CM II Week 5 (CVA & TIA)
1/62
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
63 Terms
time based definition of TIA
➢Sudden onset of focal neurologic deficits lasting <24 hours
➢Caused by transient decrease in blood flow leading to ischemia without infarction
➢Arbitrary end point
tissue based definition of TIA
➢Transient episode of neurologic dysfunction causing ischemia of CNS (brain, spinal cord, retina) tissue without infarction
➢Tissue injury confirmed or ruled out on neuroimaging
➢Biologic end point (tissue injury)
TIA definition
TIA is defined as a clinical stroke syndrome that resolves in <24 hours without radiographic evidence of infarction
risk of stroke/MI remains high for pts who have had a TIA up to 10 years after
The ________ predicts the risk of subsequent stroke following a TIA
ABCD2 score predicts the risk of subsequent stroke following a TIA
TIA Management: Low Risk
-ASA or plavix
-Afib: consider anticoagulants
-high intensity statin
-EKG and Echo
-Carotid US
TIA management: moderate to high risk management
-admission
-permissive HTN to 220/120 and then gradual lowering over 24 hours (too fast: infarction)
-DAPT x21 days, then ASA indefinitely
-high intensity statin
-EKG & Echo
-Carotid US
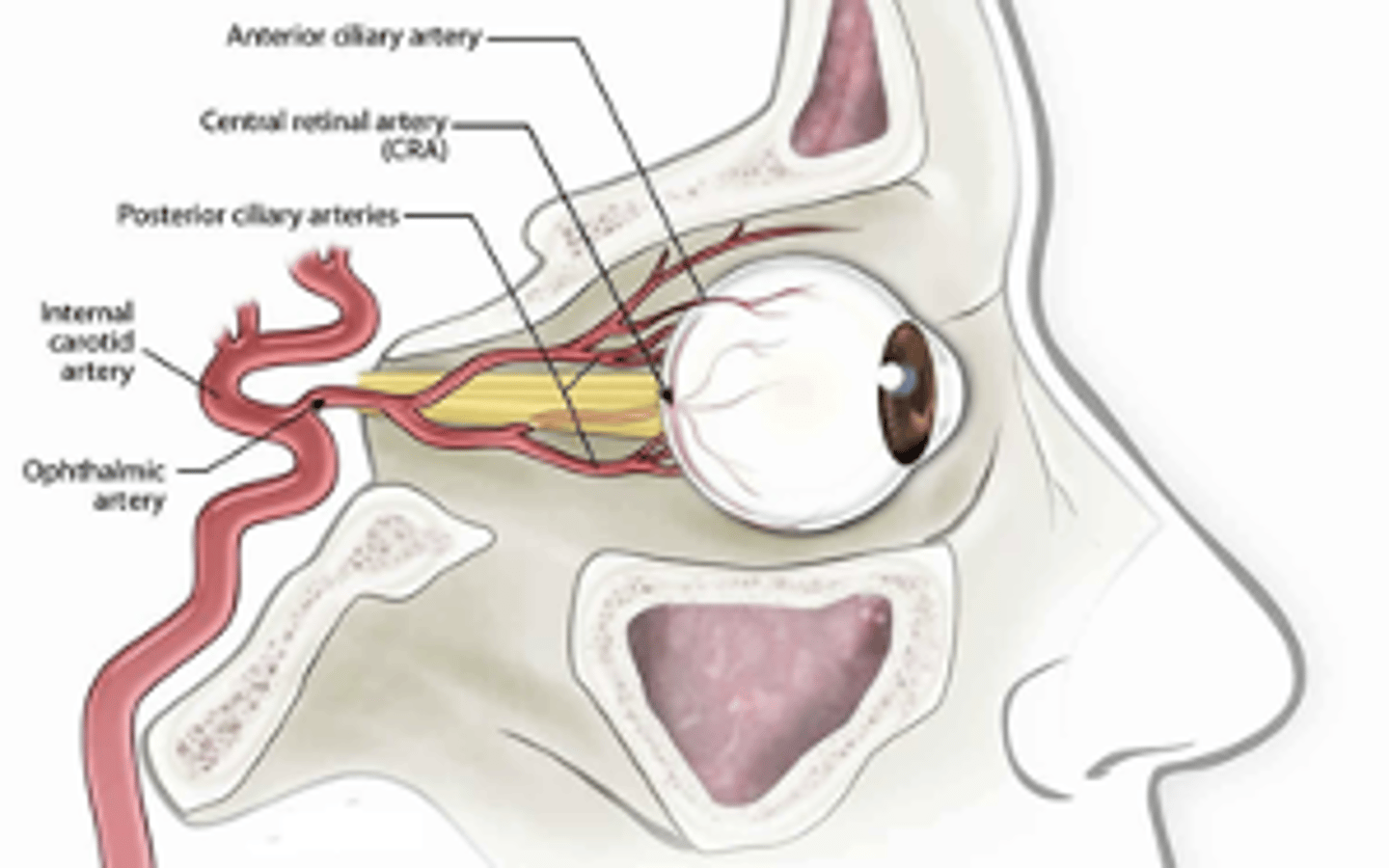
amaurosis fugax is a TIA of ____________, which causes
- the retina; transient occlusion of the retinal artery
- Leads to monocular vision loss lasting ~10 minutes
- Described as a "window shade or curtain" over the eye
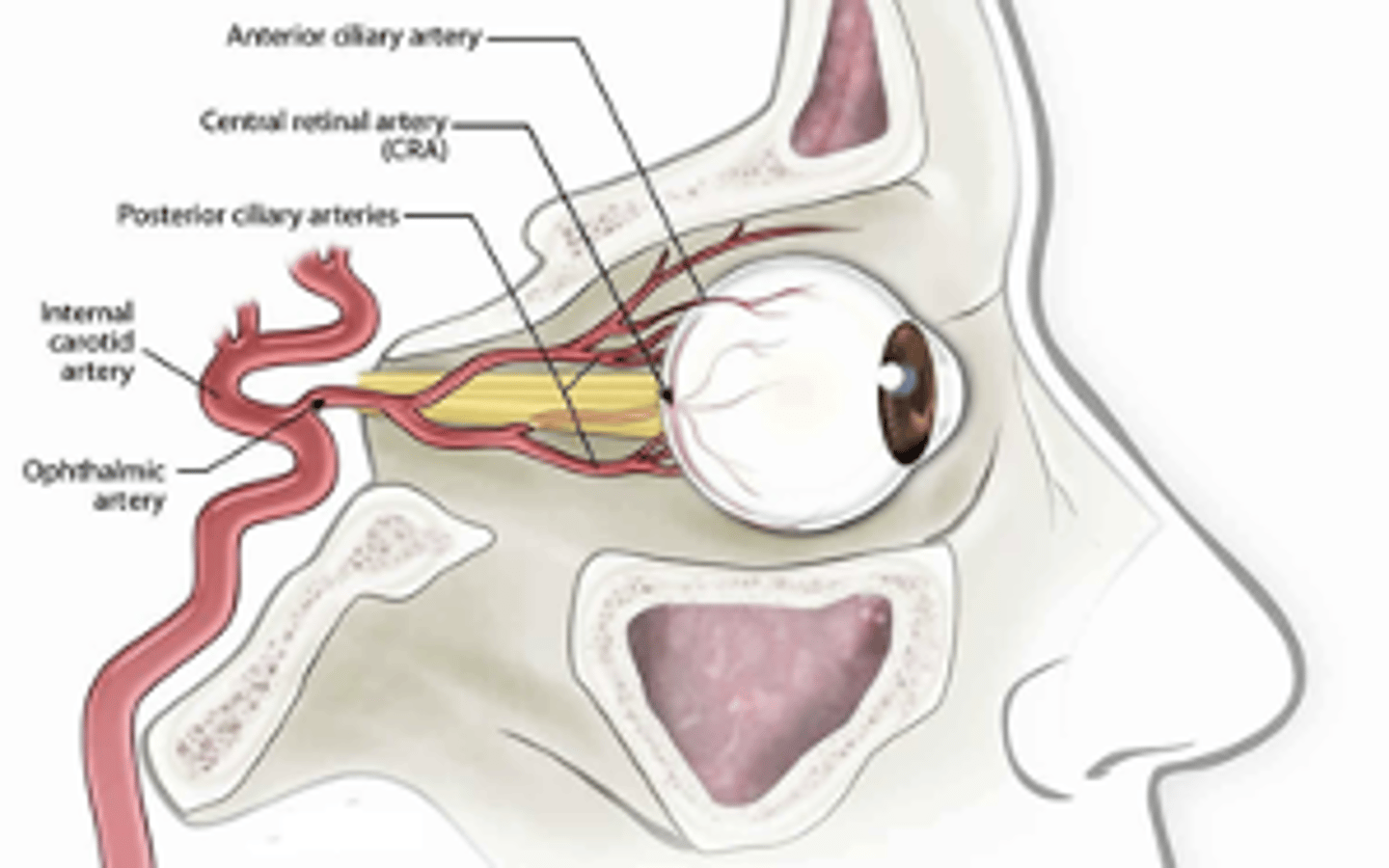
amaurosis fugax is most commonly caused by
Most commonly caused by emboli from the ipsilateral internal carotid artery
amaurosis fugax is a warning sign for
