Psych 3rd 3rd
1/111
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
112 Terms
Social psychology — we are social species
Solitary species vs social species (humans only ability)
Our ability to cooperate is one of the major reasons we succeed as a species
But comes with strings attached
Social Psychology
The branch of psychology that studies how individuals think about, influence and relate to other people
Misinfos about social psychology
• Most view being influenced as weakness (they shouldn’t)
• Most believe highly resistant to social pressures (they’re wrong)
• In certain cases, both tendencies could be a “strength”
• Achieve group cohesion + finish tasks
• We are continually participating in social networks
Social networks
Humans have history of working in small groups (e.g. tribes) (~150 members, according to Dunbar)
Quantity not all that matters — quality matters too
While overall network large, number of close relationships modest
Networks can change with time (technology, stress, age)
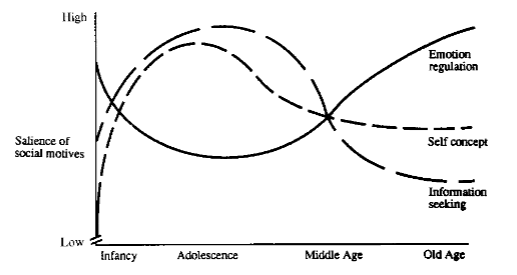
Socioemotional selectivity theory
Predicts older adults have fewer relationships — based on different motives (i.e. emotion regulation)
older —→ emotional regulation
young —→ many reasons
Need to belong theory
Humans have a fundamental drive to form/maintain relationships
.
Absence of relationships might be harmful
Solitary confinement in prison + lockdowns (effects differ by age)
quality of relationships also matter
.
Few experimental studies of isolation (most are correlational)
one study only 1 of 5 subjects lasted > 3 days
subjects given belief they would end up alone showed unhealthy behaviours, procrastination, impaired cognition
Loneliness
Loneliness is related to, but distinct from, isolation
isolation = lack of social contact, not necessarily bad
loneliness = feeling lack of connection, inherently negative
both related to health outcomes (mental, physical)
.
Reports of loneliness increasing (“epidemic”)
Before COVID: 1/3, with 1/12 cases being severe
we spend more time alone now
.
Not easily treatable
forced interaction
support networks
social skills training
Being a part of a group can change your behavior
Groups: Social contagion
When a belief rapidly spreads throughout a group
though is often pejorative (not bad or good), impact depends on belief
.
Related term: mass hysteria
Large group, behaviors both irrational and harmful
Many potential examples
Urban legends, UFO reports
emotional contagions well-accepted; clinical contagions (e.g. dissociative identity disorder and depression) suggested but more controversial
Dissociative Identity Disorder
Affected person claims to have at least two identities
may alternatively display
memory impairment of prior states common
.
More common in women (reason unknown)
.
Controversial
cultural factors
improper interventions
misdiagnosed?
Groups: Social loafing
Tendency to put in less effort/do less work in groups
Possible variation of bystander effect (e.g. diffusion of responsibility)
Many examples:
cheerleaders less loud in groups
pull less hard on rope
generate fewer/less creative ideas
May be less evident in collectivist societies
Groups: Deindividuation
Engage in behavior atypical for us but consistent w/contextual norms
.
Key factors are a feeling of anonymity and lack of accountability
.
Example: behaviour when masked
child wearing masks more likely to take ‘forbidden candy’
presence of mirror may reduce
.
Major potential examples: online behavior, crowd behavior, stanford prison study
1 – Online behavior
Sometimes cute + funny (e.g. hijacking online polls and voting for ridiculous options)
.
Sometimes cruel + terrifying (e.g. cyber-bullying)
males more frequent perpertrators
associated with psychological + academic problems in victims
common: much wider age spectrum
Online behavior — cont.
Though it often involves deindividuation, it does not require it
.
In some cases: people used real identities and articulated real beliefs
Typical behavior, no anonymity but possibility of accountability
.
