GI system positioning / tipping
1/130
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
131 Terms
The specific five elements that must be permanently documented in the patient's chart following any fluoroscopic procedure
Route of contrast
Time of administration
Amount of contrast
Type of contrast
Total fluoro time
What are the 2 breathing exercises used in fluro?
Valsalva maneuver
Modified valsalva maneuver
The specific healthcare professional responsible for ensuring that an inpatient has strictly complied with all pre-examination preparation orders
Nursing Staff
The direct method by which a radiographer verifies pre-examination preparation compliance for an outpatient
Asking the patient directly as a core part of taking their history
The dynamic imaging tools obtained prior to contrast administration specifically to evaluate the effectiveness of the patient's bowel preparation
Scout Radiographs
An inert, water-insoluble positive contrast medium that does not dissolve in water but instead mixes with it to form a suspension
Barium Sulfate
The thickest physical form of barium sulfate, specifically utilized during specialized swallowing evaluation studies
Paste Form
Water-soluble iodinated compound solutions such as Gastrografin or Oral Hypaque used when standard barium is strictly contraindicated
Iodinated Media
The four distinct clinical scenarios where standard barium sulfate is strictly contraindicated and water-soluble iodinated contrast must be used instead
Impending abdominal surgery
Suspected perforation
High risk of barium impaction
Neonatal patients
The two primary clinical risks or body complications associated with administering water-soluble iodinated contrast media to a patient
Severe dehydration and Aspiration complications
The specific anatomical or structural abnormality during an esophageal examination where water-soluble iodinated contrast is explicitly contraindicated
Suspected Fistula
Malignant tumor arising from the lining of the esophagus
Carcinoma of esophagus