Warning sign for impending retinal or cerebral infarction
amaurosis fugax workup
same as TIA
CVA: Ischemic stroke
➢Acute onset of symptoms, maximal at time of onset
➢Most commonly caused by decreased perfusion from a blood clot in the vessel
➢Symptoms associated with affected vascular territory
CVA: Hemorrhagic stroke
➢Acute onset of symptoms, crescendo in nature
➢Caused by intraparenchymal hemorrhage (IPH), epidural hemorrhage (EDH), subdural hemorrhage (SDH), or subarachnoid hemorrhage (SAH)
➢Associated with sxs of elevated ICP: headache, vomiting, depressed LOC
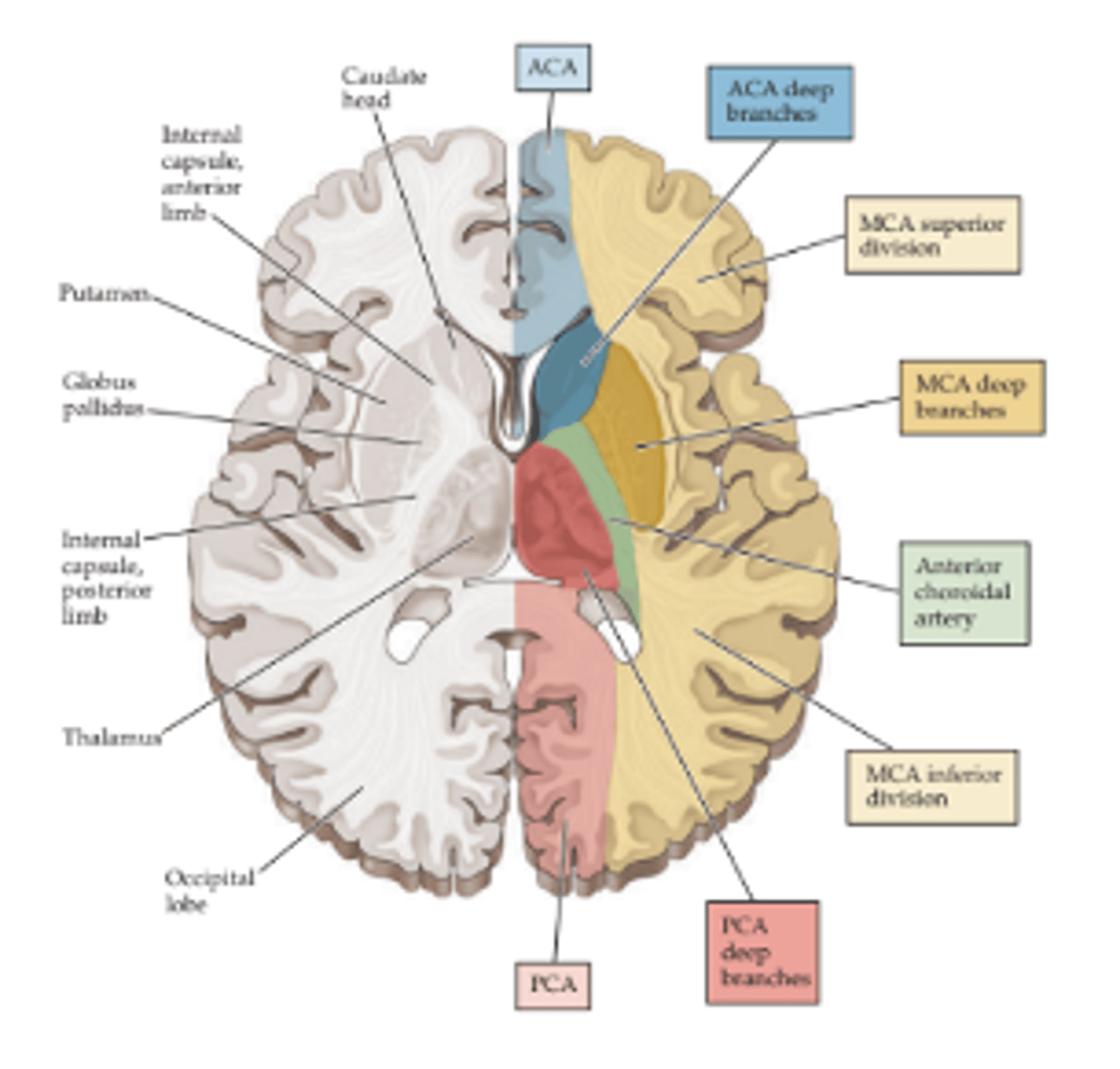
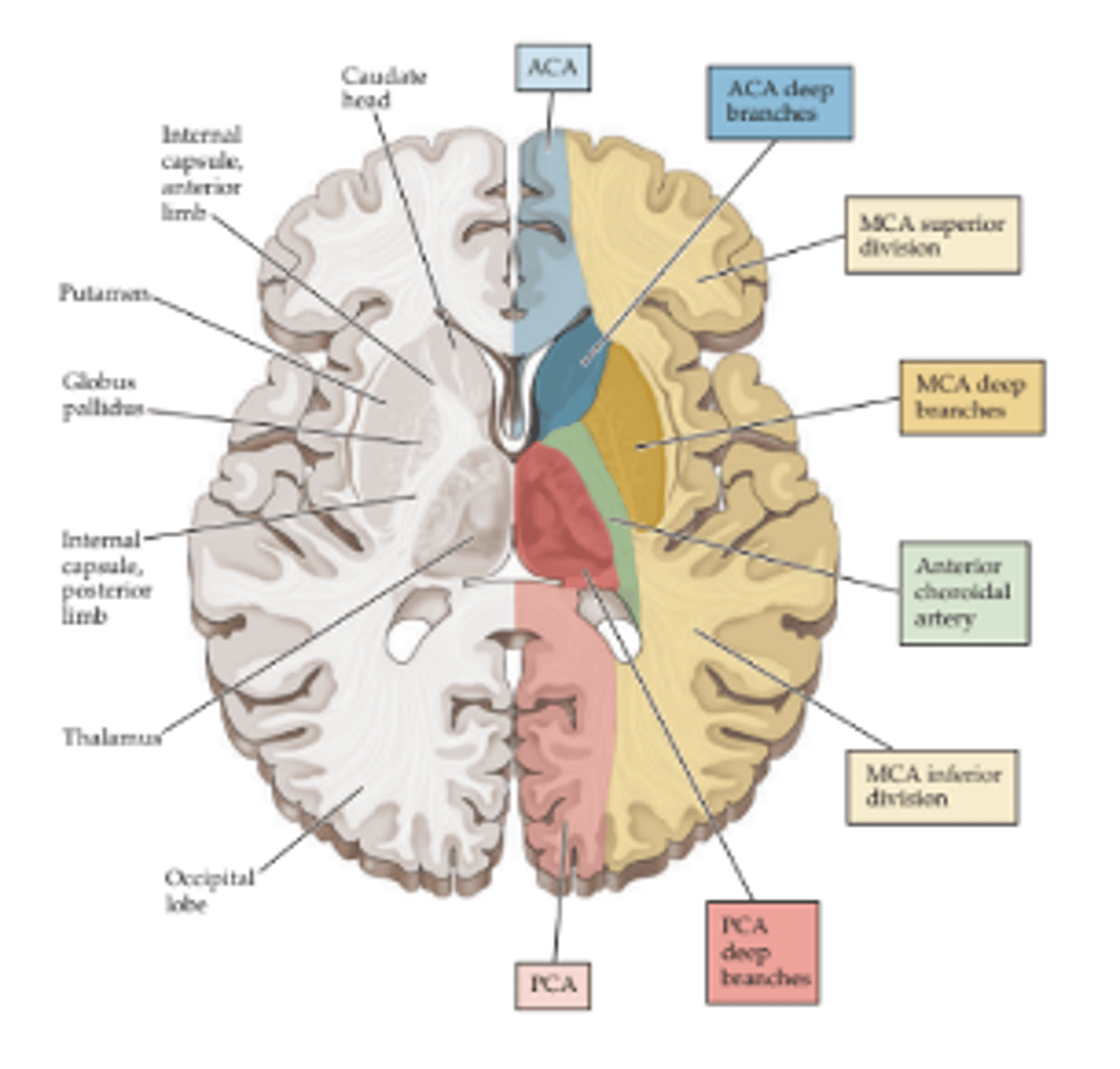
anterior circulation acute ischemic stroke
Internal carotid artery (ICA)
Middle cerebral artery (MCA)
Anterior cerebral artery (ACA)
posterior circulation acute ischemic stroke
Vertebral artery
Basilar artery