Motivating factor is likely a desire to enforce certain ideals: cultural, political and religious values
think youre speaking the truth
2 – Deindividuation in Crowds
People routinely gather in large groups
One of the most striking example of this is protests
Many throughout history, some of which include 10 000+ people in one place
Most crowds and protests are peaceful
3 – The Stanford Prison Study
Observational, not experimental
24 participants randomly assigned to roles of prisoner/guard, head of study was superintendent
people reportedly became consumed in roles, losing identity and behaving atypically
very popular and controversial
The Stanford Prison Study — cont.
Though initially most participants believed that they were incapable of cruelty, cruel behaviors did emerge
Some guards (~33%) showed aggressive and concerning behaviors (humiliation, do push-ups, strip naked and clean toilets with bare hands)
supposed to be two weeks but was ended after six days
Criticisms of stanford prison study
Small sample size (n)
Selection bias (whoever responded to the ad)
Demand characteristics (some ideas of what the experimenter wants) + observer effect (know experimenter is watching)
Emphasis on qualitative, anecdotal reports: difficult to verify and analyze quantitatively
Experimenter (Zimbardo) was involved (superint.)
Numerous ethical issues (never fully repeated)
When discussing influence…Obedience and conformity
Obedience: Listening to a figure of authority (e.g. a persuasive politician or a strong sergeant)
generally explicit
.
Conformity: Adopting the predominant belief or behavior of a group due to pressure from that group
generally implicit
.
Not by themselves bad
issues from blindly following without asking questions
Obedience: Milgram’s story
Child of Jewish parents who grew up through World War 2
Preoccupied with atrocities of Holocaust and wondered how people could commit such horrific acts
Prevailing view at the time was such acts were due to “twisted minds” (bad people do bad things)
However, Milgram’s research suggested that situational factors could have also played a role (bad situations, rather than bad people)
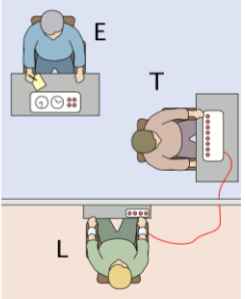
Milgram Experiment
(E) is an experimenter overseeing everything
Participant acts as a teacher (T) who asks the learner (L) questions
(T) is told to give (L) a shock for wrong answers*
(L) is an actor who pretends to be shocked and protests to the shocks
(confederate: working with the study)
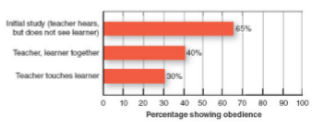
Important Factors of Milgrim experiment — saying no
Proximity + contact with learner reduced willingness to give shocks
Some participants stopped complying as intensity increased (15 to 450V), but majority (66%) stayed
When a confederate scientist was present and disagreed with the experimenter, compliance was 0%
value of dissenting voices
when someone else disagrees, more comfortable disagreeing ourselves
Important Factors of Milgrim experiment — performance
No major cultural differences or gender differences
Compliance is not related to sadistic tendencies, but is related to other traits (obedience and authoritarianism)
Failure to comply is related to moral development, though this relationship is not especially strong
Despite many increasing criticism of late (e.g. ethics, internal validity), it does have value
Conformity: Asch’s study on conformity
Subjects participated in a study w/several confederates
.
Subject had to declare which of 3 lines was longer
.
