ERGs and Hereditary Disease - Neurophysiology and Perception Spring 2026
1/95
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
96 Terms
yes
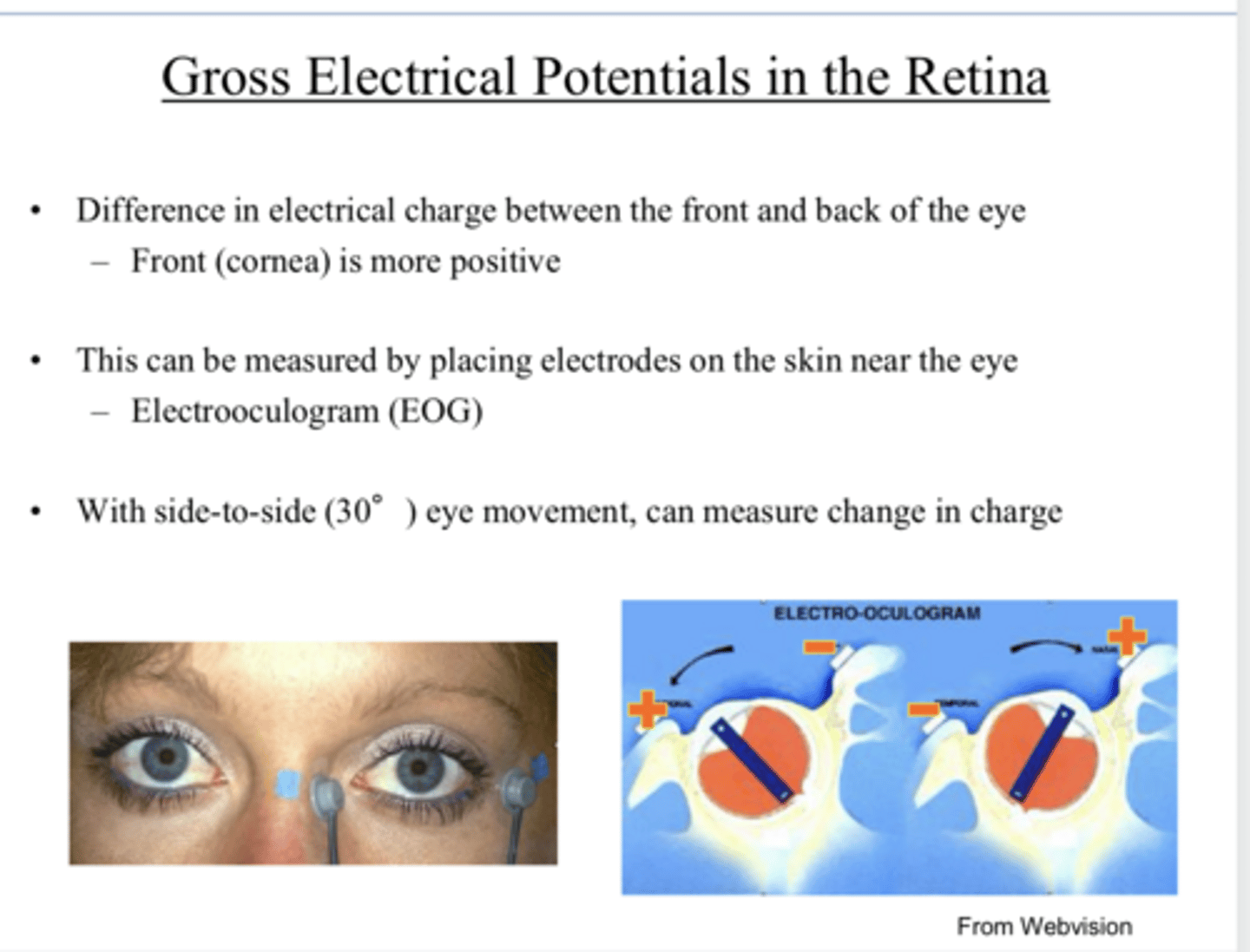
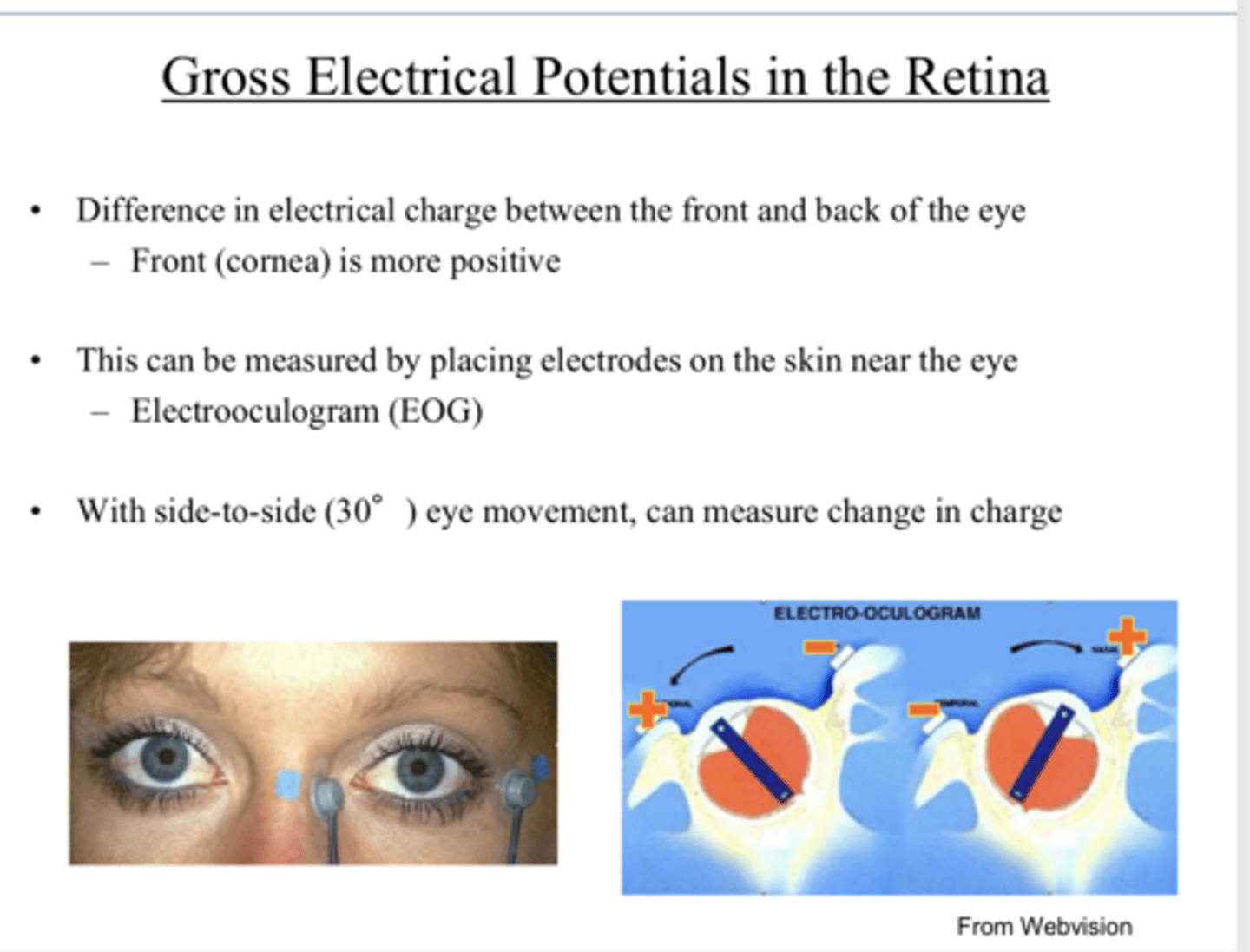
Is there a difference in electrical charge between the front and the back of the eye?
frnt
The (front/back) of the eye is more positive
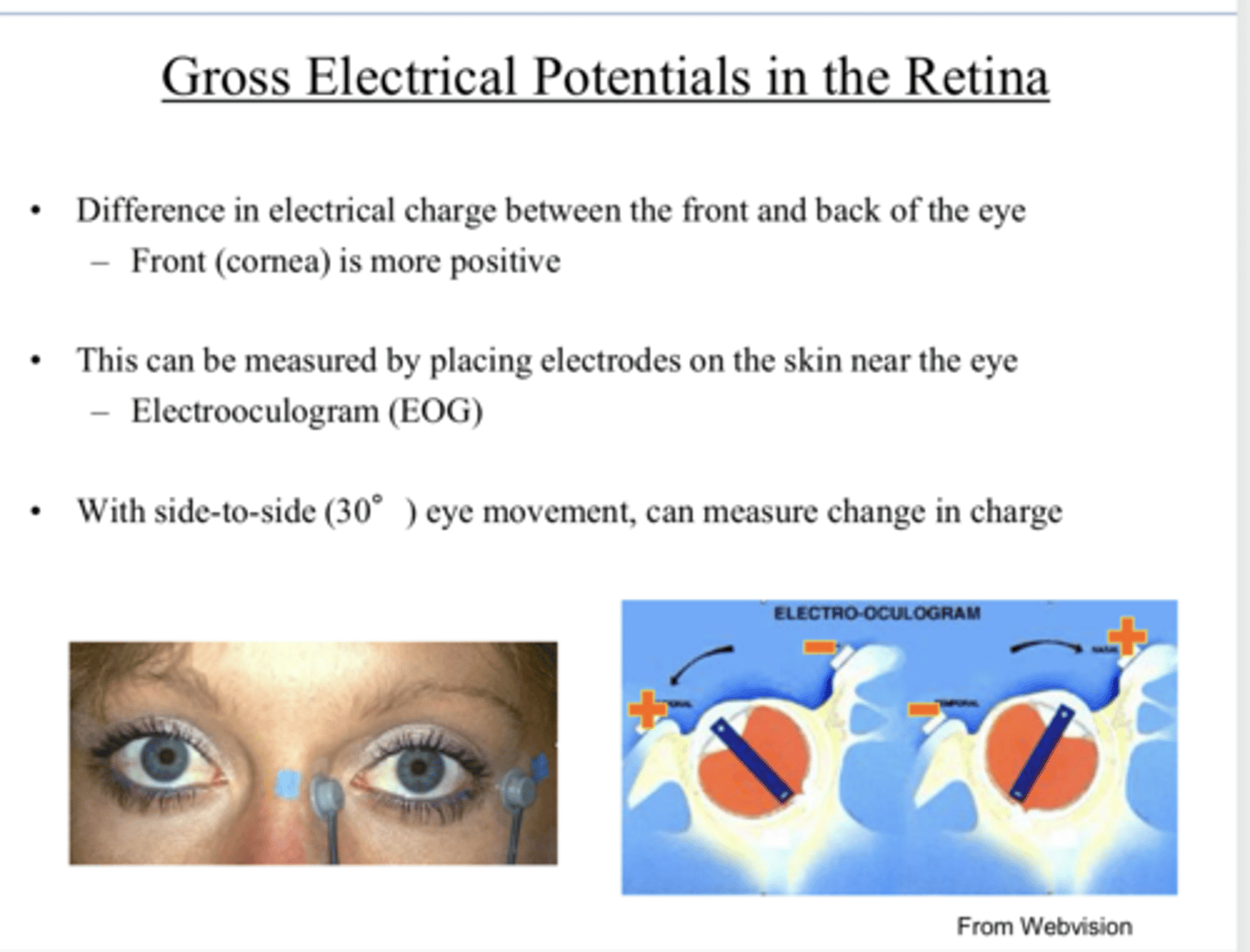
-By placing electrode on the skin near the eye (EOG)
-With side to side movement, you can measure changes in charge
How can electrical potentials of the retina be measured?
decrease
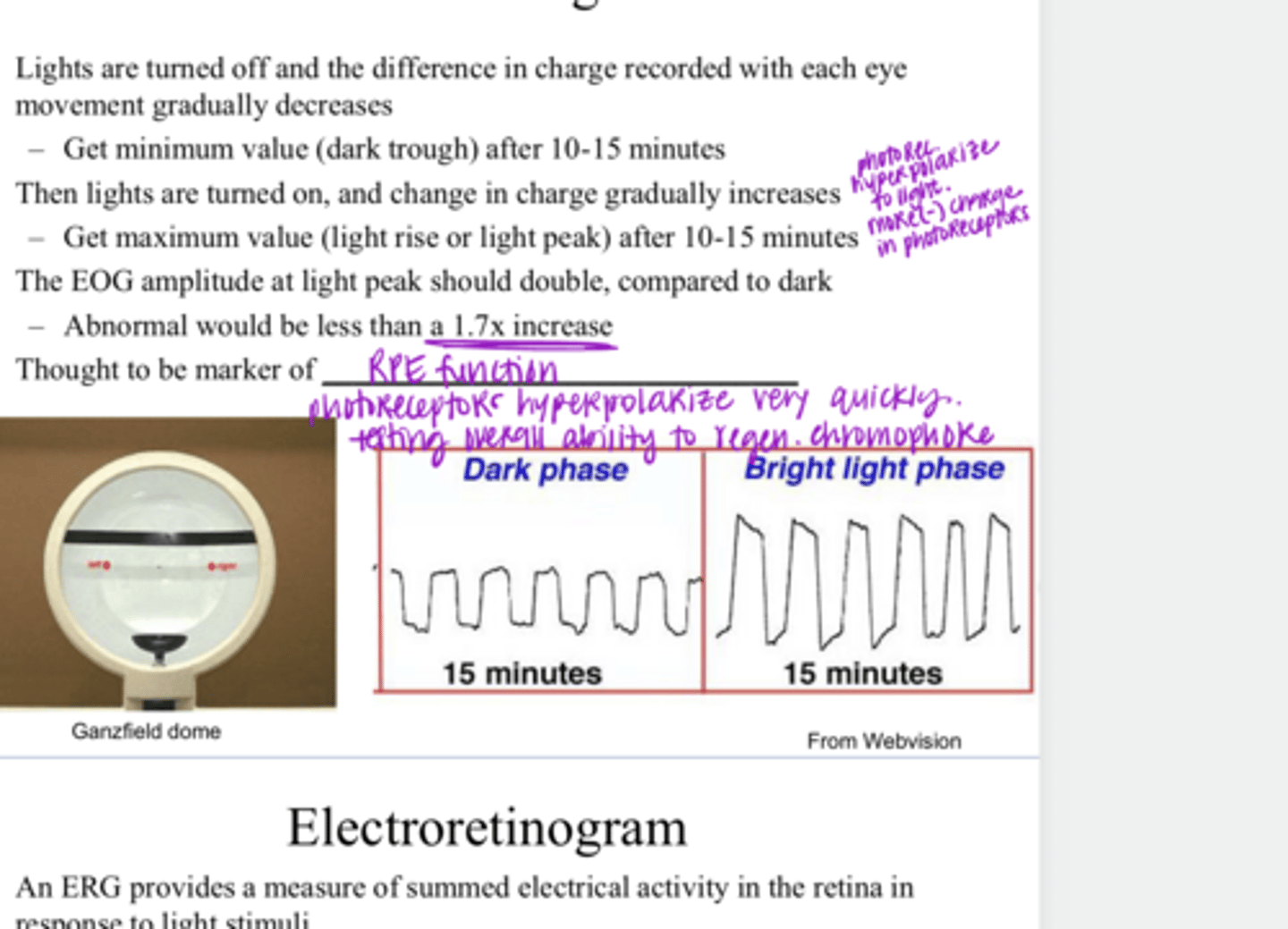
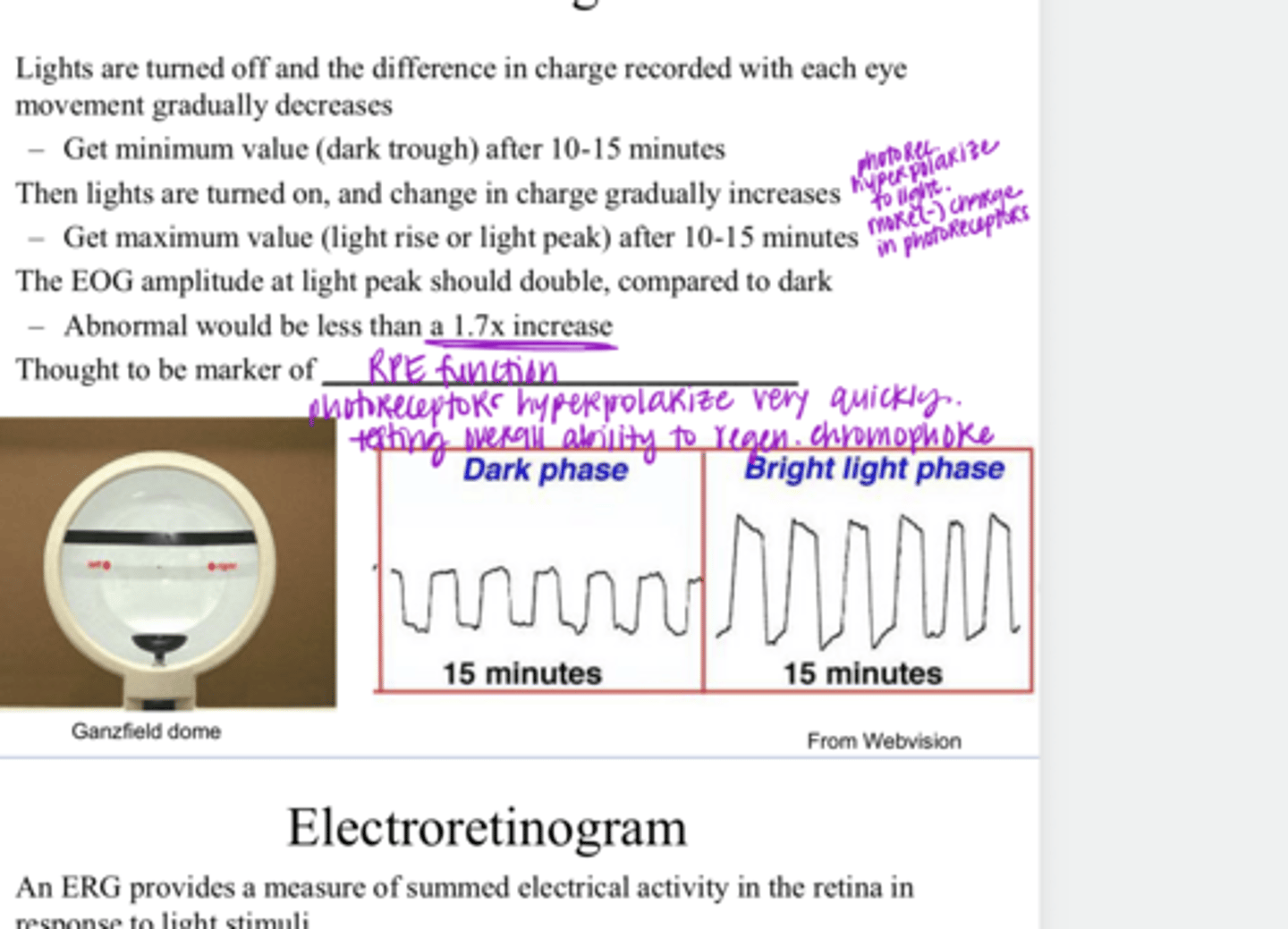
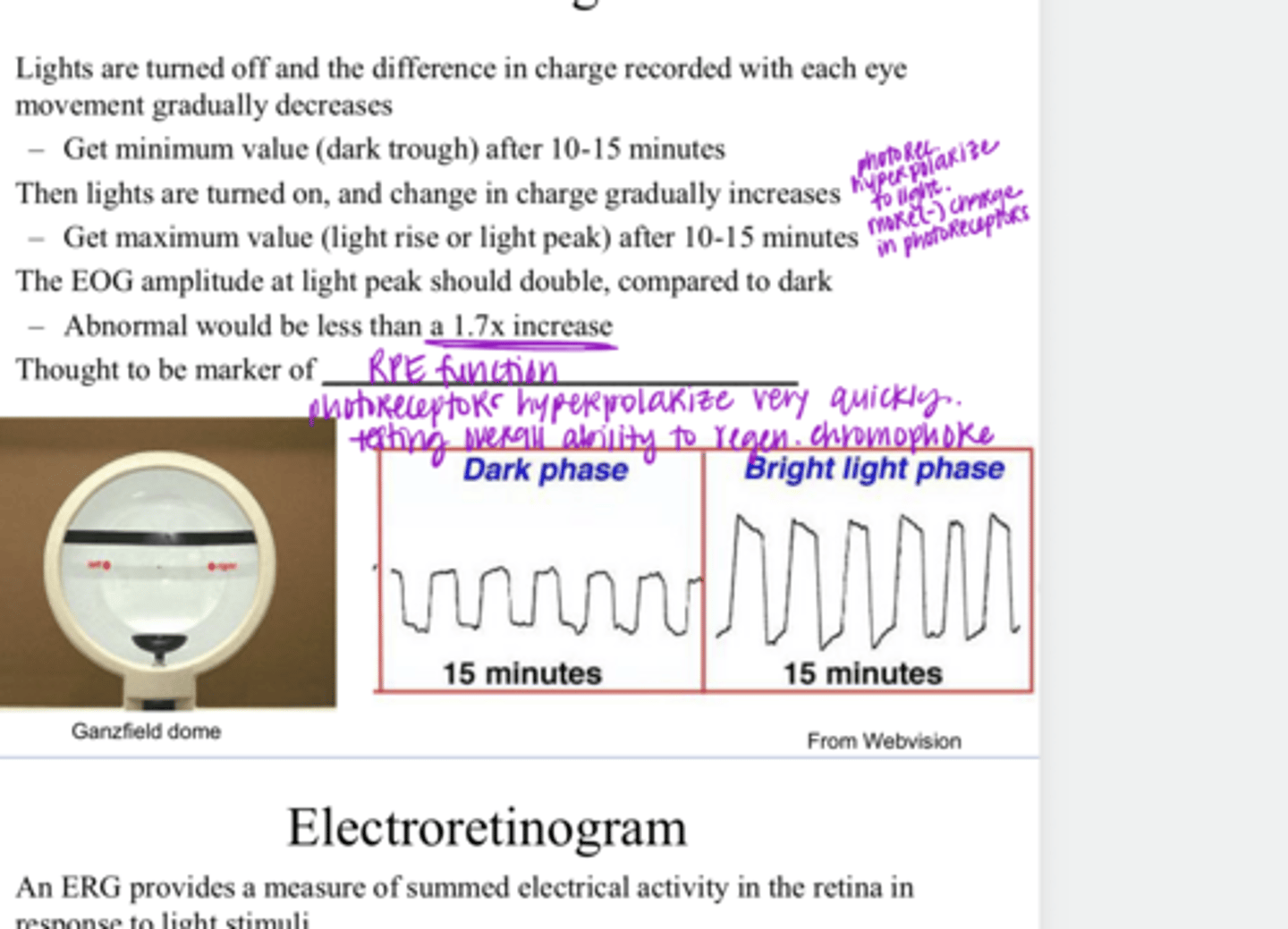
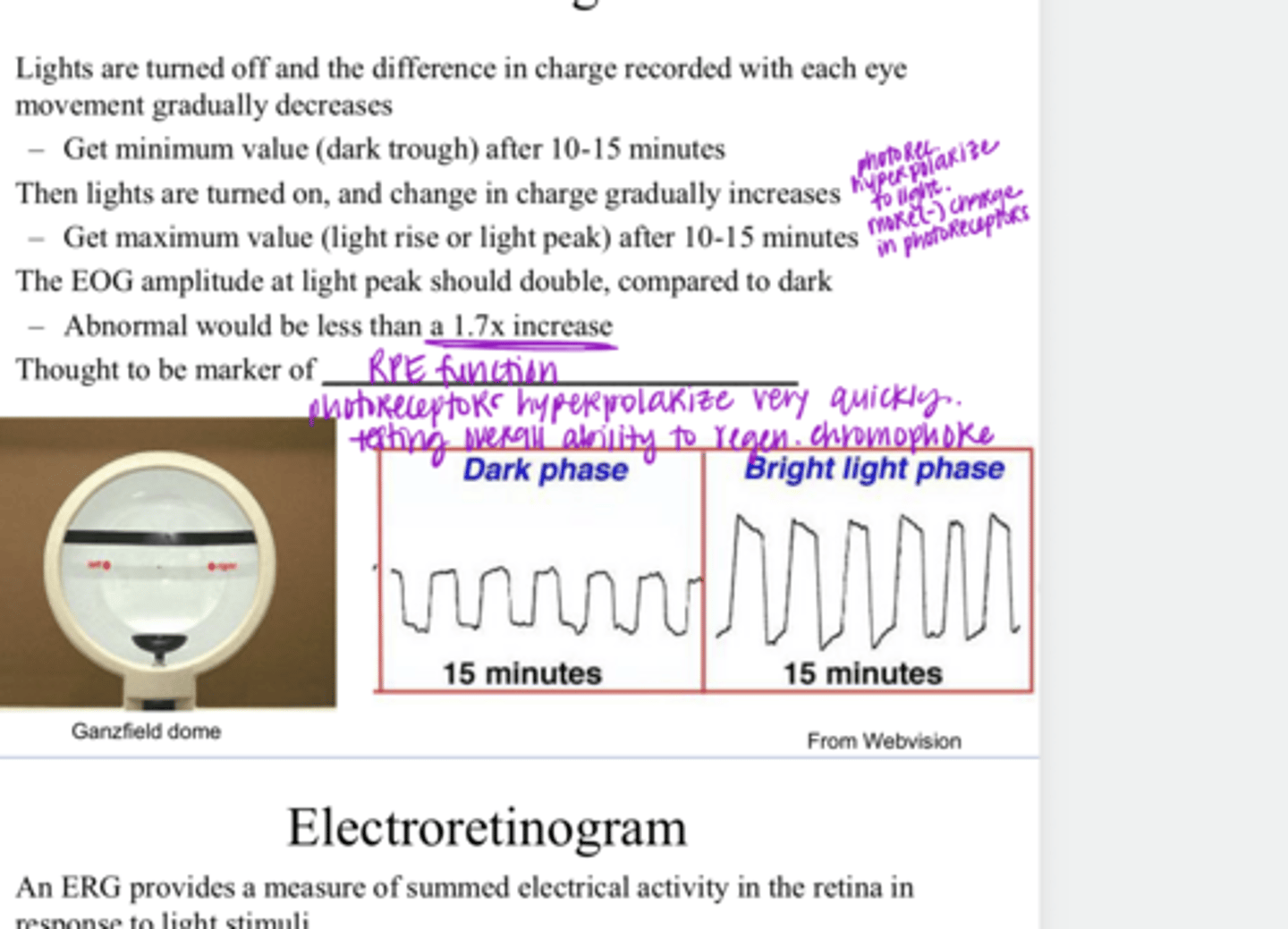
When the lights are turned off, the difference in charge will be recorded with each eye movement, and the charge will gradually (increase/decrease)
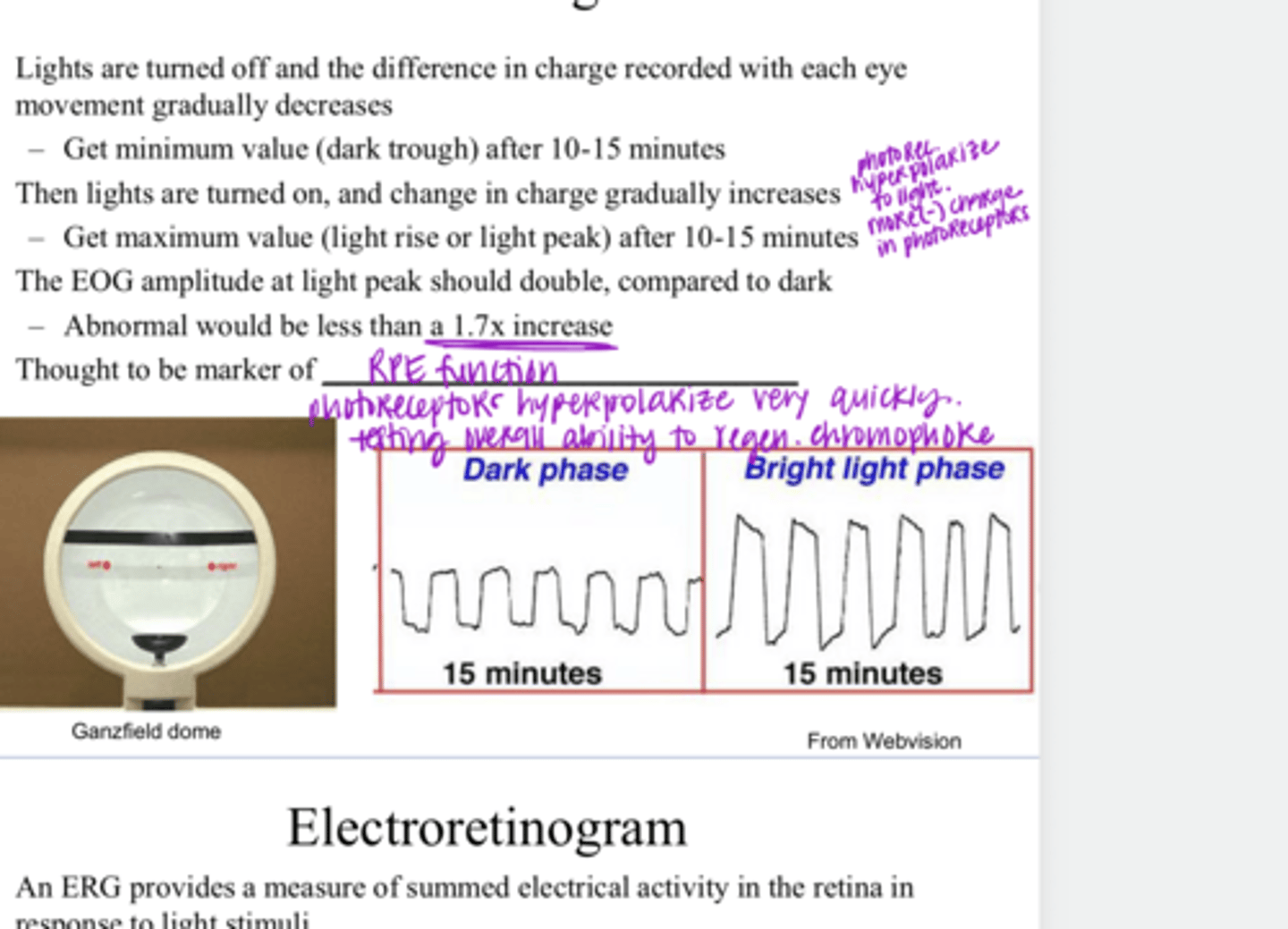
10-15 min
You will get a minimum value for electrical charge difference (dark trough) after approx how many minutes in the dark?
the change in charge will gradually increase
When the lights are turned on, what happens during an EOG (electrooculogram) measurement?
10-15 min
You will get a maximum value for electrical charge difference (light rise or light peak) after approx how many minutes in the light?
double
The EOG amplitude at light peak should ______, compared to the dark
Less than 1.7x increase from dark to light
An abnormal EOG amplitude is what?
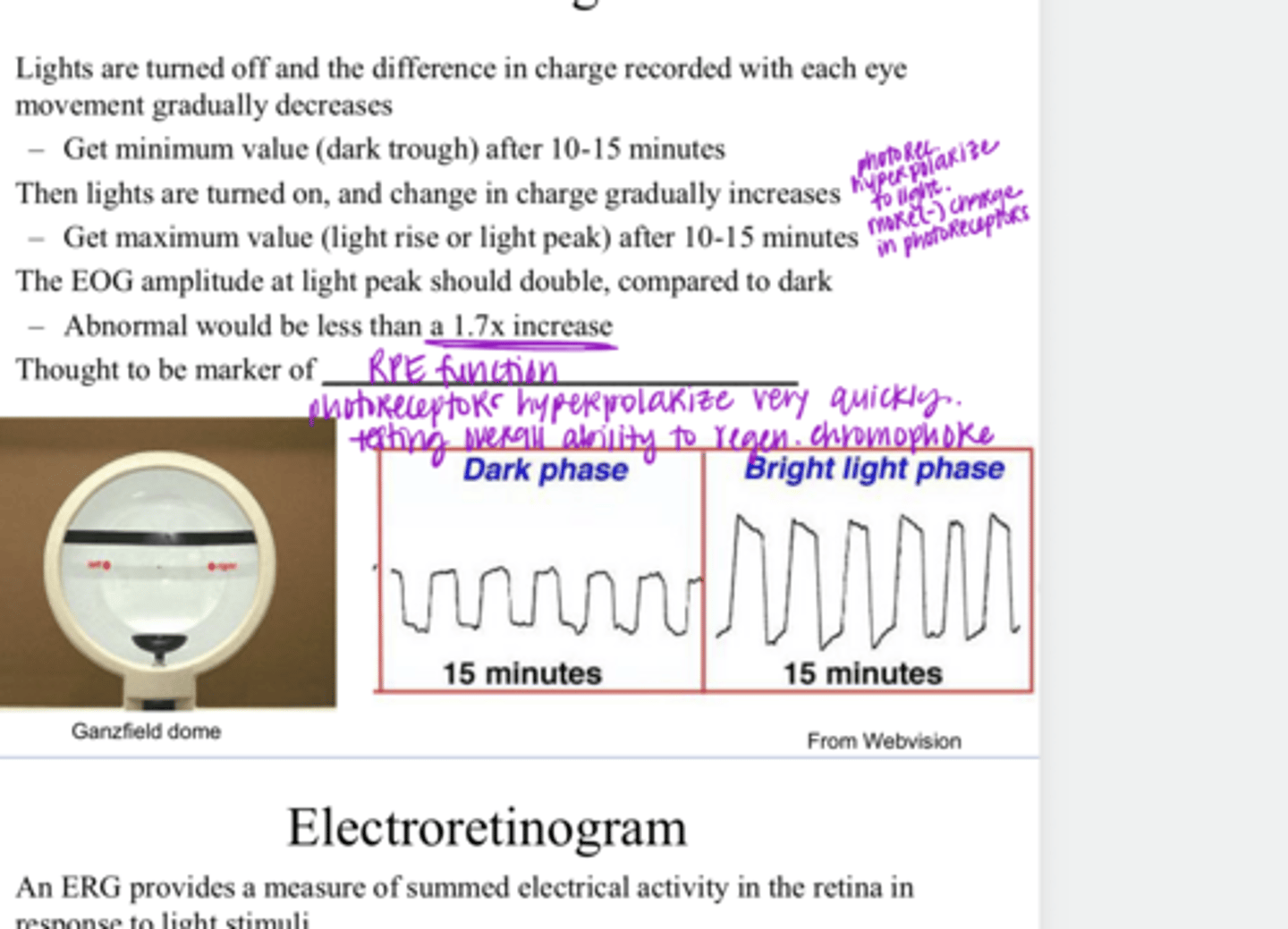
RPE function
**overall ability to regenerate chromophore
Electrooculogram is a marker of what?