A negative contrast agent that increases the visibility of the mucosal lining by increasing image density in double-contrast studies
Air Contrast
An injected intravenous drug used to relax the GI tract, slow down peristalsis, and effectively reduce patient abdominal cramping during an exam
Glucagon
The involuntary contraction waves by which the digestive tube propels its internal contents toward the rectum
Peristalsis
The average number of peristaltic contraction waves that naturally occur per minute within a completely filled stomach
Three to Four Waves
The average physiological emptying time required for a standard, healthy adult stomach to completely clear
2 to 3 Hours
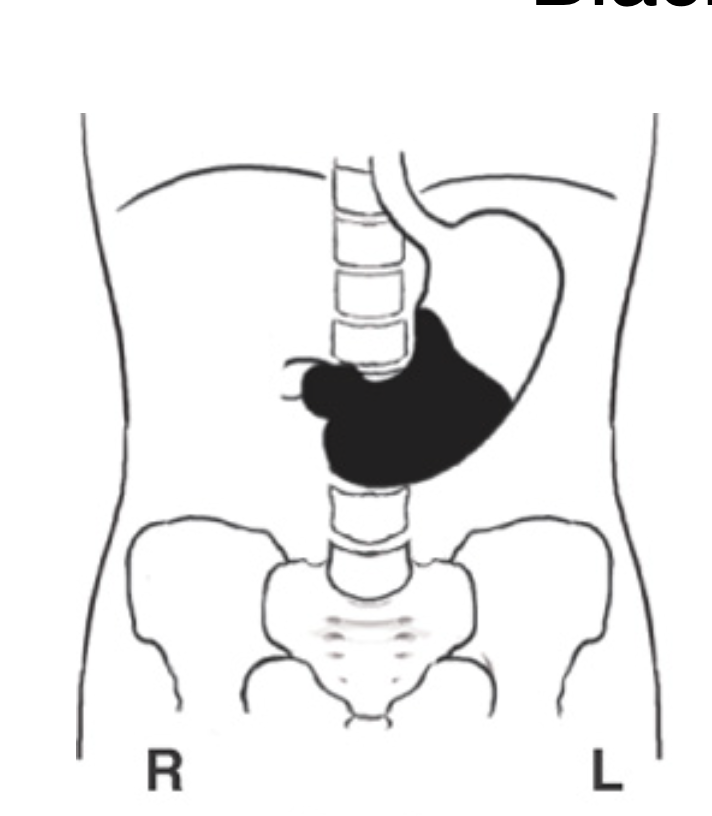
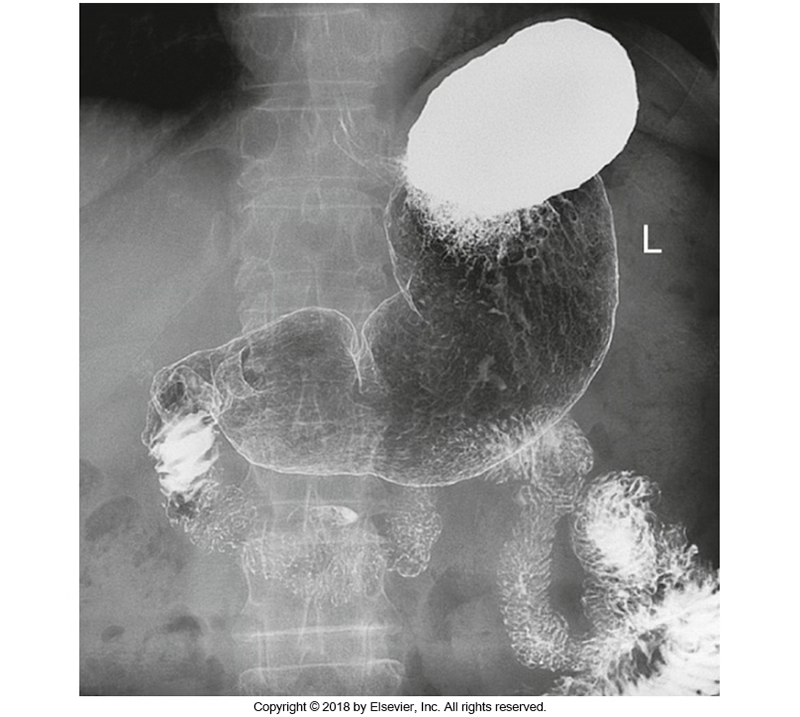
What patient position is this?
Supine
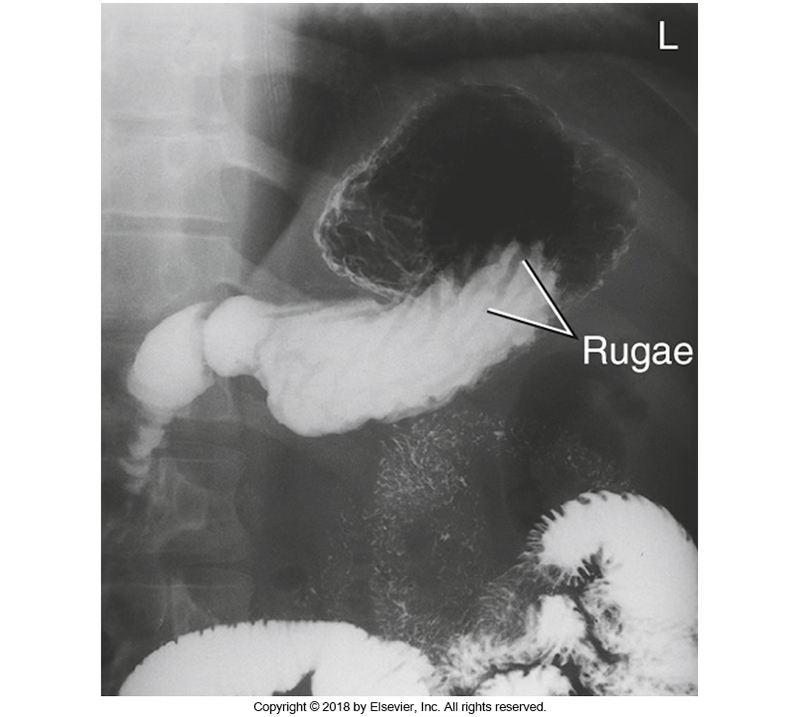
3 structures shown for a PA oblique RAO stomach
Entire stomach
Duodenal loop
Pyloric canal
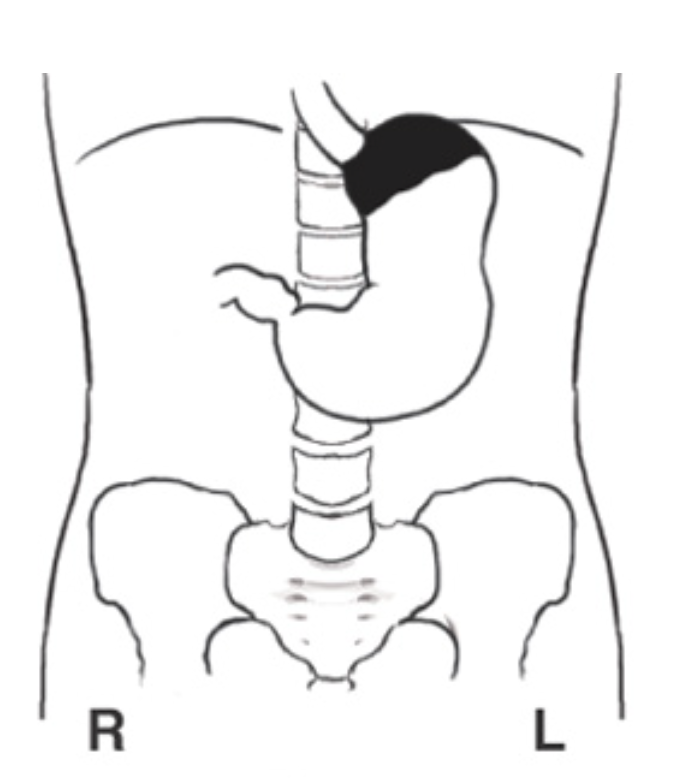
What patient position is this?
Prone
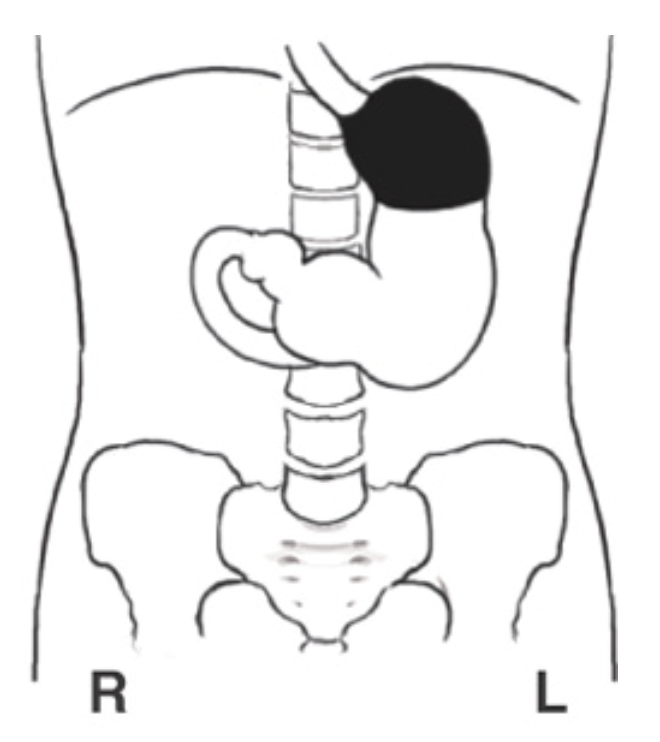
What patient position is this?