Before the subject made their judgement, they heard several confederates make an incorrect judgment
subjects readily conformed to wrong opinion
rates of conformity increased w/group size to a point (ceiling effect)
On conformity
We all show some capacity; the question is how much and how often
Low self-esteem predicts high conformity
Cultural differences possible; conformity may be greater in collectivist cultures than in individualistic cultures
Gender differences in conformity are disputed
Individualism vs. Collectivism
Index reflects the degree to which people are integrated into groups
High index of individualism = individualistic society
Low index of individualism = collectivist society
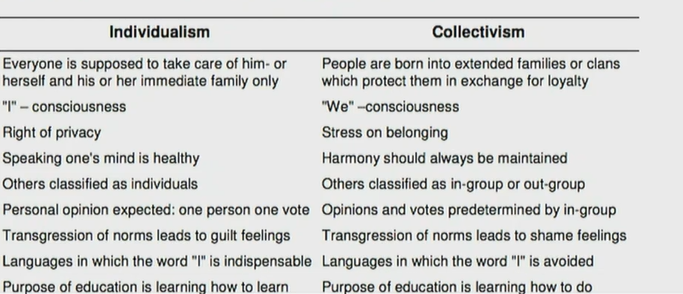
Individualism vs. Collectivism — details
Western societies — tend toward individualism
Eastern societies — tend toward collectivism
.
May infulence many behaviors
family attitudes
facial expressions
prosocial behaviors
creativity
.
Must avoid stereotypes and focus on what is scientifically proven
findings often controversial
Cults
Groups with intense and unquestioning devotion to a single cause
NXIVM, heaven’s gate, etc
.
Difficult to study due to secretive nature
.
Several consistent features:
persuasive leader who inspires loyalty
members disconnected from outside world
questions/dissent discouraged
training practices that gradually indoctrinate members
Misconceptions of cults
Cults are easy to identify and define
Most cults are dangerous to others
most peaceful to others, even if harmful to members
Most people in cults are mentally ill (FAE)
33% (higher than normal), most cult leaders are mentally ill
Brainwashing is required (controversial)
Prosocial behavior
Voluntary behavior for the benefit of others (e.g. friends, family, strangers or enemies)
Assume altruistic (unselfish concern) = prosocial
Prosocial behaviors are associated w/higher psychological + physical well-being in the helper
feels good to be good
What about punishment?
Just punishments can also be regarded as prosocial
discourage bad behavior, benefits group
educate transgressor
costly punishments (punisher pays a cost to deliver punishment) percieved as more legitimate
.
Controversial idea
punishment may not be based on universal principles; could simply be defensive response to your community being attacked
Predicting prosociality
Mood (esp. good moods)
Timing (when not rushed)
Potential for escape (likely to help if we can’t leave)
Background (e.g. doctor, nurse…)
Trait extroversion and empathy
Characteristics of the person in need (matching)
Egotistic reasons (relieving personal distress, joy of others we’ve helped, image of being a “better person”)
Bystander effect
Reduced likelihood to assist others when in groups
Many explanations
pluralistic ignorance (maybe its not really a problem)
diffusion of responsibility (someone else will do it)
cost of intervention, physical or psychological (feelings of judgement/vulnerability)
Among the strongest and most replicable effects
Aggression
Behavior intended to harm others, either verbally or physically
.
Most real-world studies are observational
.
Most laboratory studies use different measures (i.e. a test), do not resemble aggression in real world (e.g. assault)
unethical otherwise
.
