L08 The GABAergic System
1/49
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
50 Terms
The GABAergic System
Main inhibitory transmitter in the CNS
Acts on GABA receptors: GABAA , GABAB and GABAC
GABAARs are most well-studied, will be our focus
GABA type A most important
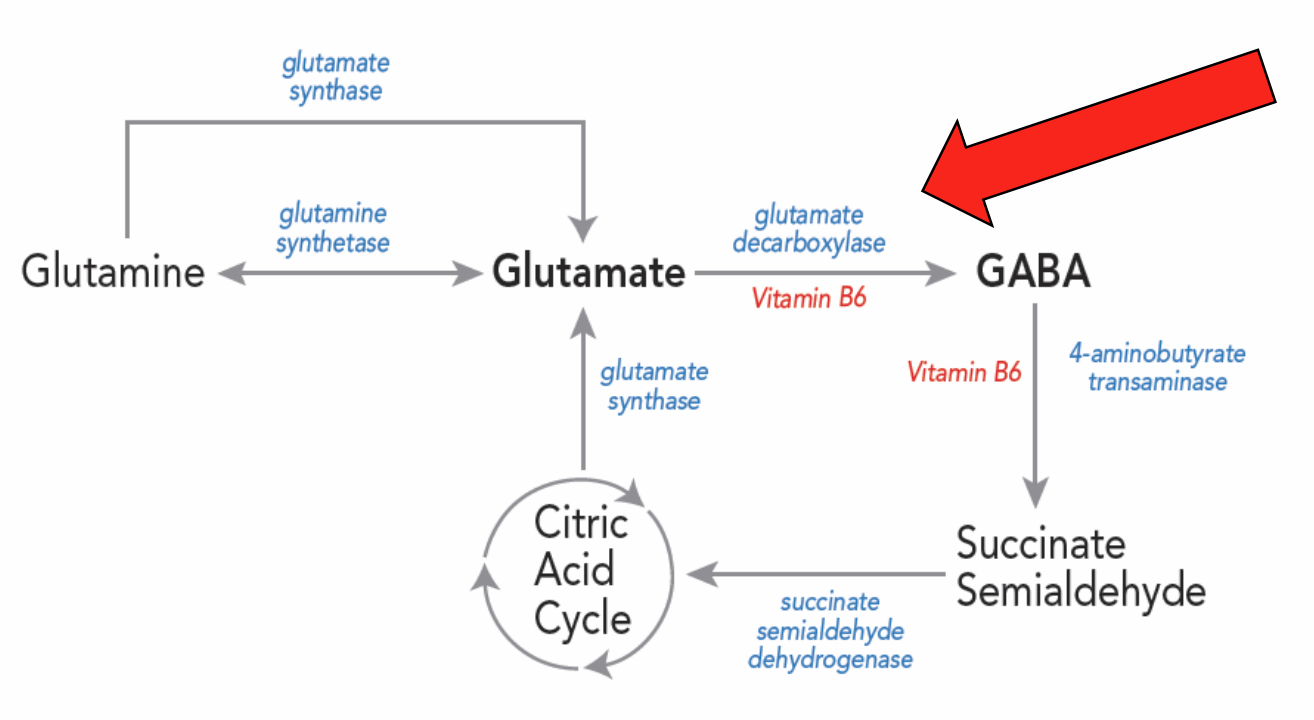
GABA synthesis
Made from glutamate via glutamic acid decarboxylase (GAD65 + GAD67)
key synthesizing enzyme
GAD65 + GAD67 marker of GABAergic neurons (key in many studies)
GABA levels
Abnormal levels associated w/mood disorders (e.g. depression, evidence inconsistent)
Interest in modifying GABA levels w/supplements
Research problematic
Conflicts of interest are apparent
Passage across blood-brain barrier questioned
controversial to say OTC supplement would max/min GABA levels
supplement unlikely to reach the brain → doesn’t cross BBB
The basics of GABA
Receptor subtypes
Receptor localization
GABA synthesis and metabolism
Transport
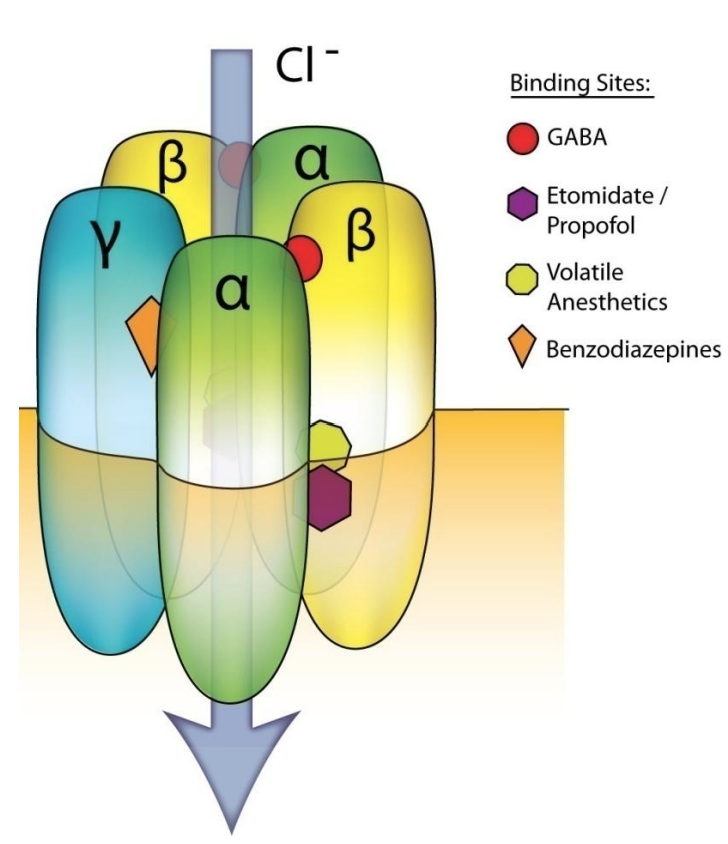
GABAA receptors
Ionotropic, generally ligand-gated channels
Permeable to Cl- ions
Fast inhibition (hyperpolarizing and/or shunting)
Composed of 5 subunits from a family of many members (16+)
2 α (1-6), 2 β (1-3) and 1 of γ (1-3), δ, ε, π or θ
targets for GABA
receptor is a transmitter and a channel → fast inhibitory signal
key feature: permeable to Cl- ions
conductance of -ve ion hyperpolarizing doesn’t make it inhibitory
clamps/fixes neuron from reaching MP (threshold)
5 subunits from subunit pool → makes GABAA receptor
2 alpha, 2 beta, 1 miscellaneous
review
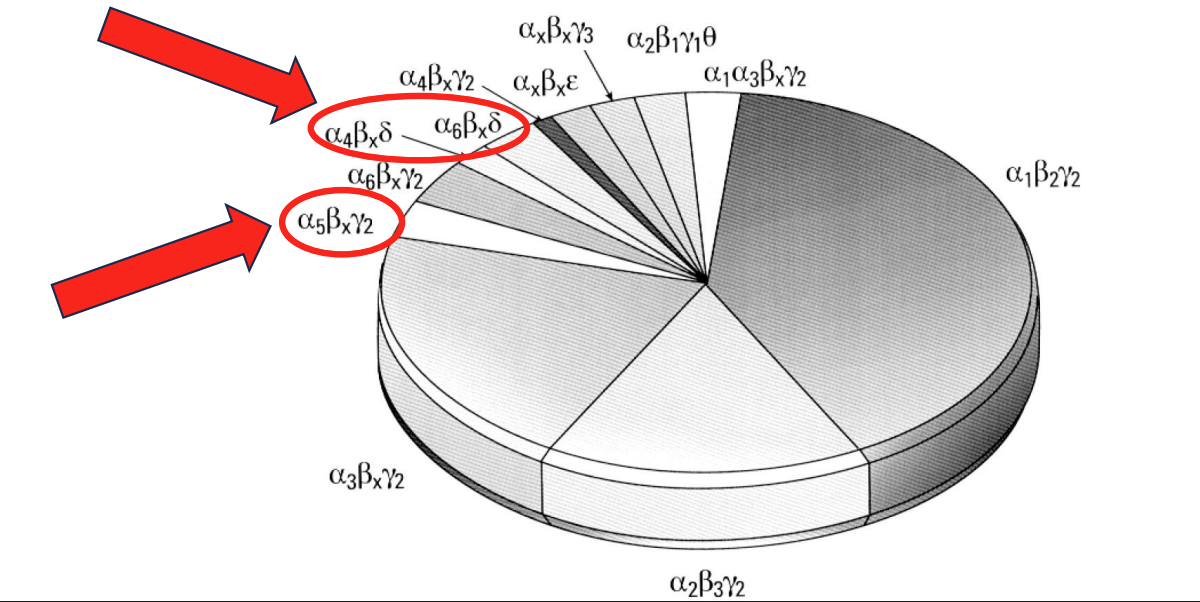
Native GABAA receptor abundance
Preferred stoichiometry of 2α:2β:γ or δ. Though many are possible, only a handful exist. Some are more common than others!