Erect
Average transit time to ileocecal valve is
2 to 3 Hours
The four miscellaneous supplies that should always be proactively gathered in the room specifically for an Esophagogram or Upper GI series
Washcloth
Straw
Barium pill (or substitute)
Bucky slot shield
The specific action a radiographer must take regarding the fluoroscopy table and Bucky tray layout during preliminary room setup
Bring the radiographic table to a fully vertical position and ensure the Bucky tray is moved completely out of the way
The fundamental clinical rule regarding gonadal shielding during digestive system radiographic imaging
Shielding should be used on all children and adults of reproductive age whenever smaller IR are used- or per site protocol
The two alternative medical names used interchangeably within clinical facilities for a Modified Barium Swallow Study
Swallowing Dysfunction Study or Videofluoroscopic Swallow Study (VFSS)
The specific clinical team required to be physically present to conduct a diagnostic Modified Barium Swallow Study
Speech therapist, Radiologic technologist, and Radiologist
The proper patient and part positioning for a lateral view MBSS
Seated or standing in a true lateral position with shoulders depressed and the midcoronal plane perpendicular to the image receptor
The required collimation radiation field boundaries for a diagnostic lateral view MBSS
From the level of the external acoustic meatus (EAM) down to the jugular notch
The specific anatomical structures that must be clearly shown on a diagnostic lateral view MBSS image
Contrast-filled mouth, pharynx, and cervical esophagus
The CR for AP projection MBSS
At the level or just below the laryngeal prominence
The main diagnostic purpose of obtaining an AP view during an MBSS evaluation
Demonstrating unilateral structural or functional abnormalities
The preliminary patient preparation or dietary restriction required before starting a standard esophagogram
No Prep Required
The standard weight-to-volume percentage of low-density barium used during a single-contrast esophagogram
60% Weight/Volume
The standard weight-to-volume percentage of high-density barium used in conjunction with carbon dioxide crystals for a double-contrast esophagogram
210% to 250% Weight/Volume
CR and IR size for an AP or PA projection of the esophagus
MSP at T5-T6 using a 14x17 or 7x17
The patient position, body rotation, and CR for an RAO esophagus projection
Rotated 35 to 40 degrees with CR entering 2 inches lateral to the MSP at level of T5-T6
The key anatomical placement criterion for a diagnostic RAO esophagus projection
Esophagus filled with barium between the vertebrae and the heart
The precise CR and patient positioning for a lateral esophagus projection
CR perpendicular to MCP at level of T5-T6 with the patient in a right or left lateral position and arms moved forward away from the body
The four diagnostic testing methods or maneuvers used during fluoroscopy to actively detect esophageal reflux
Breathing exercises (Valsalva)
Water test
Compression technique
Toe-touch maneuver
The maneuver where a patient takes a deep breath and bears down as if trying to move the bowels to induce reflux
Valsalva Maneuver
The maneuver performed by having the patient close their mouth, pinch their nose closed, and try to blow out against the resistance
Modified Valsalva Maneuver
The diagnostic reflux test performed with the patient in a slight LPO position swallowing water to observe the esophagogastric junction under fluoroscopy
Water Test
The reflux detection method where an inflated paddle is placed under the stomach with the patient in a prone position to apply localized pressure
