Breast Cancer
1/34
Earn XP
Description and Tags
A set of 35 vocabulary-style flashcards covering the pathology, risk factors, screening, molecular subgroups, and treatment modalities for breast cancer based on the lecture notes.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
35 Terms
Invasive ductal carcinoma (IDC)
The most common type of invasive breast cancer, accounting for about 70–80% of cases, which spreads through the ducts to other parts of the breast.
3 pathology types
Invasive ductal carcinoma (IDC)
Invasive lobular carcinoma (ILC)
Ductal and lobular carcinoma in situ (DCIS/LCIS)
Invasive lobular carcinoma (ILC)
A type of invasive breast cancer that spreads through the lobules to other parts of the breast and accounts for approximately 10% of cases.
DCIS and LCIS
Non-invasive forms of breast cancer, officially Ductal and lobular carcinoma in situ, which are limited to the ducts or lobules and have not spread to surrounding tissue.
Masterectomy is crative in >95% of patients
Developed countries incidence
Breast cancer rates that are around 3–5× higher than in developing countries, with the UK having approximately 94/100k cases compared to India's 26.6/100k.
NHS screening interval
The frequency and age range for invitations to mammograms, occurring every 3 years from age 50 up to 71.
Symptoms
New lump or thickening in breast or underarm should be evaluated
Swollen lymph glands in the armpit can rearely indicate breast cancer (often related to infections)
changes in breast appearance (size, shape, feel)
nipple discharge - fluid leaking from non-pregnant or breastfeeding woman
nipple changes - any changes in position or appearance should be noted
Risk factors
Age: women over 50
Family history
lifestyle (alcohol, diet, physical activity)
environmental (radiation and chemical exposure)
Role of hormones
Imbalances: imbalances such as menopause and infertility can increase risk
menstrual cycle: women who start menstruating early or have late menopause onset, or have never given birth can increase factor
use of HRT after menopause can increase risk
oral contraceptives can increase risk
male breast cancer
~1% of all breast cancers
presents later due to low symptom awareness
risk factors:
age
klinefelter syndrome
testicular disorders
obesity
family history &. BRCA2 mutations
radiation
most are ER-positive ductal carcinomas
treated similarly to post-menopausal female breast cancer
Sporadic breast cancer
most common form of BC, arises by chance without family history and wiwthout BRCA1/2 mutation
hormone exposure is major risk factor
hormone exposure exposure increases the number of target cells by stimulating breast growth
by driving proliferation, hormones also place cells at risk for DNA mutations
metabolites of oestrogen can also directly cause mutations or generate DNA-damaging free radicals
Familial breast cancer
about 5-10% of breast cancers are hereditatry due to mutations
BRCA1&2 responsible for 80-90% of these,also rasing risk for ovarian, prostate and pancreatic cancers
BRCA1&2 mutations are present in ~1 in 400 of general population
BC screening
NHS invites mammograms overy 3 years from age 50-71, over 71 may self refer
Screening results
Either mammography (M) or ultrasound (U).
M1/U1 - normal breast tissue
M2/U2 - benign (not cancer)
M3/U3 - abnormal or uncertain but prob benign
M4/U4 - suspicious and possibly cancer
M5/U5 - cancer
Aspiration Cytology (FNA)
A diagnostic method using a needle to sample cells from a suspicious area, such as enlarged lymph nodes, which is less invasive than surgical or core biopsies. Aided by imaging. C1 - C5
Needle core biopsy
The diagnostic gold standard for most suspicious breast lesions, enabling full histological assessment, tumor grading, and biomarker status.