some are most abundant
a1, a3, b, gamma are possible but far less common → possibly restricted expression
significant for learning, memory, mood, and more (ones highlighted)
show diff pattern of exp + functionality than other receptors (next slide)
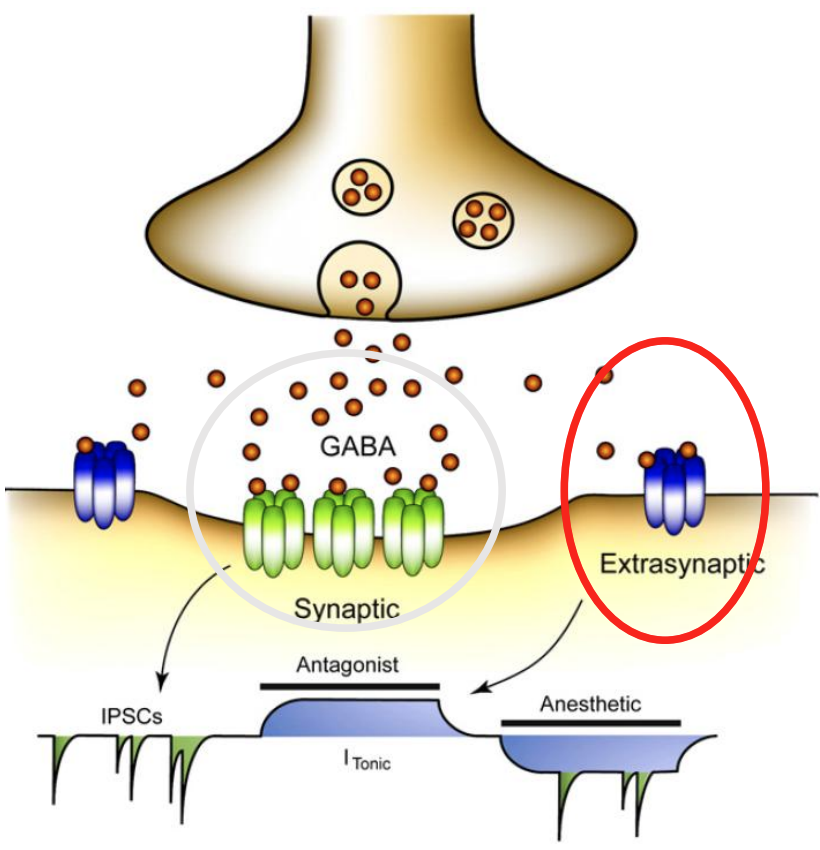
GABAA receptor localization
Synaptic or extrasynaptic regions
Synaptic:
αxβxγ2
αxβxγ3
“strong but transient”
Extrasynaptic:
α4βxδ
α6βxδ
α5βxγ2
αxβx*
“Weak but always on”
GABA binds to receptor → brief, strong current
focus: receptors that are outside (extra synaptic) → operate in low levels of GABA, not action-dependent release of GABA
middle = phasic (action-dependent release of GABA associated); extra synaptic + tonic currents
review
Our discussion of learning and memory will focus on α5 and δ receptors.
lower affinity + higher efficiacy
opposite true for extrasynaptic (bc low GABA and would otherwise not be on)
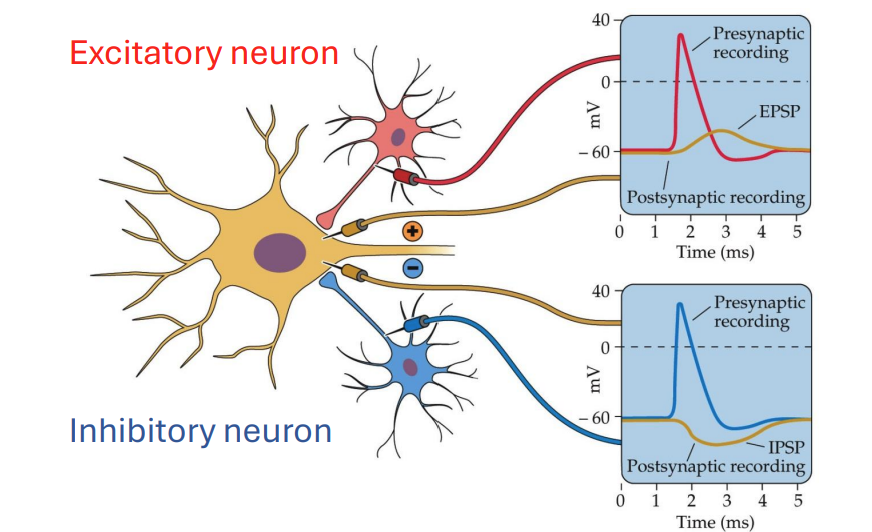
Excitatory and inhibitory signals
more signallng, less likely firing thru hyperpolarization/shunting
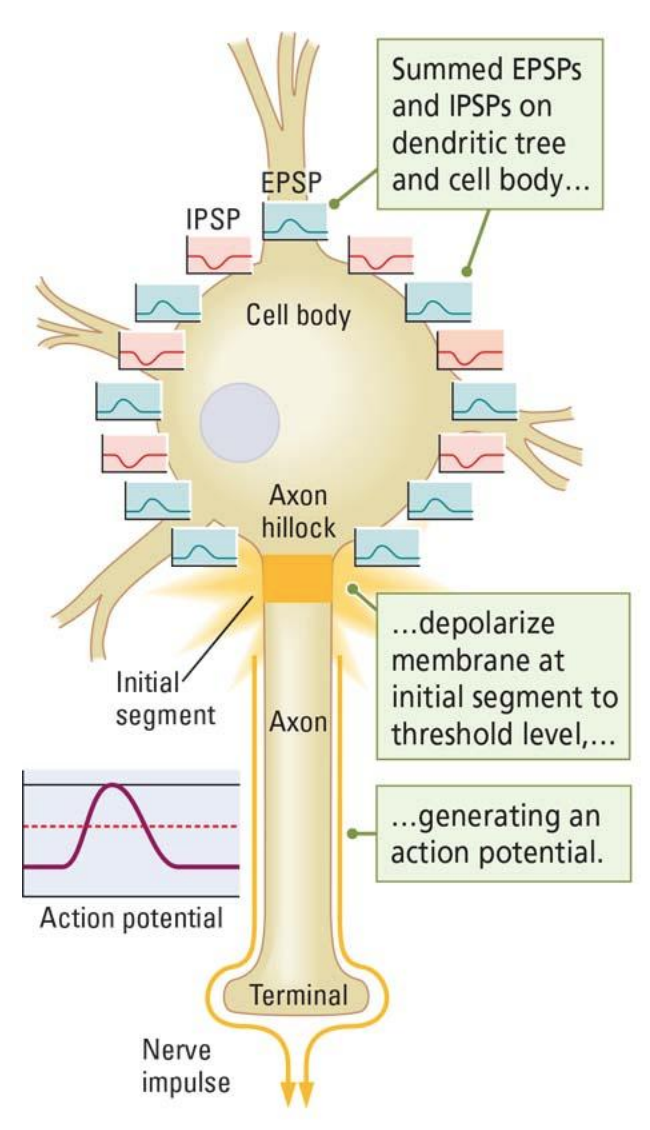
Summation of signals
Any one neuron generally receives many signals
All these signals are summated
If the sum exceeds a given threshold (excitatory >>> inhibitory), the neuron will fire
Inhibitory signaling decreases the likelihood of firing
excitatory + inhibitory signals incoming simultaneously
what is relative amount of each?