Compression Technique
A dual-purpose maneuver that is highly effective for radiographically demonstrating both gastric reflux and a hiatal hernia
Toe-Touch Test
A diagnostic evaluation of the distal esophagus, stomach, and small intestine using ingested contrast media
Gastrointestinal Series (GI Series / UGI)
The strict pre-examination dietary instructions required of a patient prior to an Upper GI series
NPO after midnight or for at least 8 hours before the exam
The two common habits that are strictly restricted prior to an Upper GI series because they stimulate unwanted gastric secretions
Smoking and chewing gum
An evaluation that combines both single-contrast and double-contrast methods during the exact same Upper GI procedure
Biphasic Examination
The proper patient positioning, CR, and breathing instructions for an AP scout image of an Upper GI
Supine or prone, centered to MSP 3 inches above the iliac crest, on expiration
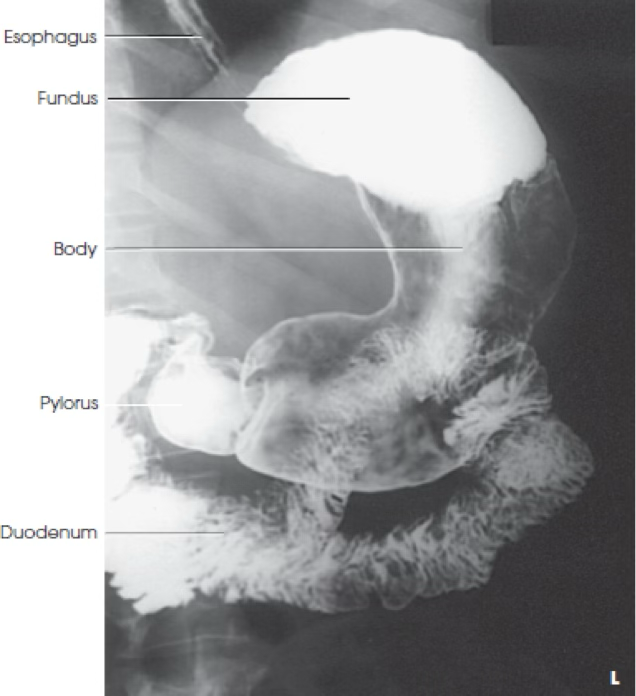
The specific anatomical areas demonstrated on a diagnostic PA projection of the stomach
Barium-filled stomach and duodenal loop, detailing size, shape, and position
The specific anatomical areas demonstrated on a diagnostic AP projection of the stomach
Contrast-filled fundus, delineation of the body/pylorus/duodenum, retrogastric portion of the duodenum/jejunum, and diaphragmatic herniations
The body rotation range and CR for a PA oblique RAO stomach
Rotated 40 to 70 degrees with CR at level of L1-L2
The precise part alignment and body rotation details for an AP oblique LPO stomach projection
Recumbent LPO rotated 40 to 70 degrees (average 45) , centered between xiphoid process and lower rib margin
In a lateral stomach, the right retrogastric space shown in _______
Recumbent right lateral
In a lateral stomach, the left retrogastric space shown in _______
upright left lateral
The specific anatomical regions highlighted on an AP oblique LPO stomach projection
Fundic portion of the stomach, duodenal bulb, and C-loop
The required central ray centering level for a right lateral stomach projection in both recumbent and upright positions
Centered at L1-L2 for recumbent position, L3 for upright position
The three administration routes used to introduce contrast media into the small intestine
Orally
Reflux filling via a large-volume barium enema
Direct injection via a tube (Enteroclysis)
The most common clinical method utilized to perform a standard small bowel series
Oral Method
The strict dietary and mechanical prep required before a small bowel series
NPO after the evening meal, a low-residue diet for 1 to 2 days prior, a cleansing enema, and emptying the bladder immediately before the exam
The exact image receptor centering adjustments required for a timed small bowel series based on the time interval
Centered 3 inches above the iliac crest for the 30-minute interval image, and centered directly at the iliac crest for all subsequent delayed images
The technical definition and visual marker that signifies the completion of a small bowel series
Opaque contrast reaches the ileocecal valve and visualizes progressive filling of the cecum
The maximum temperature to which a barium enema mixture may be warmed to prevent thermal injury to the bowel mucosa
Body Temperature (never warm above this)
The primary and most crucial patient preparation requirement before performing a retrograde barium enema examination
The colon must be exceptionally clean and entirely free of residual fecal material