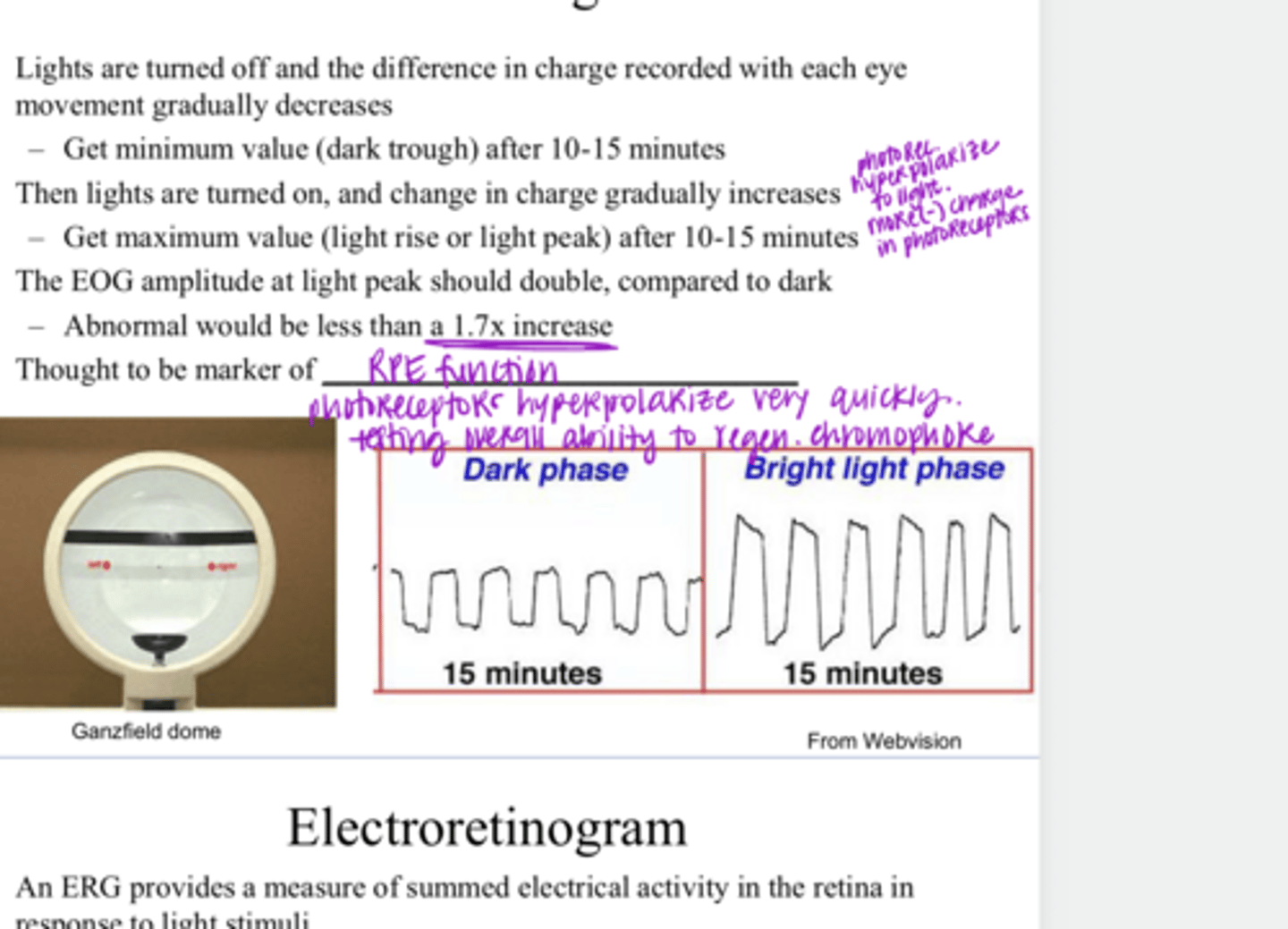
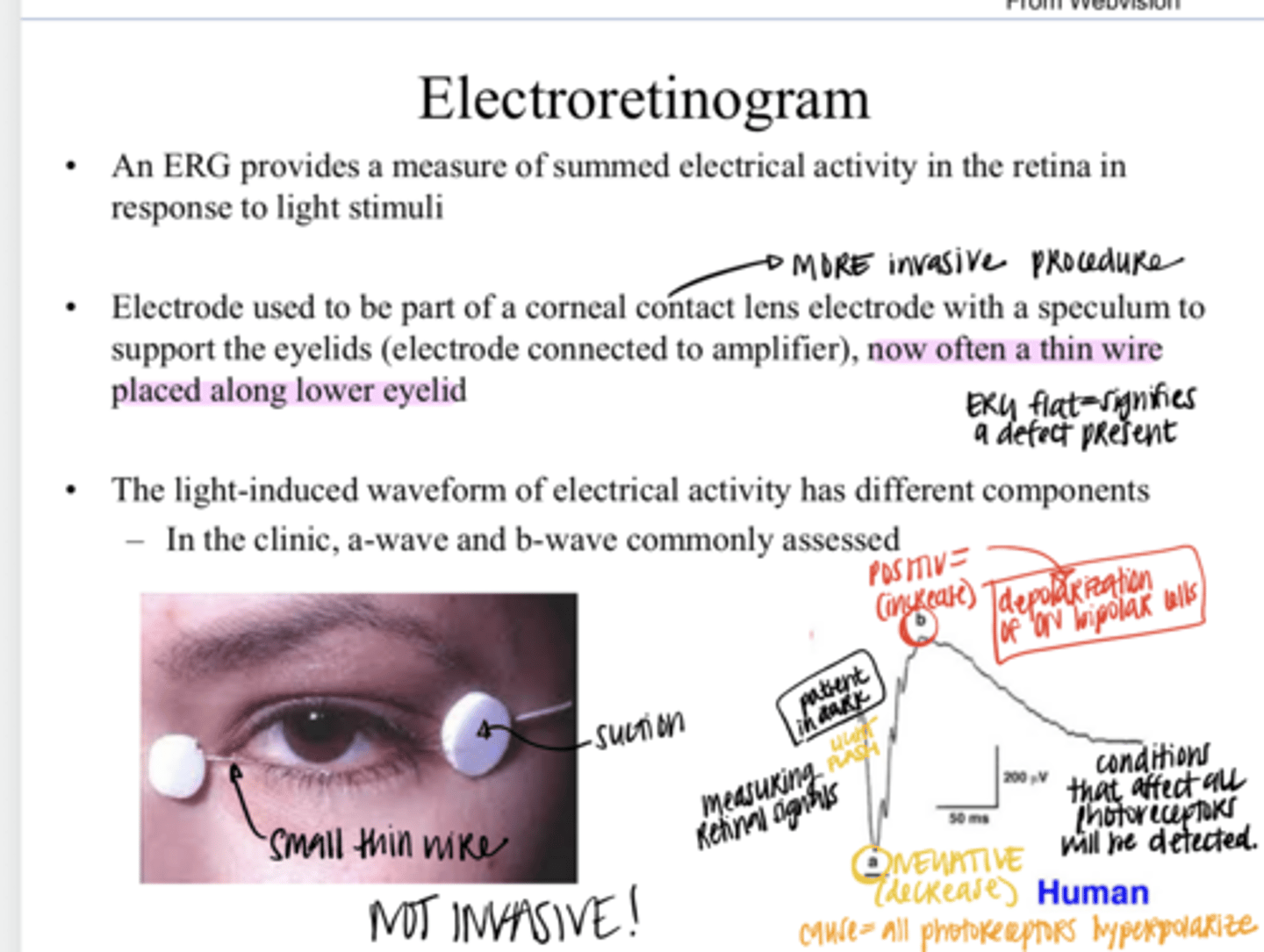
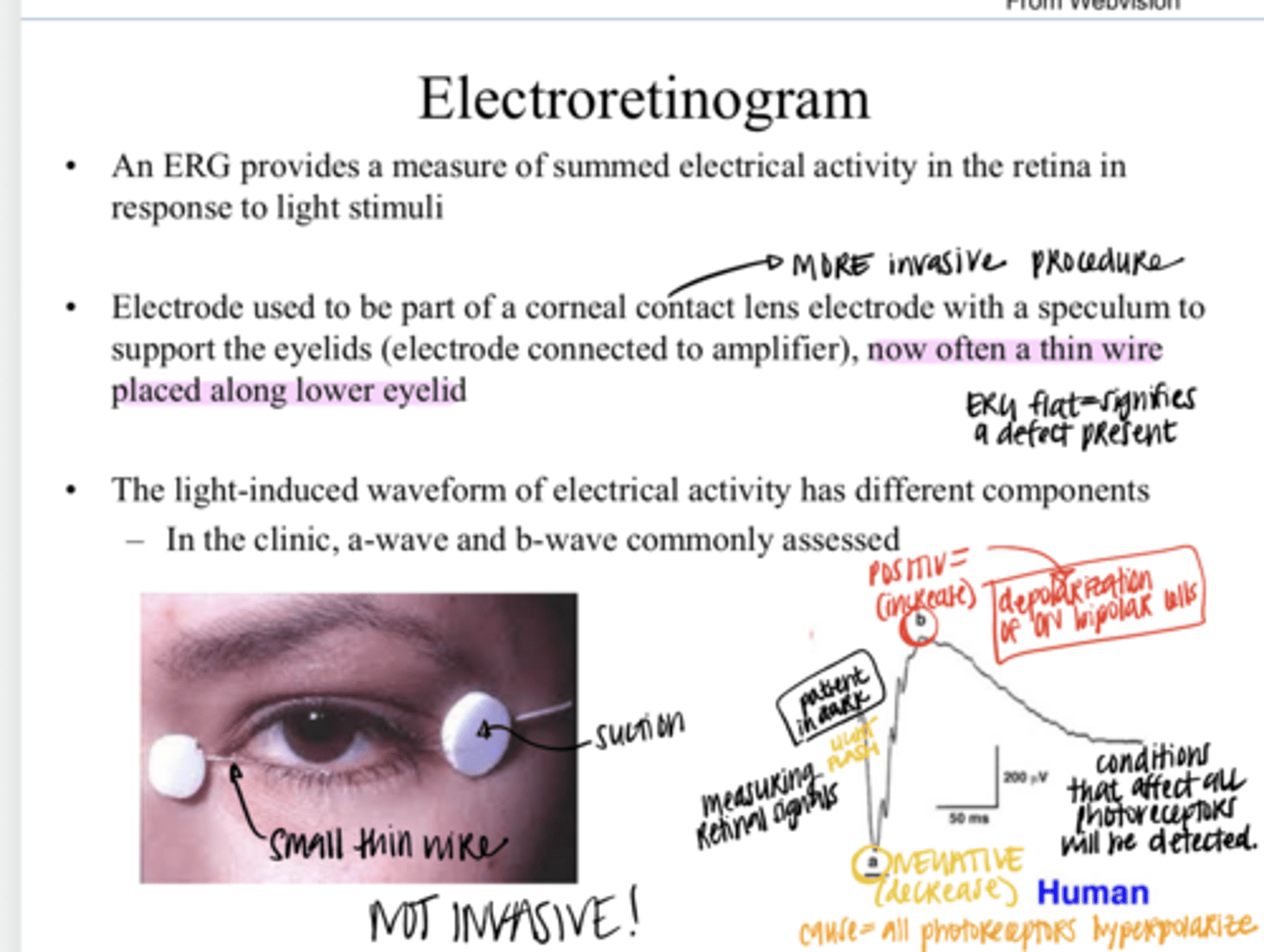
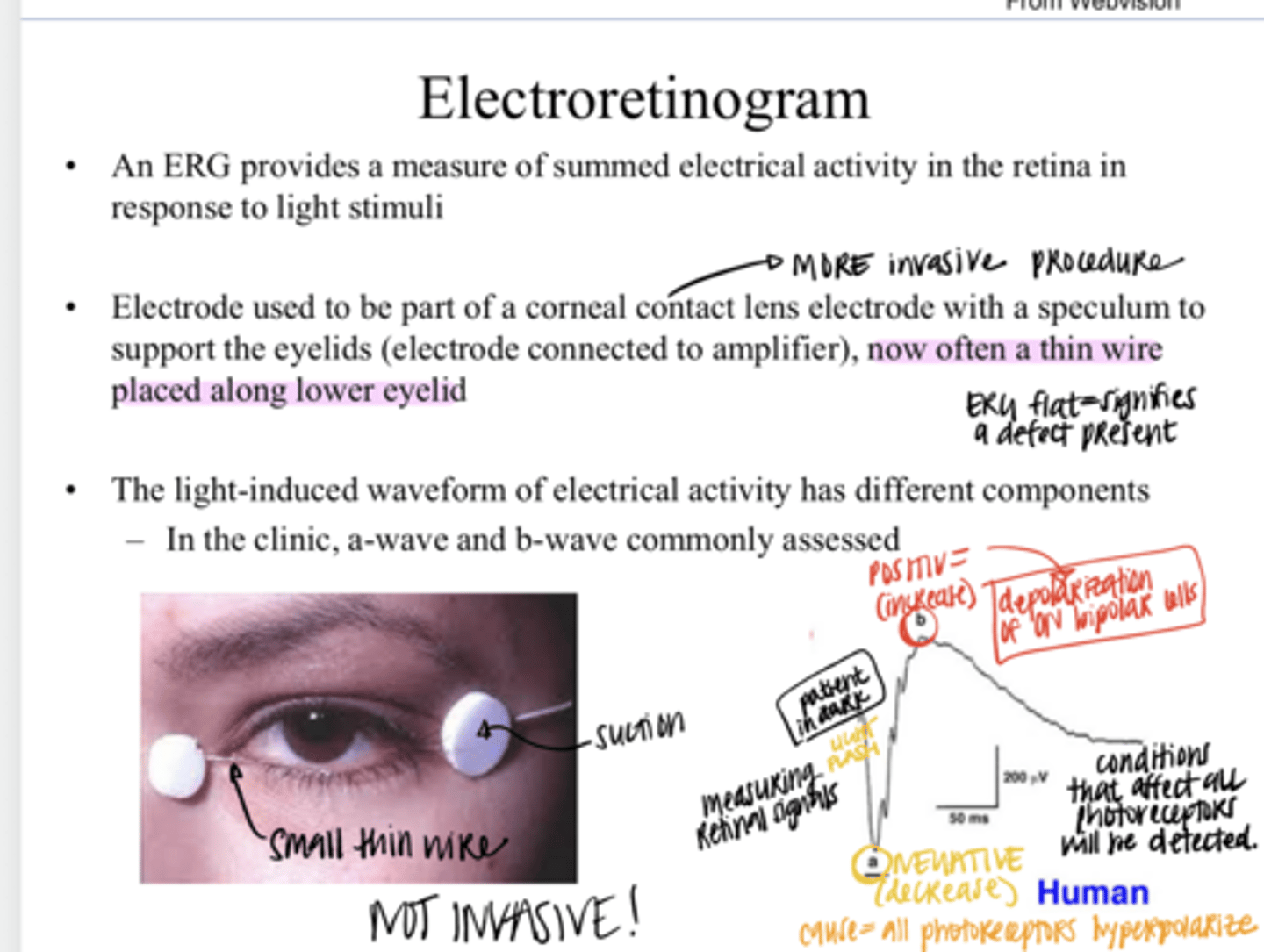
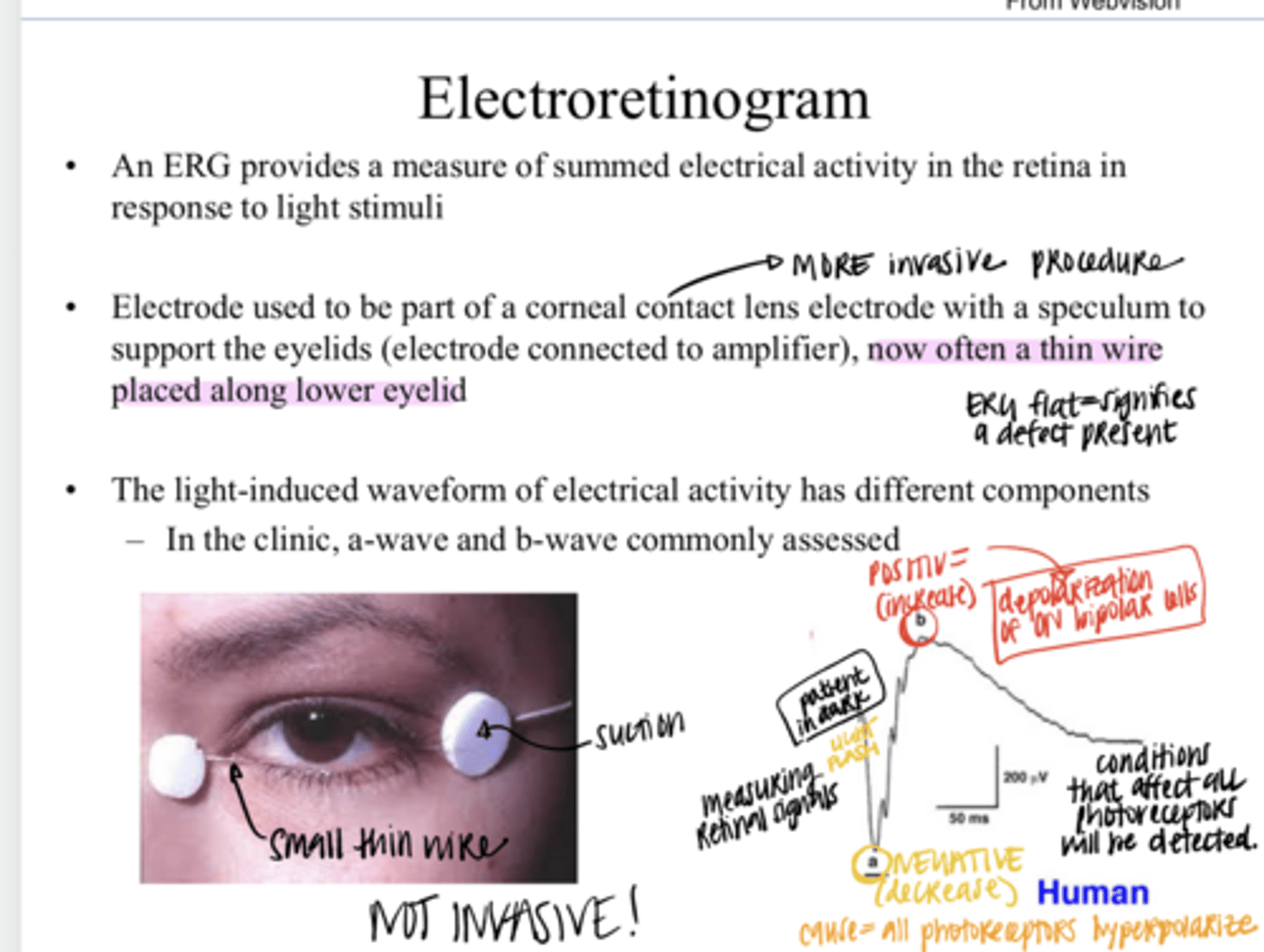
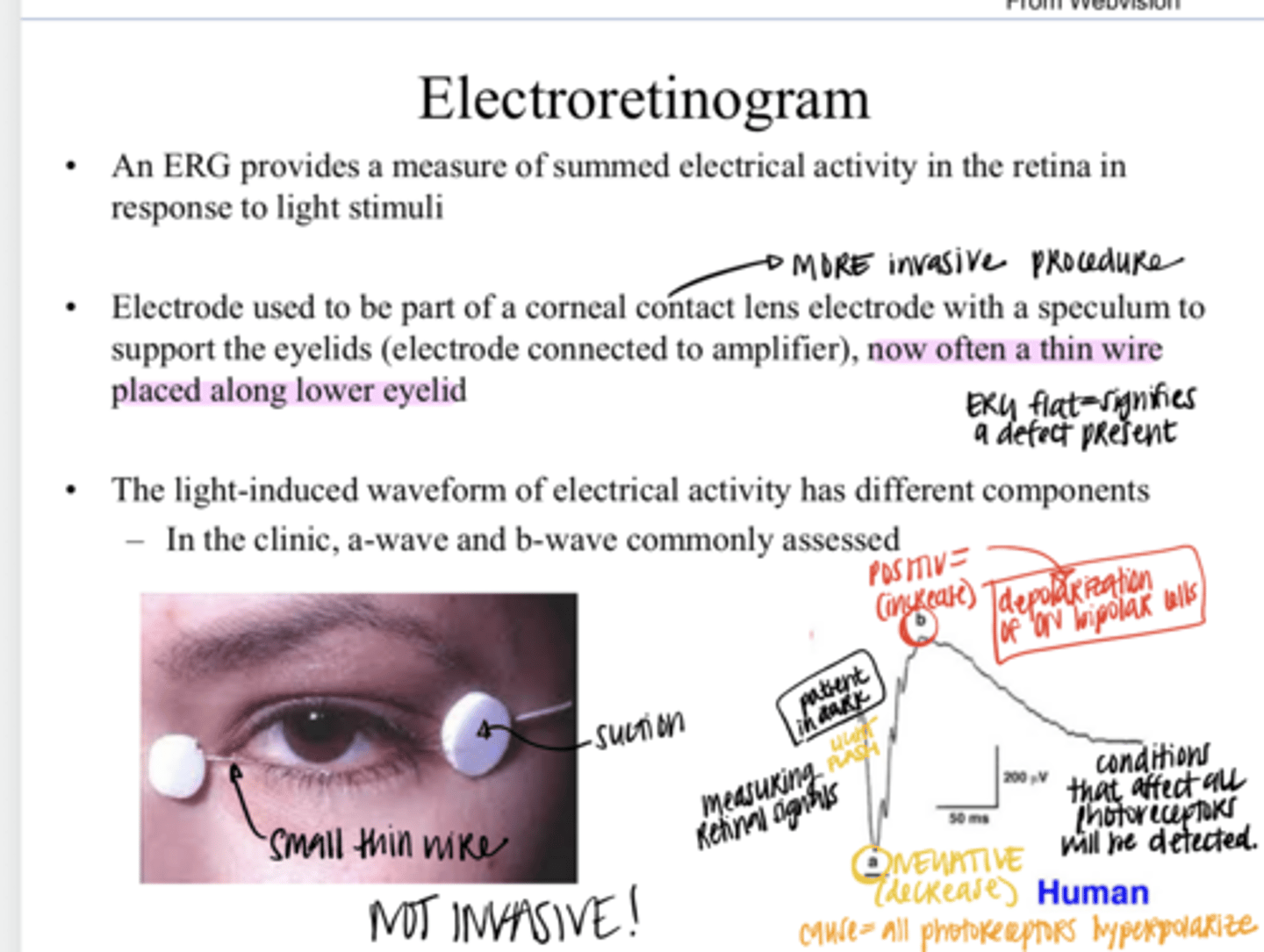
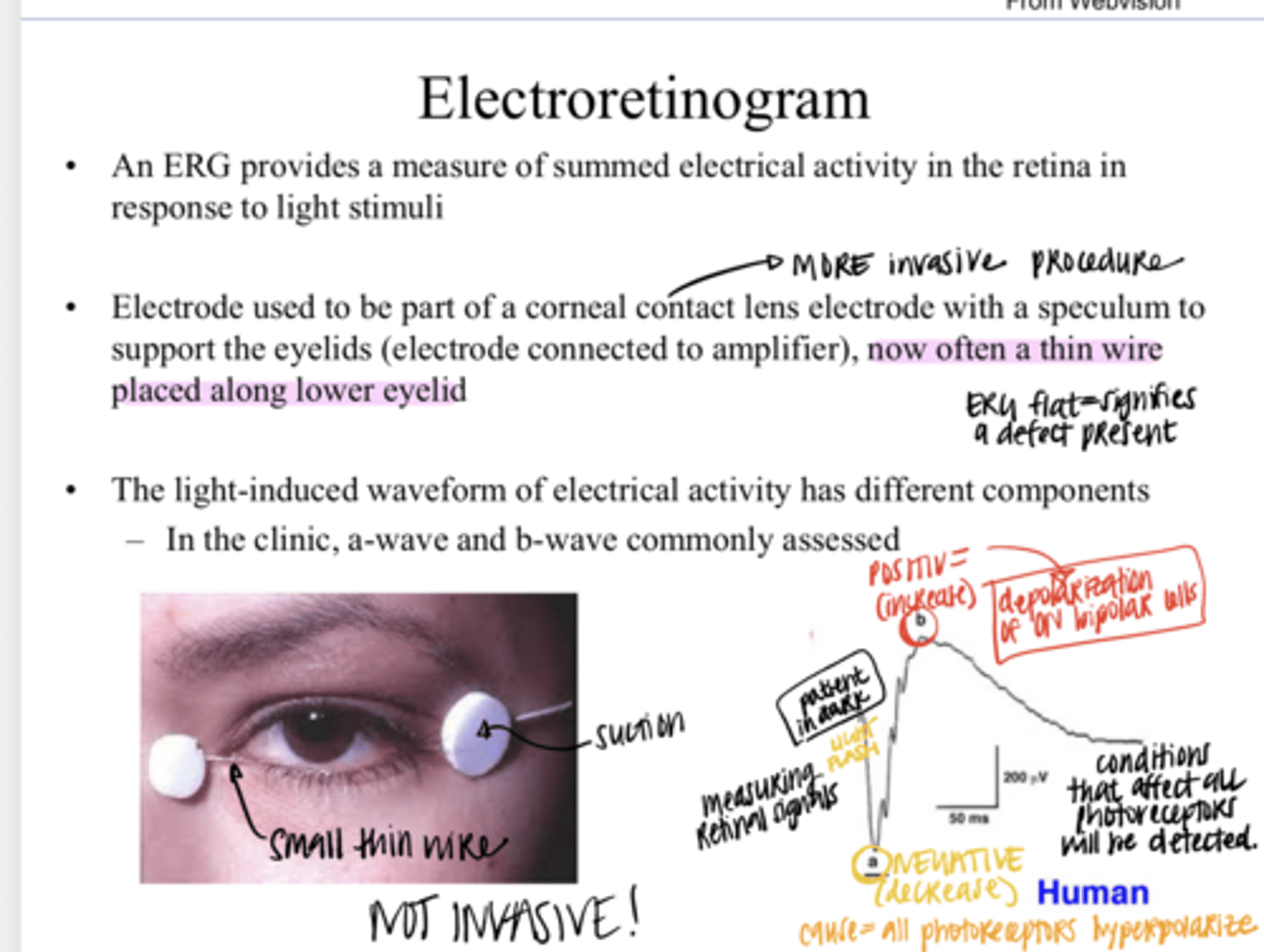
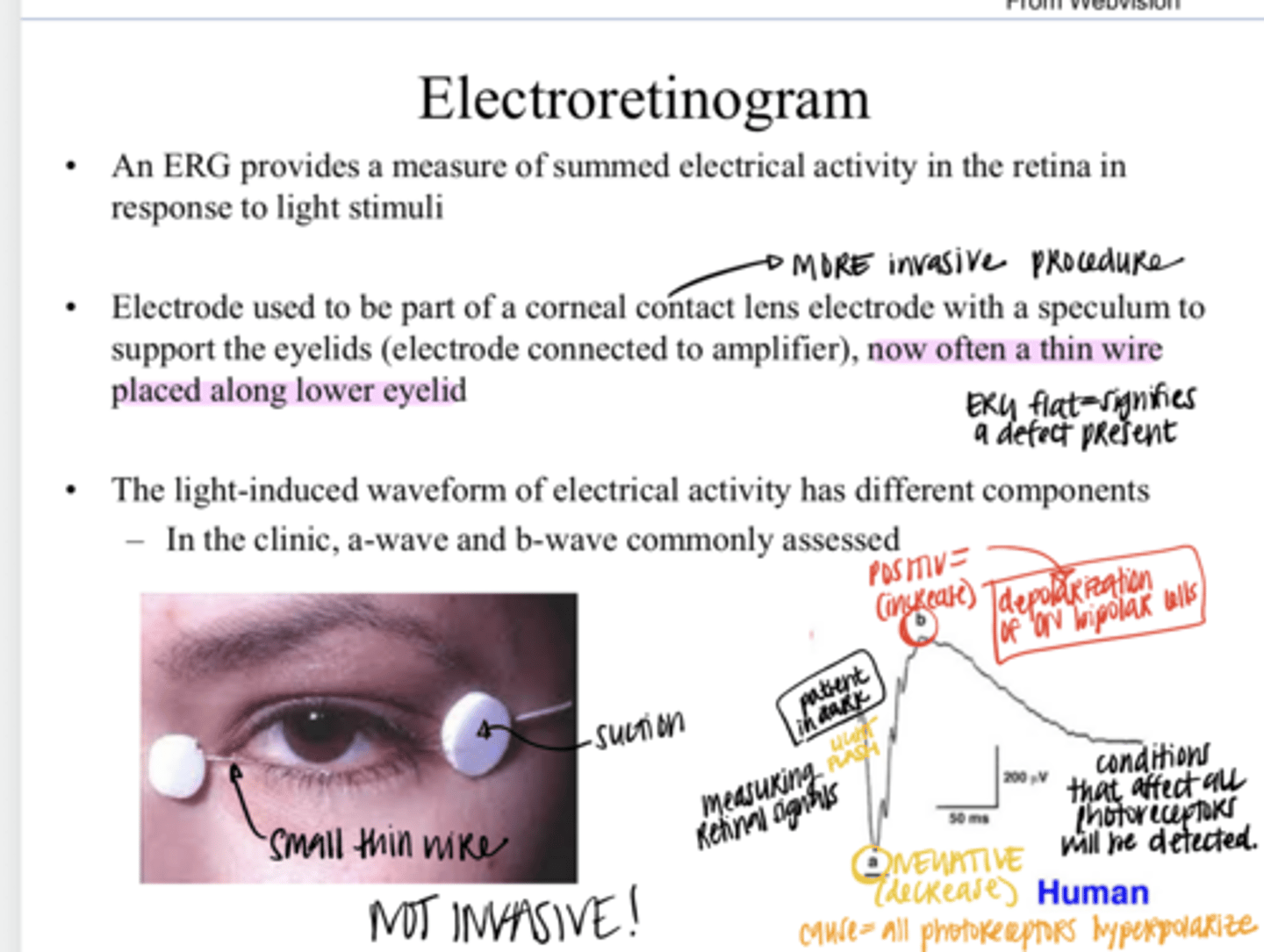
a measure of summed electrical activity in the retina in response to a light stimuli
What does an ERG (electroretinogram) provide?
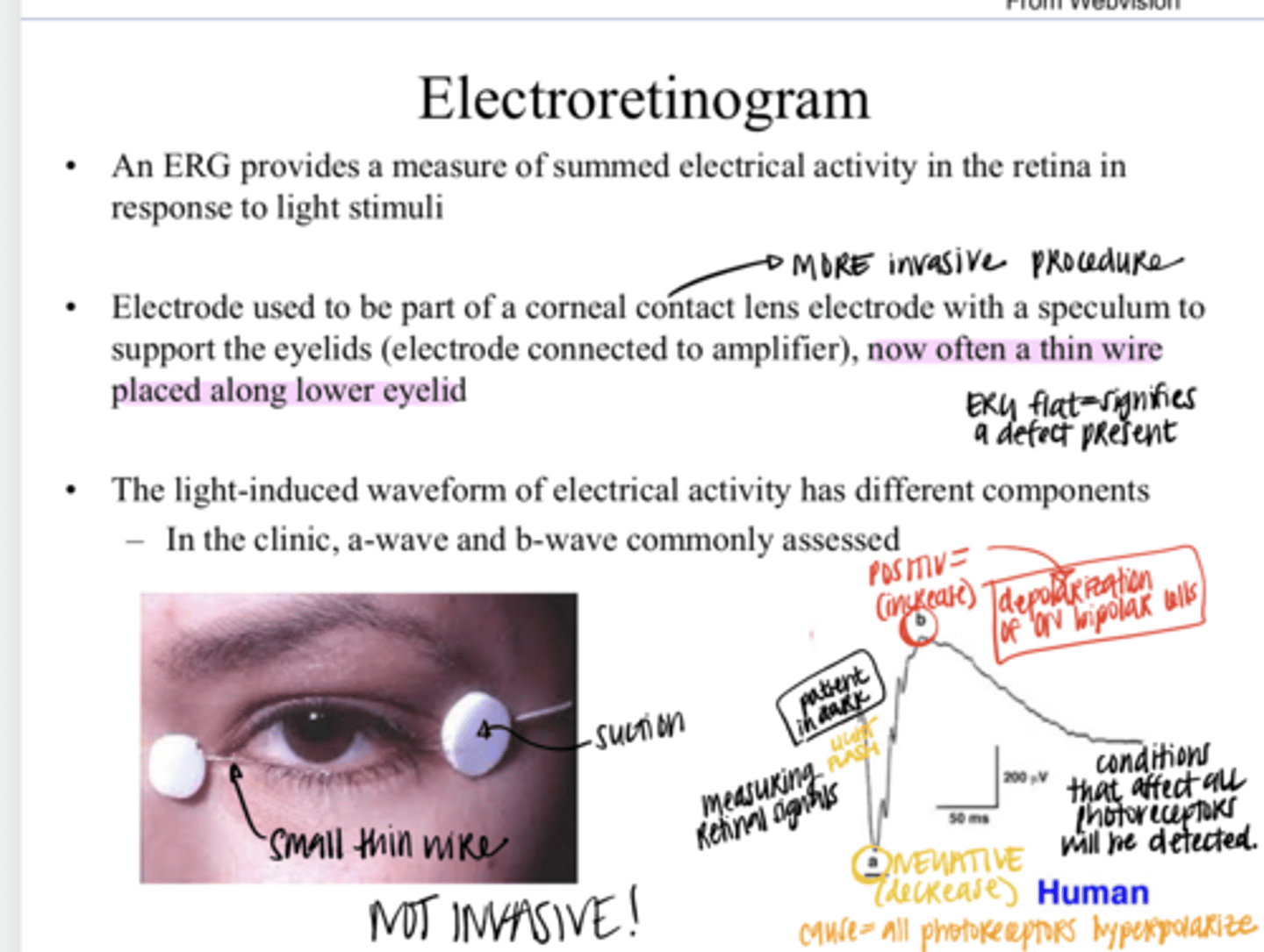
thin wire that is placed along the lower eyelid
What is the design of a electroretinogram today?
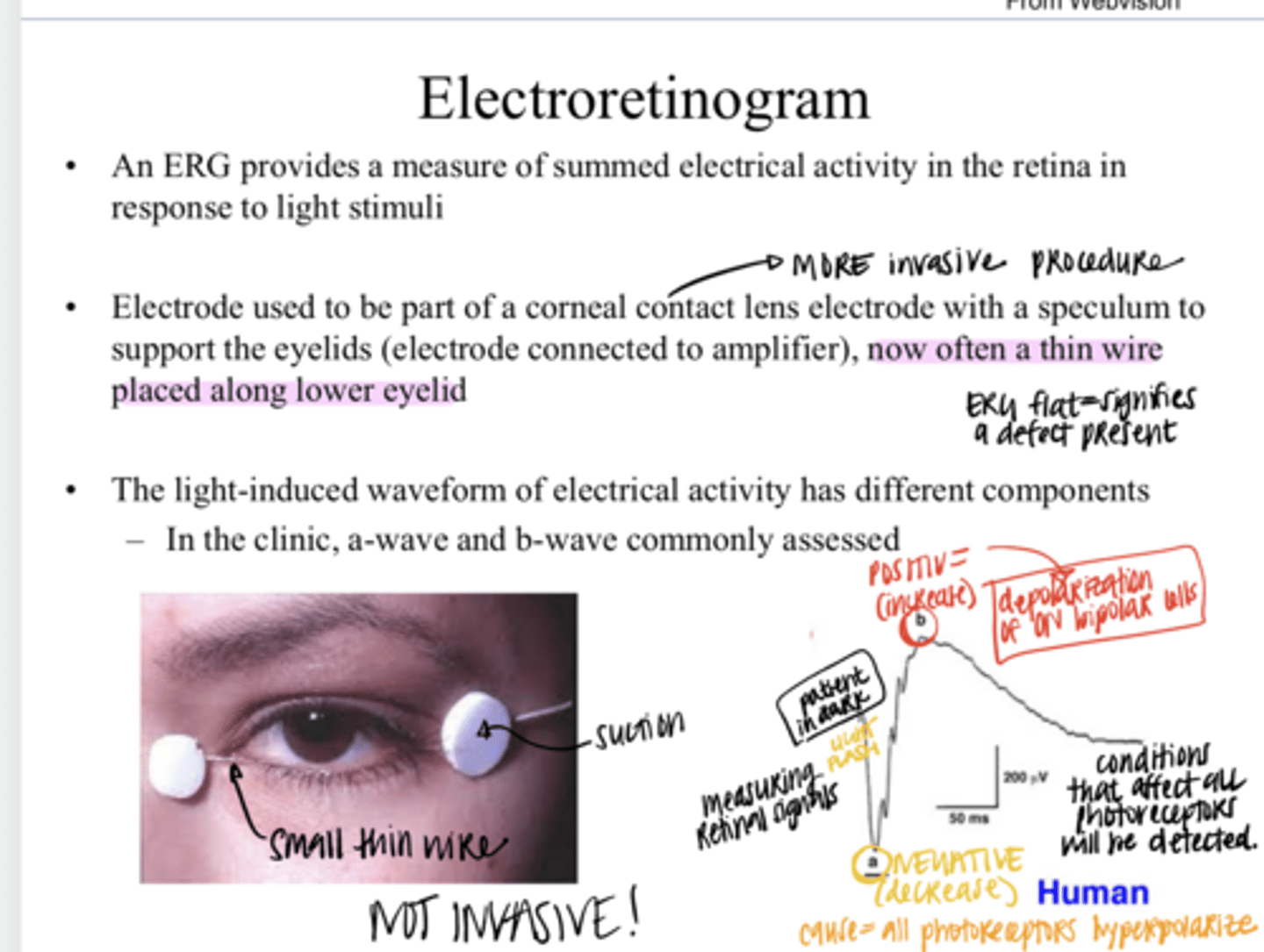
a and b
The light-induced waveform from a ERG has different components. In the clinic, a ____ wave and a _____ wave are commonly assessed?