good amount of GABA keeps it from firing, but lots of ex would also may cause it to fire
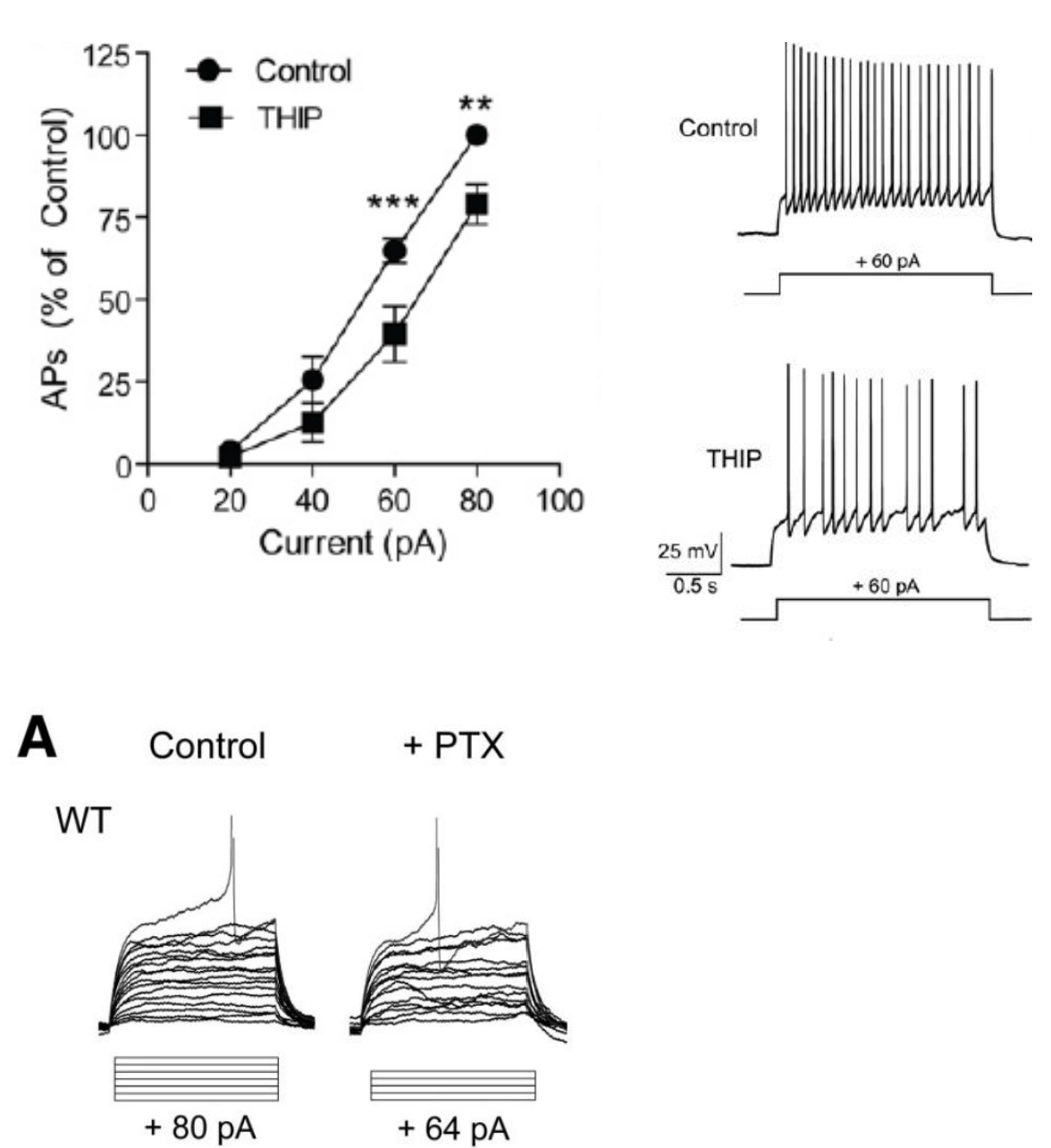
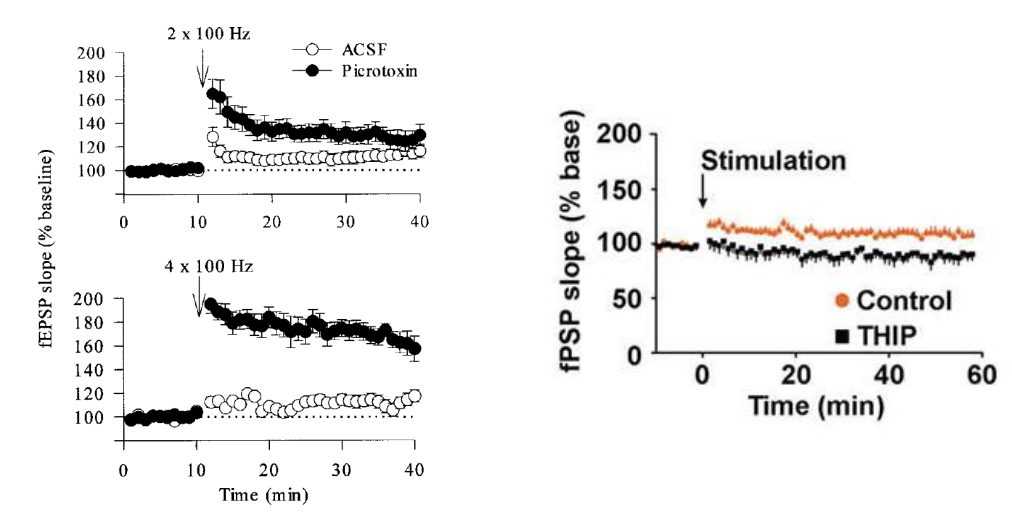
GABAARs reduce excitability
Top: Activating GABAARs with THIP decreases excitability → less APs / time unit
Bottom: Blocking GABAARs with picrotoxin increases excitability → excitability would skyrocket
blocking → less pA needed to fire neuron
excitability = amount of AP / time unit
less excitable = less APs/ time unit (and vice versa)
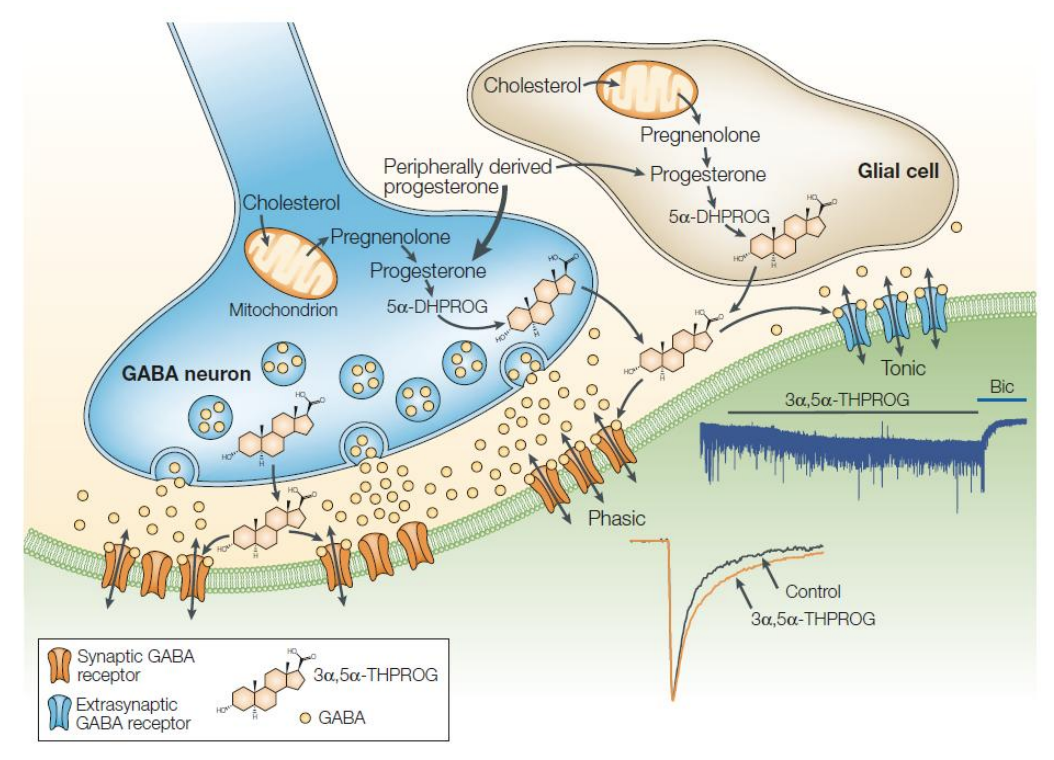
GABA and neuroactive steroids
The activity of GABA at its receptor can be modified by many compounds, including neuroactive steroids.
steroids can act on receptors; tuning role increasing activation of receptor in presence of GABA (pregnenolone, progesterone etc.)
