11: options other than glasses
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
spectacles
most commonly prescribed
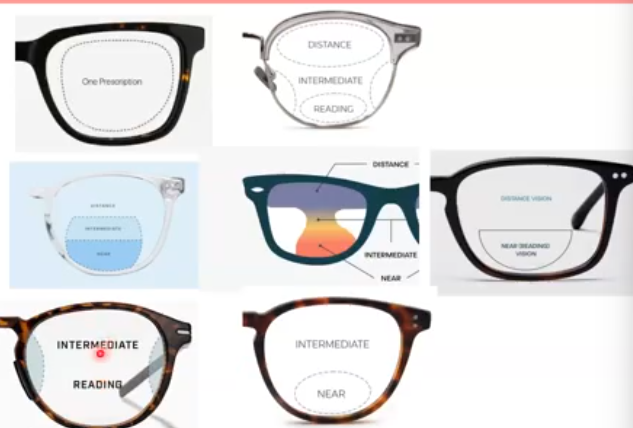
single vision
bifocal - near at bottom, distance at the top
trifocal - distance at top, intermediate and near at bottom
varifocal/progressive - distance, intermediate and near, smooth transition bewteen int and near, but can get distortion around edges
degressive/office/occupation - intermediate and reading only
what ways lenses can be adjusted by
tinted - darker at top, lighter at bottom
polarised - removes reflections
mirrored - mirror surface where people cant see your eyes
transitions - reactive to light, slowly gets darker from clear to dark when exposed to UV. work better when cold
prism - bends light all in one direction
advantages of specs
cheaper
reusable
customisable and fashionable
can include therapeutic treatment
minimally invasive/ risk of infection
potential for AR or VR technology and digital tools
disadvantages of specs
cant fit all faces
custom specs are expensive
can be broken
not subtle, can cause sensitivity
can get lost
types of contact lenses
soft contact lenses
rigid permeable contact lenses
miscellaneous speciality contact lenses
soft contact lenses
low oxygen transmission
thin flexible lenses made from hydrogel and silicone hydrogel
mainly contains water, allows oxygen to pass through to the eye
advantages of soft contact lenses
discreet- no specs needed
versatile
reusable
customisable
can fit faces that specs may be difficult for
disadvantages of contact lenses
cant fit all eyes
some people cant wear them
requires certain amount of dexterity
can be expensive
risk of infections and side effects
contact lens optics
no back vertex distance
no change in retinal image size with a contact lenses, with specs the images will either be magnified ( hyperopia) or minified ( myopia)
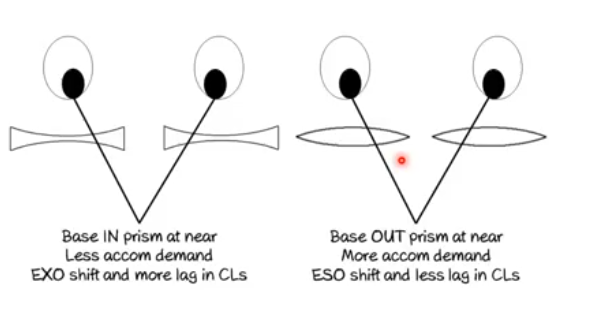
contact lens optics- accom
accom and convergence does not change with contact lenses as no BVP
rigid contact lenses
small, unbendable, and sit on the cornea and let oxygen through
mostly made from fluorosillicone acrylates and oxygen permeable
cover the entire cornea
advantages of RGPs
good vision
less risk of infection
used to give vision for diseases like keratoconus
much cheaper over time
disadvantages of RGPs
require adaptation to initial discomfort
not as simple to fit
can cause a ptosis over long term use
complex contact lenses
used for those with complicated eye conditions or vision problems
hybrid - rigid centre, soft outer skirt and used for keratoconus, high astigmatism and px who cant tolerate RGPs
piggyback - wearing 2 CLs on the same eye and a RGP is placed on top of the soft contact lens : keratoconus, irregular cornea
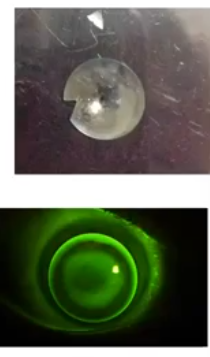
orthokeratology - specially designed rigid lenses worn overnight to temporarily reshape cornea
sclera/corneaoscleral lenses - large RGP lenses that rest partly on the cornea and partly on the sclera. creates tear filled space over conea and helps smooth out irregular corneal surfaces
refractive surgery options
radial keratotomy- cutting through the cornea until it becomes flat
LASEK
LASIK
clear lens extraction/replacement
can correct myopia, hyperopia, astigmatism and presbyopia
laser surgery- LASEK
laser epithelium keraromileusis
creates a flap of the cornea using 205 alcohol solution for 30 seconds to soften cornea and dissolve adhesion of hemidesmosomes to bowmans membrane
epikeratome is then used to push the flap created to the side
anterior corneal stroma is then abalated by the required amount where needed and then replaced back into stroma
bandage CL used to keep flap in place until readhered
used more when cornea is thin and there is less tissue to use
disadvantges of LASEK
more pain and photophobia
smaller area of vision as limited by size of epithlial flap
distorted vision and sometimes haze initially- depends on the state of healing, but also size of flap, if too small you may get edge of disortion
Rx stabilised after 3 months
can have some regression
laser surgery- LASIK
corneal flap is cut now instead, slightly deeper to allow middle stromal shaping
cut either with a microkeratome or femtosecond laser
topical anasthetic needed
lid speculum holds lids open and suction ring put on cornea. IOP can rise above 50mmHg
reshape underneath and then reposition flap
imporvements include wavefront guided laser surgery to remove higher order aberrations and imporve visual quaility
timeline of LASIK
fast recovery- sometimes within a few hours
grittiness and watery vision in day 1
2 days flap subsides
1 month to get less glare and haloes around lights
some refractive shift still may occur in first 6 months
Rx stabilised in few months with reduction of scar until only visible on slit lamp or with fluorescein
post op complications of laser surgery
infections
over or under correction likely
5% may need retreatment
irregular astig and persistent haloes
reduced constrast sensitivity
dry eye sensations- up to 6 months
stromal haze
diffuse lamellar kerititis
myopic regression- cutting too much of cornea can cause keratoconus
refractive surgery- IOLs
either clear lens extraction for high myopes or essentially an early cataract operation with adjustment to the presciption to correct refractive error
case:
40 year old myope
large prescription: -20D in each eye, stable for the last 5 years
specs causing facial irritation, and px wants change
what alternative refractive corrections are there?
how could you explain the pros and cons of the different options
too high of a prescription for laser surgery
IOLs: better option due to age and how high the prescription is
pros are that is is not permanent so px can change mind,
case 2:
20 year old hyperope
shy, and come in for routine sight test and wants to be an uber driver
refraction: +10.00/-2.00 × 180 Rx in both eyes
px unhappy with their glasses
what options does px have and what is most recommended
are there any requirements in relation to their work aspiration?
no surgery as high prescription
RGPs more better, can do soft contact lenses