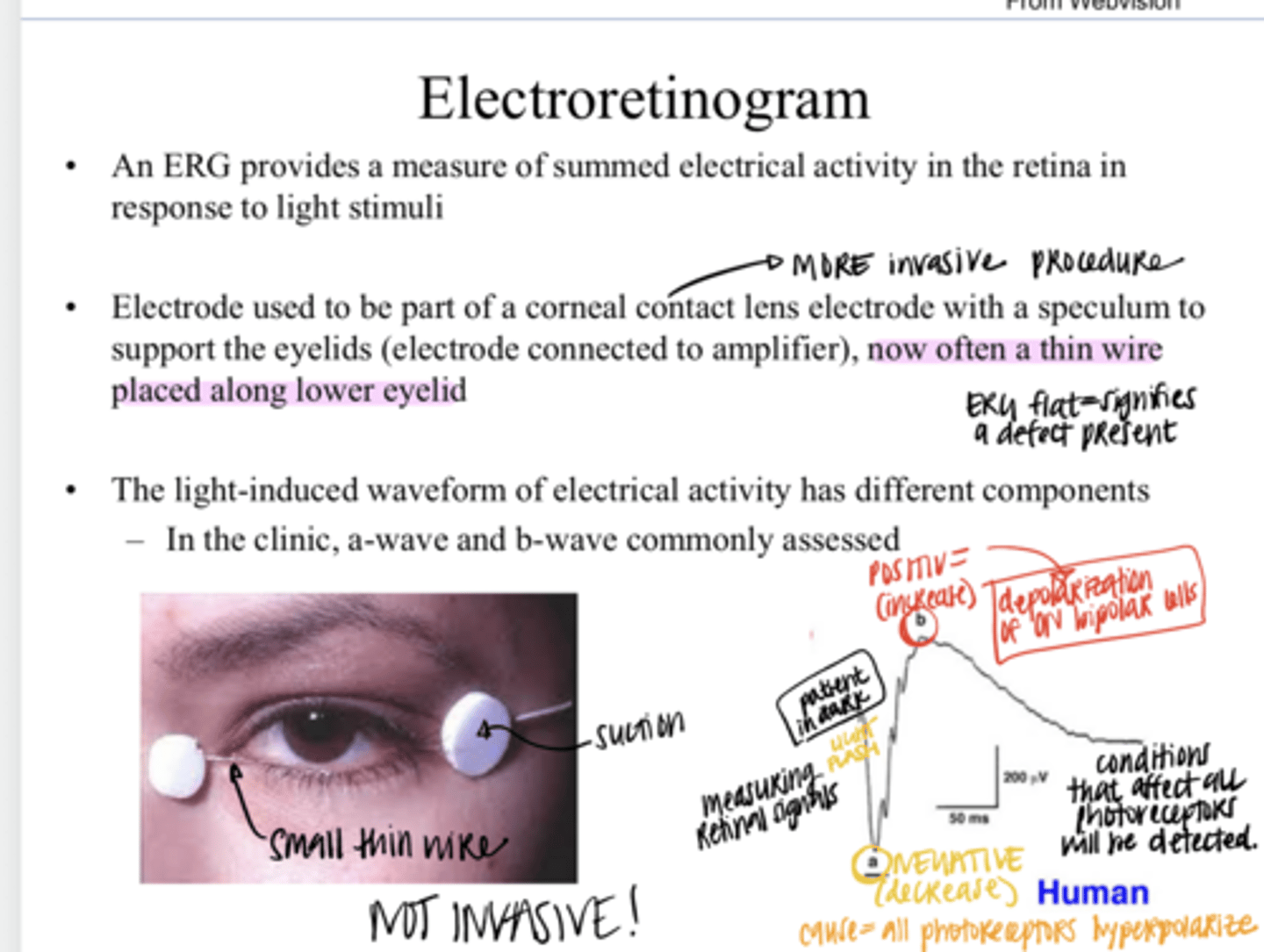
to the reduction in the "dark current" in photoreceptors stimulated with light
The negative a-wave is thought to be d/t what?
the functional integrity of photoreceptors
The negative a-wave is thought to reflect what?
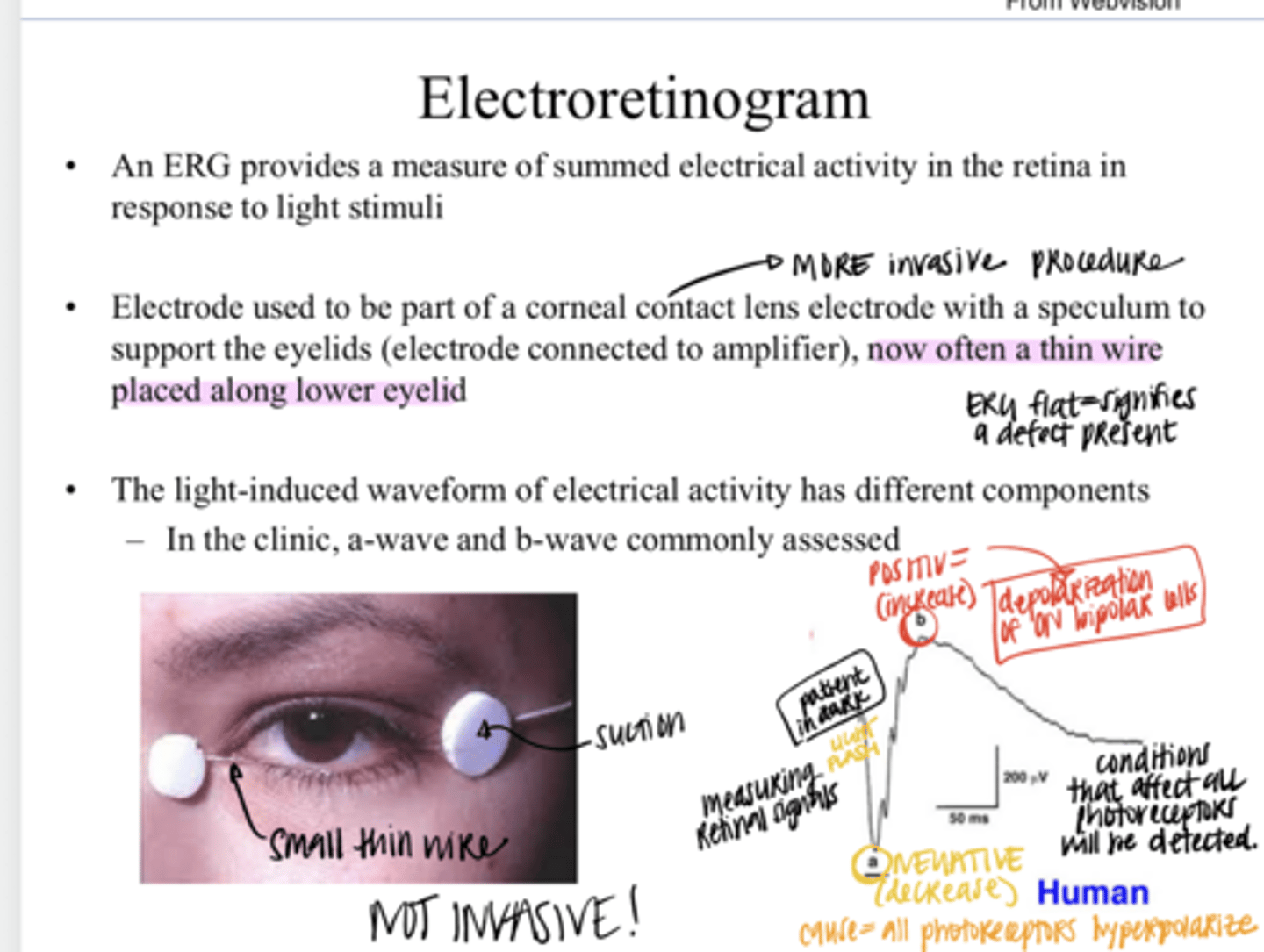
mostly d/t the depolarization of ON bipolar cells, but Muller cells are likely also involved
What is the b-wave origin?
light responses in cells post-synaptic to photoreceptors -- a marker of photoreceptor output
The b-wave is thought to reflect what?
There are many more rods that ONLY talk to ON bipolar cells. Cones talk to both ON and OFF bipolar cells. Patient is dark adapted and rods and cones will both respond to light stimulation. LARGE ON RESPONSE.
Why do you think the ON bipolar cells are dominating the B wave?
There are many less cones in the retina and thus less OFF bipolars are stimulated in comparison to ON.
Why do you think the b-wave is so large when you flash a light on a dark-adapted eye?
outer
The ERG seems to be driven by changes in the (inner/outer) retina
No -- ERGs are driven by changes in the outer retina and RGCs are in the inner retina
Do the inner neurons, such as RGCs, have a lot of contribution to ERGs?
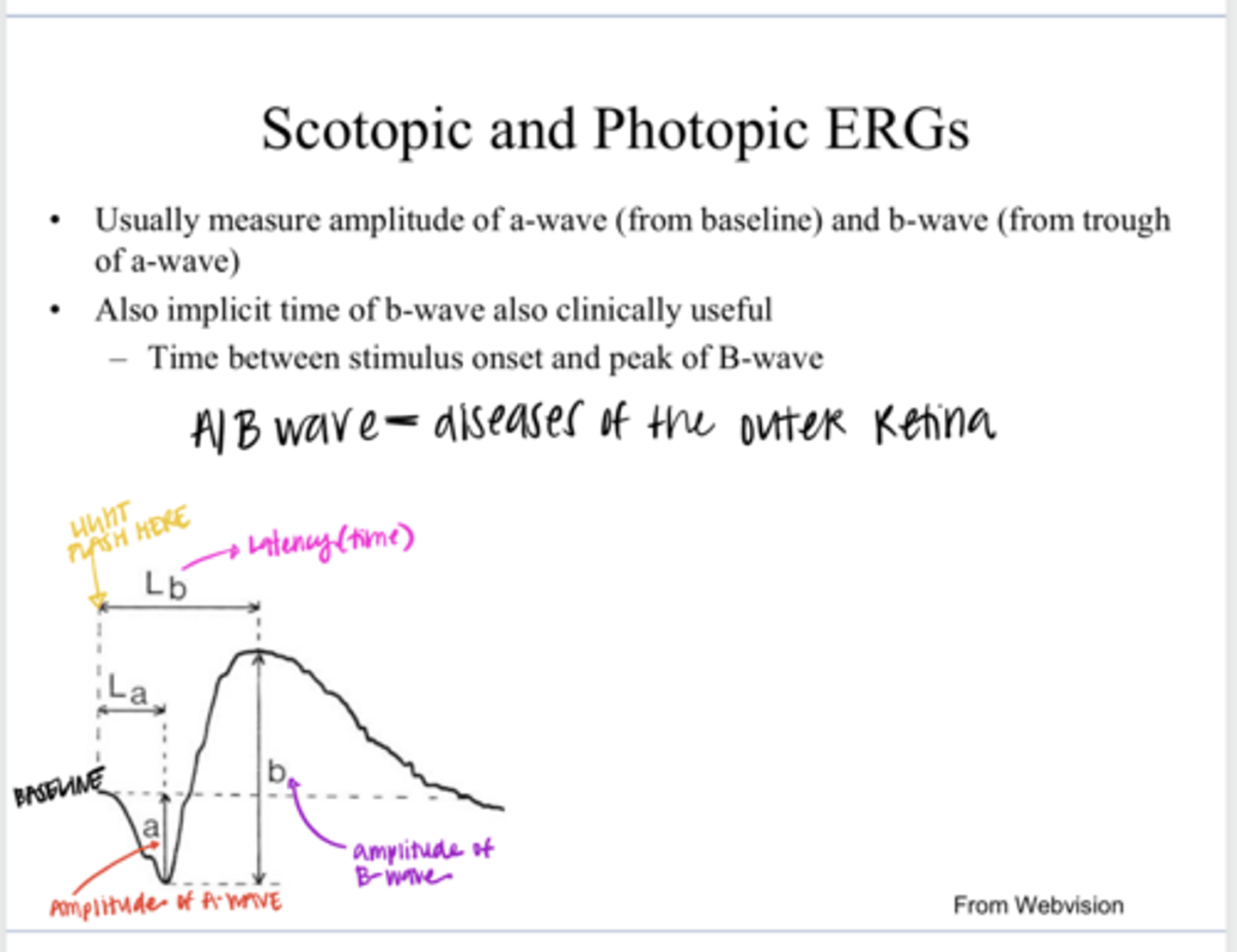
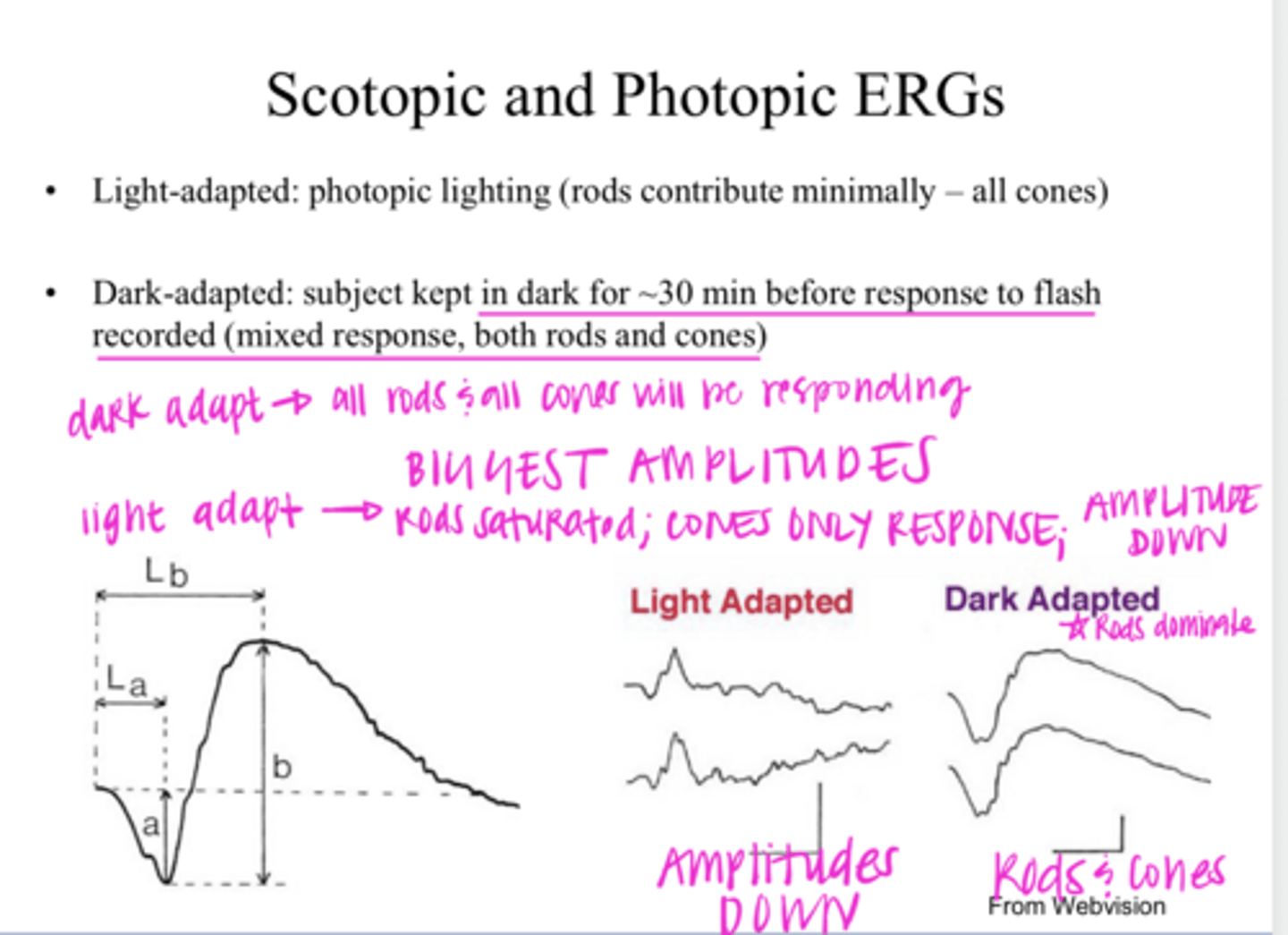
from baseline to the trough of the a-wave
How to measure amplitude of the a-wave of a ERG?
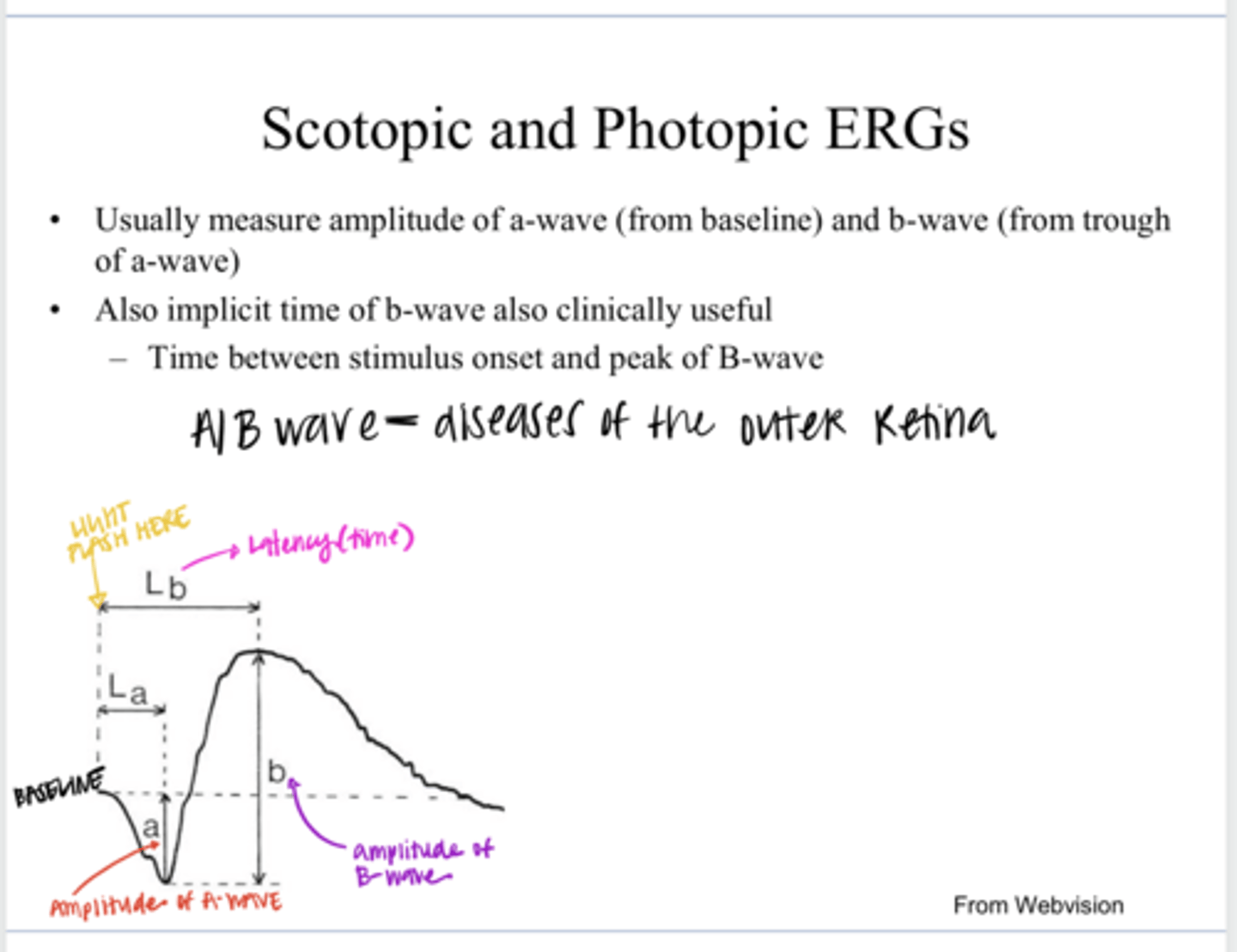
from the trough of the a-wave to the peak of the b-wave
How to measure amplitude of the b-wave of a ERG?
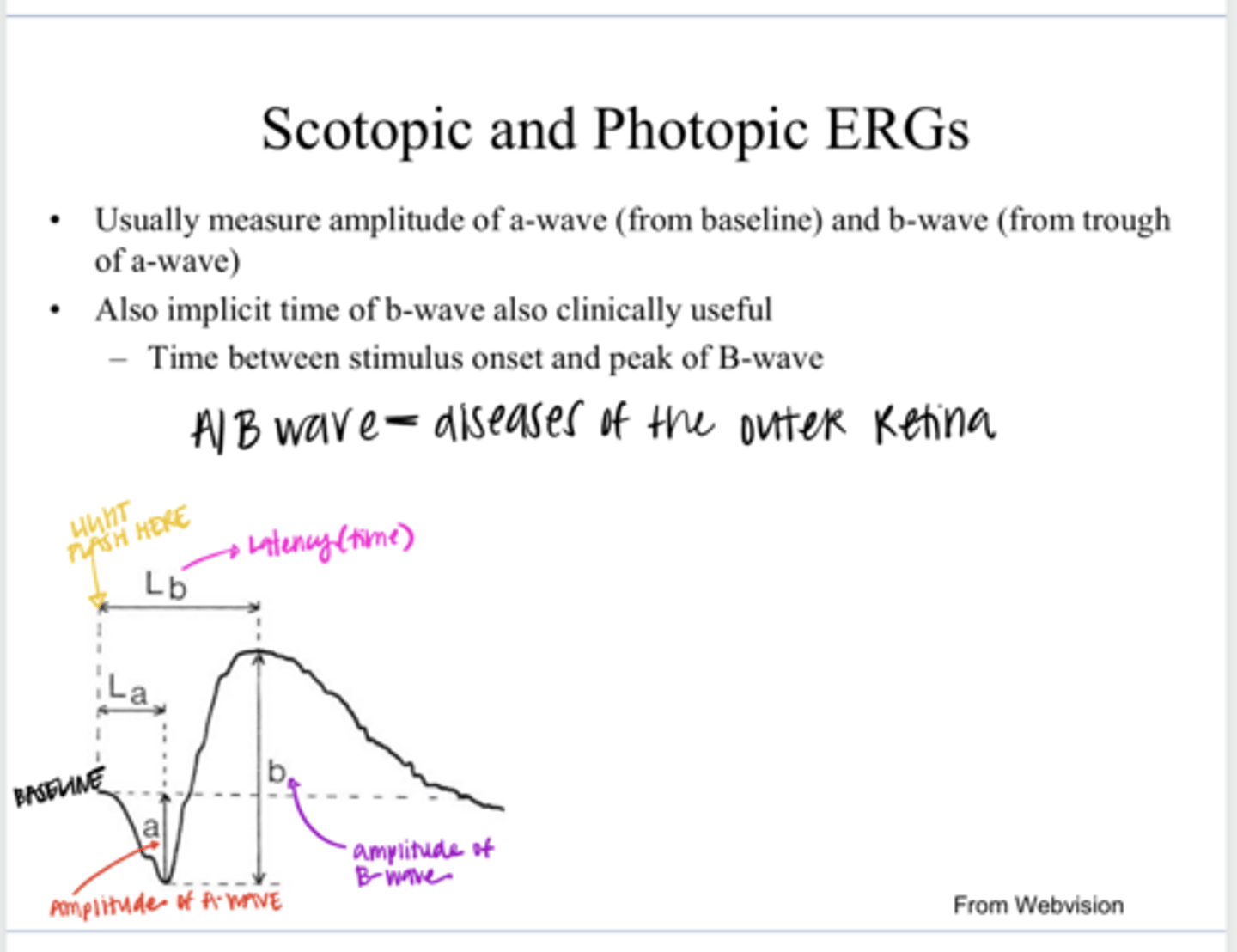
the implicit time of the b-wave (the time between the stimulus onset and the peak of the b-wave) or LATENCY
Besides the amplitudes of the waves on ERG, what is also clinically useful?
Cone only response d/t rod saturation; amplitudes will be reduced
When the patient is LIGHT ADAPTED, the ERG will look like what?
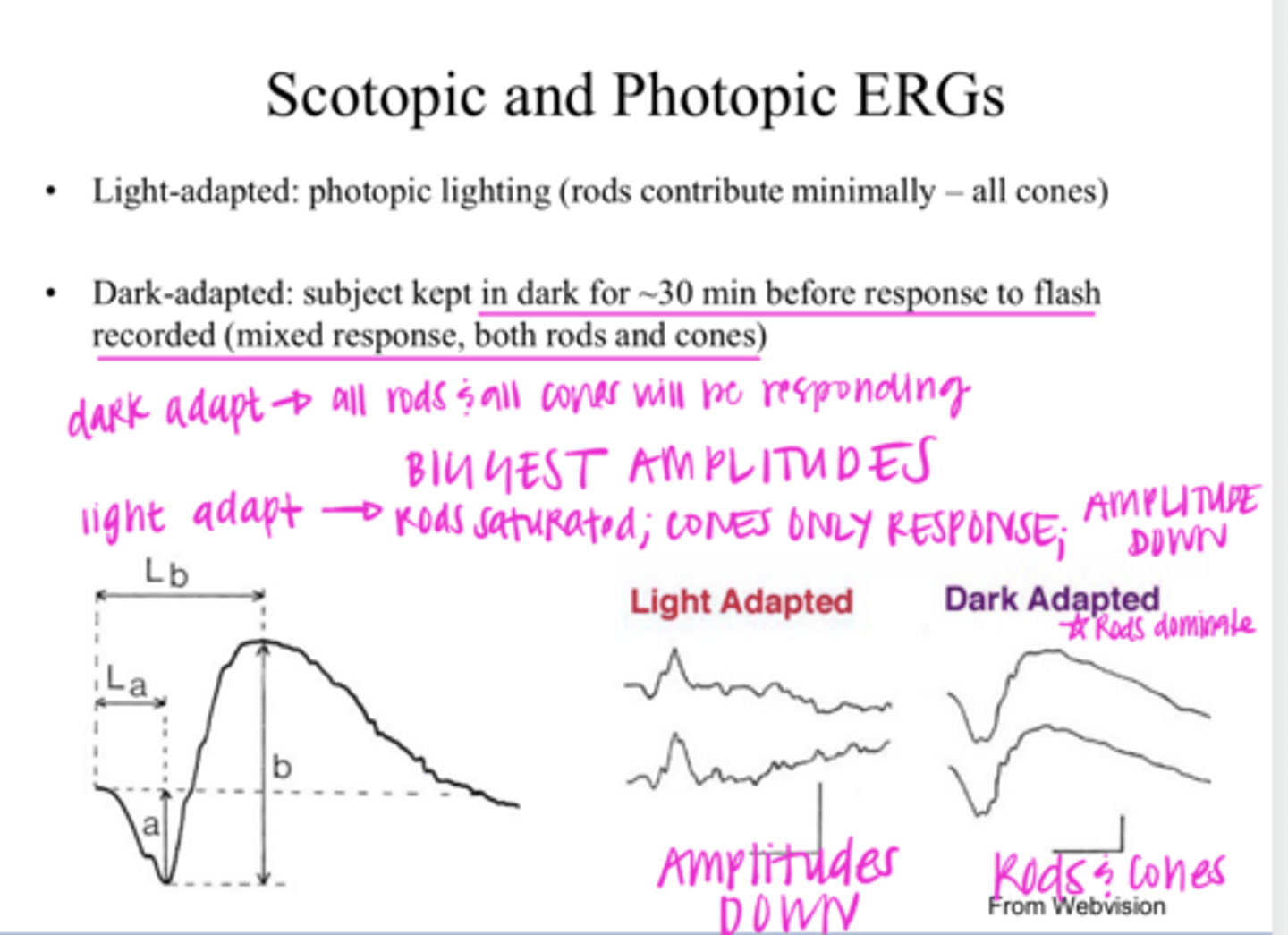
Rod and cone response; maximal amplitudes
When the patient is DARK ADAPTED, the ERG will look like what?
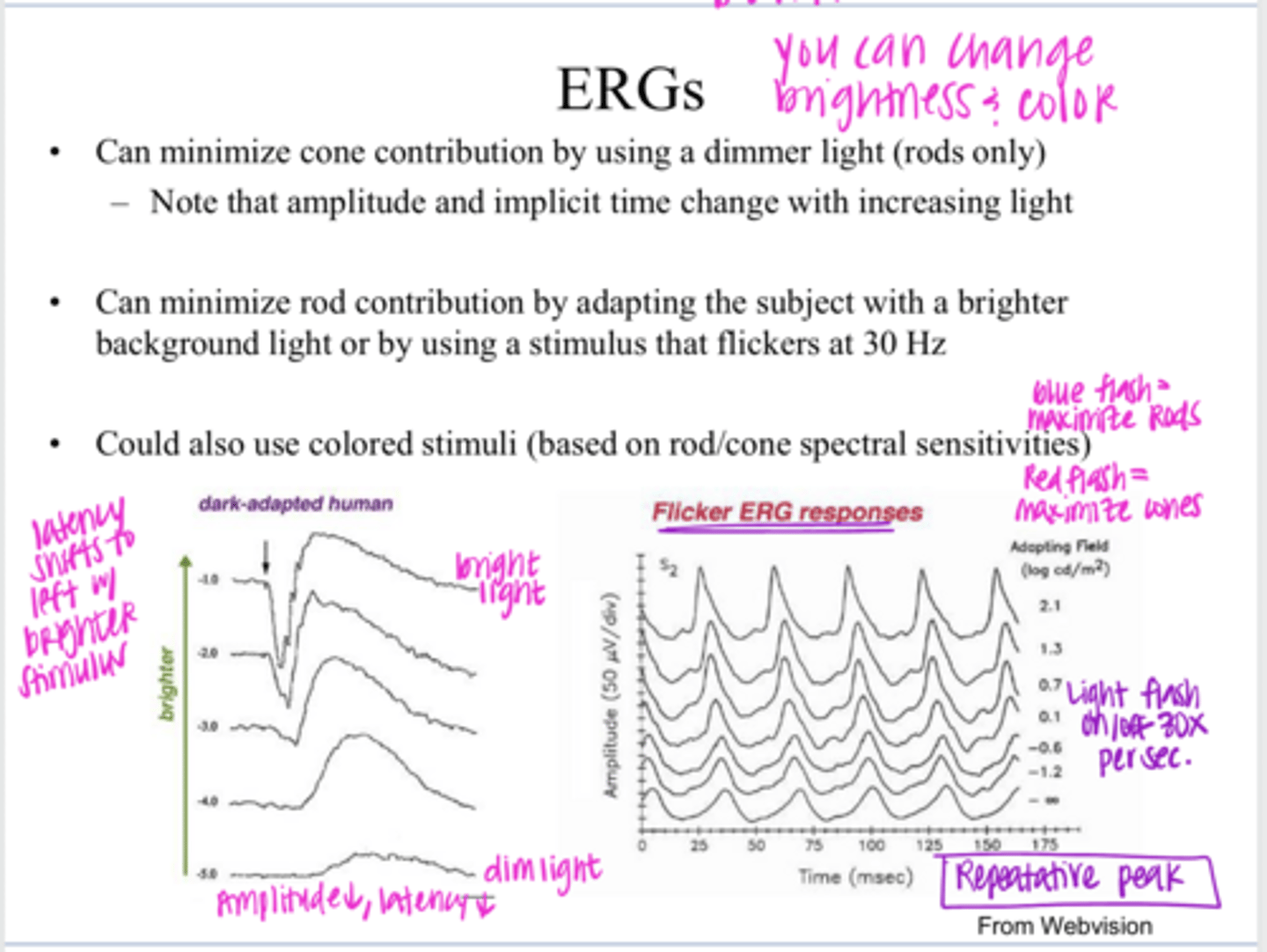
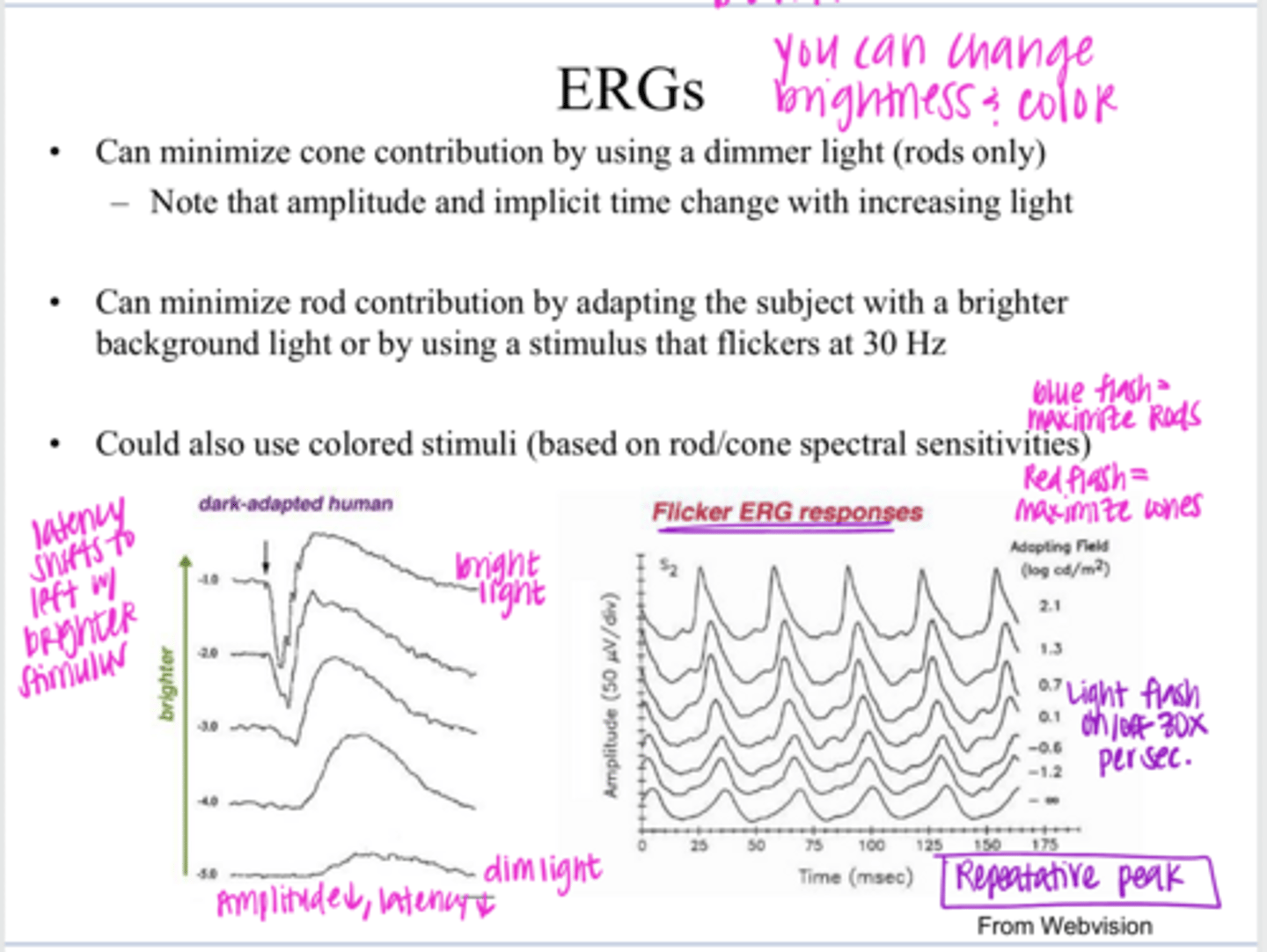
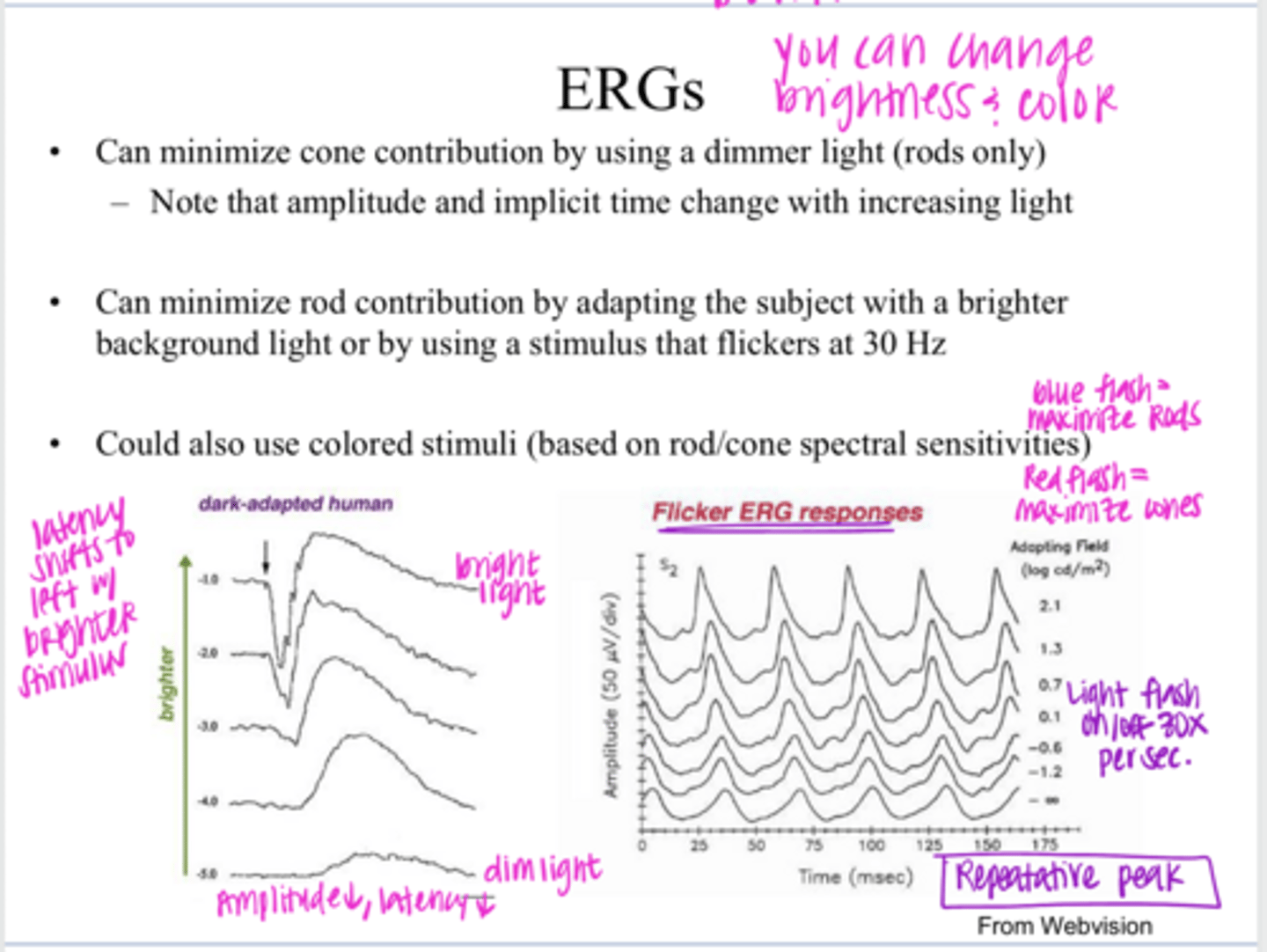
use a dimmer light
How can we minimize cone contribution to an ERG (ie have a rod only response) by changing the brightness?