positive, allosteric modulators b/c of delta receptors (they will tune up in presence of GABA)
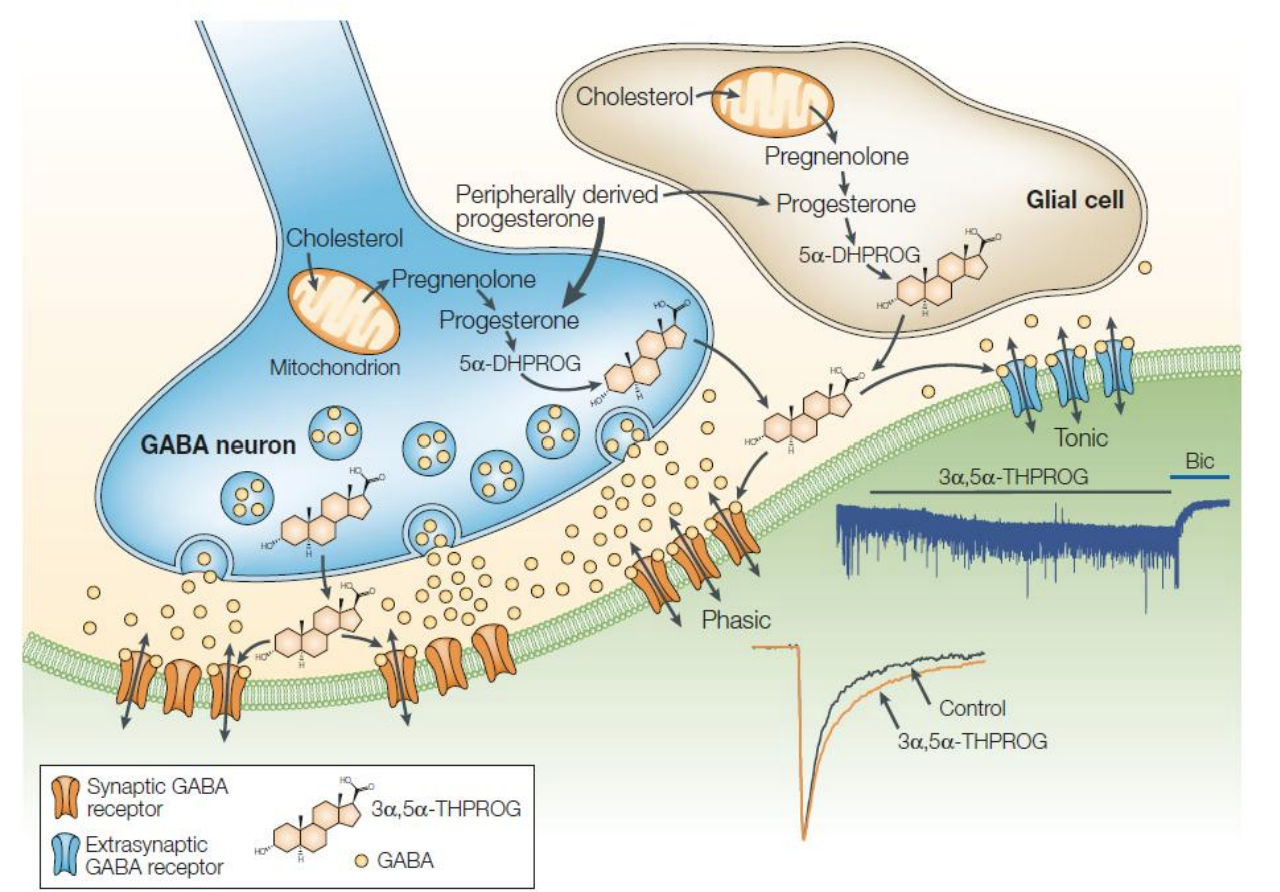
Neuroactive steroids
Steroid hormones naturally produced by the body
Levels vary during development (e.g. puberty), reproductive cycle (e.g. postpartum) and with stress
Generally increase activity of GABAA receptors, particularly δGABAA receptors
Positive allosteric modulators
Some have anxiolytic and antidepressant properties
Brexanolone/Zulresso for post-partum depression (IV) and Zuranolone/Zurzuvae (oral)
more activated by agonists
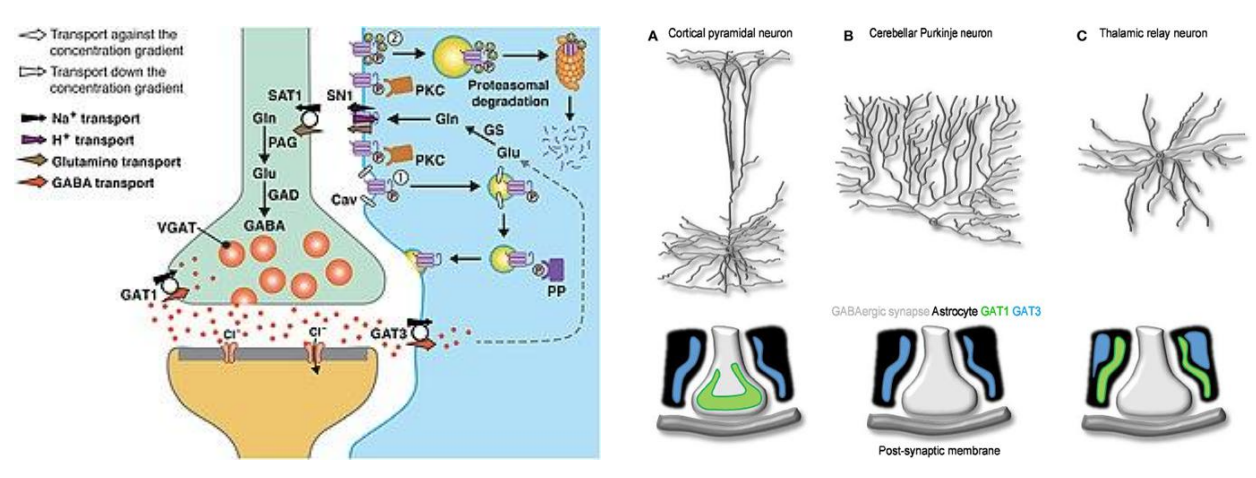
GABA transporters (GAT)
Three types; GAT1 + GAT3 most abundant in the brain
Found in neurons (GAT1) and astrocytes (GAT3)*
Target of clinical drugs (e.g. antiseizure medications)
how GABA is moved around
drugs of epilepsy target GABARs
Controversies
Some GABAA receptors do not require GABA to open (spontaneous, ligand-independent)
Shifts in GABA receptor expression + function during development (perinatal, pubertal, adult period)
Early on, GABA may be excitatory
have yet to be resolved
GABA might be excitatory in developing neurosystems
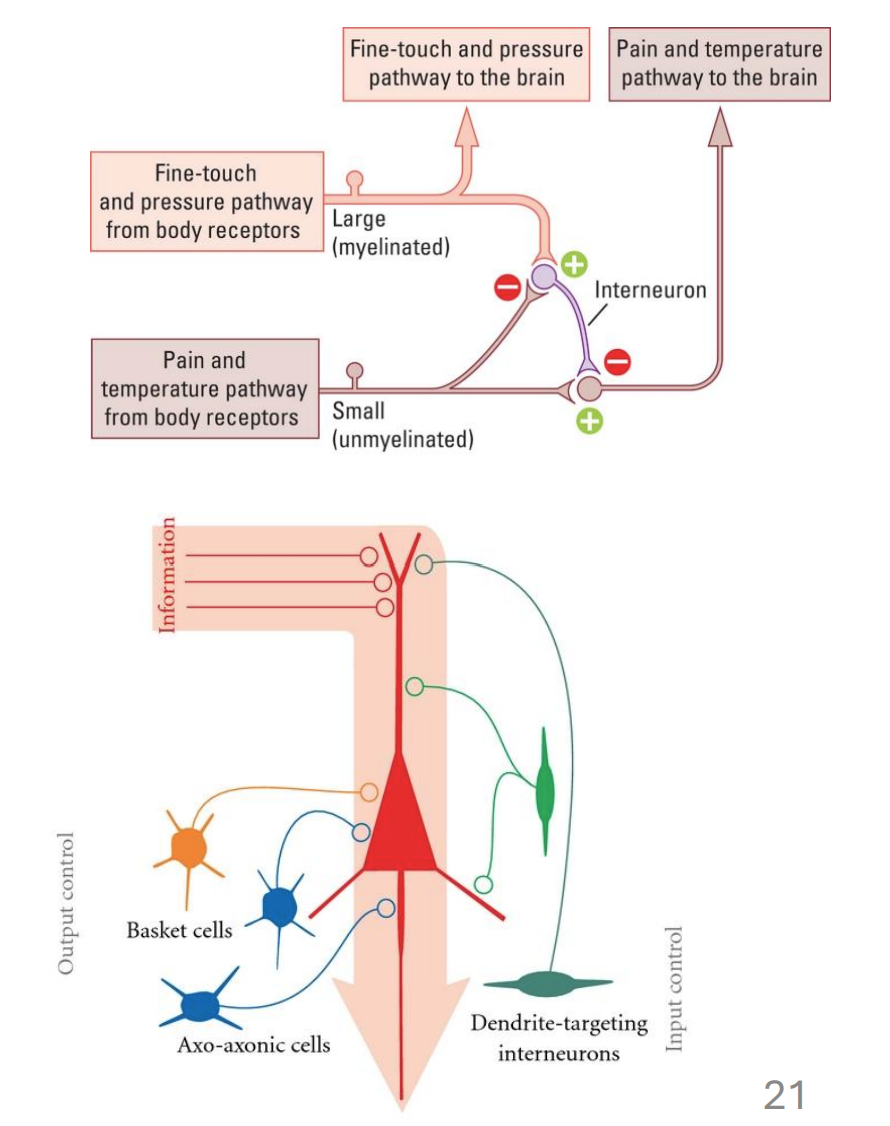
GABA and interneurons
Interneurons are not sensory or motor cells, but modulate their signals (e.g. reflexes)
Synapse on many different compartments
GABA signaling restricts excitability and shapes neuronal oscillations (L07)
inhibitory interneurons can play a role in reflexes
theories that some of these cells contribute to disorders (like SZ)
oscillations = rhythmic synchrony of neuron firing
review
Anti-seizure medications
