBs impact AT1R activation?
- ACE inhibitors decrease AT1R activation
- ARBs decrease AT1R activation
How do ACE inhibitors and ARBs impact AT2R activation?
- ACE inhibitors decrease AT2R activation
- ARBs increase AT2R activation