Anxiety Disorders
1/24
Earn XP
Description and Tags
lecture 5
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
25 Terms
what is the definition of anxiety
feeling of unease, such as worry or fear, that can be mild or severe
more constant than normal stress or anxiety and impacts daily life
different types of anxiety disorder
Generalised anxiety disorder (GAD)
Panic disorder
Obsessive compulsive disorder (OCD)
Post-traumatic stress disorder (PTSD)
Phobias, such as claustrophobia and social phobis
symptoms of GAD
varies in different cases:
restless or worried
trouble concentrating and sleeping
dizziness
heart palpatations
diagnose using DSM-5
needs to persist for over 6 months and be uncontrolable
include at least 3 of 6 symptoms
rule out other medical conditions
Panic disorder
anxiety disorder with regular panic attacks
intense symptoms that come on fast without reason
some symptoms can overlaop with other conditions (egl low blood pressure)
range from 1-2 a month to multiple a week
last 5-20 mins
Obsessive compulsive disorder
combination of obsessive thoughts and compulsive activity
Obsession = unwanted or unpleasant thought causing anxietyb
Compulsion = repetitive behaviour to supress negative thoughts
must be time consuming and impact daily life
Post-traumatic stress disorder (PTSD)
caused by traumatic effects → affects 1 in 3 who experience trauma
re-lived through nightmares or flashbacks
avoidance of linked memories
cognative distortions of the event
lasts over 1 month and impairs function
without other cause
Phobias
overwheling and debilitating fear of somthing with little or no danger
specific phobias → anomals, environments, situations, bodily
complex → agoraphobia, social phobias
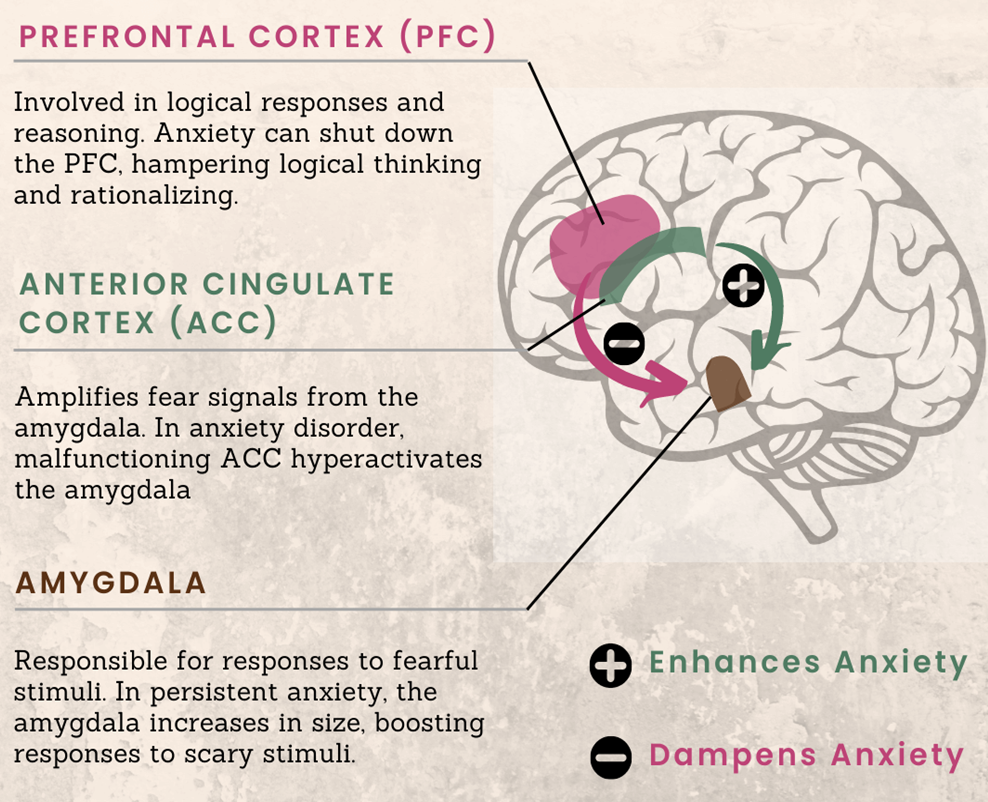
3 brain regions involved in GAD
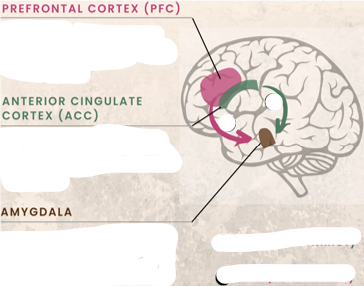
role of prefrontal cortex in GAD
controls rational logical thought to reduce anxiety
role of anterior cingulate cortex (ACC) in GAD
amplifies negative information, increasing anxiety
role of amygdala in GAD
inhibits PFC and initiates fight or flight
interraction between brain regions in anxiety
normally there is functional connectivity between PFC, ACC and amygdala to manage anxiety
in anxiety disorders the connections are disrupted → increased amygdala activity and decreased PFC
fMRIS show weaker functional connectivity between PFC and amygdala compared to healthy controls
increased functional connectivity between supramarginal gyrus (SMG) and PFC and between posterior cingulate cortex (PCC) and medial temporal gyrus (MTG)
reduced funtional connectivity between SMG and inferior temporal gyrus (ITG)
Genetic changes in GAD
around 30% heritability
Risk genes linked to monoamine neurotransmission and neurotrophic signalling:
5-HT reuptake transporter short alleles (S/S homozygous)
5-HT1A receptor C1019G polymorphism → increases negative feedback and decreases serotonergic signalling