Degree and severity affected by many factors
Aggression is more likely if…
Male, especially for direct aggression (w/confrontation)
Provocation by the individual (specific)
Overall frustration (non-specific)
Physiological arousal (w/provocation + frustration)
Reinforced by media (e.g. television, video games) and cues (e.g. guns)
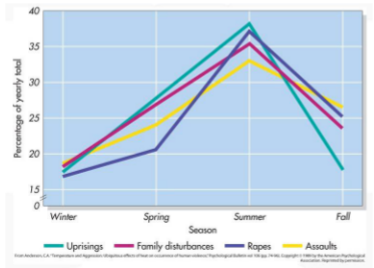
Alcohol and temperature
Aggression and Temperature
Relationship holds in many countries and for many types of aggression, including severe (assaults) and mild acts (beanballs in baseball — throwing ball at batters face)
Heuristics
An approach to decision-making, problem-solving or discovery
We are faced with many problems, must make many important decisions quickly
Heuristics are useful
can be executed quickly, dont require lots of information
but, arent always accurate
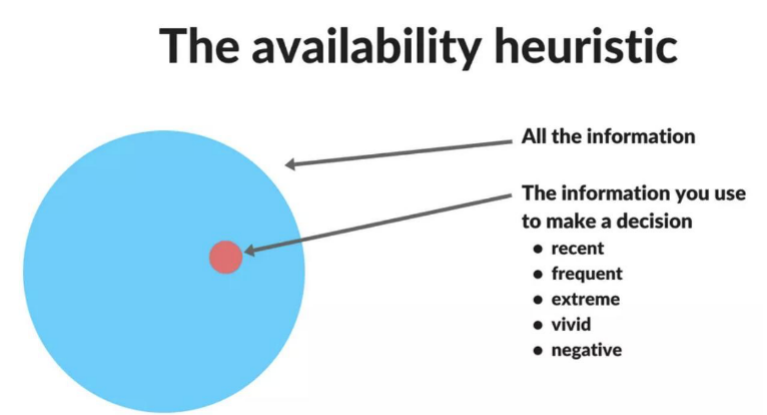
Heuristics examples
Availability heuristic — what kind of info used to make a decision?
recent
frequent
extreme
vivid
negative
Representativeness Heuristic
Our tendency to organize information based on similarity of that information to already established categories
can be useful to extent (sorting objects)
applied to people can be problematic
Representativeness Heuristic — example
Stereotyping
Can lead to prejudicial and discriminatory behavior
All have some risk for stereotyping
All benefit from experience, can affect thoughts, feelings and behaviors
If aware of a stereotype, can change behavior.
however, not always aware of the stereotypes
Implicit discrimination
Driven by associations of which individual is unaware (implicit associations)
Learned associations may influence unconscious processing and drive decision-making
One measure — implicit associations test (IAT)
many variations, critical is measurement of response time
implicit associations test — IAT
Subjects shown word or image — categorize it into one of two groups by hitting a key (“E” or “I”)
response time and keystroke logged
info comfortable with tends to be delivered quickly
differences in response time may reflect implicit associations (which could be biases)
Criticism of the IAT
Test-retest reliability concerns
Correlation to discriminatory behavior unclear
However, it has been argued that
weak effects become important on the societal level
IAT could be combined with other tests
Population scores change over time
Group biases
Biases emerge even if the groups involved are relatively new and based on arbitrary criteria
dot counting (Tajfel’s minimal group paradigm)
eye color (elliot’s original classroom study)
ingroup vs outgroup
.
Can be counteracted partially
Forced cooperation (e.g. Robber’s cave study)
Increased contact (e.g. Jigsaw Classrooms), provided proper context
Stereotype Threat
Stereotypes might not just affect judgment of others, but our own behavior
Stereotype threat fear of fulfilling a stereotype in a task negatively affects performance of that task
Meta-analysis suggest effect smaller than expected
Attributions
In theory, outcome of any event in a person’s life is due to the interaction of two factors: their traits and their environment
.
In dispositional attribution, outcome explained by trait
bad grades due to poor work ethic and low intelligence
.
In situational attribution, outcome explained by environment
bad grades because tragedy happened
Fundamental attribution error
When evaluating others, we consistently overestimate the role of dispositional factors
one of the most relevant and consistent findings in the field
Famous FAE experiment
Subjects randomly assigned to debate pro- and anti-Castro positions
Afterwards, each debater submitted a rating of other debater’s beliefs
Even though the participants knew speech assignment was random, they assumed the debaters agreed with the ideas that they presented
On FAE
Major reason for not including situational factors in evaluation of others is that we are unaware of them
Relavent to our view of world history: often fail to consider the unique situational factors that world leaders had at time of decision making
Bias may be lower in collectivist and greater in individualistic
Defensive Attributions
We particularly overemphasize dispositional factors when we succeed and overemphasize situational factors we fail (self-serving bias)
common in individualistic cultures (Western) where there is emphasis on achievements
self-serving biases might negatively affect performance (dont make right adjustments)
General criteria for a disorder
Statistical rarity
uncommon
.