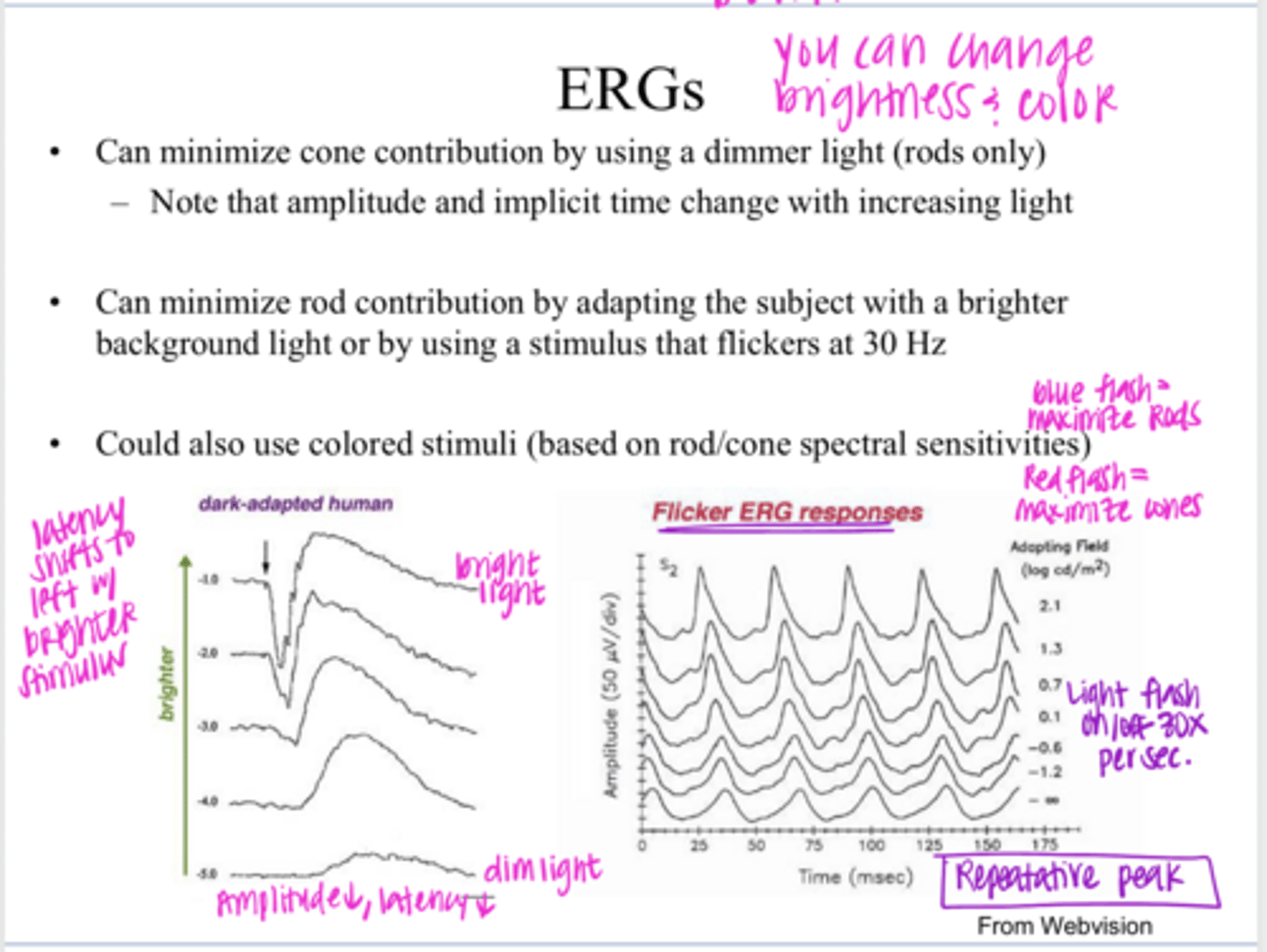
by adapting the patient with a brighter background light or by using a stimulus that flickers at 30Hz
How can we minimize rod contribution to an ERG (ie have a cone only response) by changing the brightness?
-Critical Duration of Rods: 100msec
-There are 10 100msec blocks in 1 second
-30Hz = rods cannot resolve this light because it is too fast; cones can resolve this
Why would a flicker at 30Hz stimulate a cone only response on ERG?
Yes
Could you use colored stimuli to get a cone or rod only response on ERGs?
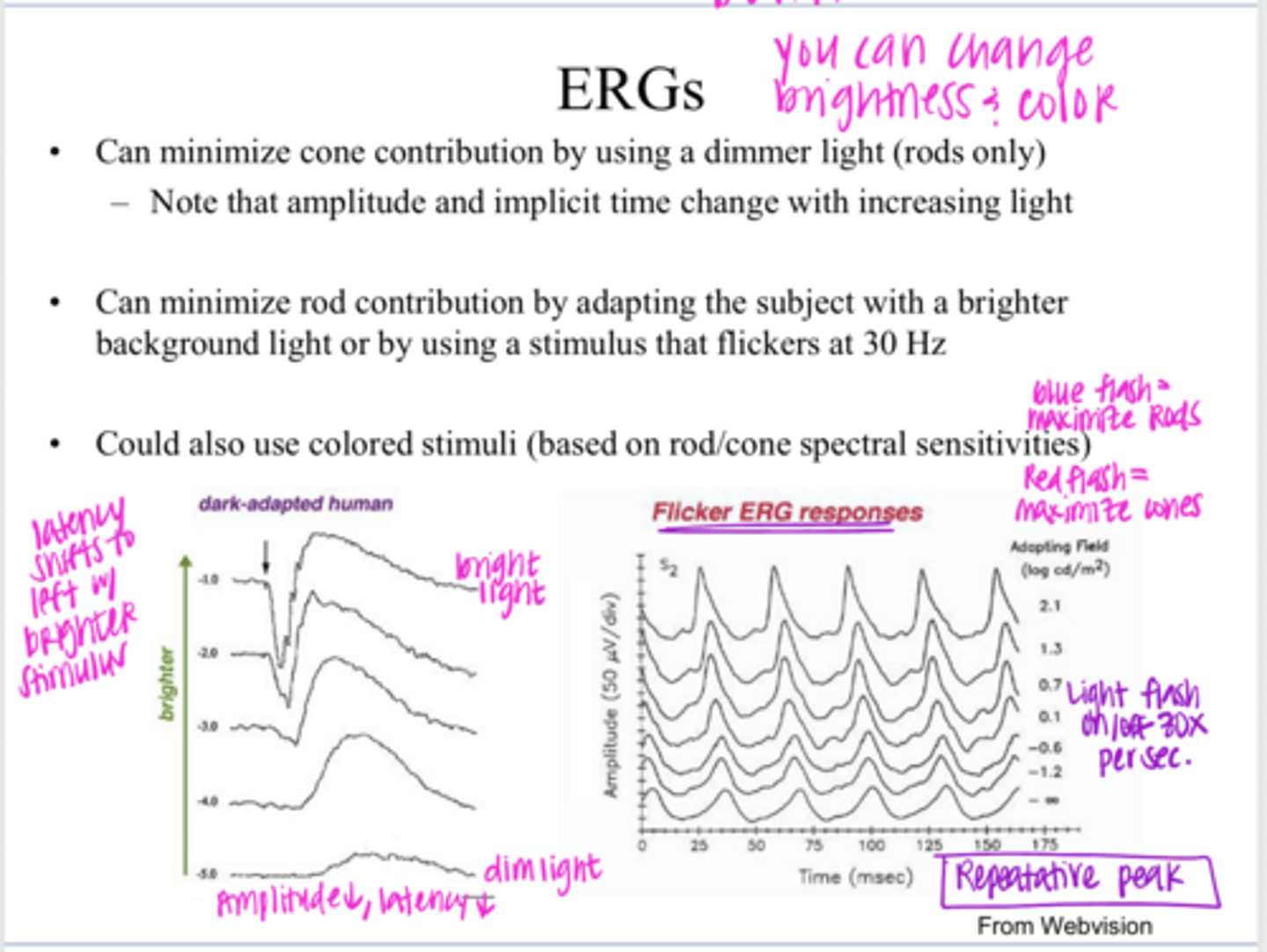
blue
What color stimulus could you use to get a rod only response on ERG?
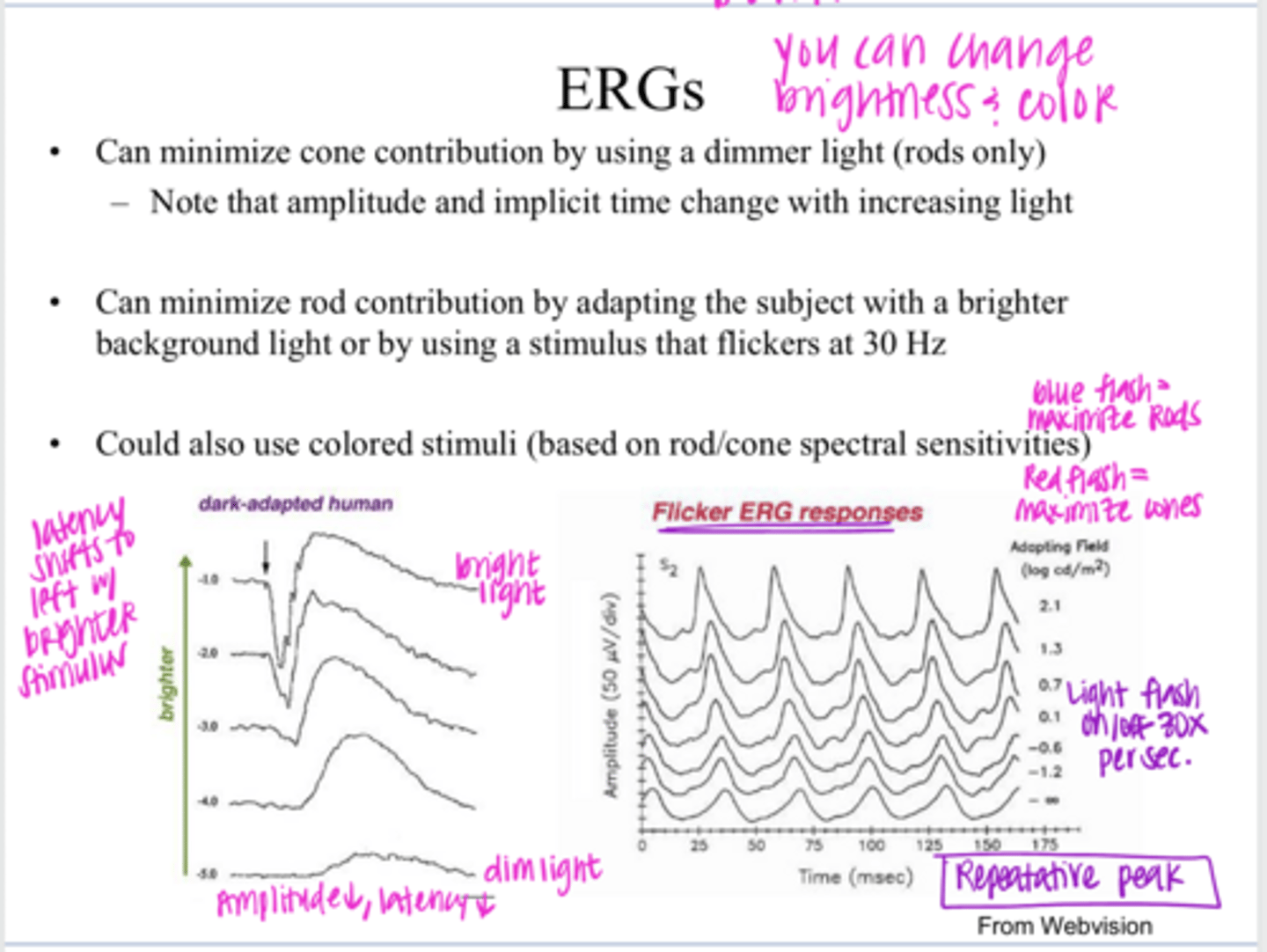
red
What color stimulus could you use to get a cone only response on ERG?
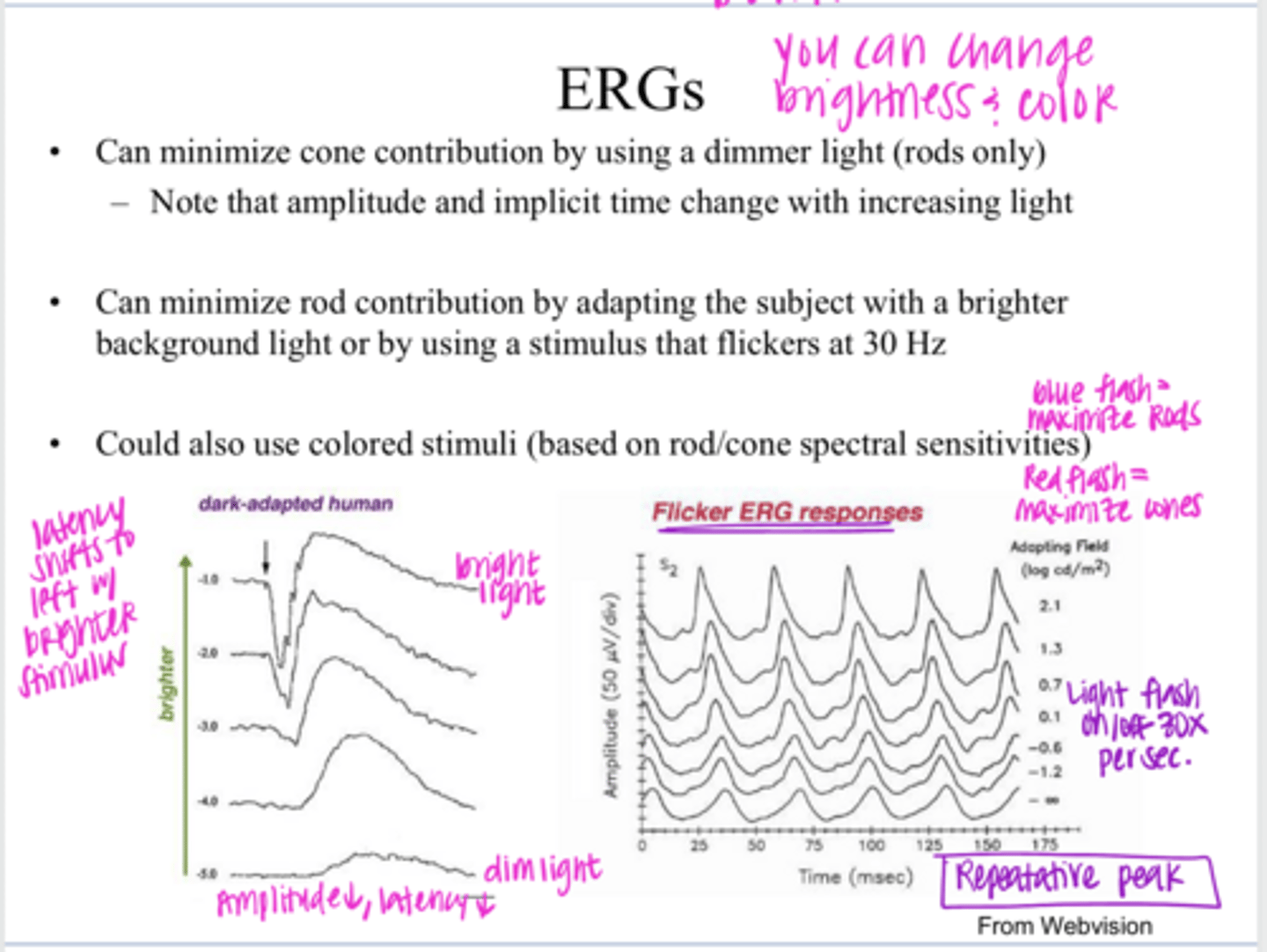
left
The latency of the b-wave will shift to the (right/left) with a brighter stimulus
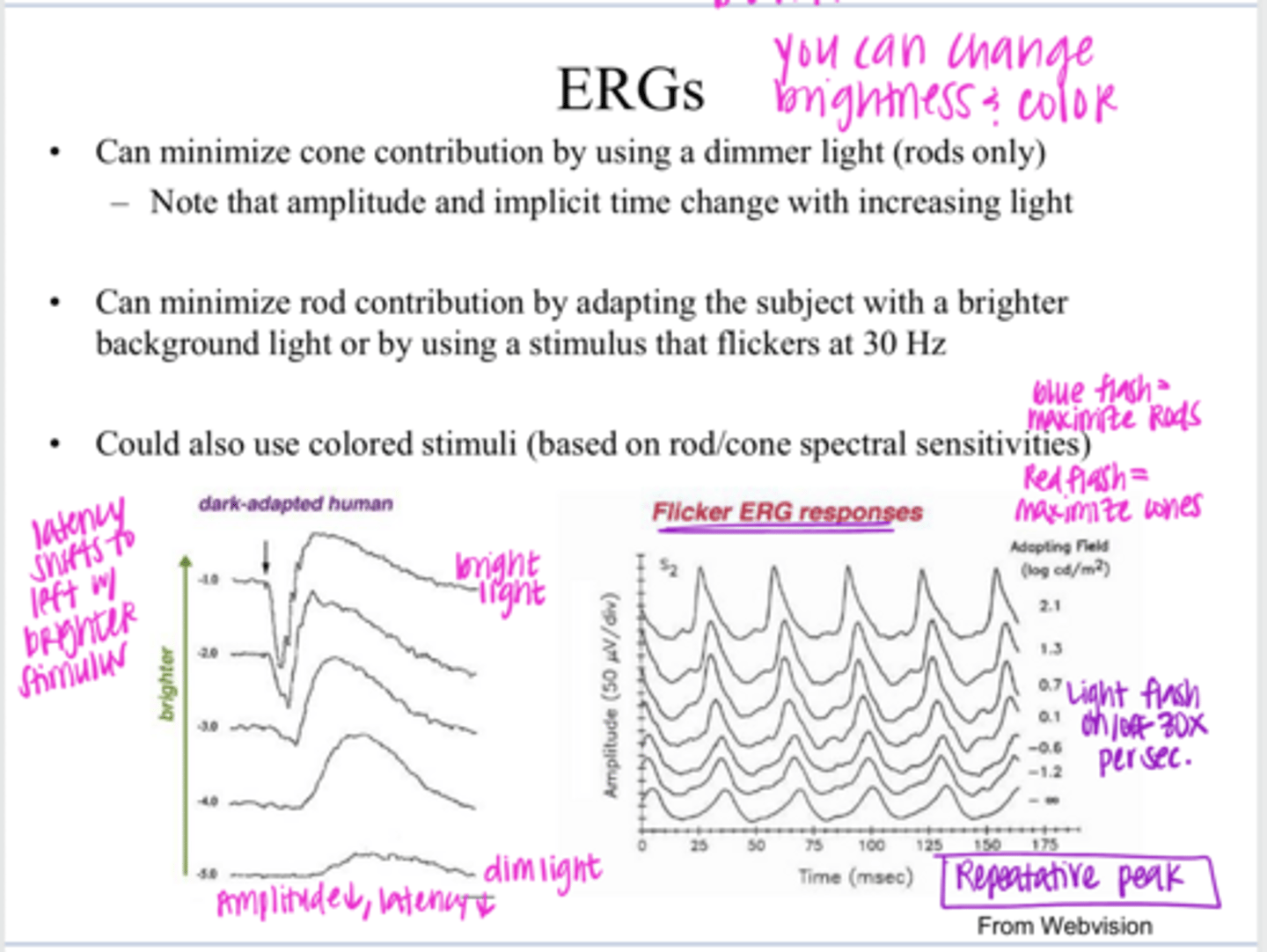
right
The latency of the b-wave will shift to the (right/left) with a dimmer stimulus
to the International Society for the Clinical Electrophysiology of Vision (ISCEV)
To achieve inter-clinic consistency, standardized stimuli (background and stimulus luminance, flicker frequency) should be used according to what?
-dilate pupils and dark adapt the patient for 30 min
-put electrode on under the dim red light
-use dim flash to get a rod response
-use a bright flash to get maximal (mixed) response
-increase background luminance to suppress rods and to get a cone response to a single flash
-get flicker response at 30Hz
What are the standards to use when running an ERG?
yes
Is it possible to use more specialized protocol and look for waveforms in the ERG that occur after the A and B waves to isolate out function of inner retina?
to look at issues that affect the outer retina, and in particular, issues that affect MOST or ALL of the outer retina
**hereditary diseases like retinitis pigmentosa
In general clinical testing, full-field ERGs are used for what?
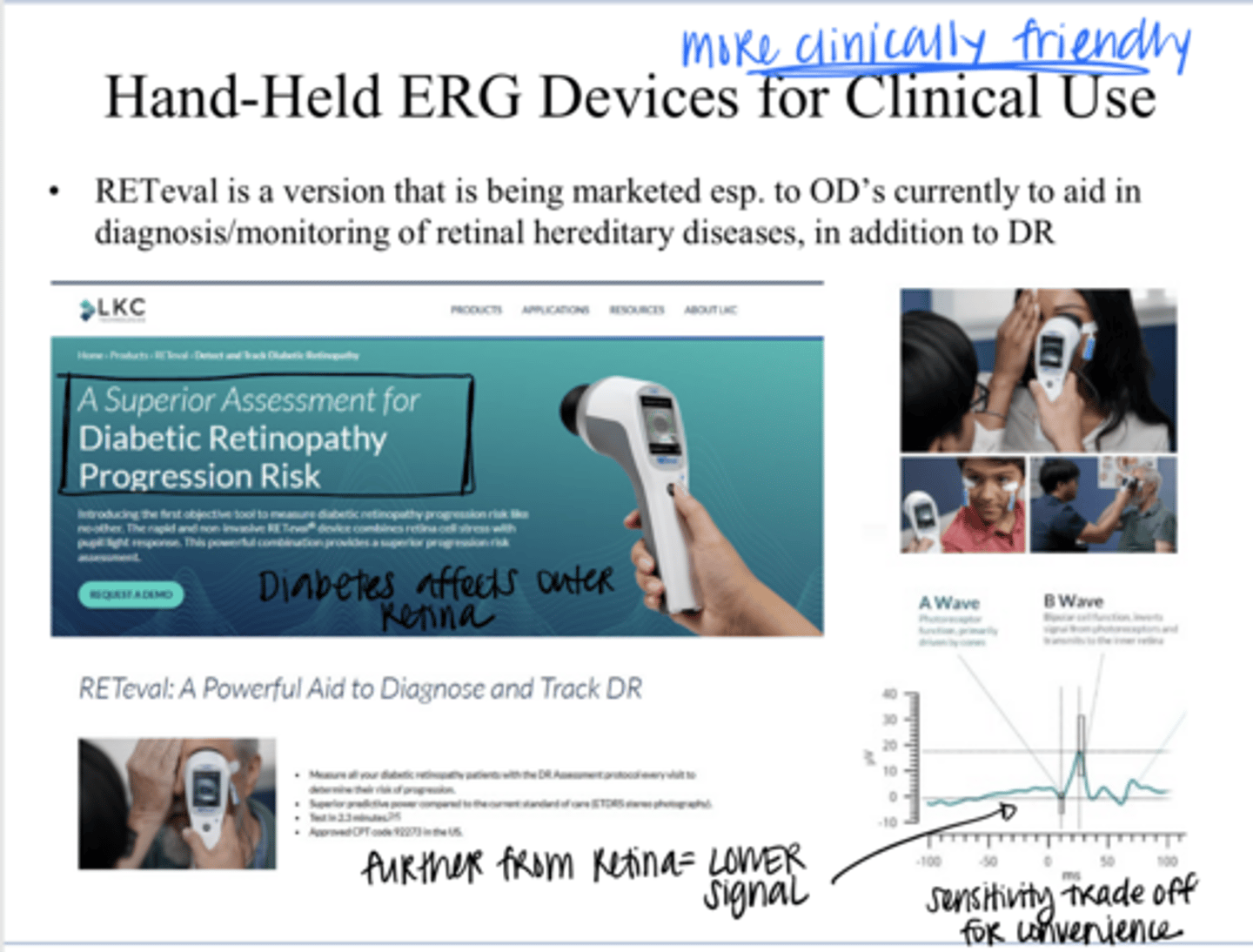
RETeval (Hand-Held ERG Device)
_______ is a version of the ERG that is being marketed to ODs currently to aid in diagnosis/monitoring of retinal hereditary diseases
flashes of light
What do ERGs utilize to illuminate the whole retina?
"full-field" ERG
When a ERG uses flashes of light to illuminate the WHOLE RETINA, it is termed what?
overall retinal activity
What does a "full-field" ERG give a measure of?
picking up more focal defects
What is a "full-field" ERG not very good at?
uses a small flash of light in a confined macular region
What is a modified focal ERG?
Yes
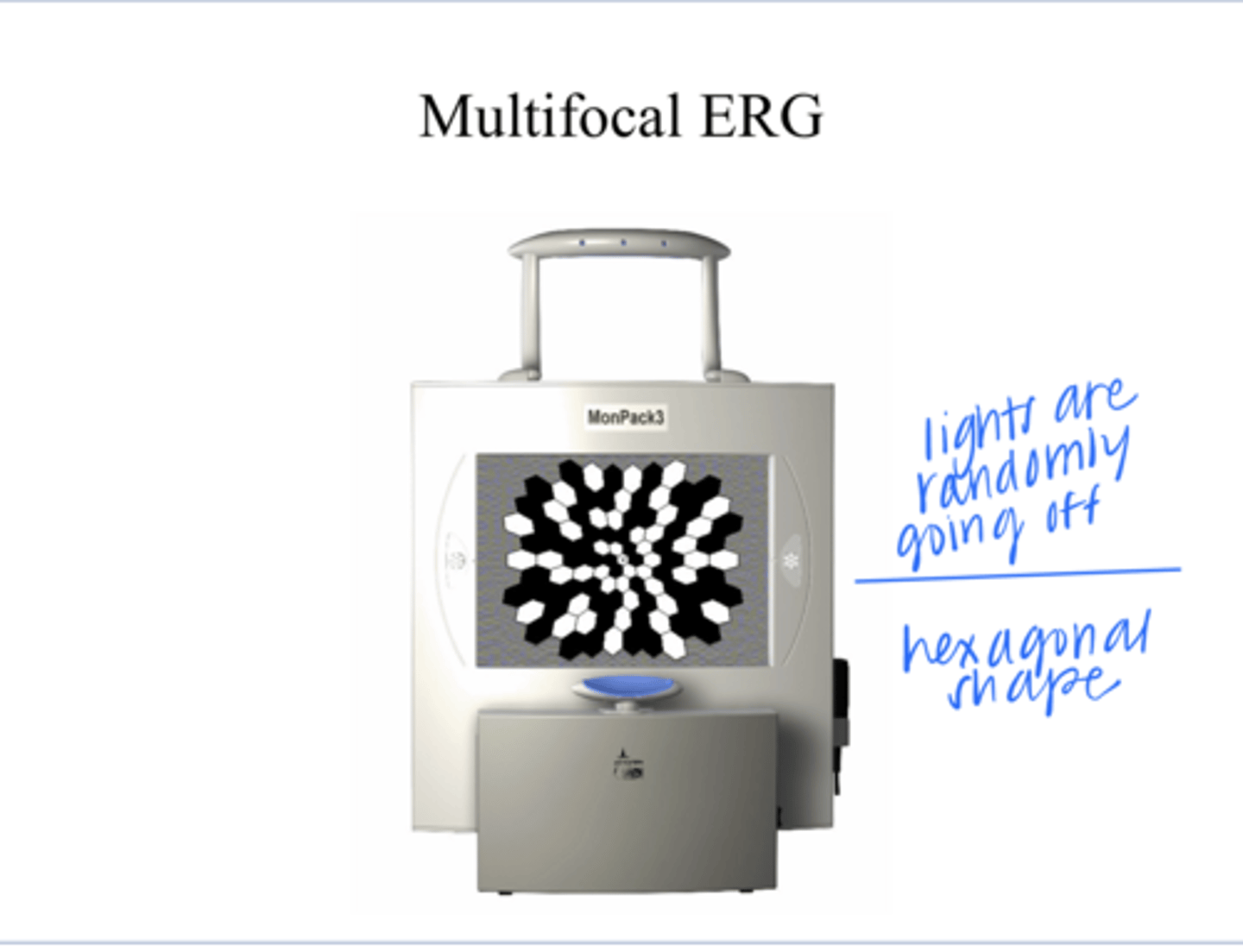
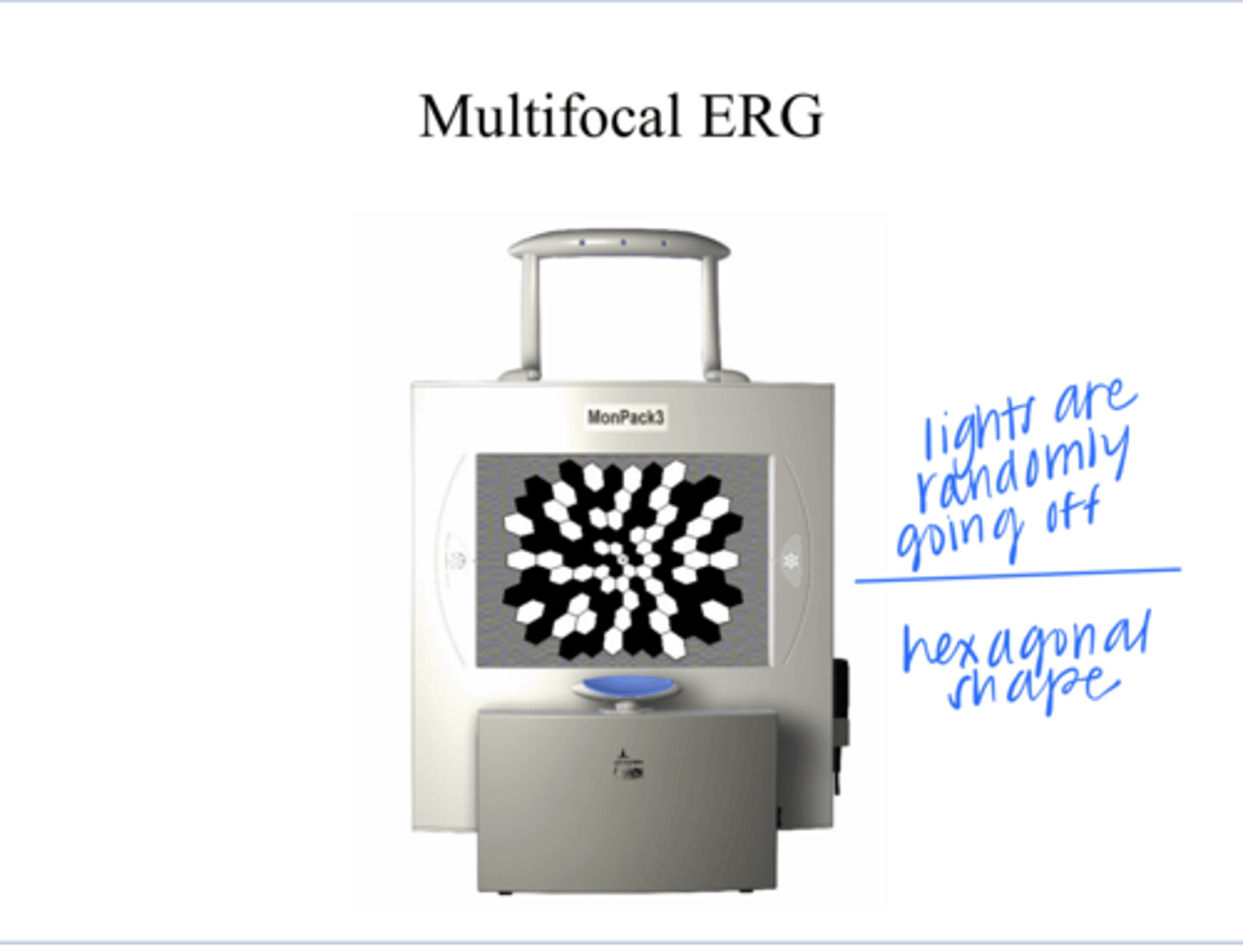
Has a multi-focal ERG been developed in which an algorithm sorts out the ERG for the corresponding retinal areas that are stimulated by each area?