Drugs that enhance inhibitory transmission via GABA
Affect GABA receptors, GABA transporters
Drugs that reduce excitation via glutamate
Drugs affecting channels in the action potential
Inhibit voltage-gated sodium + calcium channels
for treatment in epilepsy → viewed as disorder of imbalance in excitation + inhibition
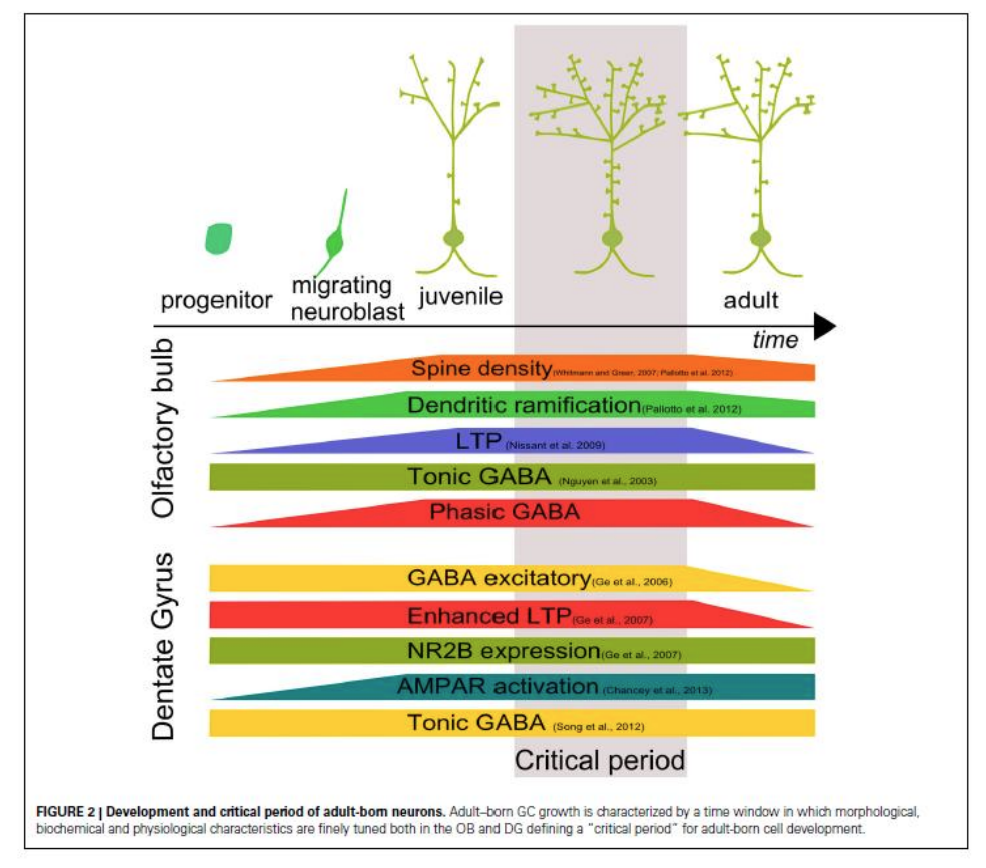
Role in neurogenesis
GABA in neurodevelopment
evidence suggests that GABAR are expressed early on
GABAergic signaling may be significant in early neurons
if we activate, neurogenesis should activate
or KO of GABAR would affect adult neurogenesis
review
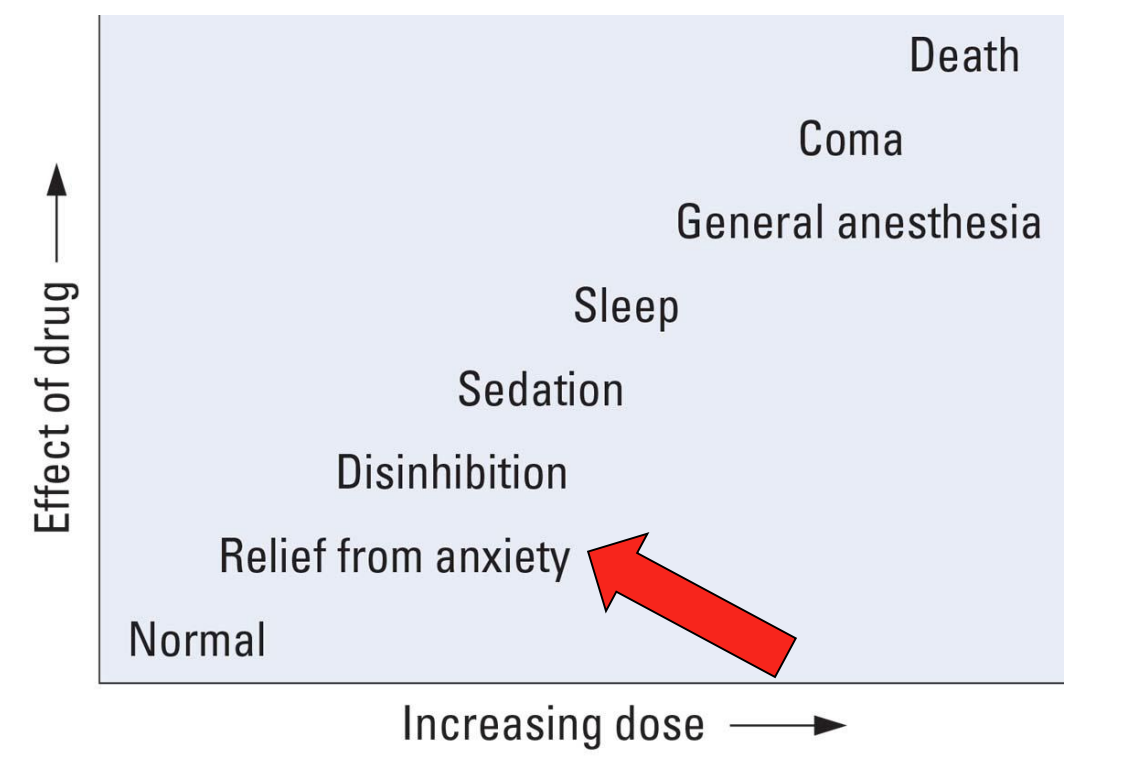
Drugs affecting GABA
Many effects: Anxiolytic, Amnestic, Anesthetic, Sedative-hypnotic, Antiepileptic, Analgesia
Included in this category are benzodiazepines, barbiturates, anesthetics, alcohol and anticonvulsants
Some drugs are more preferred than others for a given effect (e.g. benzodiazepine > barbiturate)
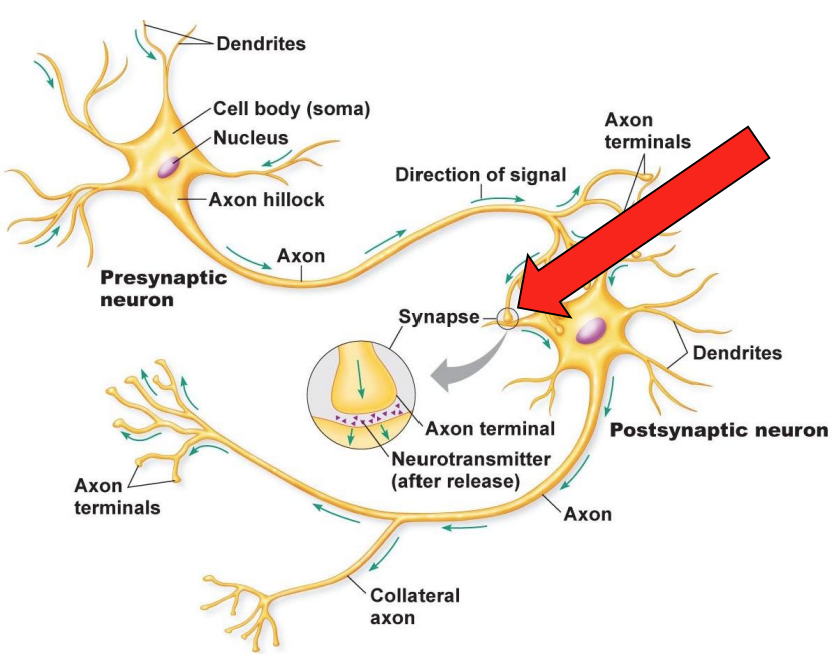
Synapses are modifiable!
Changes in synaptic strength might contribute to learning
strength of signaling from neuron A > B can change
A can become better at activating B = long-term potentiation (synapse b/w A + B gets stronger over time)
Synaptic strengthening
First compelling evidence obtained by Bliss + Lomo (1973) in the hippocampus
High-frequency stimulation of synaptic connections persistently strengthened them
experience-dependent
This phenomenon is called long-term potentiation (LTP) is viewed as a neural correlate of learning
potential for synapse to get stronger is modified by GABA
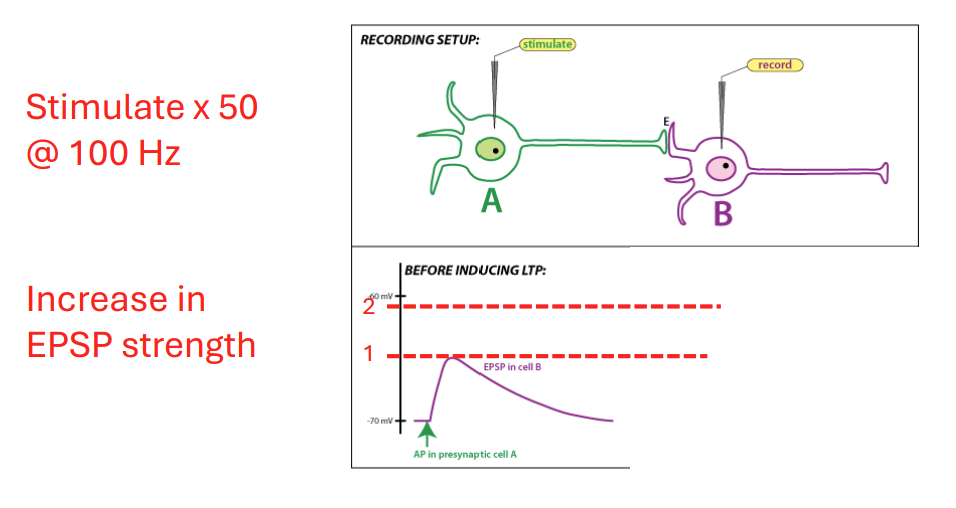
What is LTP?