Subjective distress
low quality of life, poor mental well-being
.
Impairment
cognition, emotional regulation, attention
.
Biological dysfunction
significant abnormalities in nervous system
.
Significant exceptions can exist, role of context
“Types” of Disorders
Cluster structure
Descriptive, not mechanistic
Not strongly supported
Man-made invention
Major perspectives on Disorders – 1
A disorder (e.g. schizophrenia) is an invented classification, may not perfectly capture everything
.
We group things (human categories), but our groups may not reflect those naturally exist (natural kinds)
.
Disorders are likely heterogenous
many subtypes, with variability in causes, features, outsomes, treatment responses, etc
Major perspectives on Disorders – 2
Disease model
something biological “causes” disorder, causing symptoms
single symptom can be a suitable measurement
severity of symptoms ~ severity of disorder
.
Useful but not perfect
symptoms variable in number, frequency, and intensity
“cause” unclear
Major perspectives on Disorders – 3
Network model
disorder is an interaction between symptoms
multiple symptoms must be studied
related: dynamical systems approach
.
New, needs refinement
data collection + analysis more complex
validity less clear
Misconceptions on Models
Diagnosis is categorizing people (pigeon-holing)
person does not lose individuality with diagnosis
.
Diagnoses are unreliable (experts never agree)
clinicians agree on many disorders, some are hard to diagnose
.
Diagnoses are invalid
diagnoses can predict outcomes
.
Diagnoses negatively impact a person’s life
in right context (supportive environment), diagnosis helps
Diagnosing Disorders
Requires interview assessment from professional using standardized, evidence-based guidelines
diagnostic criteria from the DSM could guide diagnosis
.
Biological tests may be done to exclude other problems (e.g. thyroid)
.
Biological tests do not usually inform diagnosis
neuroimaging (brain structure/function) not typically used
view of disorders as “brain disorders” is impractical
genetic testing rarely used, but family history can be
DSM-5 Features
~300+ disorders
Biopsychosocial approach
biological, psychological (thinking patterns), societal factors (culture)
DSM-5 Criticisms
Not all disorders meet validity criteria
Vagueness may lead to “pathologization” of normal behavior
Categorical (binary; either/or) rather than dimensional
Comorbidities (share root cause)
Concerns about lack of transparency, pace of preparation, conflicts of interest
Anxiety disorders
Generalized Anxiety Disorder (GAD)
Panic Disorder
Phobias
~4% of people may suffer (mostly phobias)
related but now independent: obsessive-compulsive disorder (OCD) and post-traumatic stress disorder (PTSD)
1 – GAD Generalized Anxiety Disorder
Exaggerated worry/tension in day-to-day situations
May later lead to emergence of other disorders (network model)
More common in females than males
2 – Panic Disorders
Characterized by recurrent episodes of intensive fear (w/sweating, dizziness, light headaches, breathing difficulty, heart irregularities)
while many report single panic attack, in disorder the attacks are repeated and unexpected
emerges eary in adulthood
3 – Phobias
Most common of all anxiety disorders
intense, irrational fear of specific thing
may be outgrowth of panic disorder
agoraphobia (fear of marketplaces or crowded environments)
4 – OCD
Obsessions are persistent thoughts that are unwanted and/or cause stress
centered topics: sex, contamination, aggression, religion
.
Compulsions are repetitive behaviours undertaken to reduce distress and relieve shame/guilt
washing hands
re-reading sentences
What causes anxiety? Learning/Behaviorist perspective
Classical conditioning mechanisms
CS/UCS —→ CS signals UCS —→ CS leads to CR
cars + accident, car signals accident, car causes fear
.