Low complciaction risk
Higher diagnostic sensitivity than FNA
Surgical biopsy (lumectomy)
Removal of a larger sample of breast tissue through surgery
General anesthesia used to minimize discomfort
Increased accuracy of diagnosis
Invasive procedure
Potential for discomfort, pain, and scarring
Need for recovery time and follow-up care
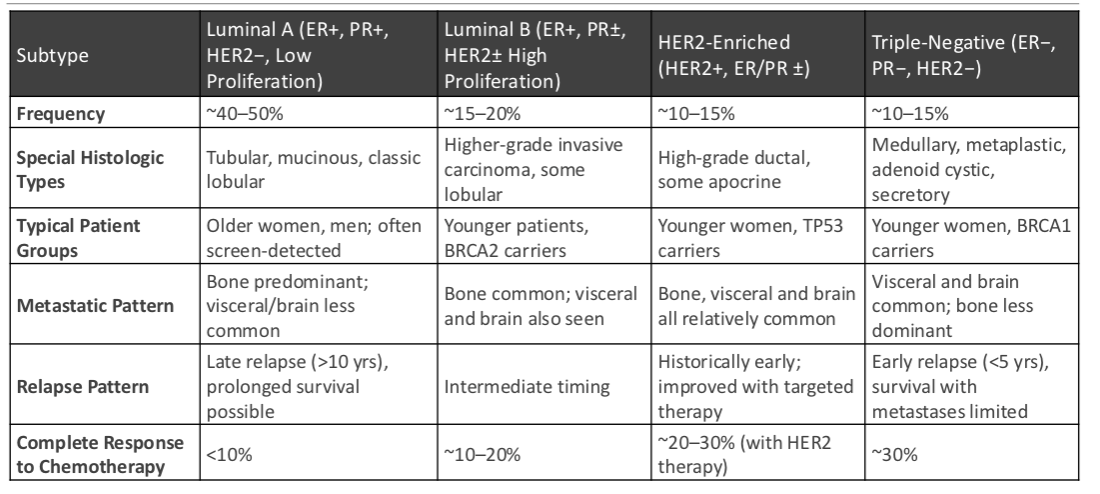
Molecular subgroups
Most breast malignancies are adenocarcinomas (>95%). 3 major bologic subgroups with different responses and outcomes
Hormone Receptor Pos/ HER2-neg (luminal) - ~70% cases
Luminal A
Luminal B
HER2 enriched - ~15% cases
Basal like/ triple neg breast cancer (TNBC) - ~ 10-15% cases
Luminal A
A hormone receptor-positive molecular subgroup characterized by slow growth, strong positive hormone status, and a better prognosis, representing 50–60% of luminal cases. Less agressive
Luminal B
A hormone receptor-positive subgroup (~10% of luminal cases) that has a faster growth rate and more aggressive behavior compared to Luminal A. poorer prognosis, lower expression of hormone receptors
Biomarkers and targeted therapies
ER/ PR positive → CDK4/6 inhibitors
HER2 over expression → IHC 2+ (confirm with FISH)
Ki-67 proliferation index → measures % of cycling tumor cells
PD-L1 expression (TNBC) → identifies candidated for immunotherapy
Nottingham Histologic Score
A grading system used for breast cancer that evaluates tubule formation, nuclear pleomorphism, and mitotic count.
Prognostic factors include tumor stage (TNM score) and the underlying biology
the five stages 0 - IV are highly correlated with survival
OSNA
One Step Nucleic Acid Amplification; a molecular detection method used intra-operatively to analyze entire lymph nodes for metastases.
Detects cytokeratin 19 (CK19) mRNA exression, an epithelial cell marker not normally present in lymph node tissue
high sensitivity
Cytokeratin 19 (CK19)
An epithelial cell marker mRNA analyzed by OSNA, which is normally absent in lymph node tissue and indicates the presence of metastatic cells.
ctDNA (Liquid biopsy)
The analysis of circulating tumour DNA from a blood sample used for non-invasive genetic profiling and early prediction of relapse.
can monitor treatment response and emerging resistance mutations
emerging clinical tool- promising but not yet routine
Treatment of localised breast cancer (stage I, II, operable stage III)
Surgery
Radiotherapy
Adjuvant chemotherapy - consider if high grade, HER2-pos or large tumor
HER2- targeted therapy: trastuzumab (Herceptin), given with/ after chemotherapy for ~1 year
Endocrine therapy (ER/PR) - tamoxifen or aromatase inhibitors, started after chemotherapy
Neoadjuvant chemotherapy - for large or advanced tumors to downstage before surgery
PD-L1 expression
A biomarker used in Triple-Negative Breast Cancer to identify patients who candidates for immunotherapy such as Pembrolizumab.
Ki-67 proliferation index
A measurement of the percentage of cycling tumour cells within a sample used to determine the rate of tumor proliferation.
Stage IV (Metastatic) Survival
A stage of invasive carcinoma with distant metastasis present, yielding a 10-year survival rate of 5–2500.
HER2 confirmatory testing (IHC 2+)
A diagnostic protocol where cases with an IHC score of 2+ must be further confirmed using FISH (fluorescence in situ hybridization) for gene amplification.
ER positive genomic pathways
Characterized by alterations such as 1q gain, 16q loss, and mutations in the PIK3CA gene.
treatment of inoperable/ metastatic cancer
First-line endocrine therapy - for luminal A disease without major organ compromise
Fisrst line chemotherapy - anthracycline based regimens for luminal B when liver/ling is present
HER2-targeted therapy - trastuzumab, usually combines with chemotherapy
Surgery (palliative) - for complications such as ulcerating breast masses, spinal cors compression or lung metastases
radiotherapy (palliative) - effective for bone pain, primary tumor symptoms or brian metastases
Bone-modifying agents: bisphosphonates
Overall goal: systemic disease control, prolong survival and optimise QoL rather than cure
AI-assisted mammography
A decision-support tool that highlights subtle abnormalities like microcalcifications and small masses to improve cancer detection and screening efficiency.
AI tools help with automated mitotc counting, tumor grading and subtype prediction
decision support tool only, augments but does not replace clinician judgement
Secondary high-risk genes
Mutations in genes such as CHEK2, TP53, PTEN, and LKB1/STK11 that account for less than 10% of hereditary breast cancers.
summary