A full dietary and mechanical bowel preparation regimen required of an outpatient the days leading up to a barium enema
Low-residue diet and increased fluids for 2-3 days, clear liquids for 24 hours, a cathartic the afternoon before, NPO for 8 hours minimum, and a cleansing enema the morning of the exam
The maximum fluid volume capacity of a standard disposable barium enema bag
3 Quarts (3000 mL)
The crucial radiation safety rule regarding the inflation of a retention catheter balloon tip during a barium enema
The balloon must be inflated using fluoroscopy just before the exam, limited to one complete squeeze of the inflator (approx. 90 mL)
The immediate dual-step action a radiographer must take after all barium enema radiographs have been successfully acquired
Deflate the retention balloon completely first, then carefully remove the enema tip
The precise central ray alignment, image receptor placement, and air-contrast orientation for a lateral decubitus large intestine projection
Horizontal central ray perpendicular to a 14 x 17 inch IR centered to the level of the iliac crests with the side of interest positioned "up"
The specific colon walls demonstrated on a right lateral decubitus position of the large intestine
Medial side of the ascending colon and the lateral side of the descending colon
The specific colon walls demonstrated on a left lateral decubitus position of the large intestine
Lateral side of the ascending colon and the medial side of the descending colon
The body rotation angle and central ray entry point for AP/PA oblique projections of the large intestine
Rotated 35 to 45 degrees, CR centered 2 inches lateral to MSP at level of elevated iliac crest
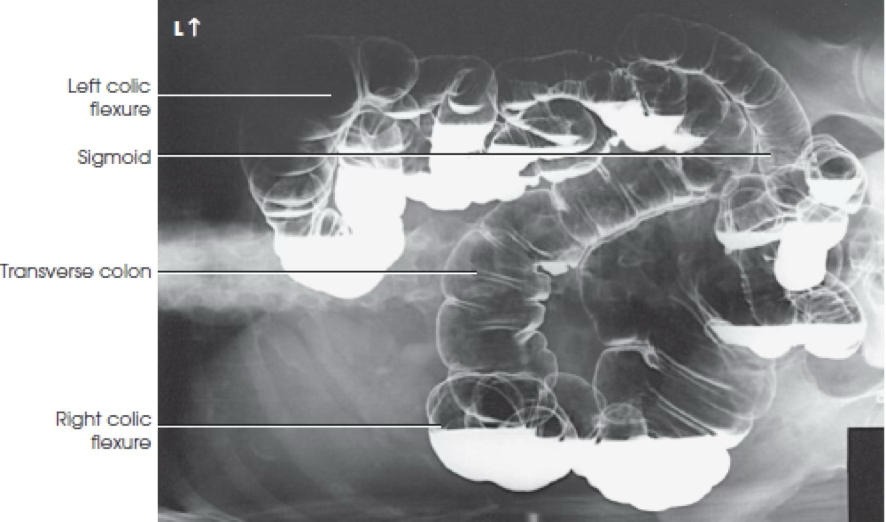
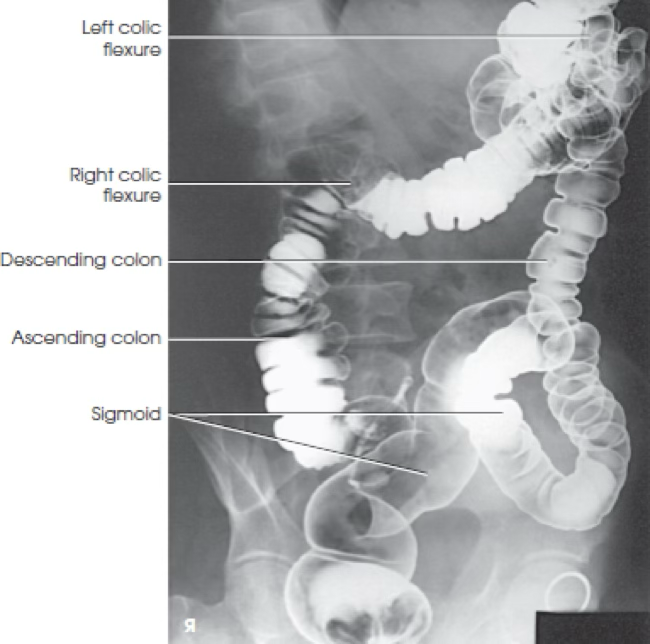
The 5 specific colon anatomy and flexure demonstrated by the LPO/RAO oblique large intestine projections
Entire colon
Right colic flexure (hepatic flexure)
Ascending colon
Cecum
Sigmoid colon
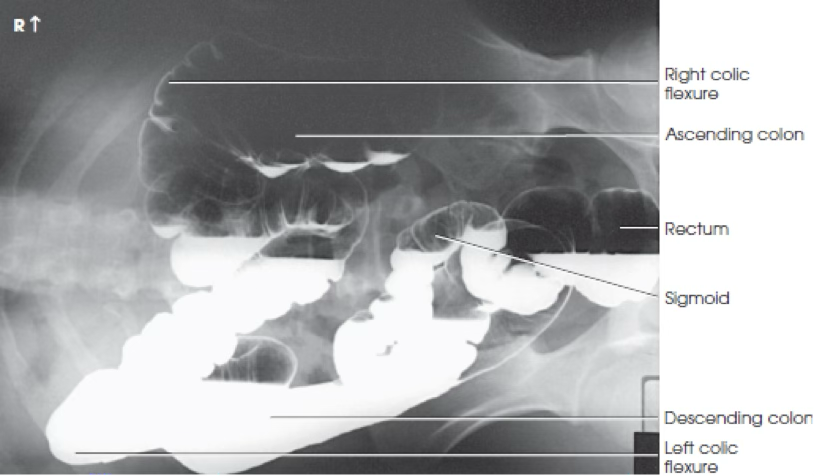
The 3 specific colon anatomy and flexure demonstrated by the RPO/LAO oblique large intestine projections
Entire colon
Left colic flexure (splenic flexure)
Descending colon
The CR angling required to clearly demonstrate the axial rectosigmoid area
Angled 30 to 40 degrees cephalad when the patient is supine, angled 30 to 40 degrees caudal when the patient is prone, at MSP on level of ASIS
The proper patient positioning and CR for a lateral rectum radiograph
Left lateral recumbent position, central ray entering 1 inch below the ASIS
A specialized radiographic exam where barium is carefully administered through a patient's stoma using a cone-shaped tip or small catheter to evaluate healing or new lesions
Colostomy Study (Loopogram)
A fluoroscopic study of the anus and rectum performed during the rest, strain, and evacuation phases of defecation
Defecography
The specialized patient preparation and high-density contrast media rules required for a defecography procedure
No advance bowel preparation required; uses a very high-density barium sulfate mixture sometimes mixed with potato starch
The five key discharge instructions that must be explained to a patient following any diagnostic barium GI study
Explain that stools will be white
drink lots of fluids
increase dietary fiber
take a mild laxative
Notify a physician if no bowel movement occurs within 24 hours to 3 days
The general respiratory instruction rule applied to all digestive system radiographs, with one specific procedural exception
All radiographs are taken on complete expiration, except for the RAO esophagus
What position was this patient in?