Operant conditioning mechanisms
If cars (S-) give anxiety, may avoid (R)
avoiding = less anxiety, motivated to continue avoiding (increase in R)
maintenance of fear through negative reinforcement
What causes anxiety? Other factors
Possible role of genetics — show some heritability
Rate of anxiety (& depression) rising — environment changes likely factor
Nature of envrionmental influence debated — digital tech, free play in childhood, occupation, relationships
What is depression?
Loss of interest or pleasure in activities normally enjoyed (e.g. anhedonia)
Decreased energy (e.g. fatigue)
Feelings of guilt or low self-worth
Disturbed sleep, appetite and activity
Inability to concentrate
Thoughts of suicide
Product of life
Global burden of depression
~5% of population 1, higher rates in young cohorts
Associated with lower quality of life, suicide, other poor outcomes, significant economic cost
Leading cause of disability worldwide
Good news: normally treatable (70 – 80% of cases)
Types of Depression
Unipolar depressive disorder
Major Depressive Disorder (MDD; chronic)
Major Depressive Episodes (MDE; acute but often recurrent)
Post-partum depression
Dysthymia
Seasonal affective disorder
.
Depressive episodes also occur in bipolar disorder, but is considered separately
Epidemiology of Depression
1. Gender
2. Community
3. Socioeconomic status
4. Occupation
5. Life history
Epid of Depression — 1 - gender
More common in women (~2x) though the severity does not differ
Reasons for disparity are complex
.
Multiple factors possible
Hormones (post partum)
Low in males due to stigma
High in females due to social pressures (family roles, unpaid labor, societal expectations)
Epid of Depression — 2 – Community
Burden of depression may be higher in Western, developed countries
.
Many potential reasons for this disparity (not exclusive):
more awareness, less stigma
better diagnostic criteria, health care access
beliefs about efficacy of emotional regulation
valuation of happiness in western cultures
description of disorder within the culture
Epid of Depression — 3 – SES
Low SES (i.e. low income) increases risk
In Eastern + Western communities, even with control for other variables
Main argument that low income leads to depression
relationship between income + well-being complex
Low income may be associated with increased risk for many reasons (e.g. lack of insurance, health care…)
.
Burden may be higher in developed countries with stronger economies, but risk is lower in people of higher SES
Epid of Depression — 4 – Occupation
If you don’t have a job, the risk is also higher (nearly x2)
Why does the risk vary by job?
Social interaction plays a role but it is complex
Difficult (service) and rare (trucking/transport) interactions both a issue
.
Stress level (high increases risk)
.
Physical activity (low increases risk)
.
Jobs offer varying degrees of validation (skills), feelings of meaning/status/acceptance, income and access to vital services
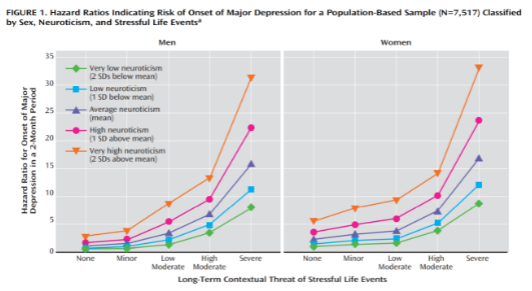
Epid of Depression — 5 – Life history
Risk for mental disorders increases with stress frequency
life events
Theoretical models
Behavioral models proposed by Lewinsohn
Low rate of reinforcement: try many things w/no success
Learned helplessness is a related concept (Seligman)
.
Interpersonal model proposed by Coyne
Look to others for assurance > others respond negatively (hostility + rejection) > increasing need for reassurance
.