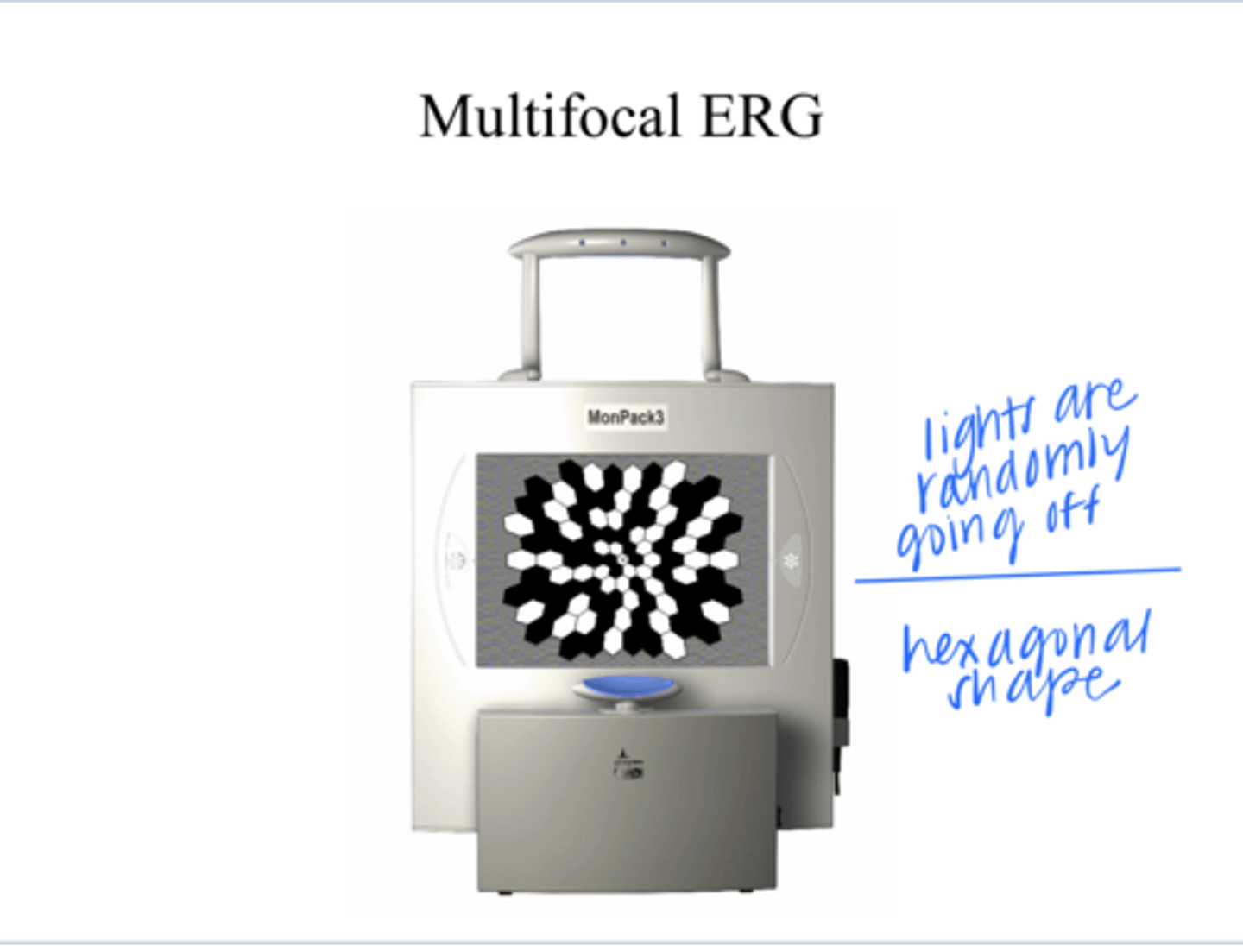
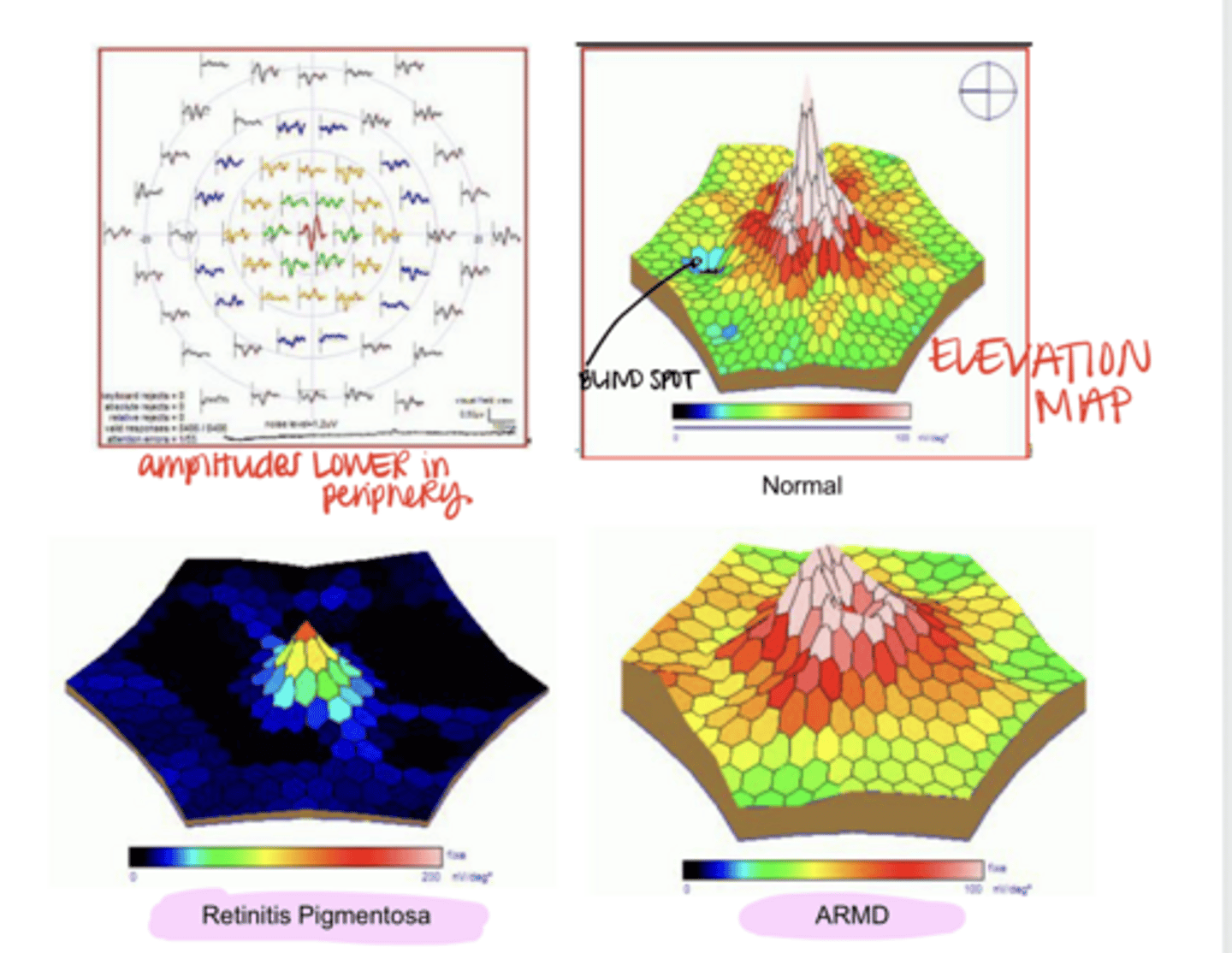
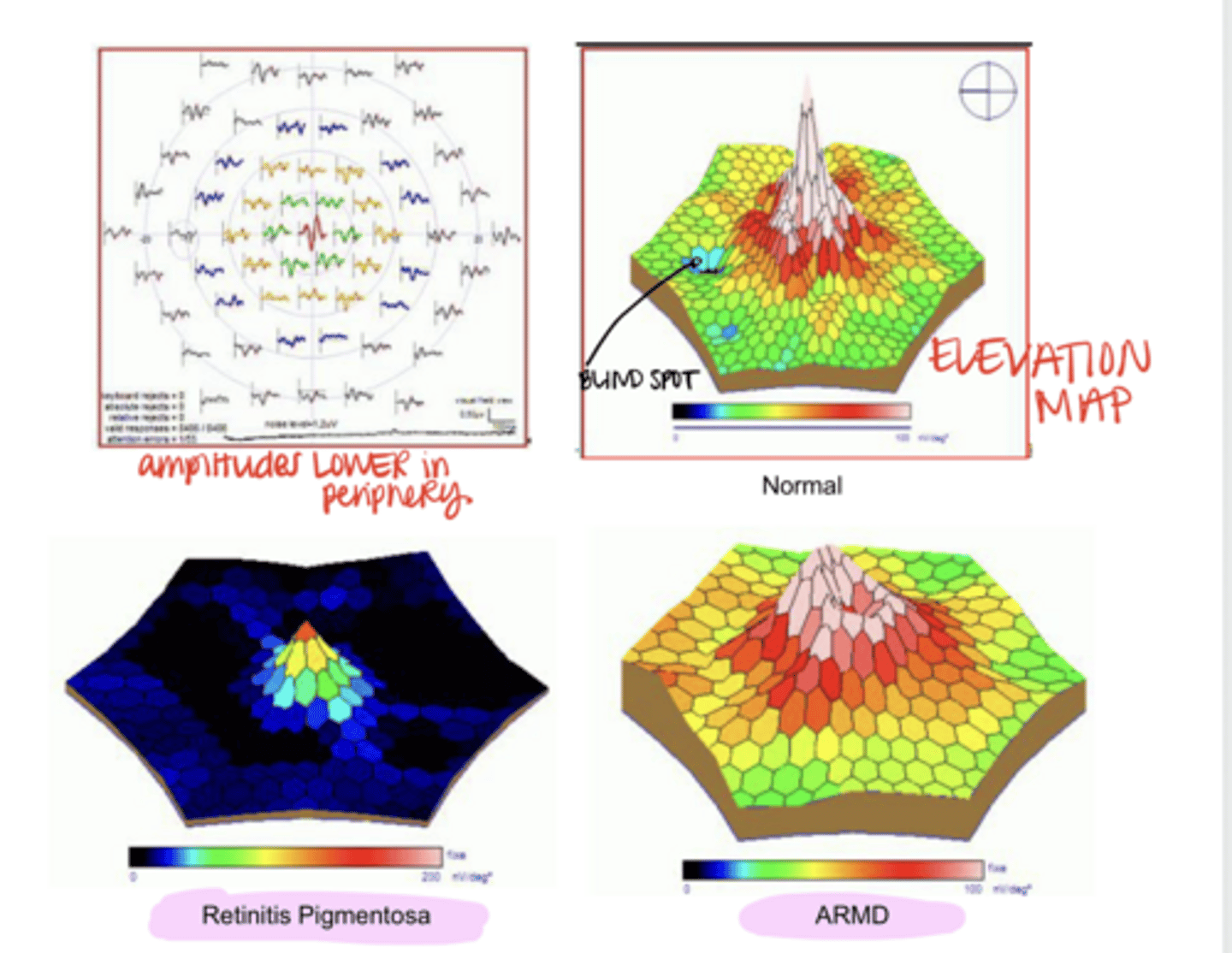
Multifocal ERG (Pic)
Multifocal ERG (Pic)
Multifocal ERG Results that Reflect Activity in the Retina (Pic)
Multifocal ERG Results that Reflect Activity in the Retina (Pic)
**not measured electrical responses
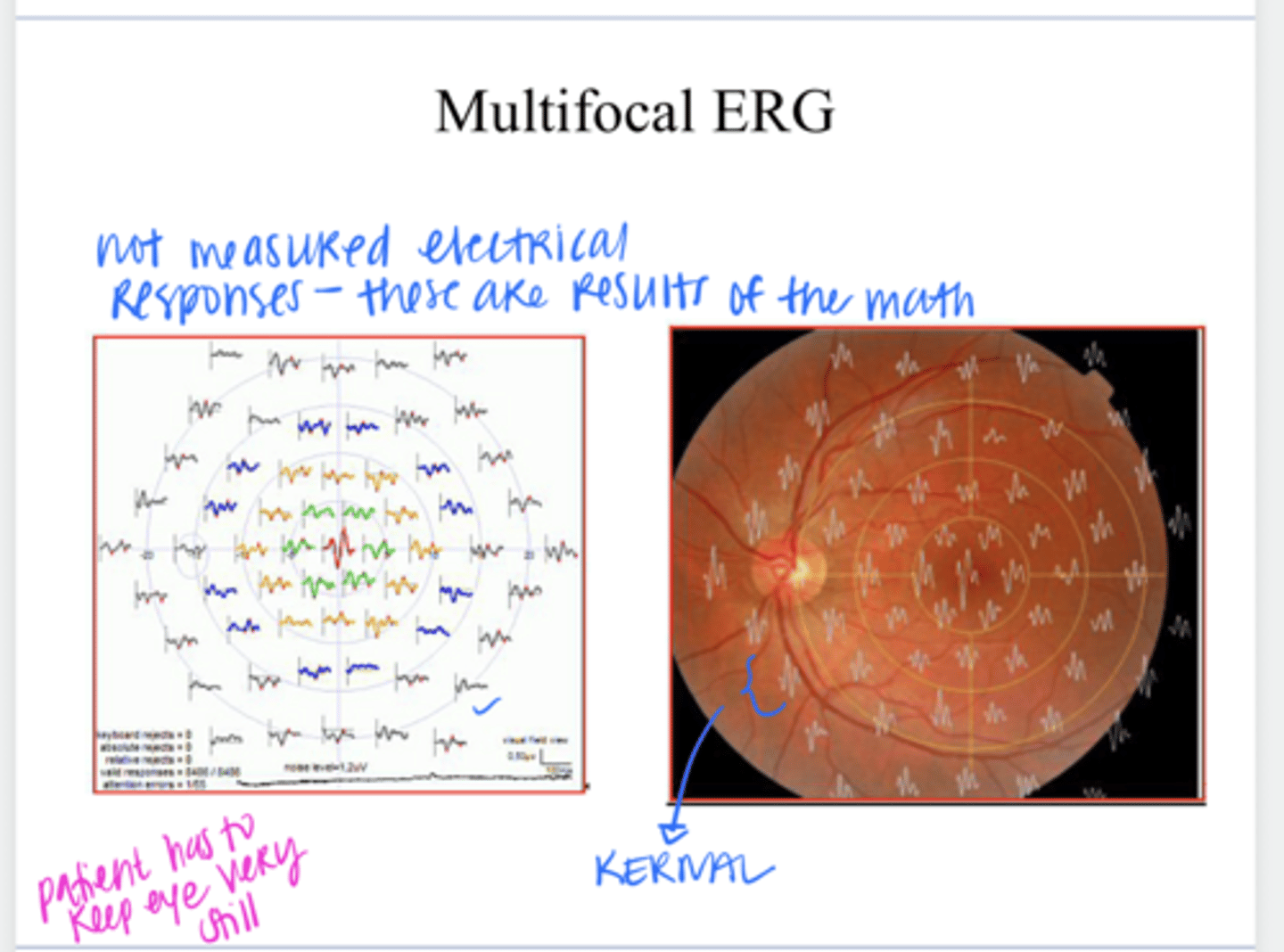
Multifocal ERG Results that Reflect Activity in the Retina (Pic)
Multifocal ERG Results that Reflect Activity in the Retina (Pic)
No -- they are mathematically derived waveforms found by pooling and subtracting out all the hundreds of recordings that were done while the subject was looking at the flicking hexagonal patterns
Are the waveforms that are generated by the mfERG of multi-focal ERG actual direct electrical recordings?
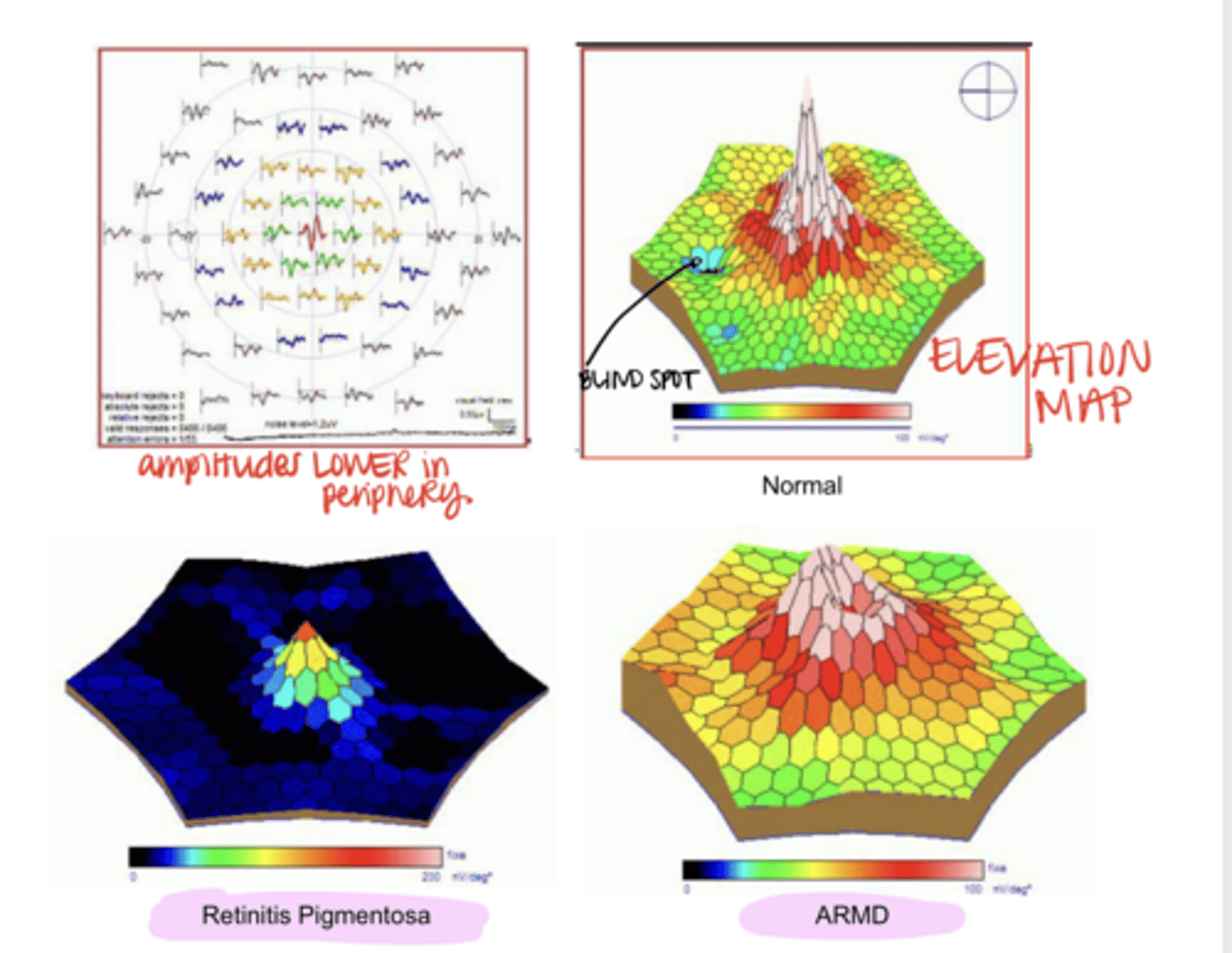
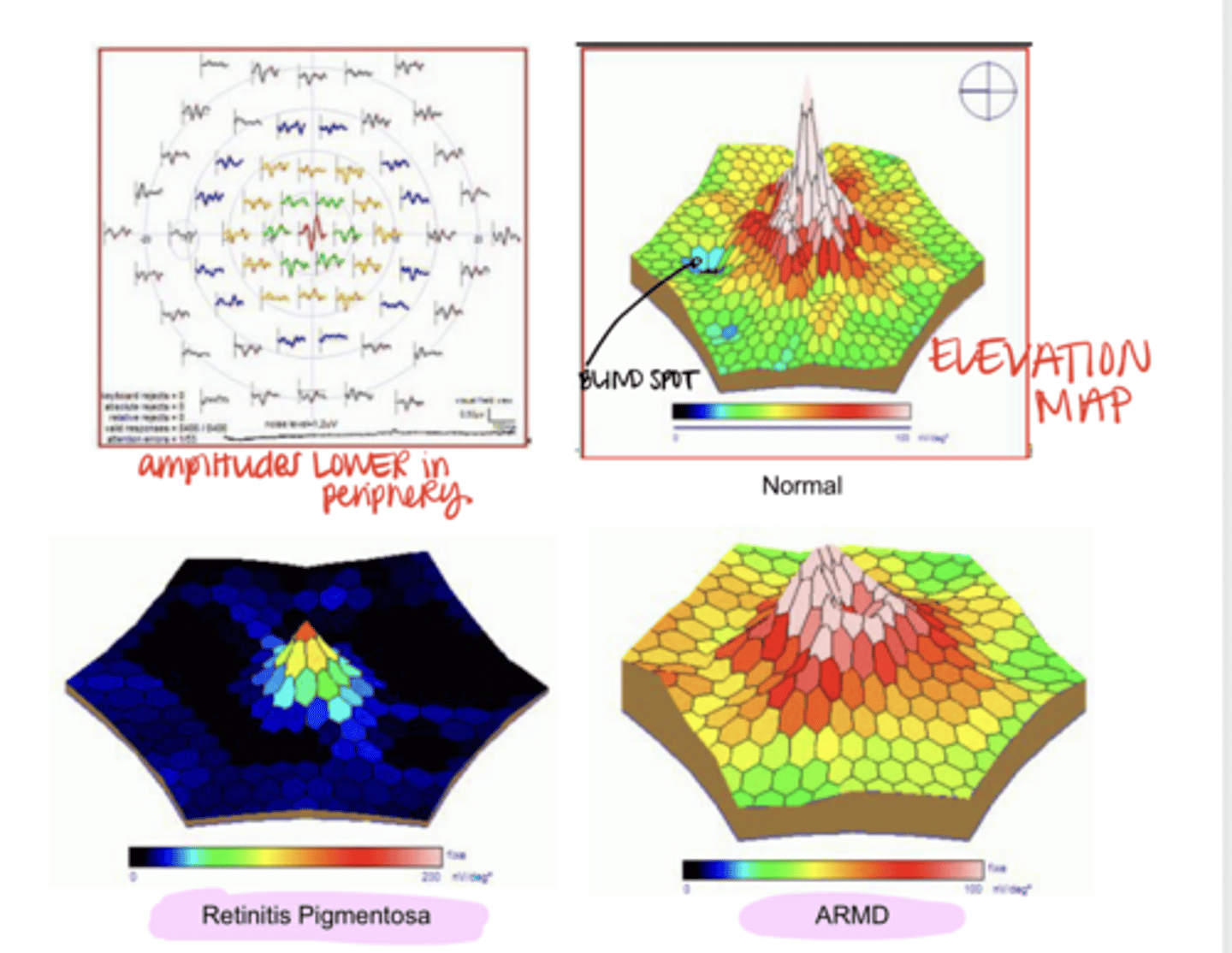
it allows localized functional deficits in the retina to be uncovered
What is the advantage of mulit-focal ERG?
requires the patient to have minimal eye movements during the recordings
What does a multi-focal ERG require?
to assist in the diagnosis of hereditary and choroidal disease (and to monitor progression)
Visual electrodiagnostic tests (EOG and ERG) are used clinically and are used primarily to do what?
ERG is used more
Which is used more, EOG or ERG?
for diagnosis of Best's Disease (vitelliform dystrophy)
What is the EOG useful for?
autosomal dominant -- although sometimes penetrance is incomplete & the patient will be a carrier
Best's Disease has ______ inheritance
Yes
Will EOG be abnormal prior to the clinical onset of Best's disease?
Yes
Will EOG be abnormal in adult carriers of Best's disease?
No -- it will often be normal
Will ERG be abnormal in adult carriers of Best's disease?
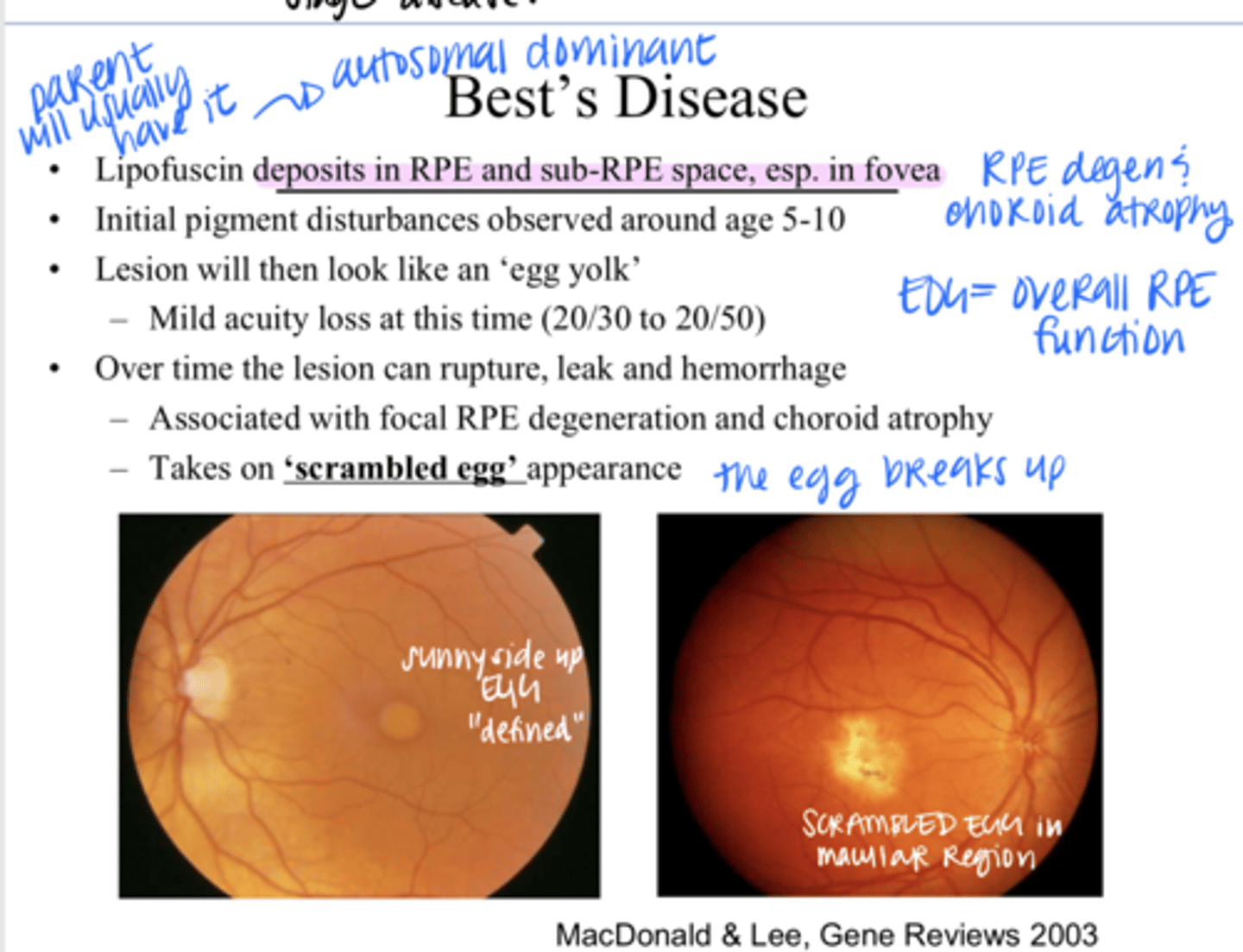
Lipofuscin deposits in RPE and sub-RPE space, esp in the fovea
What happens in Best's Disease?
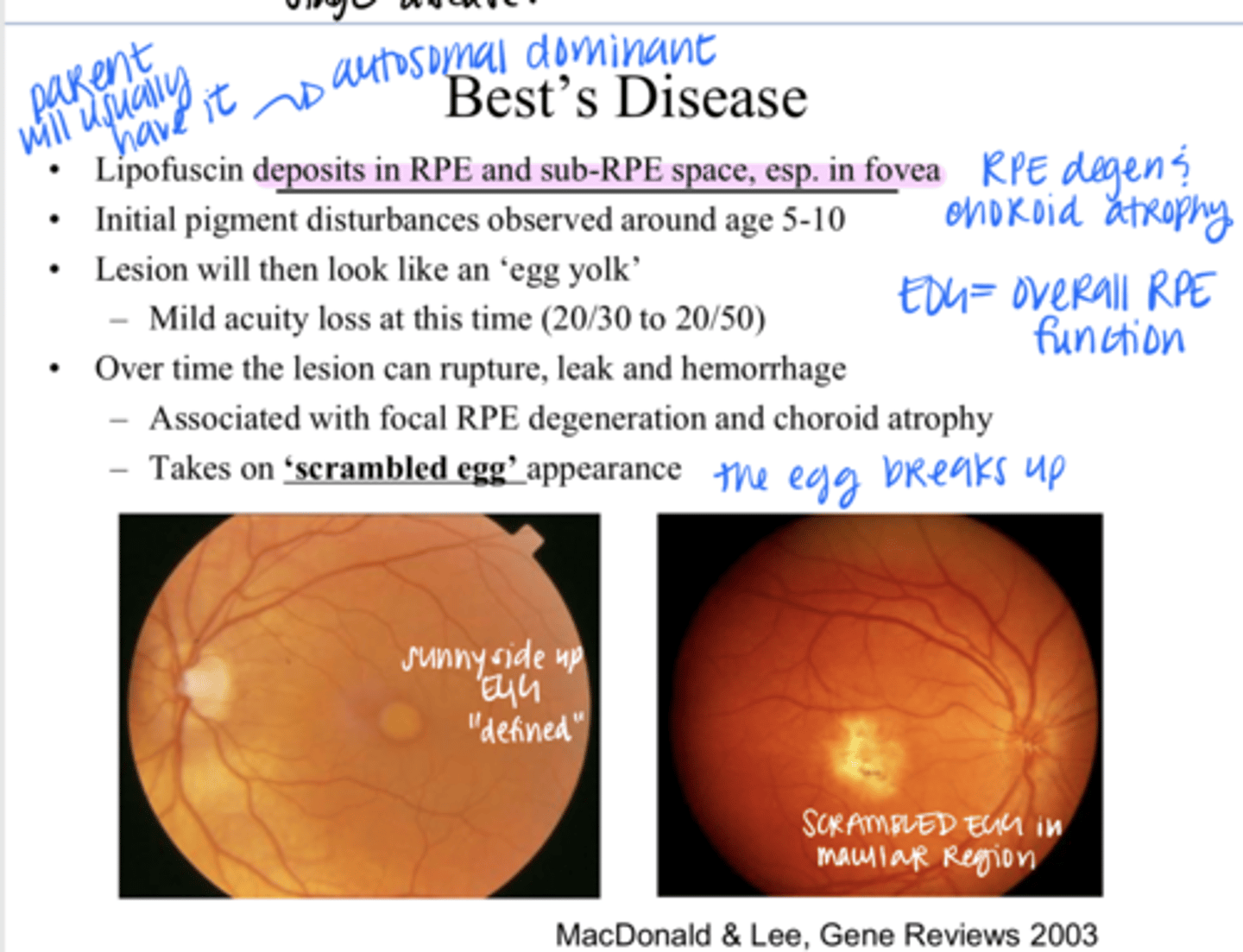
Best's Disease
Initial pigment disturbances in Best's Disease are observed around age 5-10?
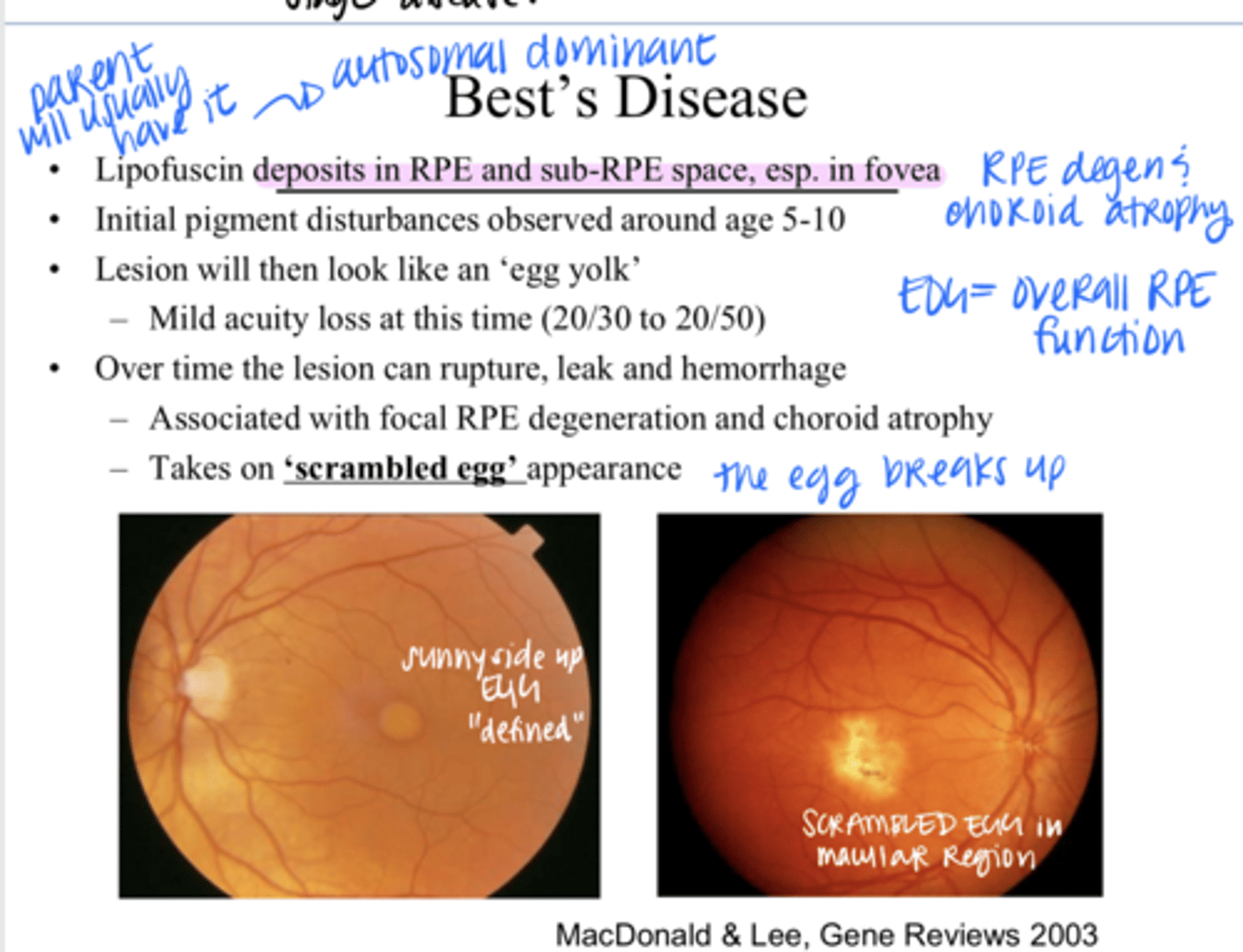
egg yolk
What will the lesions in Best's Disease look like?