MAO-A T941G polymorphism and long allele → increase metabolism of monoamines and reduce signalling
BDNF Val66Met polymorphism → reduces BDNF activity
gene-environment interraction in GAD
30% inherited, 70% environmental
environmental risk factors
childhood trauma
stressfull family circumstances
natural disasters
genetics enhance environmental effects → having genetic and environmental risk factor drastically increases chances of GAD
Childhood trauma x 5-HT transporter, COMT & MAOA variants
Hurricane victim x Neuropeptide Y variants
Daily life stress x 5-HT transporter variants
Family relationship scale x Neuropeptide S receptor 1 variants
GABA in GAD
dysregulated inhibitory neurotransmission
GABA-A receptor downregulated
treat with GABA-A agonist
5-HT in GAD
treatment with SSRIs show it plays some role
Neuropeptides in GAD
patients are hypersensitive to cholecytokinin (CCK) agonists
but trials using CCK-antagonists were unsucessfull
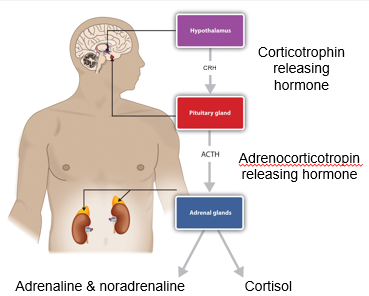
HPA Axis
Hypothalamic-pituitary-adrenal axis
hypothalamus → in forebrain
pituitary gland → below hypothalamus
adrenal glands → above kidneys
together regulate stress response, mood, immune function and metabolism
hypothalamus → (corticotrophin releasing hormone) → pituitary gland → (adrenocorticotroin releasing hormone) → adrenal glands → (cortisol, adrenaline, noradrenaline)
GAD and neurodendocrine pathway
cortisol activates fight or flight and inhibits CRH and ACTH release
negative feedback to reduce cortisol and NA
in chronic stress and GAD the HPA axis is dysregulated
considerations during medical anxiety assessment
mental health history
environmental issues
medical and drug history
degree of distress and impairment
risk of suicide
non-pharmacological treatment of GAD
self help
meditation and mindfullness
CBT/therapy
exercise
lifestyle changes
treatment for autonomic GAD symptoms
β-adrenoceptor antagonists
eg. propranolol
treatments for anxiety symptoms of GAD
SSRIs → eg. sertraline
SNRIs (serotonin and noradrenaline reuptake inhibitors) → eg. venlafaxine
Atypical antidepressants → eg. vilazodone or mirtazapine
benzodiazepines → eg. diazepam
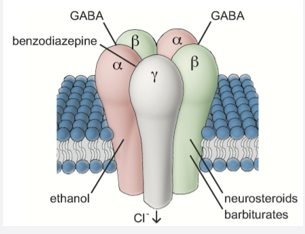
Benzodiazepines as GAD treatments
short-term use in crisis
used in insomnia, epilepsy and pre-surgey
enhances effect of GABA (inhibitory)
binds to GABA-A receptor between a and y subunits
causes conformational change to enhance GABA binding → GABA-A receptor positive allosteric modulator (PAM)
channel opens → Cl- influx → hyperpolarisation → reduced neural activity
next generation GAD treatments
current medications have issues
non-response
severe side effects → sexual dysfunction, drowsiness, weight gain
relapse
novel treatment targets:
glutamatergics eg. ketamine, riluzole, xenon
neurosteroids eg. aloradine
cannabinoids
MDMA
L-DOPA