Cognitive model popularized by Beck
Cognitive distortions affect ability to acknowledge reality or interpret it; best describes serious depression
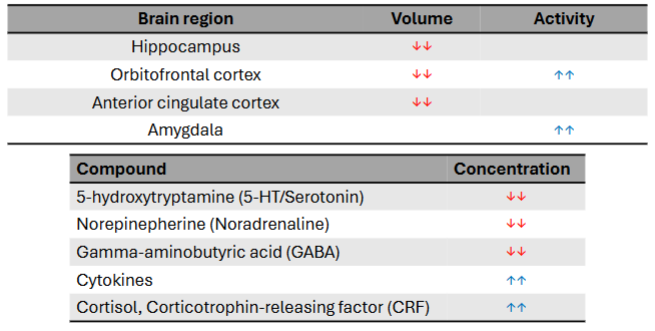
Biological Features of Depression
Hippocampus, orbitofrontal cortex, anterior cingulate cortex smaller
Substance Use Disorder (formerly addiction) — What is addiction?
Complex brain disease, there is compulsive engagement in behavior despite knowledge of harmful consequences
.
The term “brain disease” suggests considering the brain is critical
Matters for treatment, other competing perspectives exist (e.g. choice)
.
”Behavior” can mean many things (e.g. substance use, gambling, sex or video games)
.
“harmful” is itself a poorly defined term
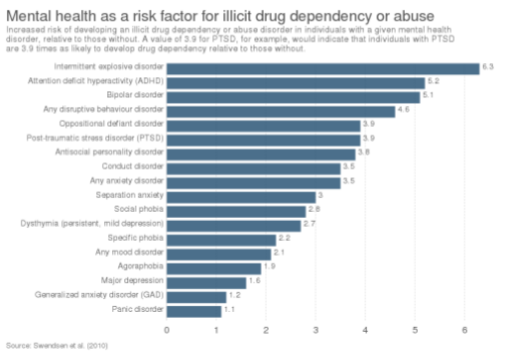
Risk factors for SUD
Stability of home environment
Early use + peer groups
Education
Employment
Genetics
Gender
Usage/dependence rates higher in men for many drugs, overdose rates higher in women for some drugs
Mental health status
Co-morbidities frequent
Comorbidities
Treating SUD
View of SUD as a “disease of the brain” or a “choice” has implications for treatment/quality of life
beliefs vary by country
.
Hybrid views favoured, extreme views not
radical version of choice: concern over aggressive policies, stigma
radical disease: concern treatments may be less effective
.
Prognosis good with treatment; majority recover
psychological and pharmacological treatments
Bipolar Disorder
Extreme swings in mood, including episodes of elevated mood (e.g. mania)
During periods of elevated mood, feels extremely energetic, happy and/or irritable
reduced need for sleep
reckless decision-making
Bipolar Disorder
~1% of the global population
One of the most costly disorders worldwide (top 10)
Risk of absenteeism, suicide and self-harm is high
Related to several other traits (particularly creativity), over-represented in certain populations (creative professionals/artists)
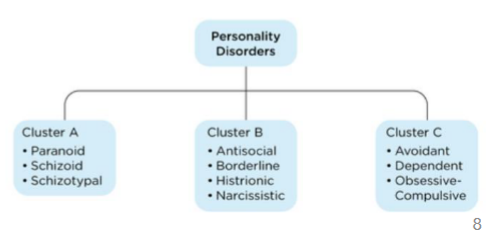
Personality disorders
Inflexible patterns of behavior — lead to distress
Emerge in adolescence, around same time as personality traits
Difficult to reliably diagnose; less researched than other conditions
Category includes borderline personality disorder, narcissistic personality disorder and anti-social personality disorder
Autism Spectrum Disorder — Symptoms
Poor social interaction
Fails to respond to name, poor eye contact, resists cuddling, prefers being alone
May not recognize/respond to social cues
.
Repetitive behaviors/Difficulty switching behaviors
Arranging objects, making sounds, hand flapping, head rolling and body rocking
Special interests
.