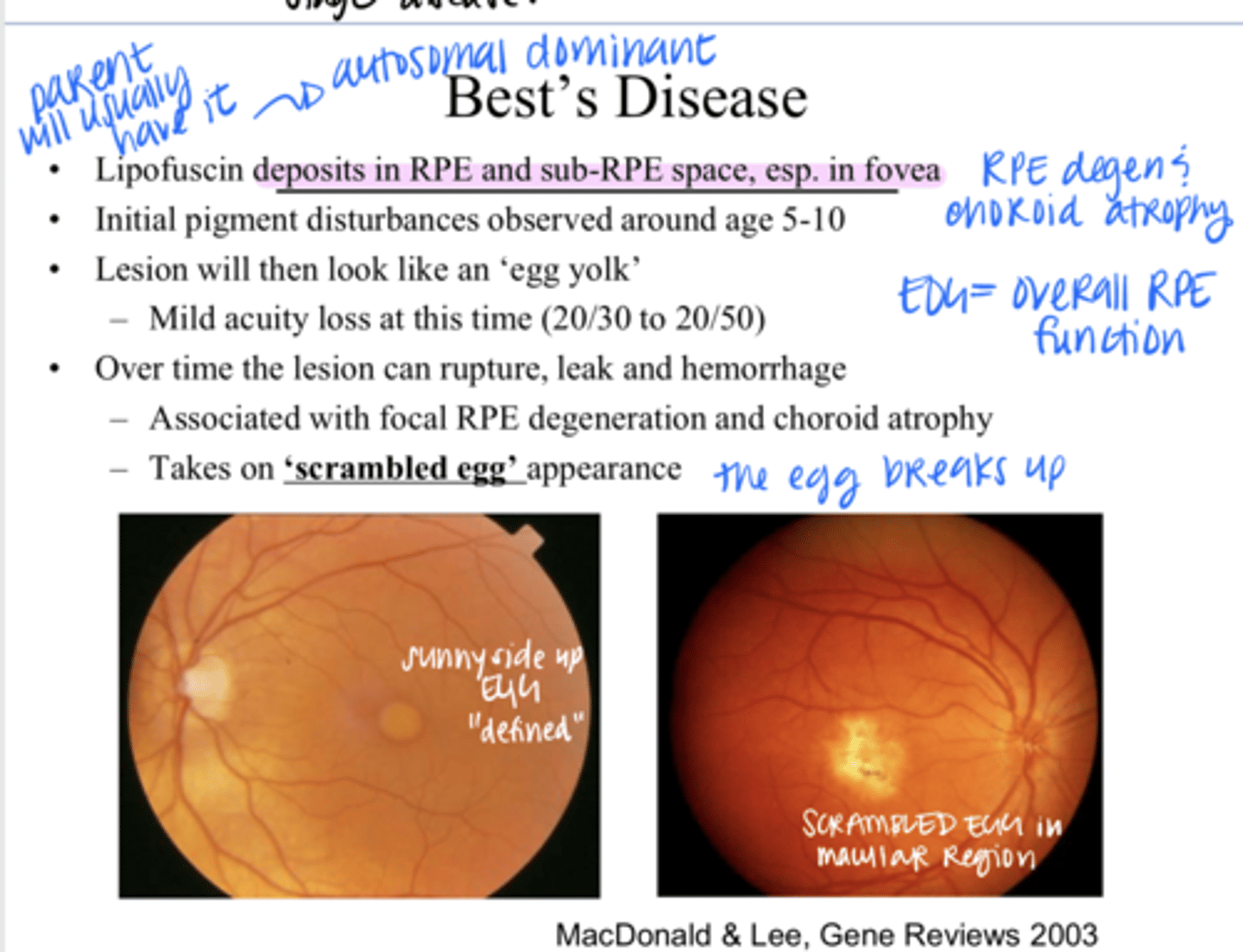
20/30 - 20/50
When there is an egg yolk, what is the visual acuity loss at this time?
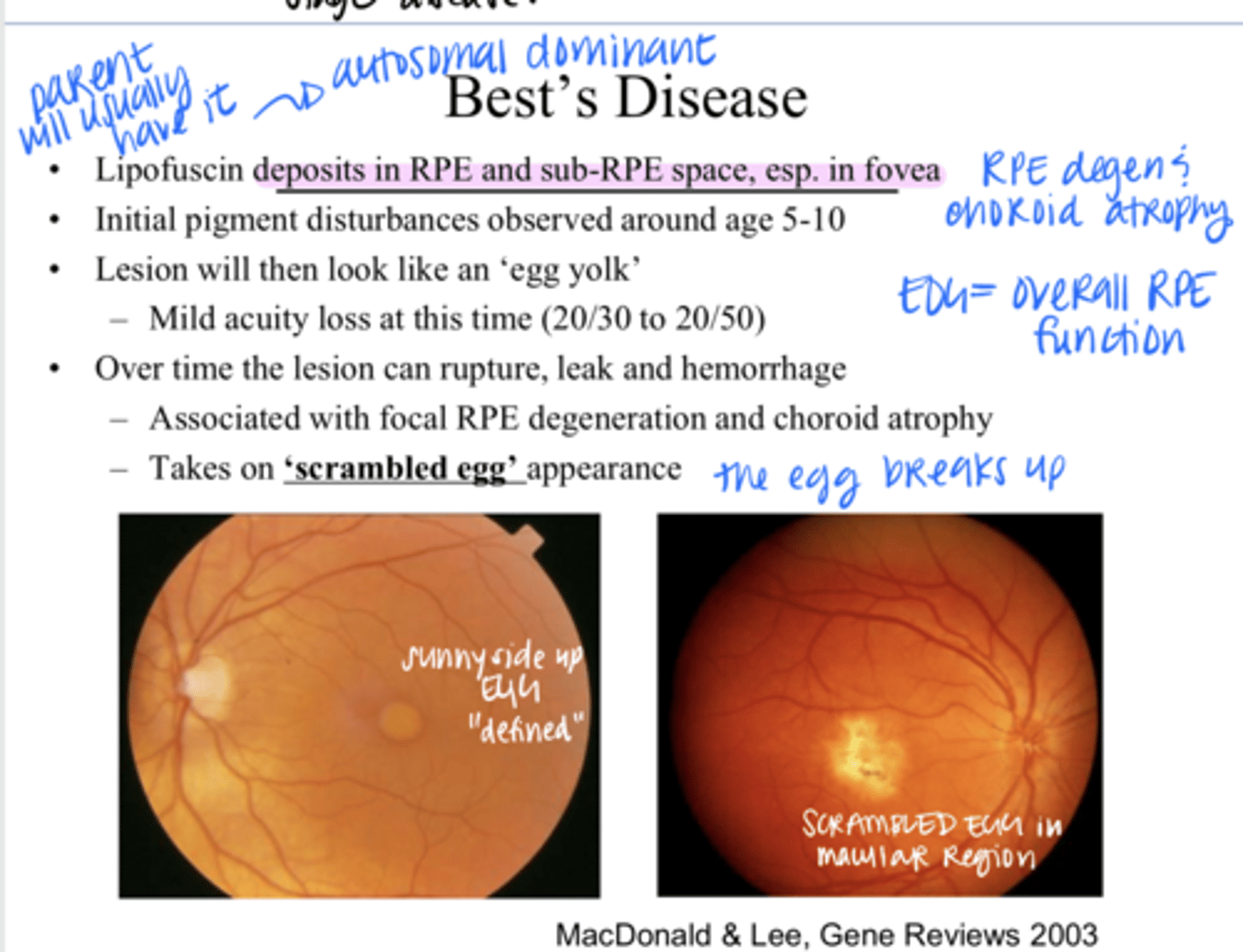
rupture, leak, hemorrhage
Over time the lesion of Best's Disease will do what?
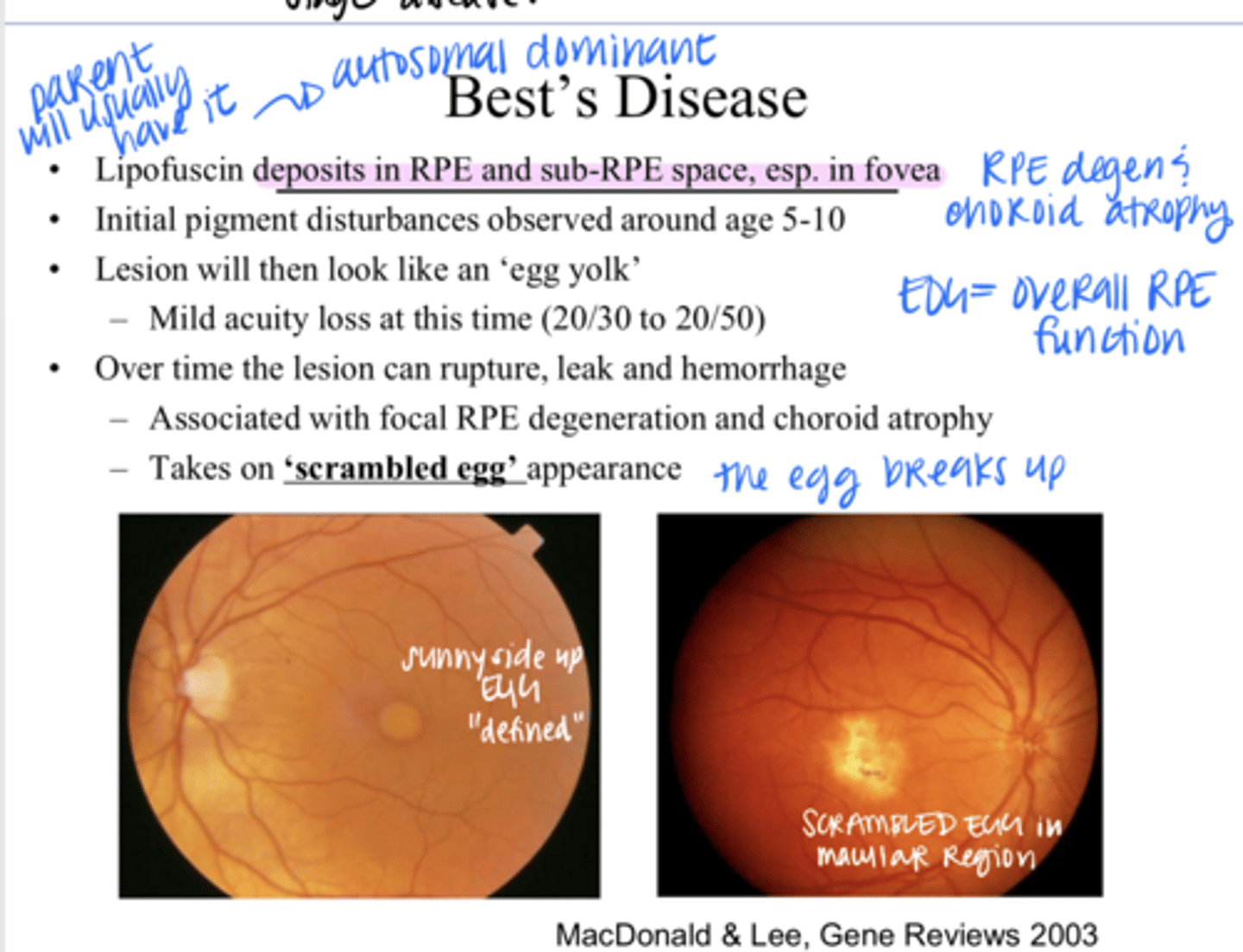
focal RPE degeneration, choroid atrophy
What is Best's Disease associated with?
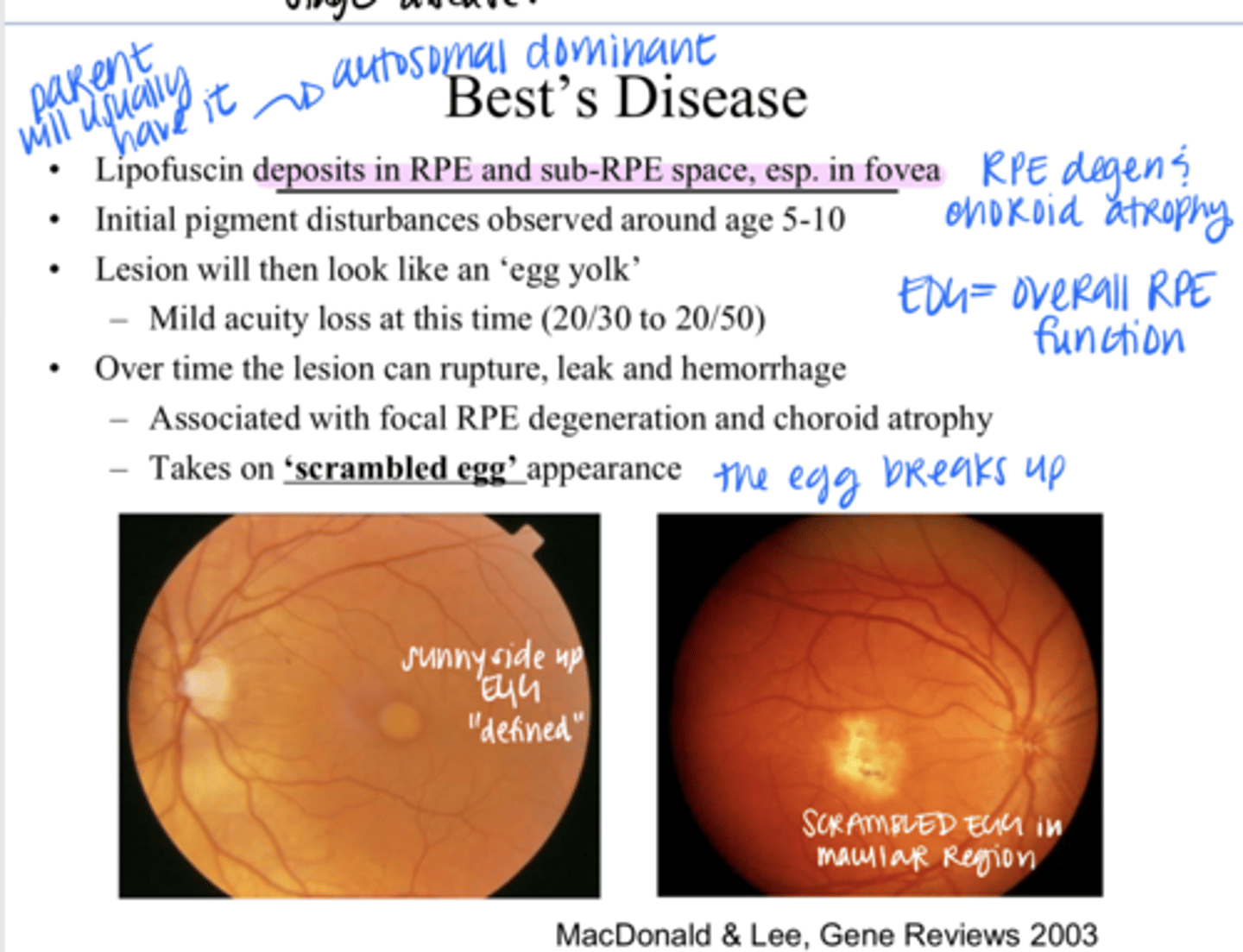
scrambled egg
Over time, the "egg yolk" appearance of Best's Disease will take on a _____ appearance?
nomral
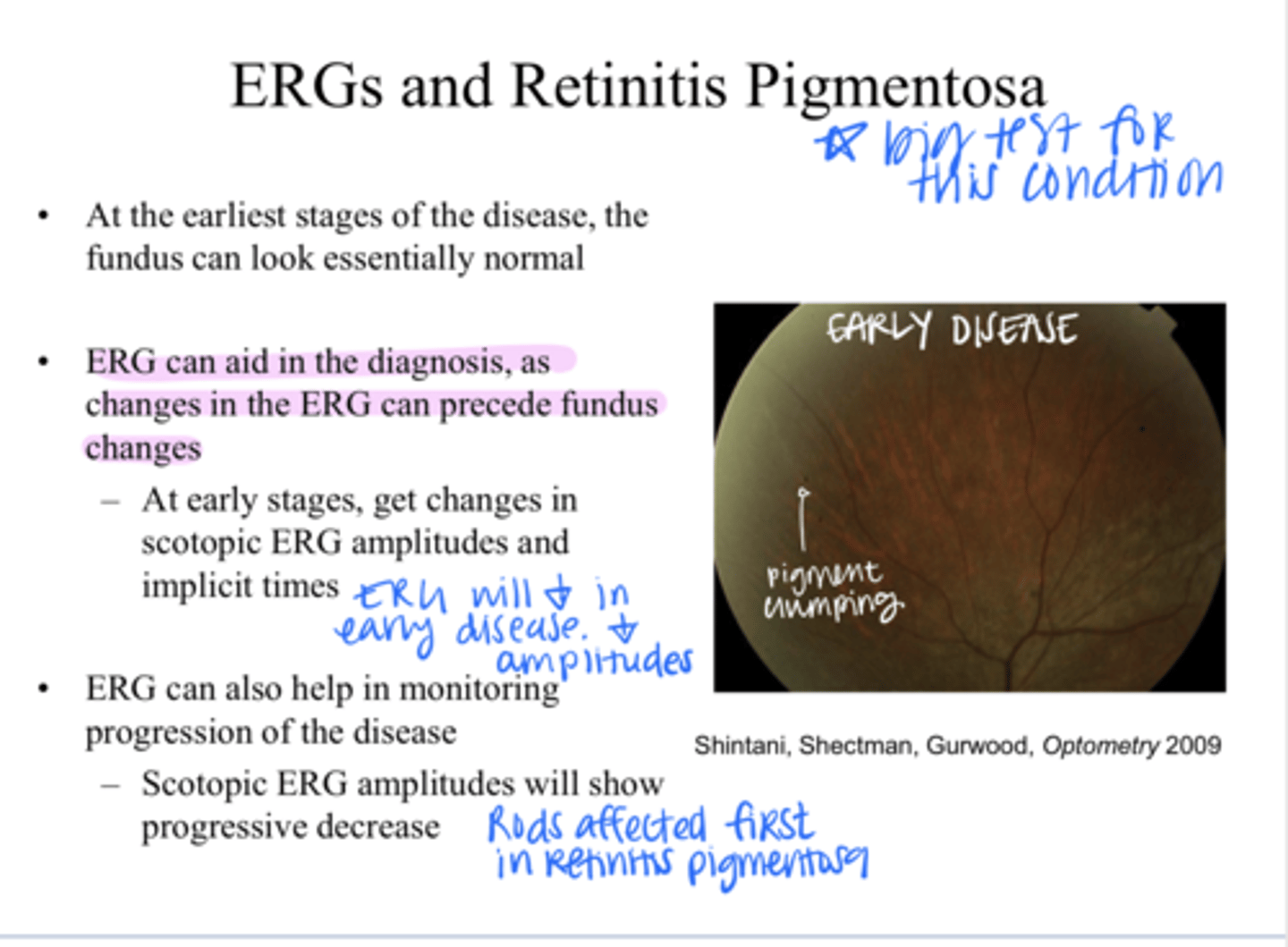
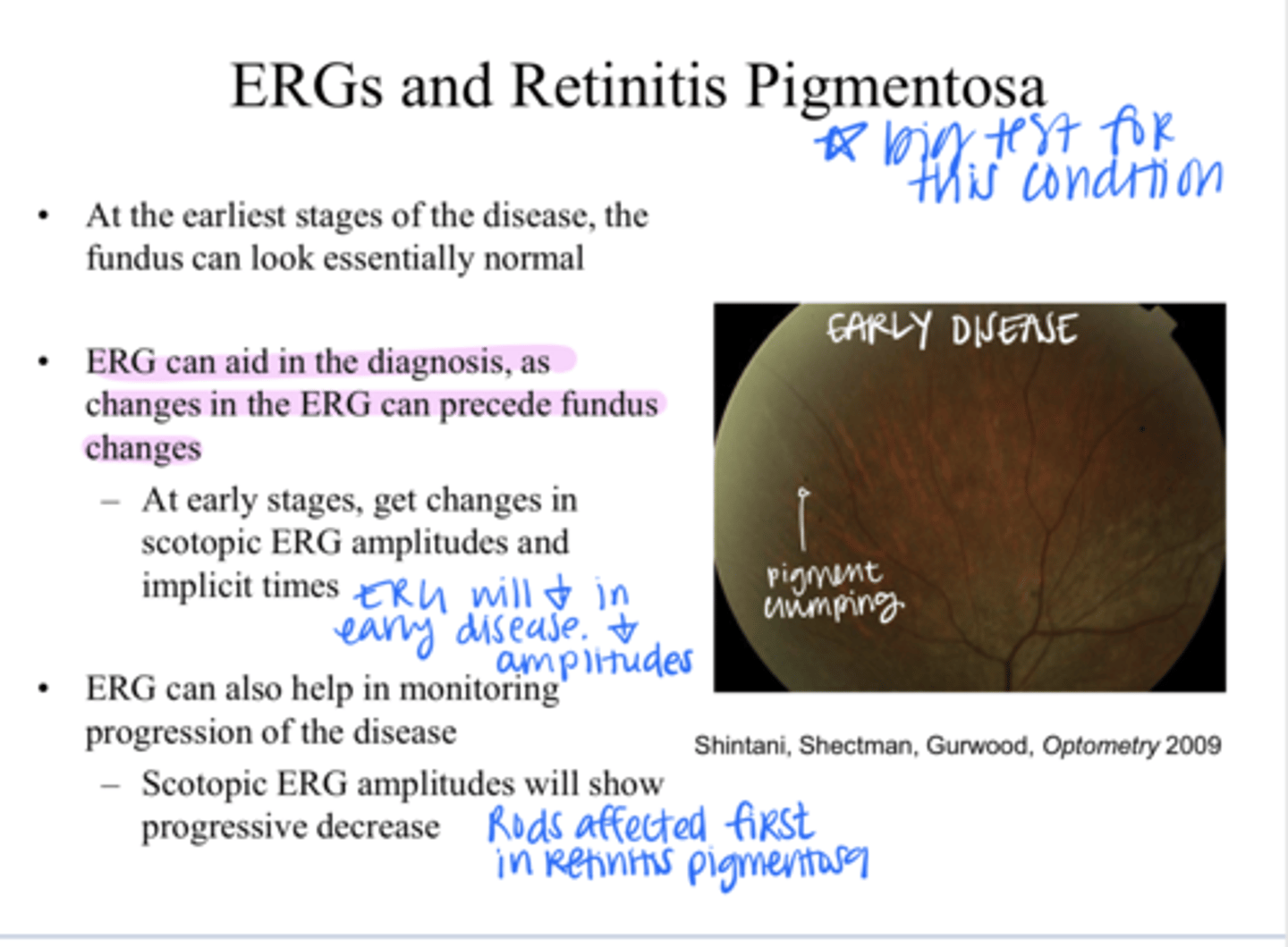
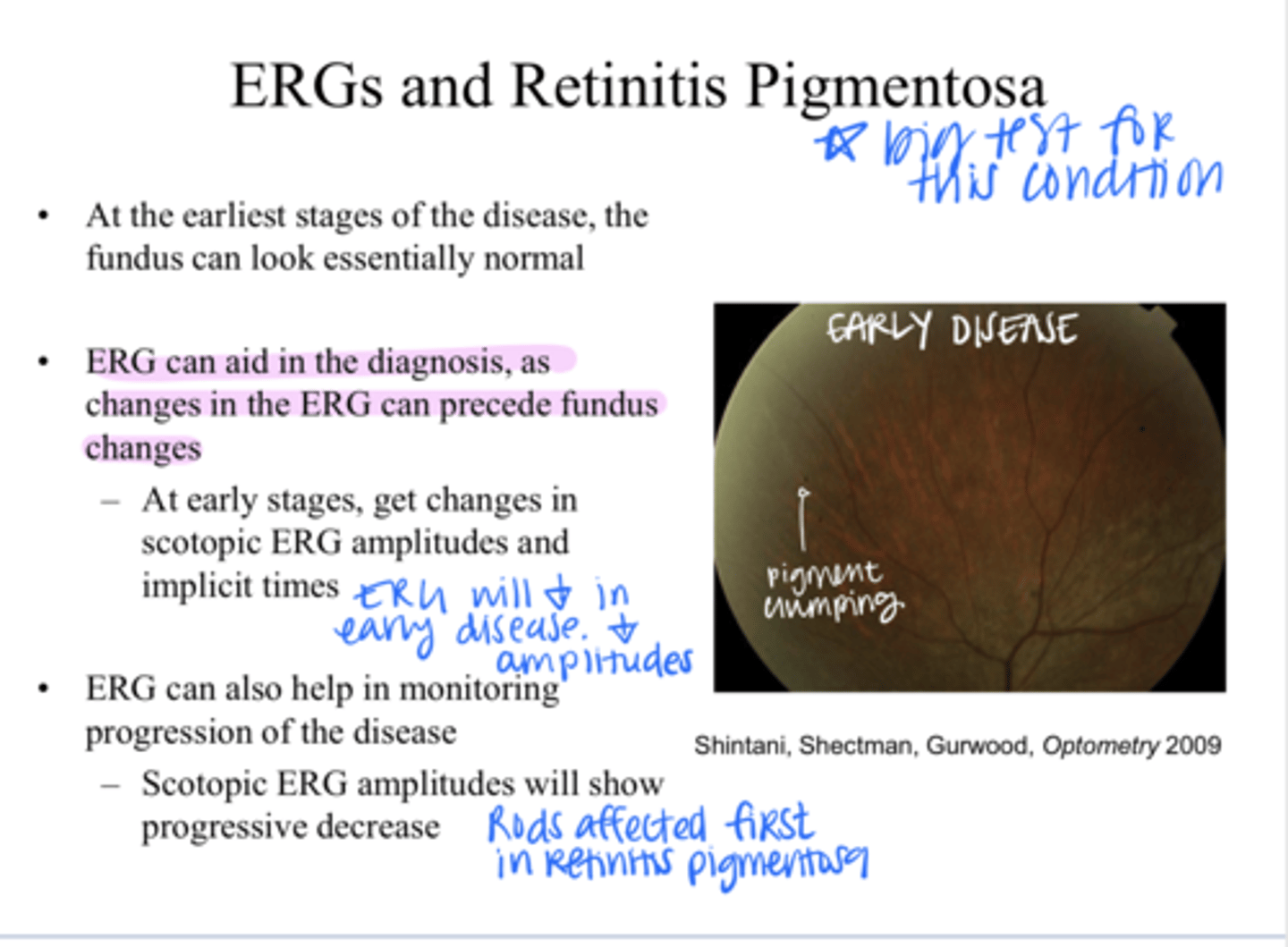
What does the fundus look like at the earliest stage of retinitis pigmentosa?
Yes -- measurement of the integrity of photoreceptors
Can ERGs aid in the diagnosis of rretinitis pigmentosa?
Yes
Can changes in the ERG precede fundus changes of retinitis pigmentosa?
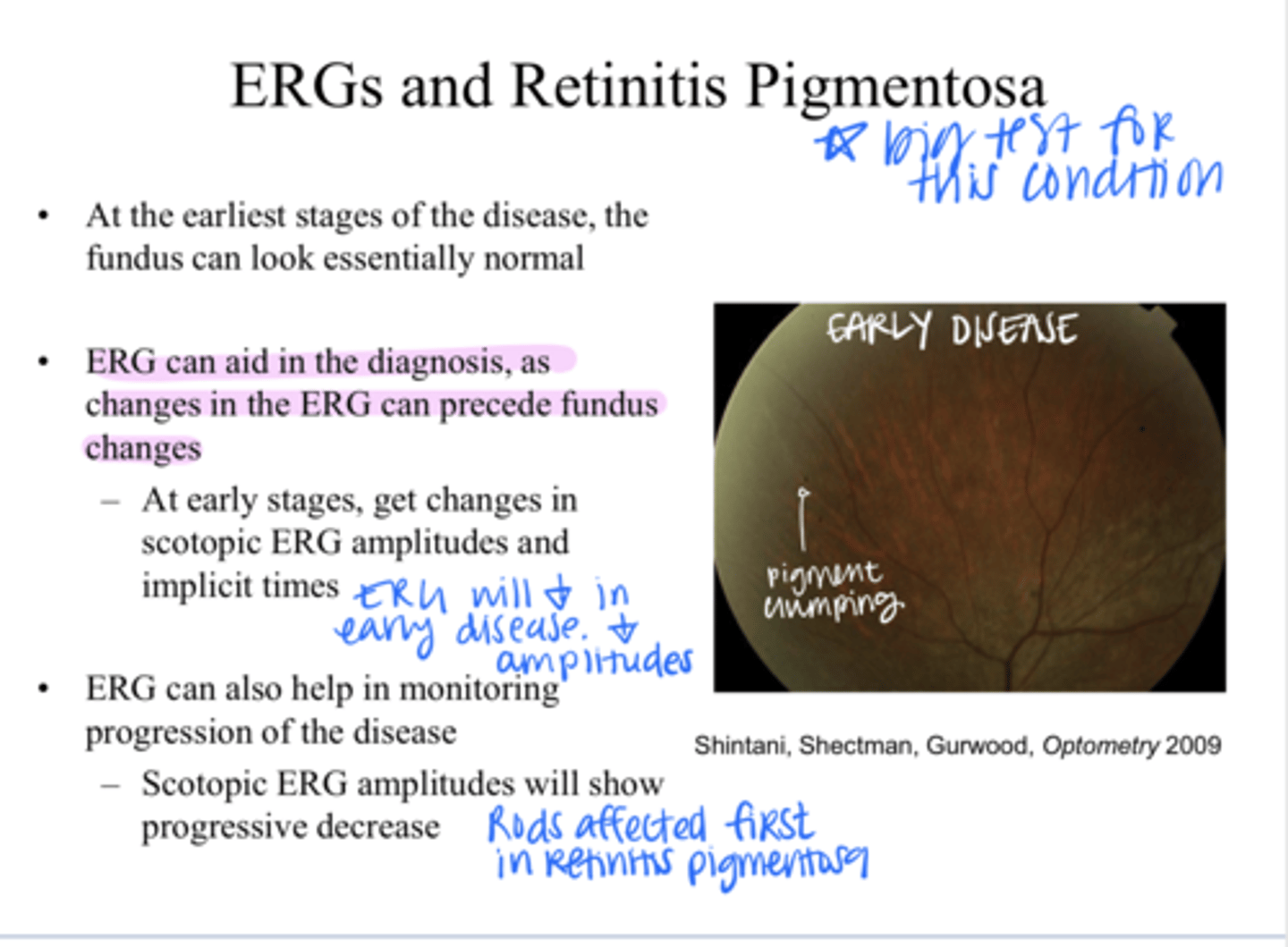
Get changes in scotopic ERG amplitudes and implicit times
What are the 1st changes on the ERG that can be detected in patients with macular degeneration?