Prone (PA)
Which position was this patient in?
Supine (AP)

What view is this?
AP MBS
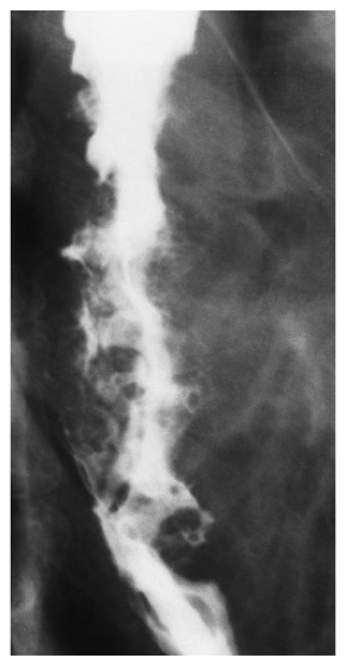
What is this?
Carcinoma of esophagus
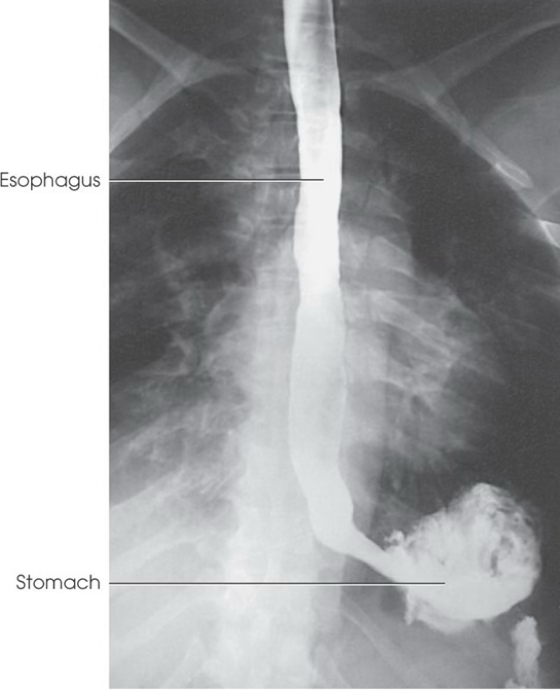
What is this?
AP/PA esophagus
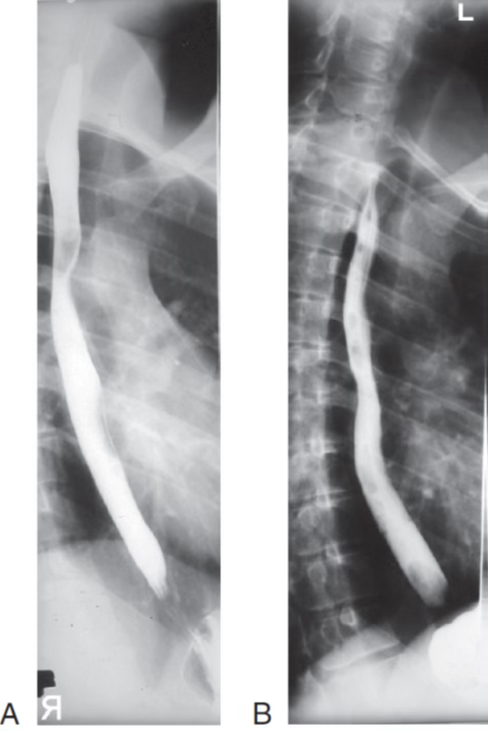
What is this?