Slow language development
Starts later than age of 2 (may remain non-verbal), repetition of words/phrases (echolalia), abnormal tone/rhythm
Autism - Spectrum
Heterogeneous group of disorders, defined by a set of symptoms varying in severity
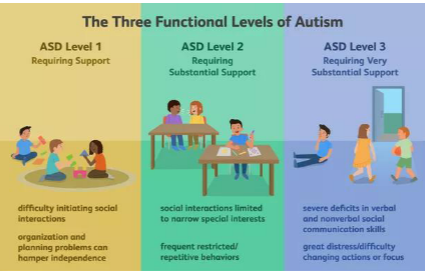
The Spectrum
Exceptional cognitive abilities are rare (~10%)
.
Strong genetic basis (twin studies: h2 = 0.6 to 0.7)
.
~1% population, more common in boys (~3:1)
could present differently by gender and be suppressed (masking)
higher genetic load may be required in women (female protective brain theory; controversial)
sex-specific pathways and hormones
Why are rates of ASD rising?
Increased awareness and more sensitive diagnosis
Inclusion of high-functioning cases
Increased parental age
Certain drugs (valproate), nutritional deficiencies, plastic exposure + more
What factor is NOT on this list?
Features of Schizophrenia
~0.5 – 1% of the population (similar worldwide)
.
Onset and severity differs by sex
Males ~18 years (earlier, worse outcomes)
Females ~30 years (later, better outcomes)
.
Associated with disrupted neurotransmission
Positive symptoms similar to effects of Dopaminergic drugs (e.g. amphetamine, L-DOPA)
symptoms reduced by drugs blocking DA (DA antagonists; typical antipsychotic drugs such as haloperidol)
Major risk factors for SZ
Prenatal + postnatal factors; “choices” (e.g. drugs) + “accidents” (e.g. illness)
Strong genetic basis (h2 = 0.6 to 0.7)
from birth
Most people imagine Psychological therapies as…
…a single authority figure, usually with significant credentials (e.g. M.D.)
…a single patient with a single problem
…a highly structured interaction with many questions, usually about the person’s past difficult experiences
…emphasis on increased awareness
…a “relaxed setting”
Types of therapists
Professional — individual with specific, intensive training and certification from recognized institution
• Clinical psychologists and psychiatrists are a good example
• Broad expertise, awareness of the complex ethical/legal/personal issues
.
Paraprofessionals — agency-specific qualifications specific to certain needs
• Pastoral counsellors
• Cannot formally diagnose or prescribe drugs
• Fill a key gap when other professionals are inaccessible
Types of therapists
Many different types of therapists, with many different strategies for different situations
The therapist is critical
“Good therapists” are viewed as warm, respectful, caring, engaged, empathetic and authentic
Ability to instill hope/positivity is another valued trait
No clear relationship between experience + outcomes
Trait matching with therapist (female-female, ethnicity-ethnicity) is often preferred, but benefits are unclear
Insight therapies
Focus on understanding how a person’s thoughts, beliefs, actions and prior history influence their current behavior
1 – Psychoanalytic therapies
Abnormal behaviors in mental health disorders may stem from early and/or traumatic experiences
.
Emphasis on unconscious and analysis of:
repressed thoughts/feelings
wishes/fantasies
recurring themes and patterns
therapeutic interaction
.
Belief that insight into unconscious is required for meaningful changes
bring unconscious processing into conscious awareness
Procedures in psychoanalysis
Free association and Interpretation
first thing that comes to mind
may be meaningful, propose explanations
.
Dream analysis
may represent subconscious desires that contribute to current mental state
wish fulfilment theory of dreaming
.
Debate over role of insight in therapy efficacy
2 – Humanistic Therapies
Related to perspectives of Rogers and Maslow
Often called client-centered (older term) or person-centered (newer term)
Emphasis on insight, positivity + self-actualization through choice (free will)
Therapist should be authentic, unconditionally positive and empathic (three critically important traits)
Less structured (client decides how time is spent)