A signaling to B (done artificially, but in reality A active due to learning)
A weakly activates B under normal conditions
stimulating synapse 100x/sec → synapse gets stronger
LTP and Memory
LTP is seen throughout the nervous system, including the hippocampus, cortex, striatum + spinal cord
LTP is often correlated with learning and memory
Deficits in learning/memory are linked to deficits in LTP
Activity-dependent variations in synaptic strength such as LTP may be a fundamental mechanism by which we acquire and modify all behaviors
Includes pain, motor learning and substance use disorder
in animals with less LTP, memory deficits are seen (rough correlation b/w learning + LTP in animals) → invasive to stimulate + record in humans
although LTP well characterized in HC → plasticity may be seen anywhere (many synapses may get stronger); anything that can change w experience (pain, substance seeking behaviour) may involve LTP
LTP may not be affected by just GABAergic signaling
GABAA receptors restrict LTP
Agonists tend to impair, antagonists increase
Baseline differences (e.g. DG vs. CA1) might be explained by inhibition
GABA agonist → less/no LTP seen
inhibit GABAergic signaling → increases LTP (picrotoxin, PTX, and bicuculline does this)
if you give 1 and 3 to human → inhibitory removal by drugs increases likelihood of seizures
The story so far…
LTP and the hippocampus are both important for learning/memory
GABA constrains hippocampal LTP (agonists ↑, antagonists ↓)
Based on this, you might argue GABA impairs learning and memory
This does happen in a few cases, which we’ll cover first
agonists impaired LTP, antagonists increase LTP
GAPA impairs learning + memory but not in all
GABAA receptors and memory
α5KO mice show improved learning in the Morris water and trace fear conditioning tasks
α5R = extra synaptic receptor
both associated with HC, which is an area where these receptors are expressed
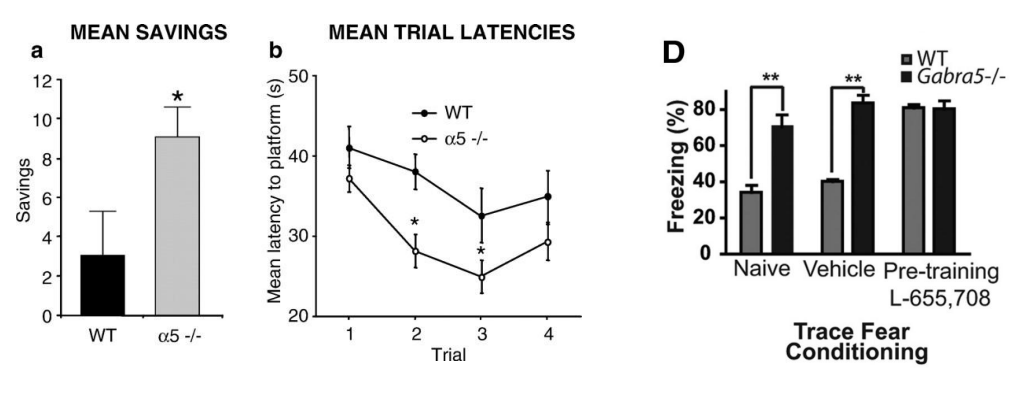
A study in contrast…
δKO mice might show enhanced fear conditioning, too!
again, delta = presynaptic receptor
improved learning + memory in some tasks but not others
GABAA receptors and memory
Drugs which increase GABAA receptor activity (e.g. anesthetics, benzodiazepines and alcohol) impair memory
Many of these memory effects have been linked to activation of α5GABAARs and/or δGABAARs
States of increased GABAA receptor expression/activity are often associated with impaired memory
Inflammation
Traumatic Brain Injury
Reproductive cycle
more GABA bad for learning
activate GABAR + interact them w substances → learning impairments
changes in GABAR expression impairs learning + memory
On reproductive cycles…
As hormones are metabolized to neuroactive steroids, hormonal levels are a factor in GABA receptor function
neuron active steroids → action depends on pathway
peripherally derived (level-dependent)
spike in hormonal levels + rapid drop = significant change in GABAR (specifically gaba delta a receptors to drugs)
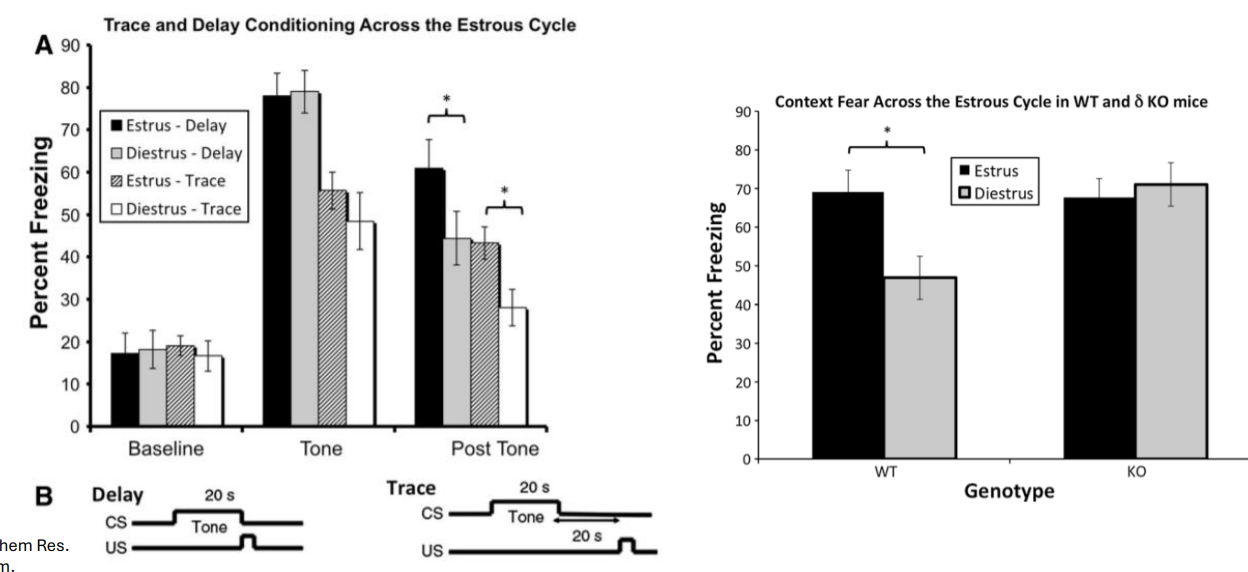
Role of reproductive cycle
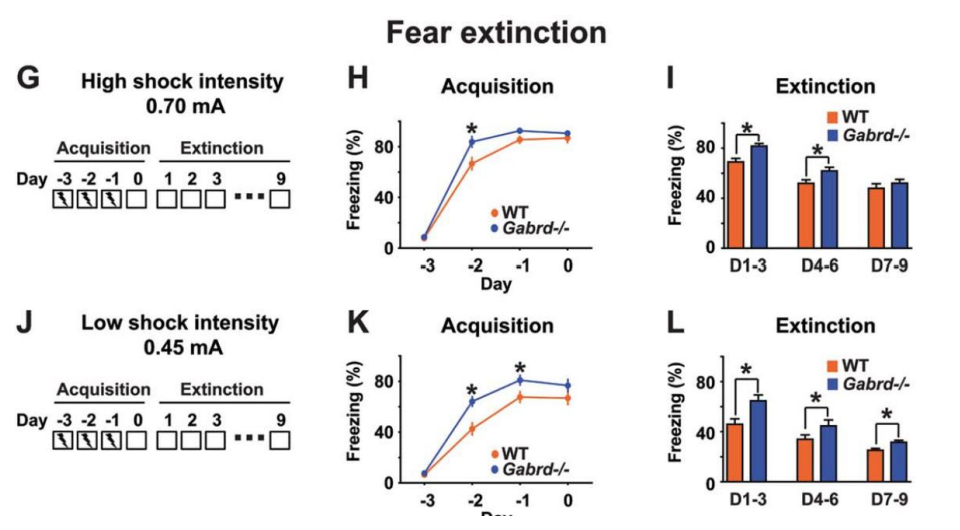
Peak in steroid levels during diestrus in females linked to impairments in memory; changes absent in δKO
they do worse at fear conditioning likely due to hormonal variations, having consequences for activity + receptors
WT mostly impaired → KO won’t (deleting receptors → less significant effect)
also receptors important in postpartum, puberty, etc.
review
Simple principle of “lower GABA, better memory” doesn’t always hold.
Some types of memory might require GABA signaling and be impaired by its removal.