Oblique esophagus

What is this?
Lateral esophagus
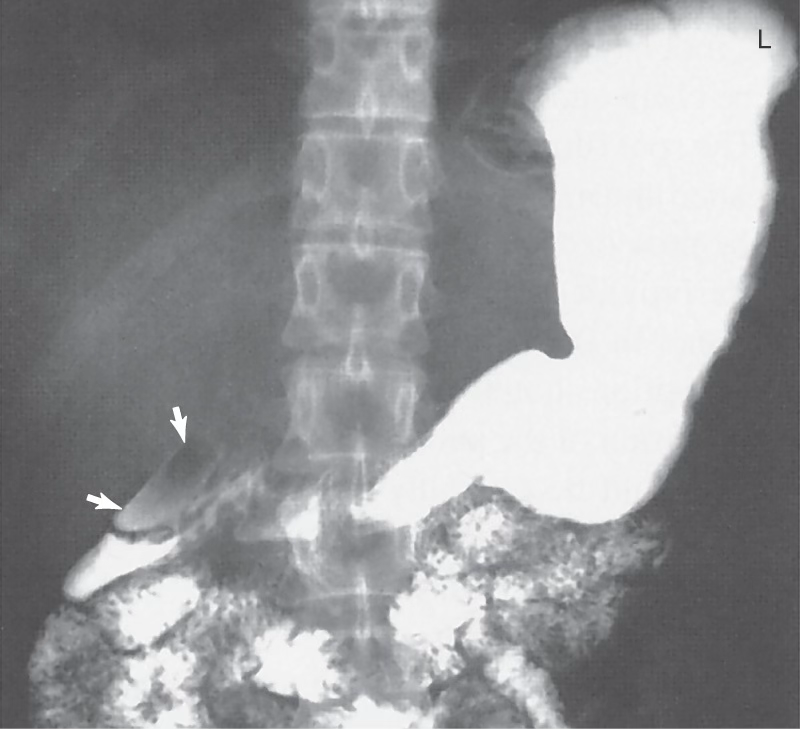
What is this?
Diverticulum in duodenum
What view is this?
PA Stomach

What view is this?
AP Stomach

What view is this?
PA Oblique RAO stomach
What view is this?
AP Oblique LPO stomach

What view is this?
Lateral stomach

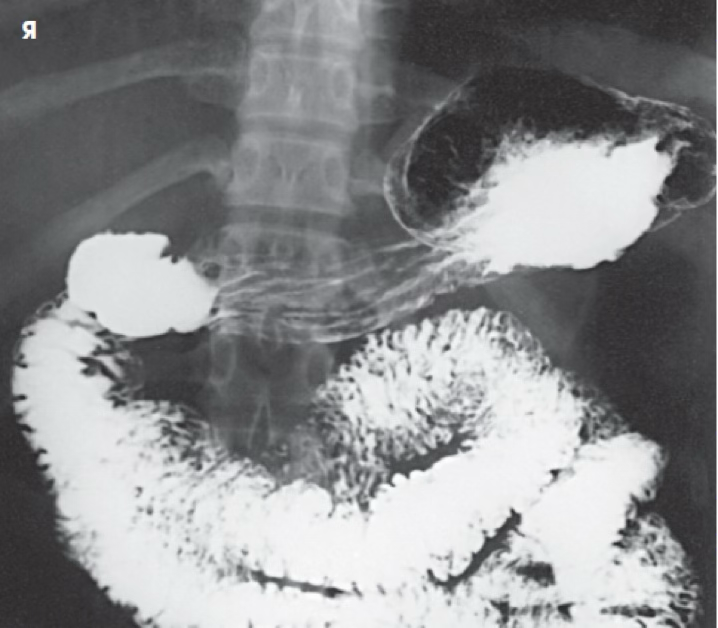
What view is this
AP/PA small bowel
What view is this?
Right lateral decub large intestine
When doing stomach exams, is it more common to do left lateral or right laterals?
Right lateral
What is this?
Left lateral decub large intestine
What view is this? Is patient in RAO or LAO?
PA oblique RAO large intestine