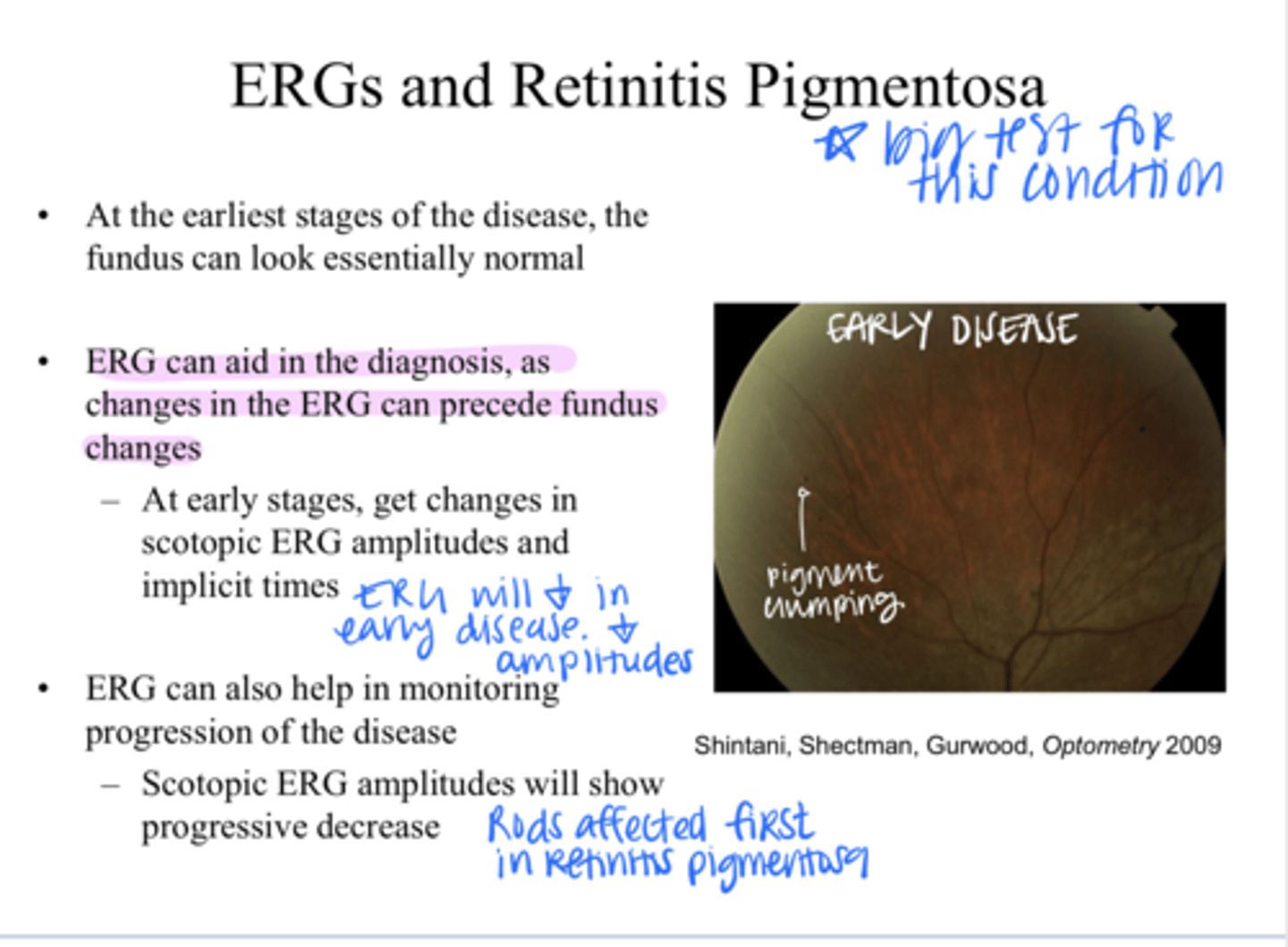
Scotopic -- the rods will be affected first usually
(scotopic/Photopic) ERG amplitudes will show progression of the retinitis pigmentosa disease
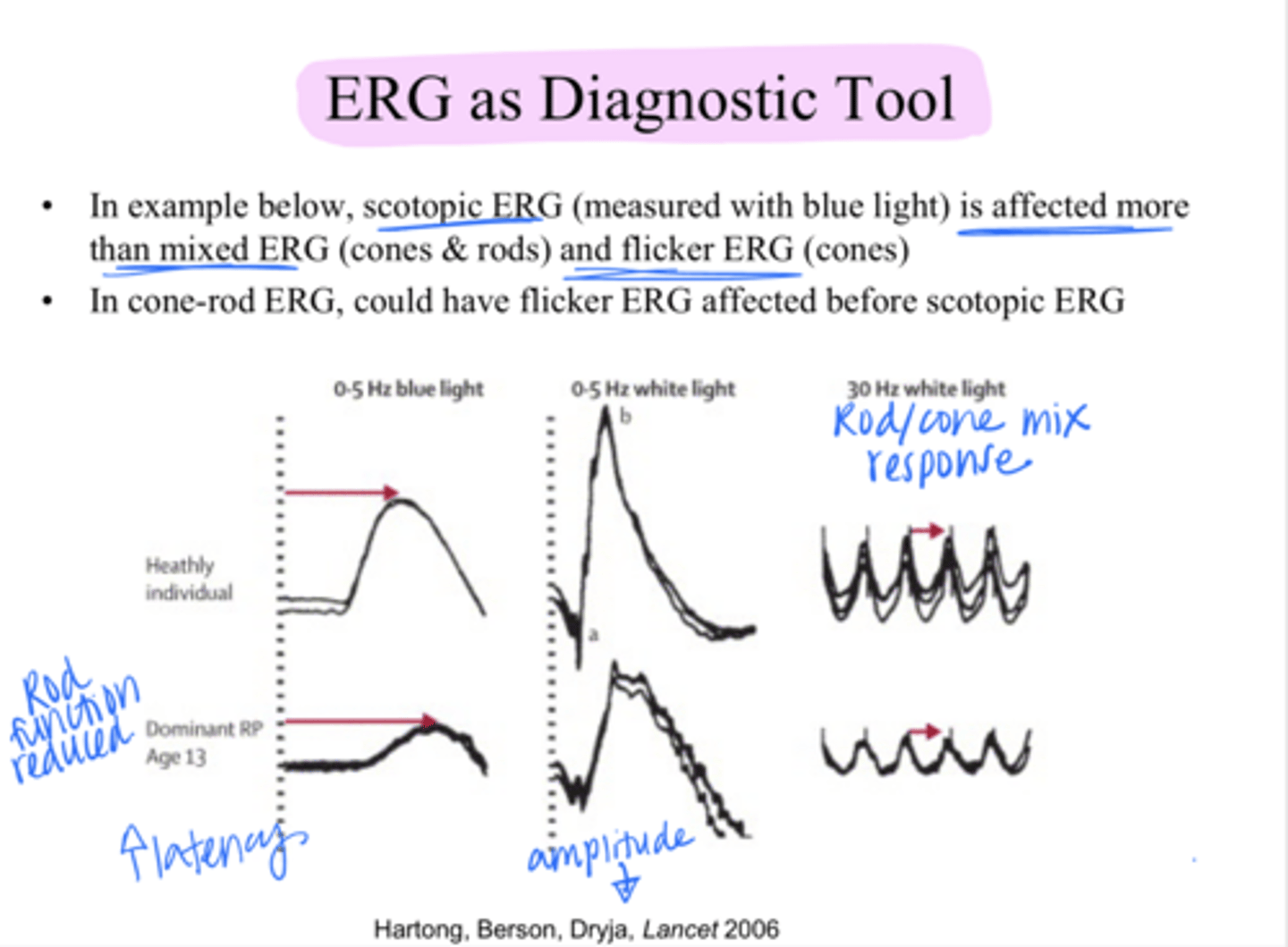
blue
REVIEW: Scotopic ERG can be measured with ____ light
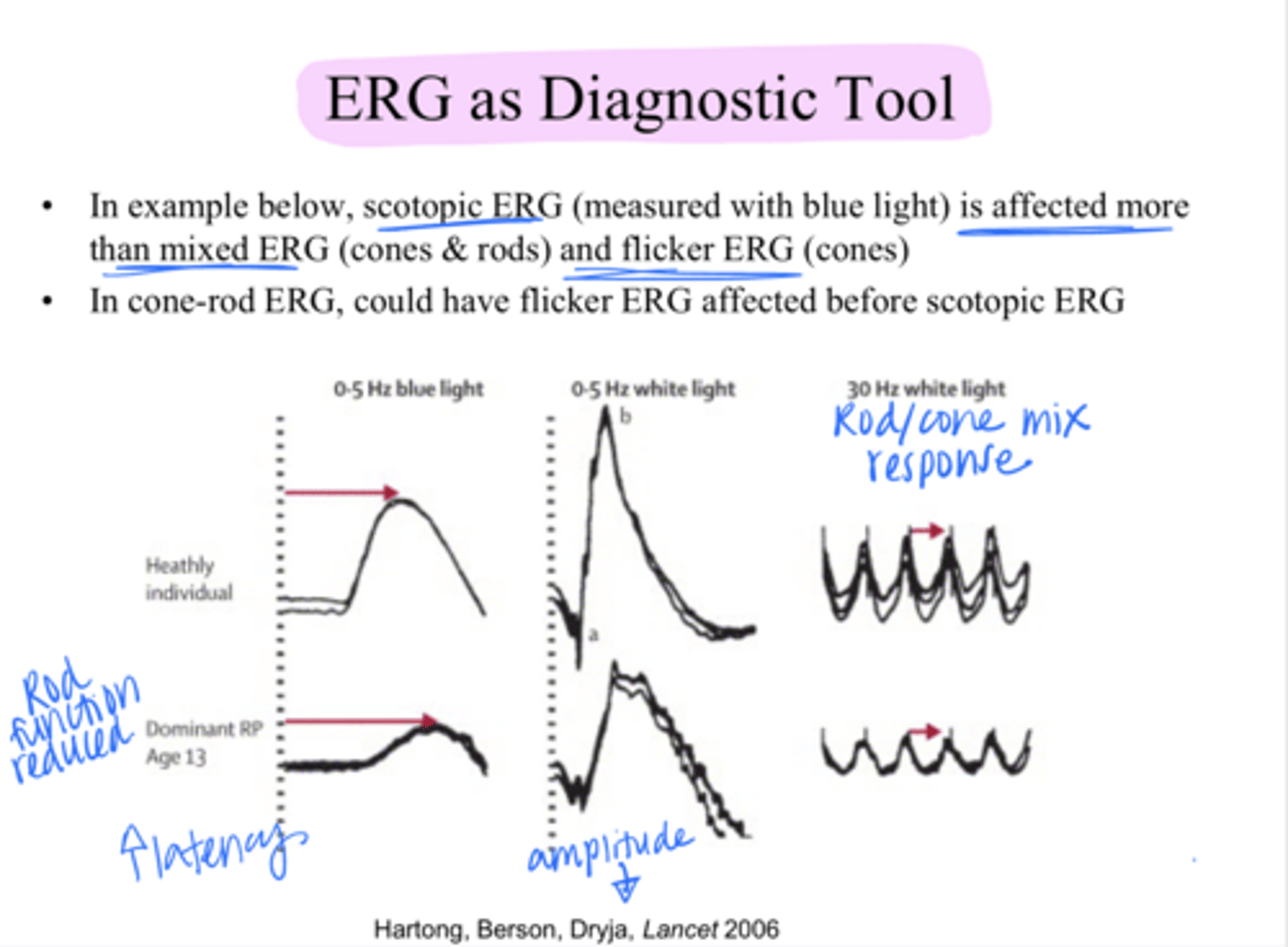
Scotopic ERG will be affected more
In retinitis pigmentosa, which will be affected more?
Scotopic ERG/mixed ERG (cones and rods), flicker ERG
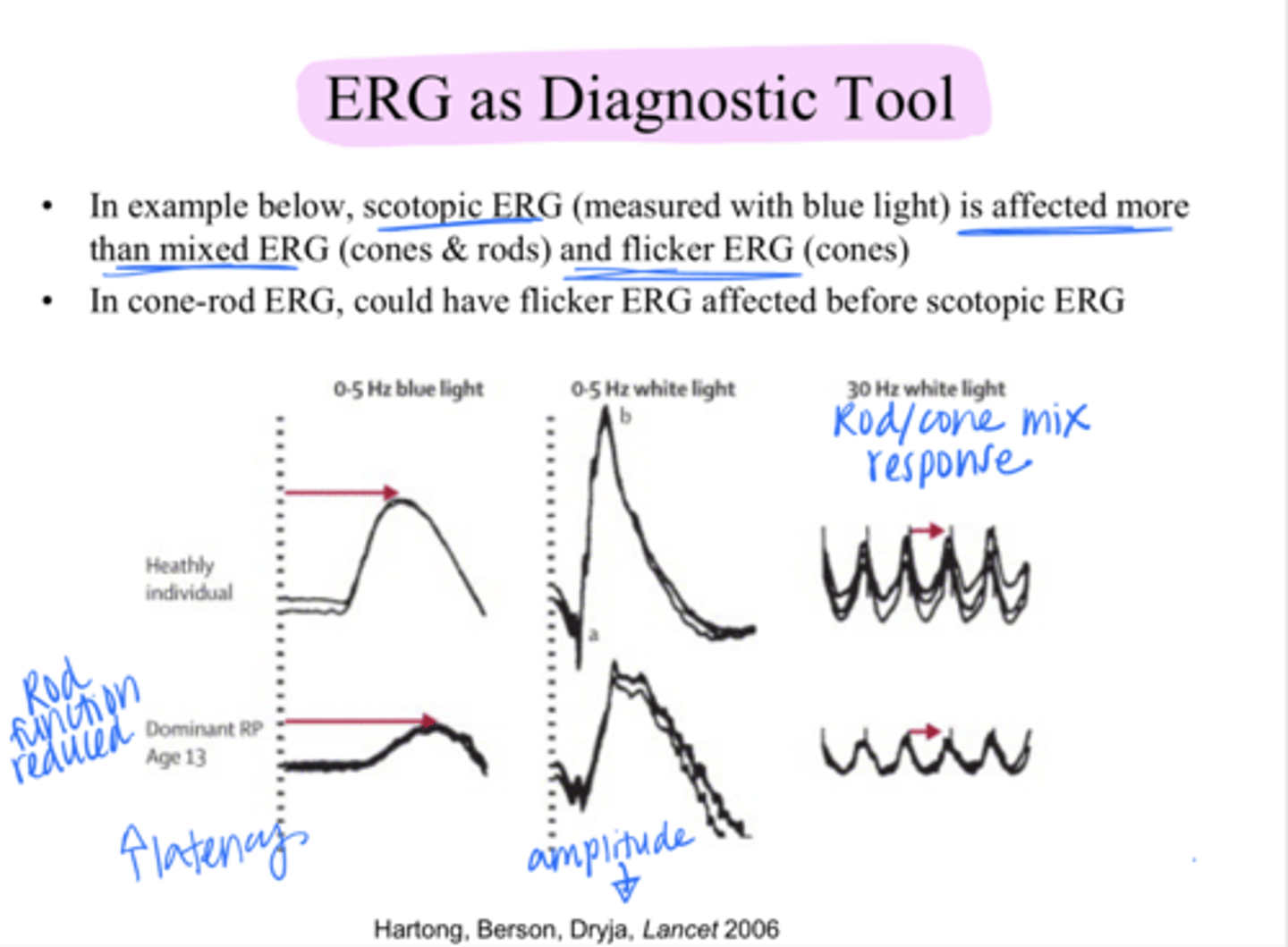
Yes
In cone-rod retinitis pigmentosa, is it possible to have the cone-flicker ERG affected before scotopic ERG?
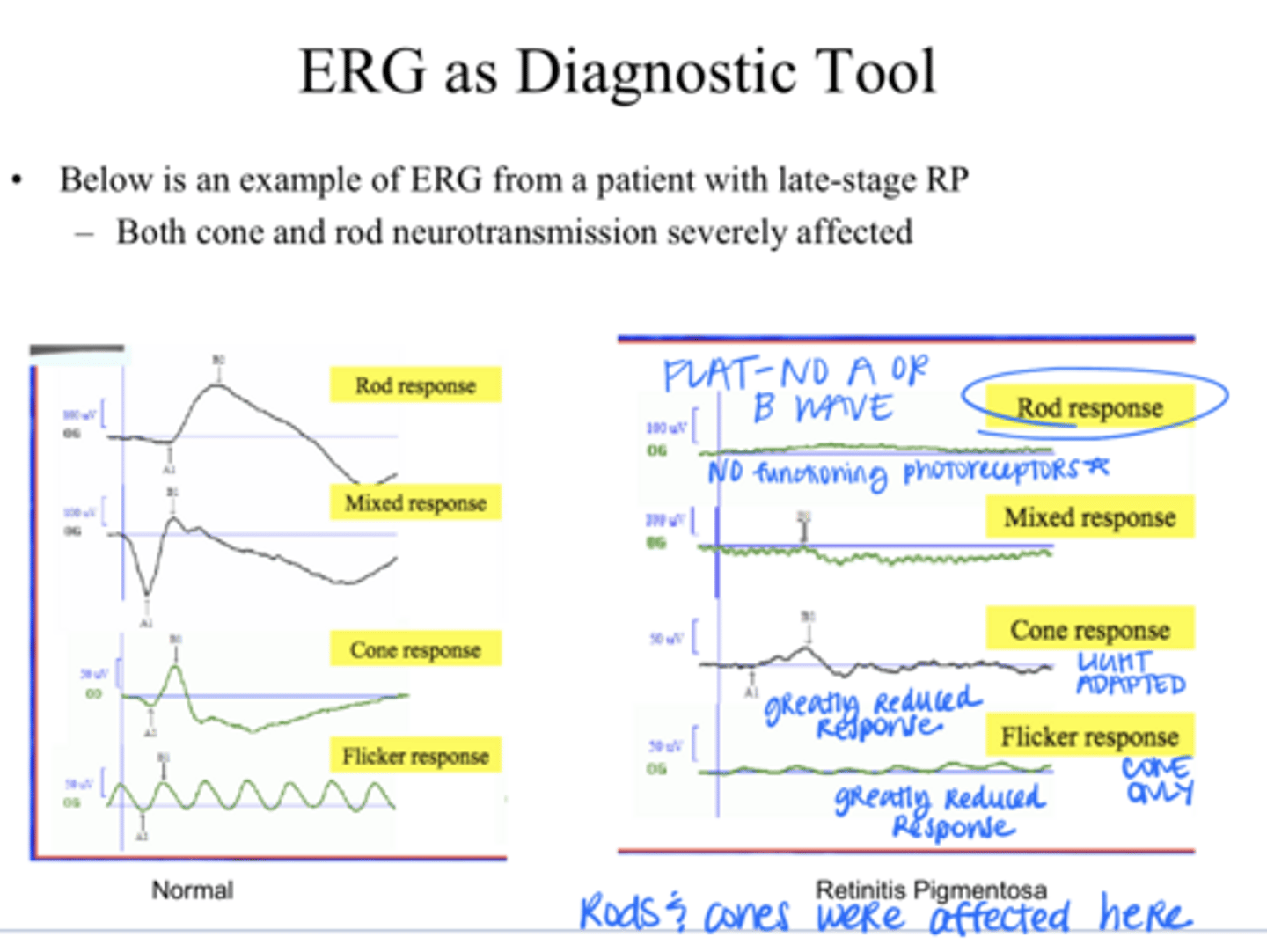
Early Stage RP v Late Stage RP on ERG (Pic)
Early Stage RP v Late Stage RP on ERG (Pic)
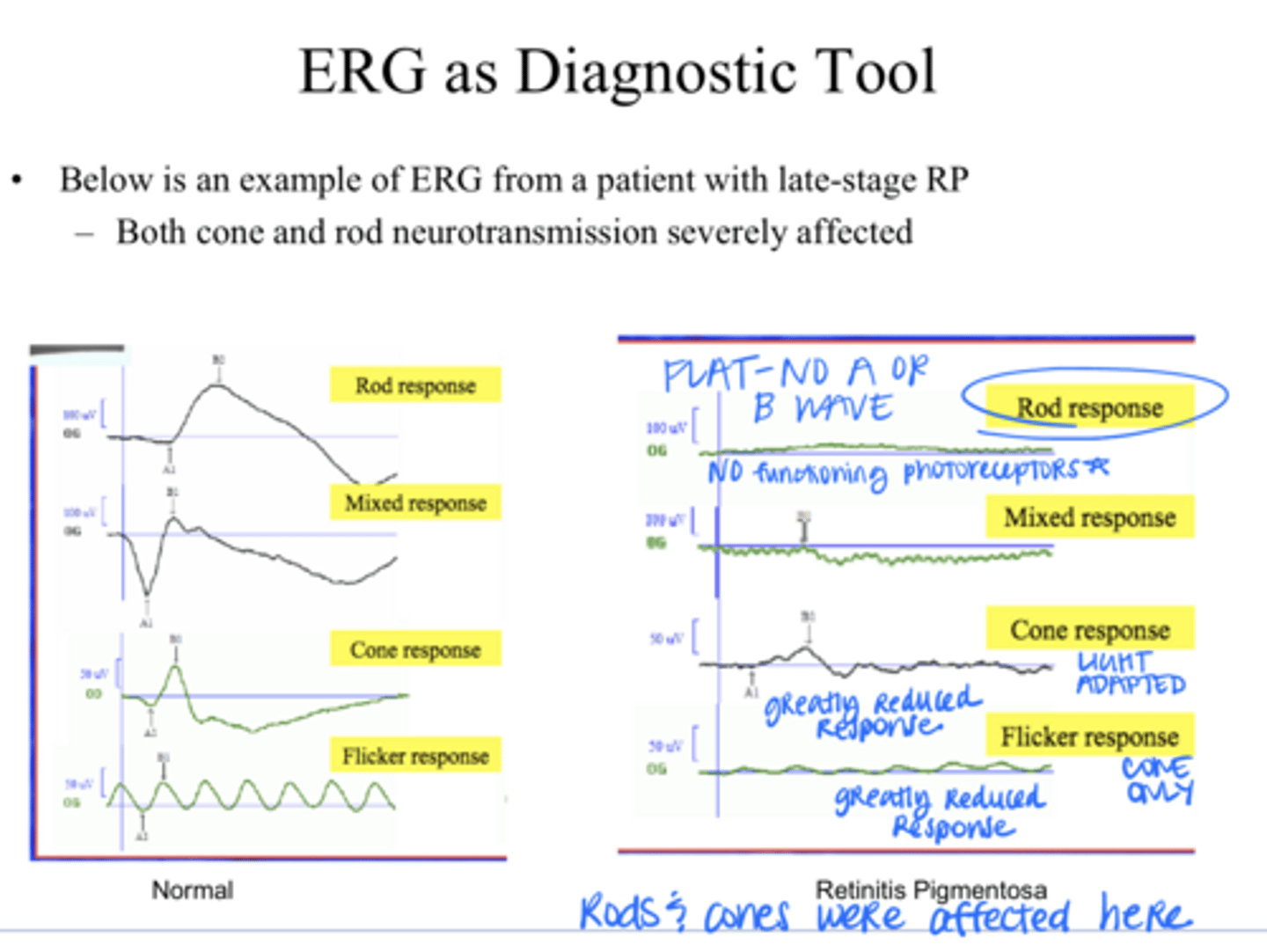
flatten -- decreased amplitudes d/t no functioning photoreceptors
As RP progresses, the lines on the ERG will ________
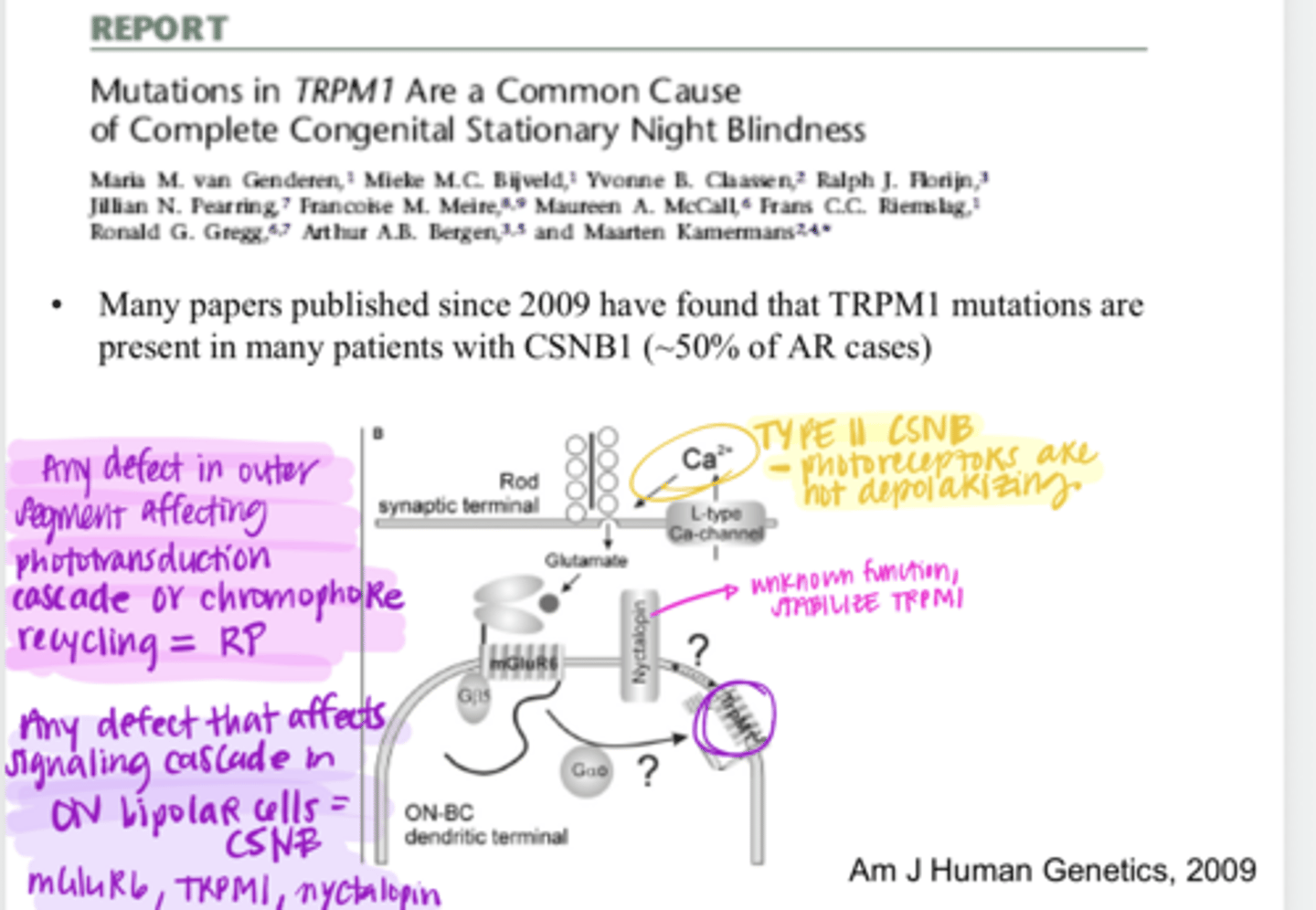
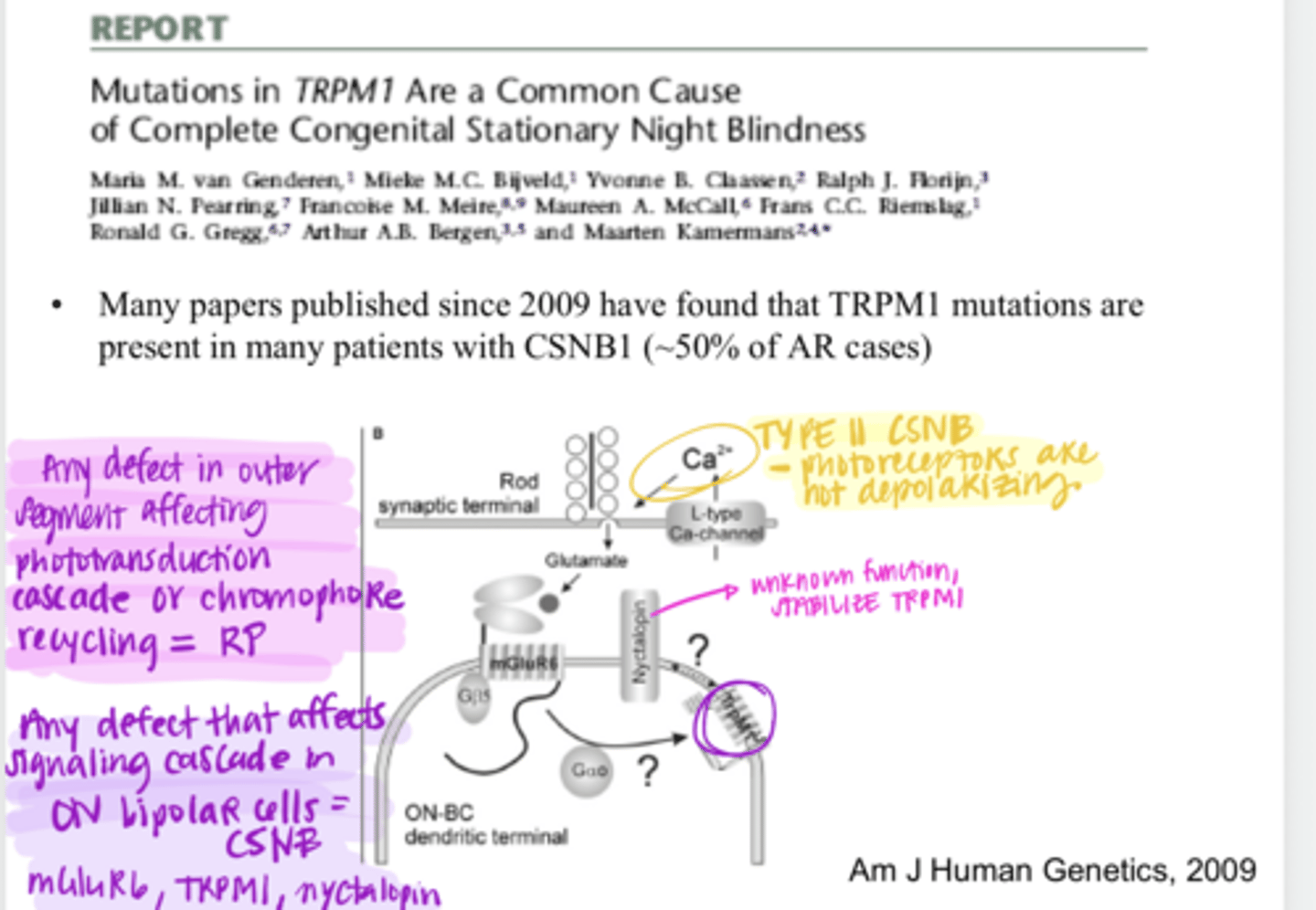
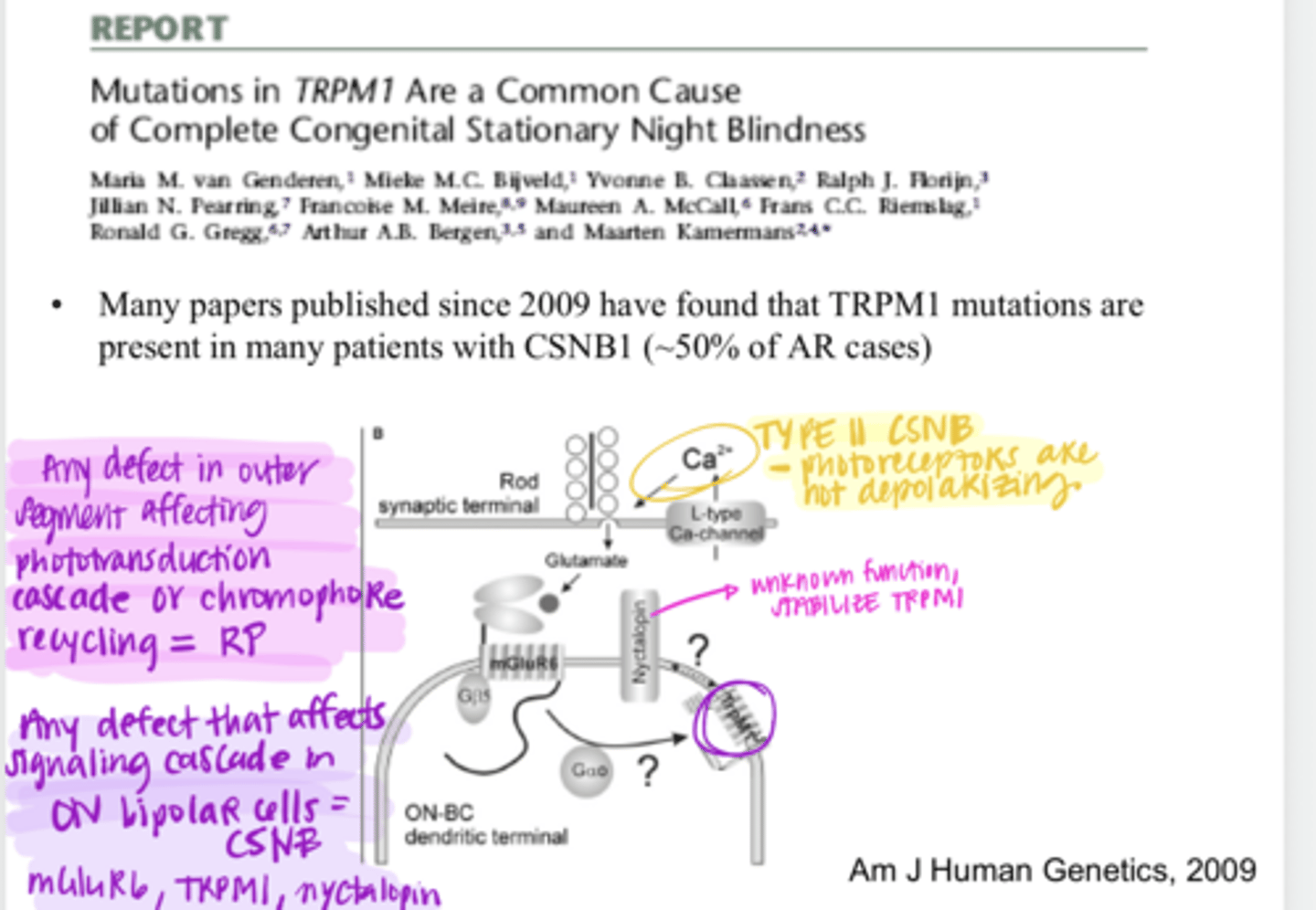
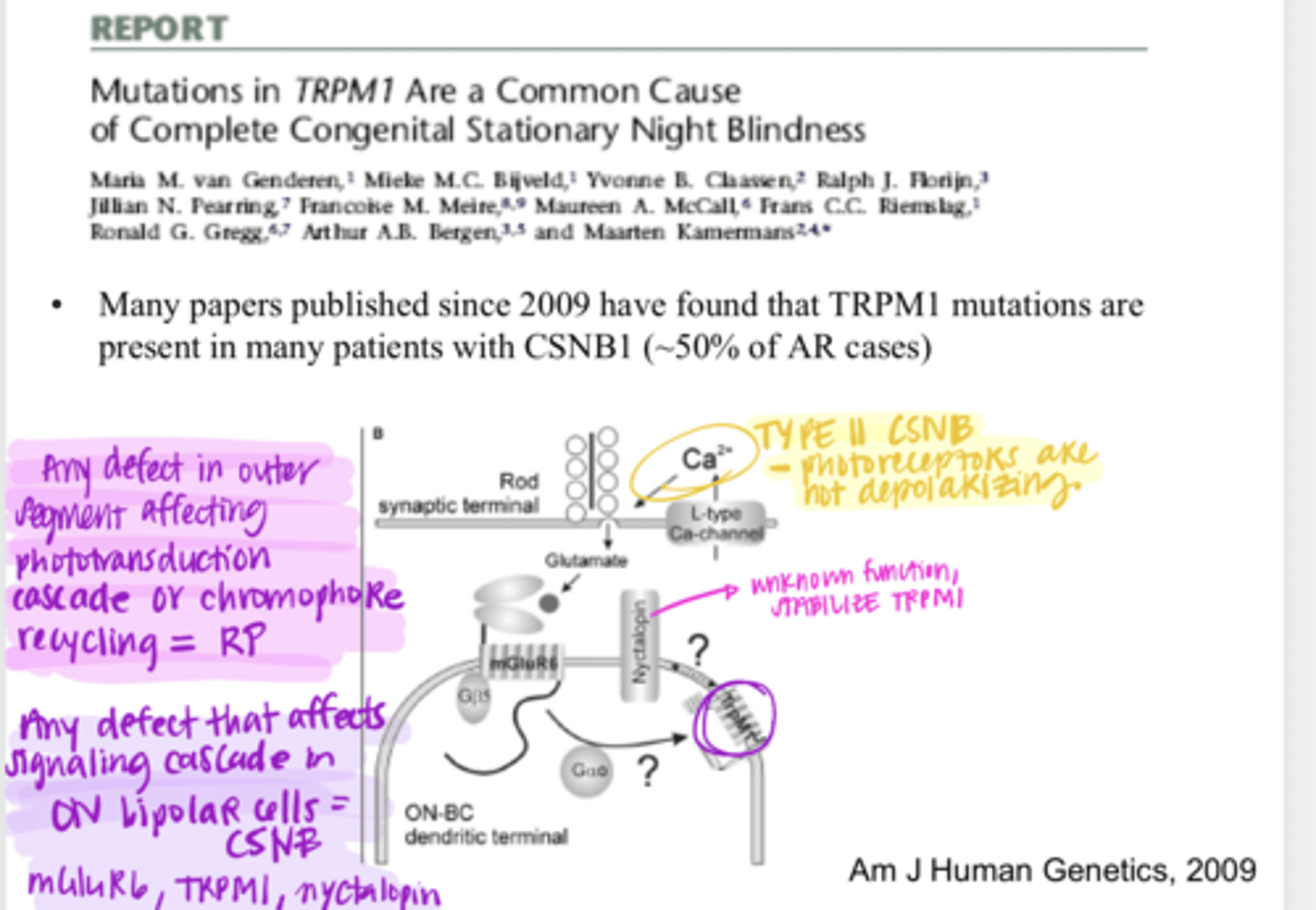
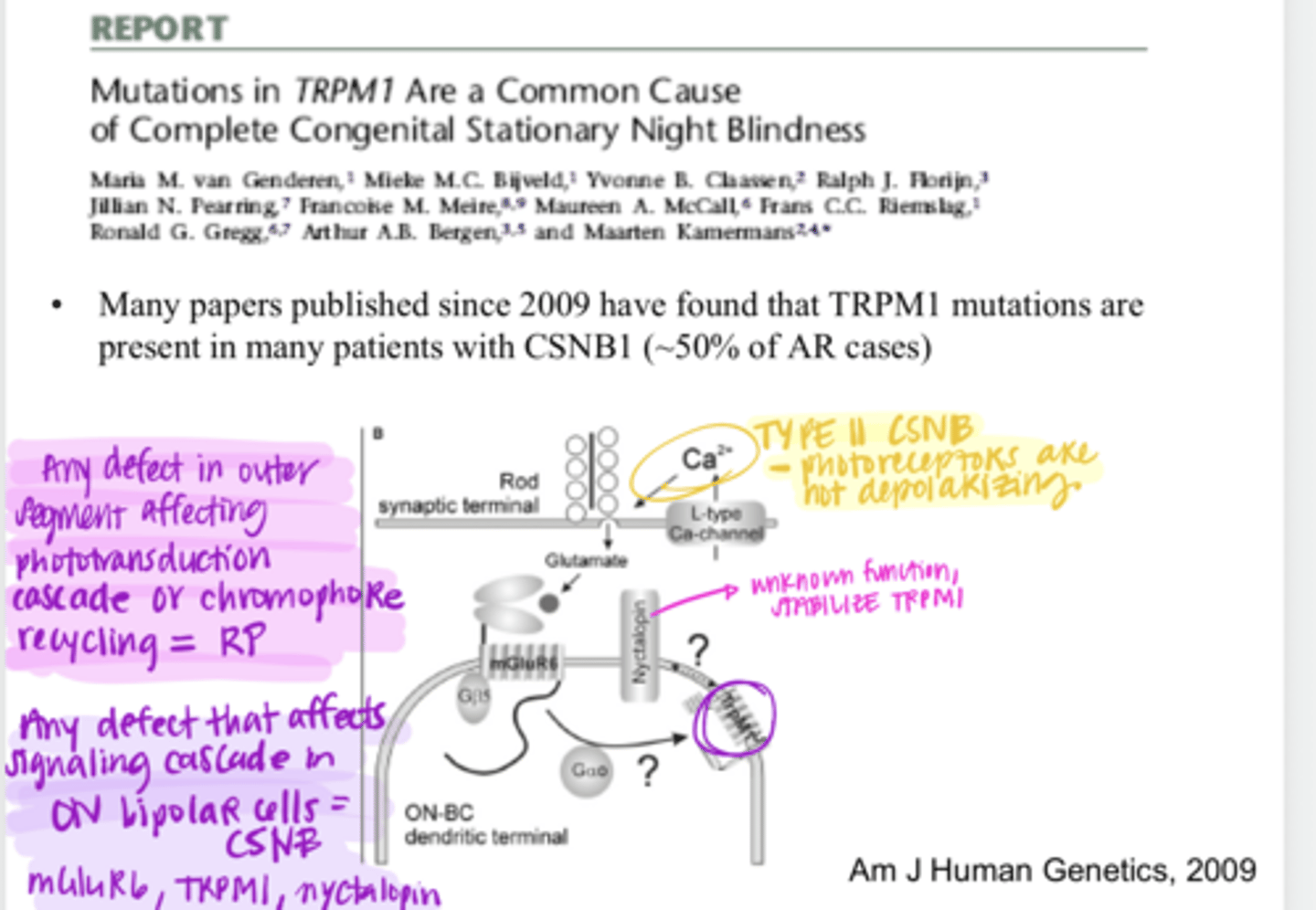
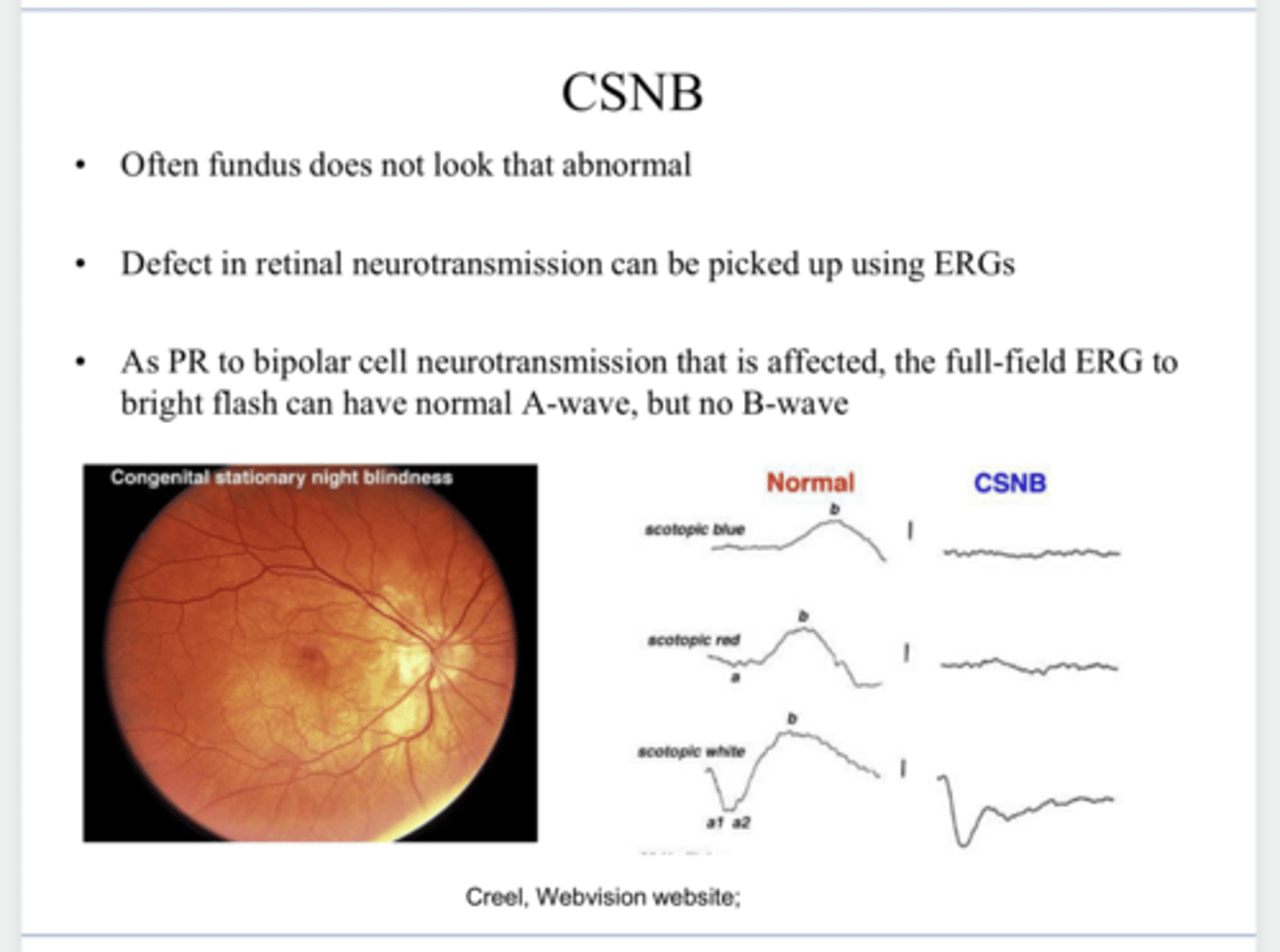
Congenital Stationary Night Blindness
Retinal disorders in which neurotransmission is altered between photoreceptors and bipolar/horizontal cells
no -- it is "stationary"
Does congenital stationary night blindness get worse over time?