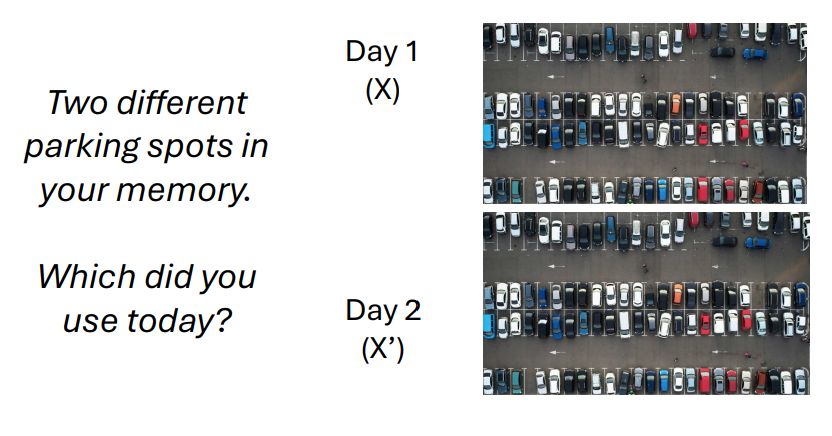
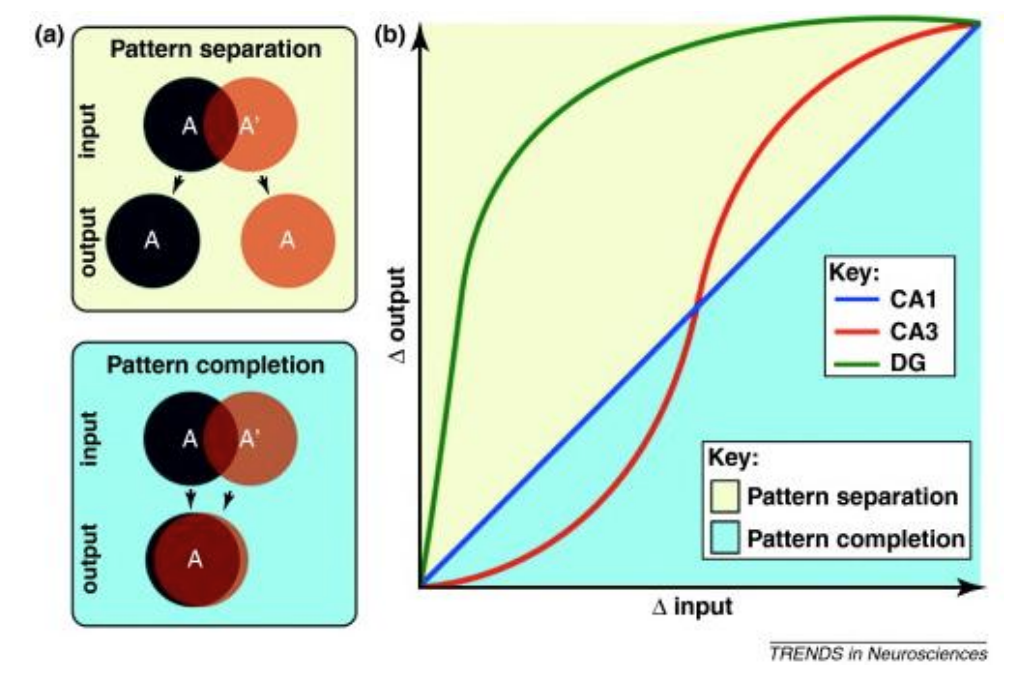
Consider the following task… → Distinguishing experiences
X and X’ might each have neural representations
Large differences (d = X-X’) might be useful in discriminating them
To maximize discrimination, the brain might transform similar inputs (X and X’) into different outputs (X and Y)
This ability is termed pattern separation
discrimination tasks may be better with GABA inhibitory signaling
brain takes similar stimuli (visually) and stores is diff in brain (to maximizing differences for late)
orthogonalization = making inputs different = pattern separation
Pattern separation
Thought to involve the dentate gyrus (DG) of the hippocampus
DG key in pattern separation - ideal for orthogonalization in this brain area
GABA and memory discrimination
Inhibition is thought to be critical to pattern separation; loss of it is associated with impaired discrimination
Hyperactivity in the DG in humans is associated with reduced pattern separation and may contribute to cognitive impairment in dementia
α5KO and δKO mice show poor pattern separation and treat different environments as being similar
In both cases, receptors in the DG are implicated
information coding could never be selected w absence of inhibition
hyperactive DG = poor performance in discrimination in humans → same effect on KO mice as well
better fear conditioning but poor pattern separation → leads to concept that inhibition may be important but may also impair
Role of GABA depends on…
The receptor subtype involved (α5 and δ receptors are different)
The learning task (e.g. FC/NOR vs. pattern separation)
Sex of animal (males and females, linked to hormones)
Physiological state (e.g. puberty, stress, reproductive, again due to hormones)
Anxiety disorders
Generalized Anxiety Disorder
Panic Disorder
Phobias
Related conditions, but now independent in the DSM-5, are obsessivecompulsive disorder (OCD) and post-traumatic stress disorder (PTSD)
Role of the amygdala
Limbic system structures (amygdala, hypothalamus, orbitofrontal cortex, cingulate gyrus + hippocampus)
emotional processing, fear-conditioning → amygdala
inhibition of such cells → expect less fear and anxiety
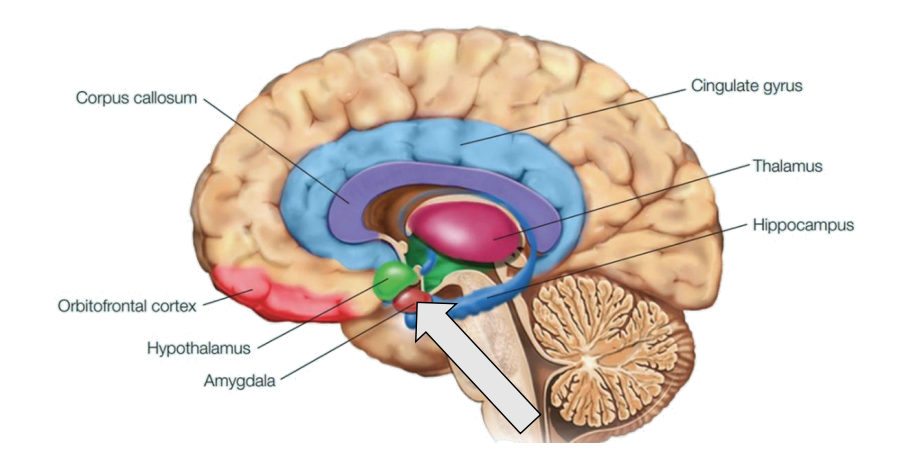
The Amygdala and Anxiety
Activated during arousing states (e.g. emotion) and other situations
Lesion can reduce fear/anxiety (e.g. Patient SM)
Selectivity inhibiting the amygdala (e.g. with drugs) reduces anxiety
Many anxiolytics increase GABAA receptor activity (see L01) and perhaps work by affecting the amygdala
Is it the case that more GABA = better mood?
short term, benzodiazepine
long term, SSRIs → better tolerated + fewer risks
GABA and mood
Correlative evidence in humans and experimental evidence in animals
In humans, there may be lower expression of GABAA receptors in psychological disorders
GABA levels may also be reduced (e.g. depression)
Reduced levels of δ and γ2 subunit-containing GABAA receptors are linked with anxiety
GAD65-KO mice also have elevated anxiety levels
variations in GABA signaling may lead to anxiety?
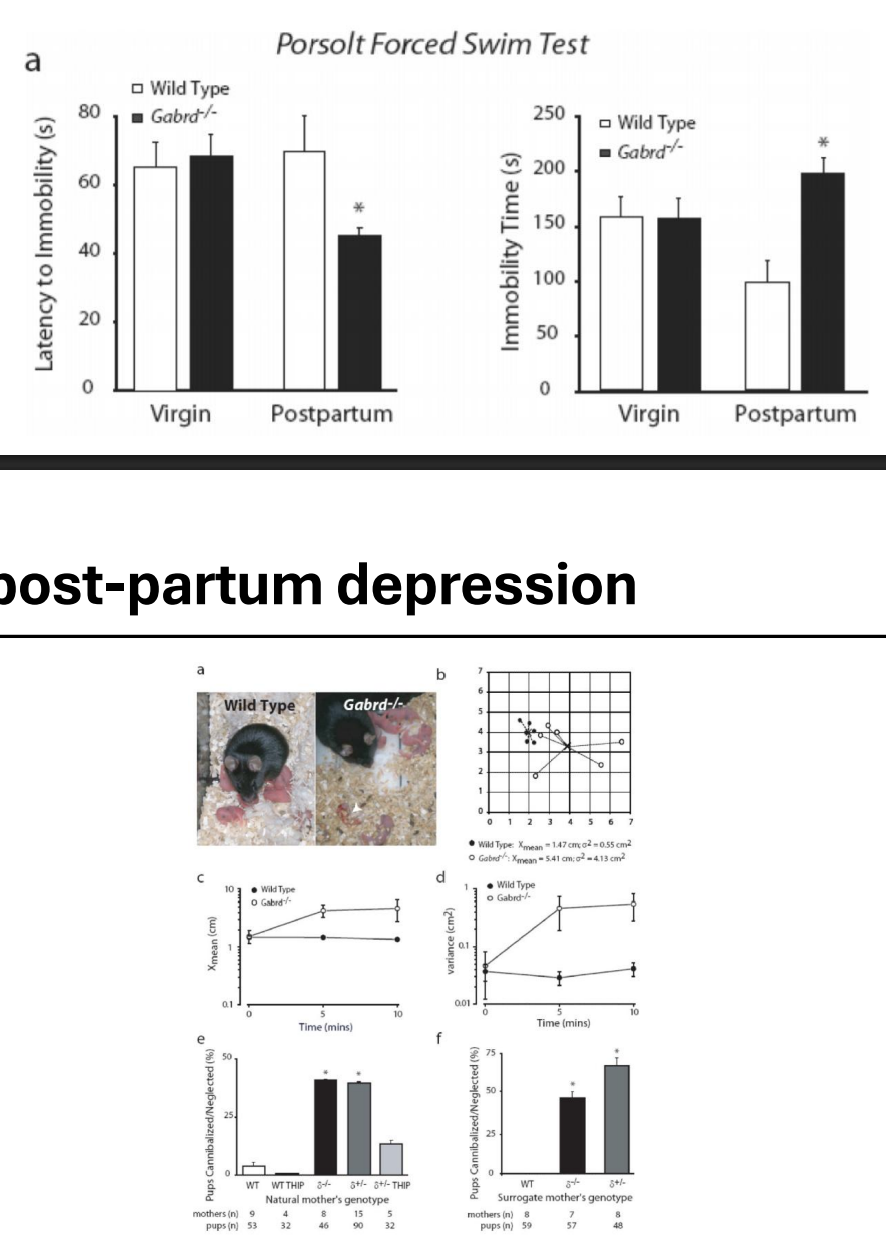
δKO + post-partum depression
Deletion of the δGABAA receptor subunit is associated with depressionlike behavior* post-partum
reproductive cycle → associated w changes in GABAergic signaling due to changes in steroids…?