-complete form
-complete absence of rod pathway function
-x-linked and autosomal recessive
Describe Type I congenital stationary night blindness
localized to ON bipolar cells
Where is the defect thought to be localized in Type I (Complete Form) congenital stationary night blindness?
genetic defect in nyctalopin, a protein that is found in dendrites of ON bipolar cells
What is the defected protein in X linked congenital stationary night blindness?
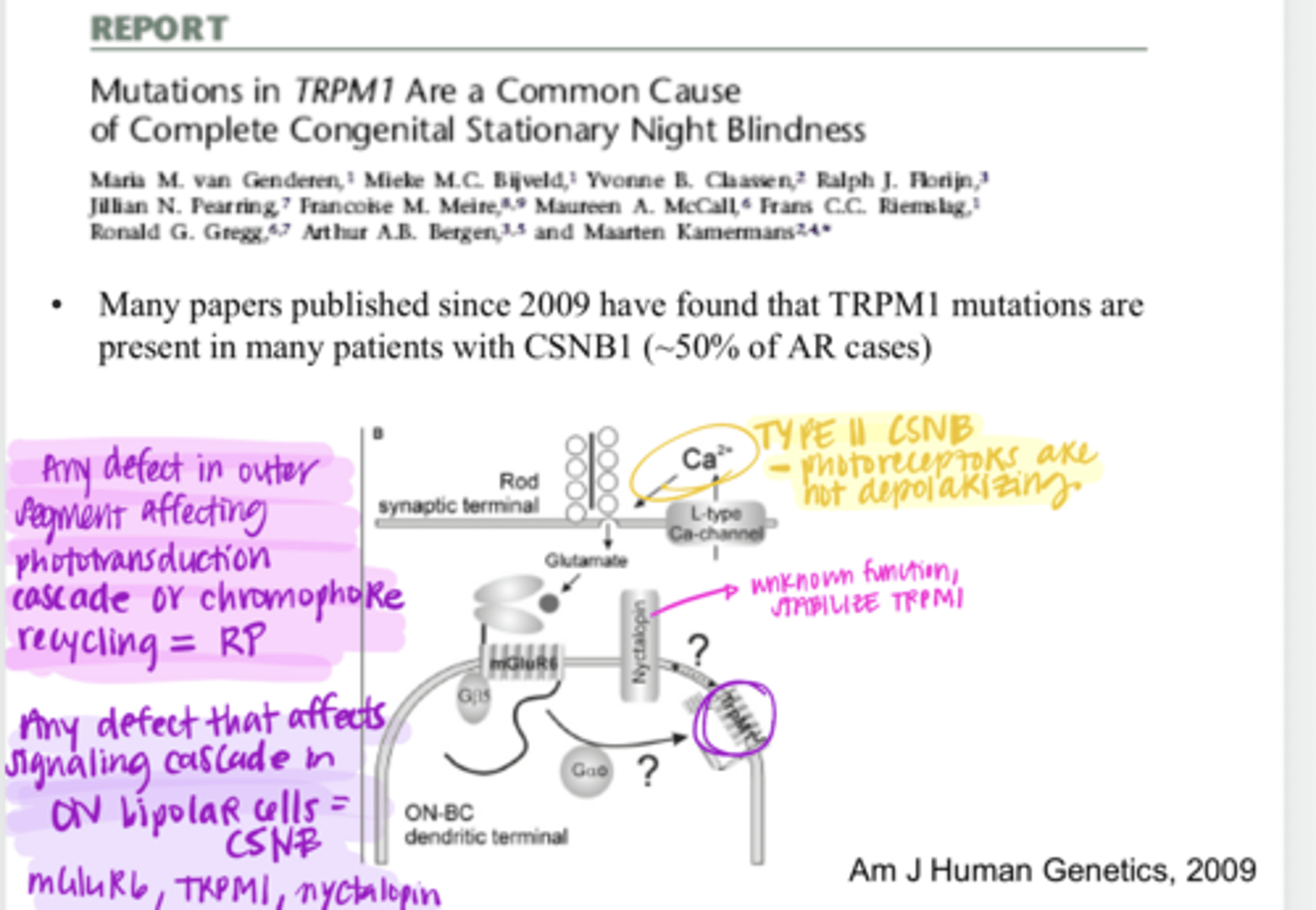
defect in mGluR6, maybe mutations in TRPM1 channel
What is the defected protein in autosomal recessive congenital stationary night blindness?
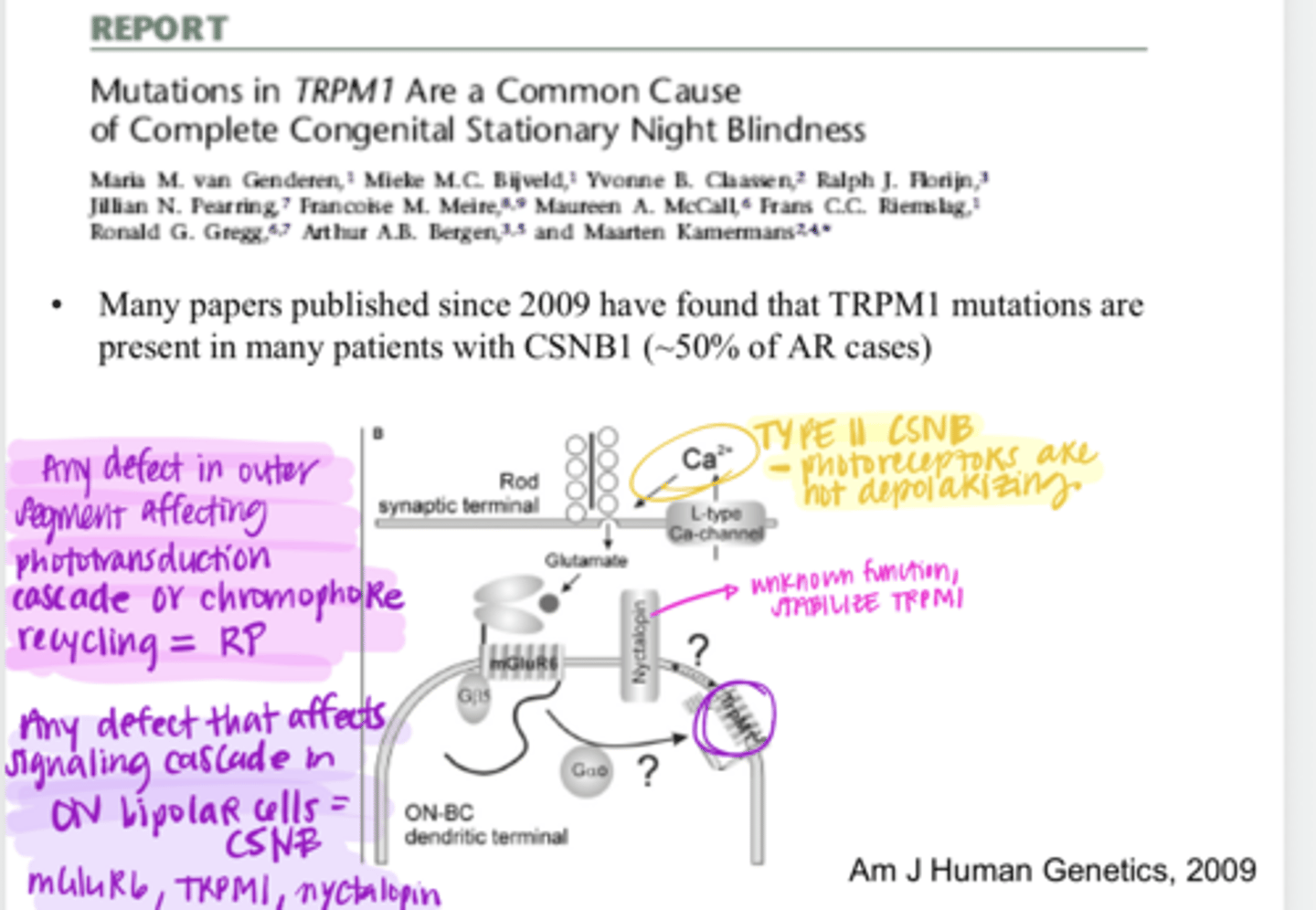
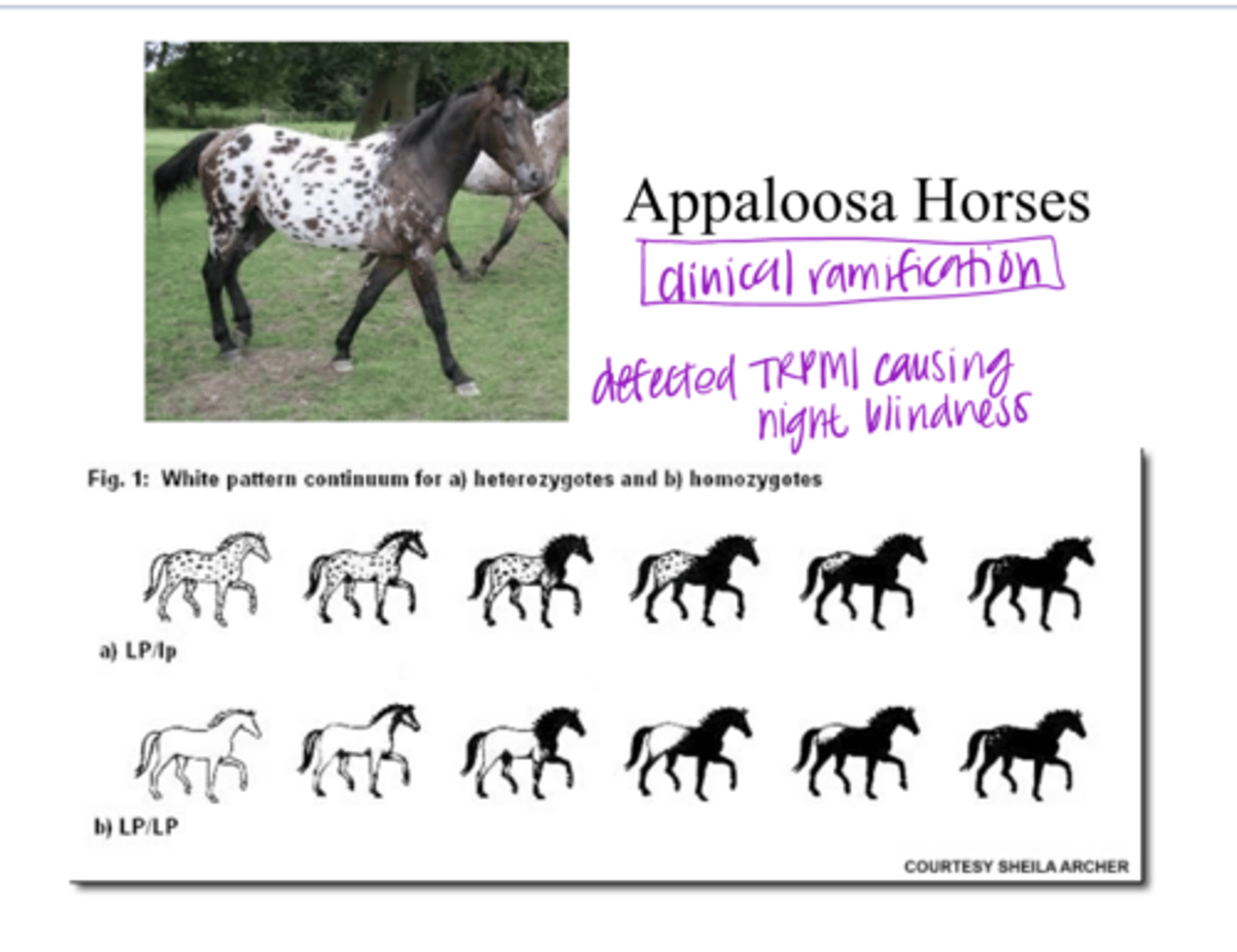
mutation in the TRPM1 channel
In about 50% of patients with autosomal recessive congenital stationary night blindness, what mutation is present?
-incomplete form
-x linked
-mutation in the gene that codes for specific VGCC found in photoreceptors
Describe Type 2 Congenital Stationary Night Blindness
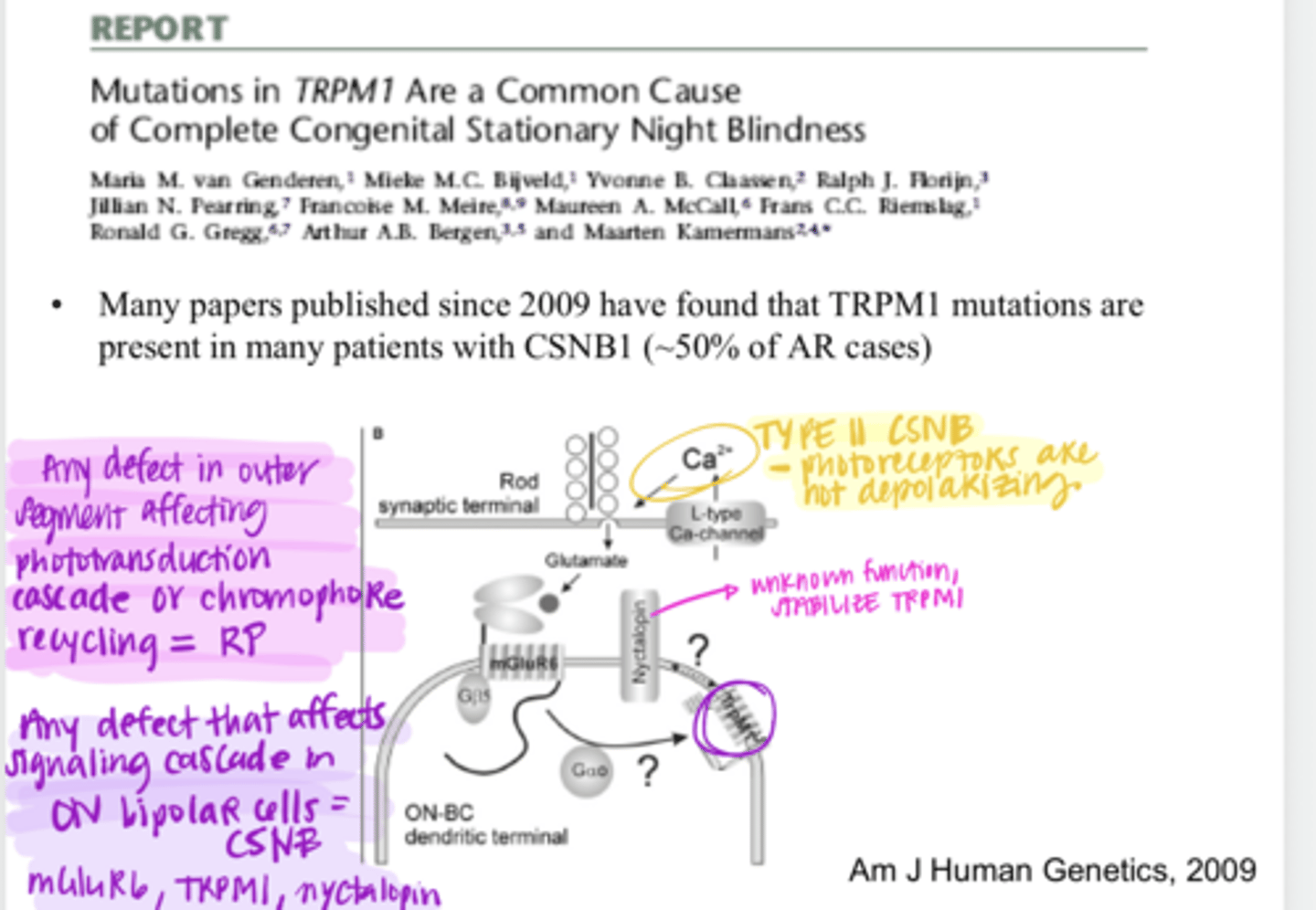
-Without Ca2+ influx, no NT is released
-Get impaired rod and cone function (Rod > cone)
Why is a mutation in the VGCC channel in the photoreceptors a problem in Type II Congenital Stationary Night Blindness?
Type I Congenital Stationary Night Blindness - likely because there are other VGCCs, particularly in cones, that are still functioning
Which vision is impaired more? WHY?
Type I OR Type II Congenital Stationary Night Blindness
nyctalopia -- night blindness
What is the primary symptom of Congenital Stationary Night Blindness?
Rods only signal to ON bipolar cells. Cones signal to both ON and OFF bipolars. There are more rods in the retina. You will shut down all the rods in the retina.
Why do you think there is such a severe affect on night vision & rod function if you affect the ON bipolar cell?
No -- it is STATIONARY
Is Congenital Stationary Night Blindness progressive?
-myopia
-hyperopia
-stabismus
**the connection between these symptoms and the defect in rod transmission is unknown
What are the "other symptoms" of Congenital Stationary Night Blindness?
can range from normal to severe (more common in T1)
What is the VA range for individuals with Congenital Stationary Night Blindness?
males -- and usually runs in families
For X-linked Congenital Stationary Night Blindness, this presents commonly in (males/females)?
No -- may look pretty normal
Does the fundus look very abnormal in a patient with Congenital Stationary Night Blindness?
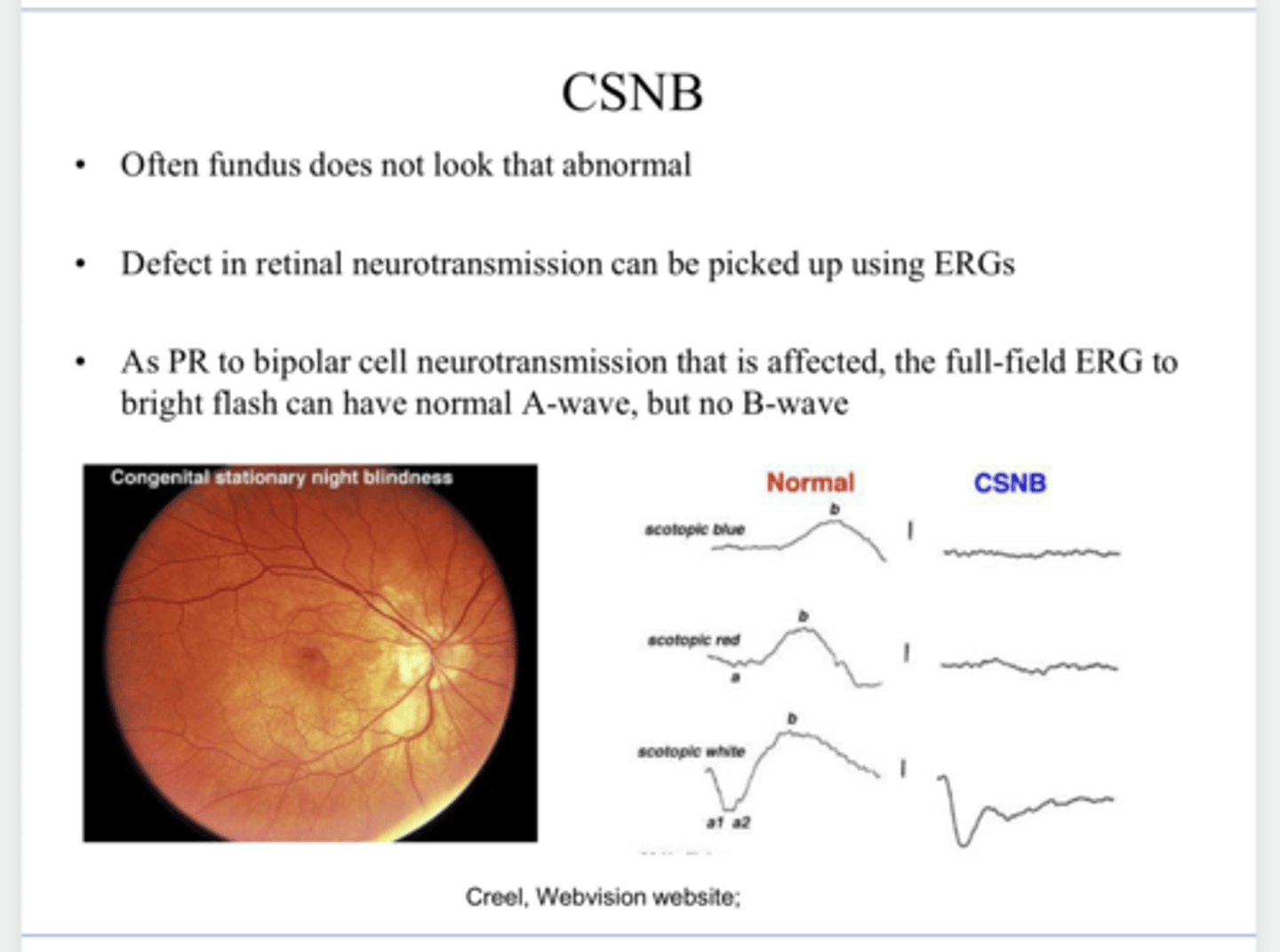
ERG
A defect in retinal transmission can be picked up using a ______?
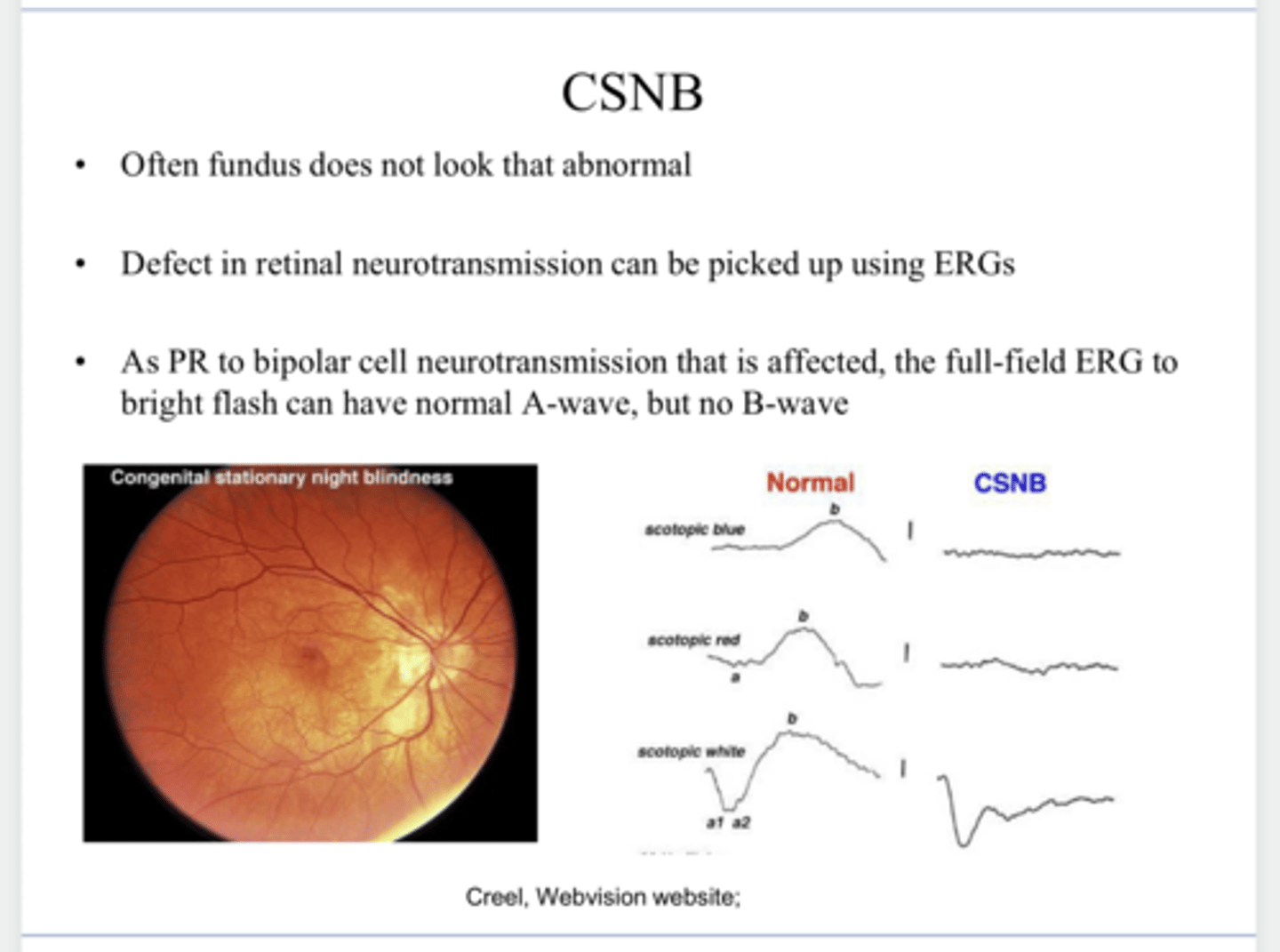
PR to bipolar cell neurotransmission is affected, the full field ERG with a bright flash can have a normal A-wave but there will be no B-wave
What will be the effect on the ERG of patients with Congenital Stationary Night Blindness?
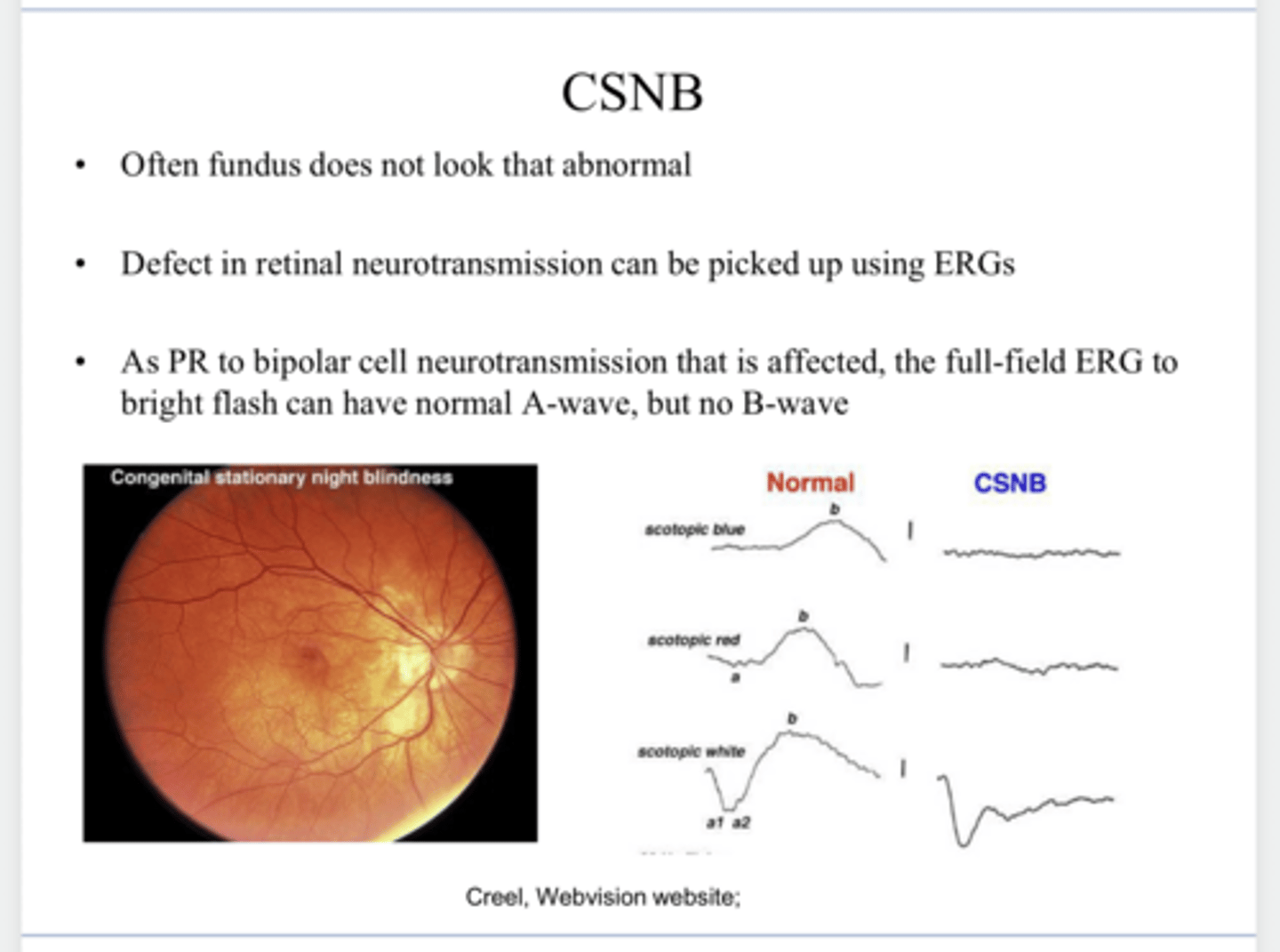
Yes -- and thus their A-wave on ERG will be normal
Does the outer segment of the retina in patients with Congenital Stationary Night Blindness respond to light?
1) Transduce visual images into electrochemical signals
2) Perform initial processing of this signal
3) Convert the processed signal into a signal that can be sent and interpreted by the brain
REVIEW:
What are the 3 principal functions of the retina?