deletion of GABAR = post-partum like phenotype
pups survive less + die at higher rates + build lower quality nests
Other cases of variation
receptor sensitive to hormonal levels →
Summary
Natural variations in GABA signaling might contribute to natural variations in mood (puberty, post-partum…)
Increased GABA signaling is associated with reduced anxiety (in general)
Decreased GABA signaling is associated with increased anxiety and depression
Modulating GABAA receptors w/drug affects anxiety*
treat anxiety thru substances that affect receptors
Drugs affecting GABA
increasing dosages → different effects to GABAergic signaling
When it comes to anxiety…
…there are many drugs possible, not just GABA drugs
What is pain? + Types of pain
Private experience (sensory and emotional) associated with actual or potential tissue damage (belief of tissue damage)
Adaptive, allows us to identify danger + withdraw
Types of pain:
Acute pain is brief, and overlaps with the healing process (associated w injury)
Normal and more manageable
Chronic pain is persistent (>3 months) beyond healing period (knee if fine but still experience pain)
Many disorders include chronic pain as a symptom (e.g. diabetic neuropathy, migraine, fibromyalgia, arthritis…)
useful signal bc it is unbearable
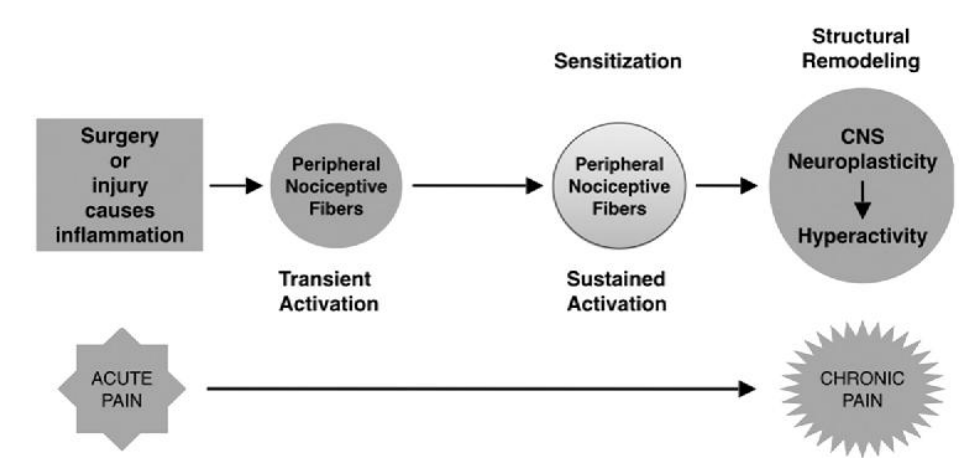
Why do we get chronic pain?
Following injury, changes in nociceptive signaling system can occur
on at wrong times, and too on/active at right times
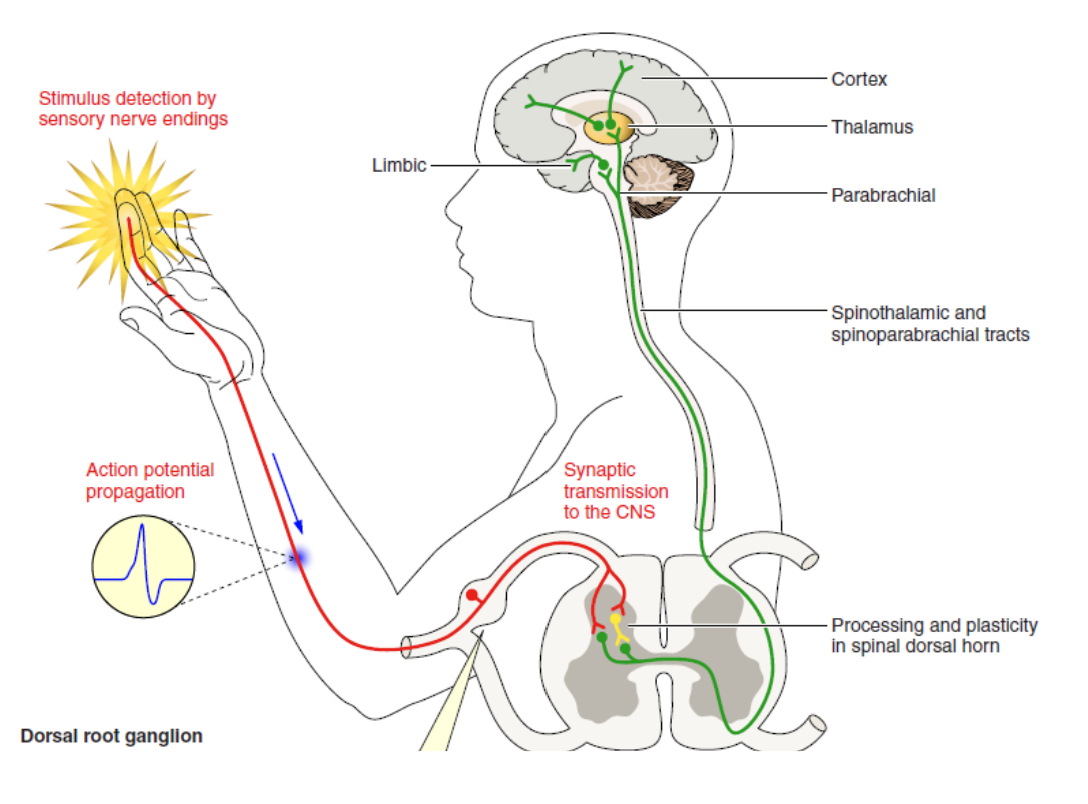
Pain pathways
The primary afferent – second order sensory synapse in the dorsal horn is key + early
The activity of dorsal horn neurons is modulated by other cells (esp. inhibitory interneurons)
primary afferent into SC
circled - may be interneurons present
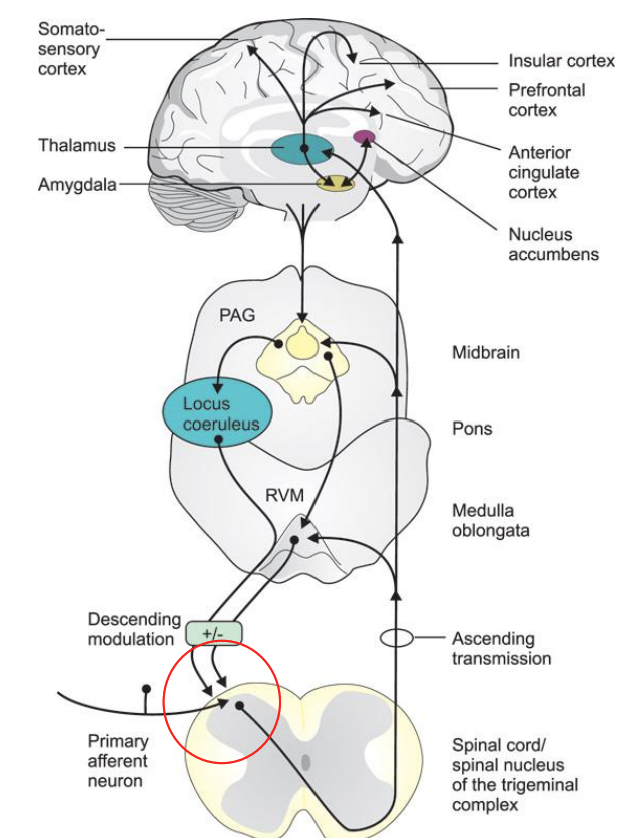
Changes in inhibitory balance
Death of interneurons could increase pain (due to regulation in pathway)
With changes in transport across the membrane, inhibitory signals could “lose their value”, becoming insufficiently inhibitory or even excitatory
Even if inhibition remains stable, increases in excitation could occur that amplify pain-related signals (central sensitization)
inhibitory signals could stop being inhibitory (removing gradients bc ions are no longer being conducted)
weaker ones may be stronger (review)
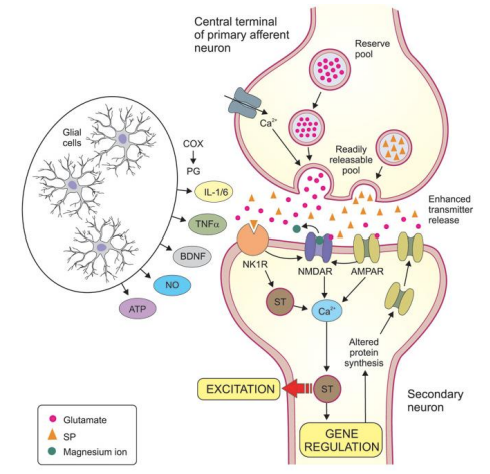
Central sensitization
Signaling at this synapse may increase in strength after injury or other forms of stimulation.
DNM diagram
Drugs for pain
GABA signaling may regulate pain and GABA receptors are a potential target for analgesic drug
Pharmacological activation of δGABAA receptors, for example, can have analgesic effects
Drugs well-known for their analgesic effects, including gabapentin, might work in part by increasing δGABAA receptor expression
certain drugs could be analgesic effects through GABAergic signaling indirectly