Posterior cerebral artery (PCA)
Cerebellar arteries (PICA, AICA, SCA)
Middle Cerebral Artery Syndrome
Left MCA stroke
➢Right facial droop
➢Right upper > lower extremity weakness
➢Right hemisensory loss
➢Right hemianopia
➢LEFT gaze preference
➢Expressive vs Receptive Aphasia (language)
Middle Cerebral Artery Syndrome
Right MCA stroke
➢Left facial droop
➢Left upper>lower extremity weakness
➢Left hemisensory loss
➢Left hemianopia
➢RIGHT gaze preference
➢Neglect (spatial awareness)
if i have a right MCA stroke, i have a ________ gaze and weakness on ________ side
right (eyes drift toward location of stroke); left upper extremity weakness
*Neglect (spatial awareness)*
posterior circulation strokes
The vertebrobasilar system supplies structures of the posterior fossa, including the cerebellum and brainstem
Warning signs of vertebrobasilar ischemia
dizziness, diplopia, dysarthria, dysphagia, ataxia, unsteady gait, and somnolence
what suggests brainstem involvement with Posterior Circulation Strokes?
Crossed signs, cranial nerve involvement, and eye movement abnormalities strongly suggest brainstem involvement
Requires immediate medical attention to prevent further brainstem infarction, coma, and death
Cerebellar Stroke
risk?
Large cerebellar strokes are at high risk of malignant edema and brainstem compression
Cerebellar stroke: what is concerning with this?
Compression of the 4th ventricle can lead to obstructive hydrocephalus and herniation
managing cerebellar stroke
Manage medically with hyperosmolars (mannitol) or hypertonic saline (23%) to draw fluid off the brain
Clinical deterioration prompts emergent neurosurgical consultation for suboccipital craniectomy (SOC) --> take skull off = relieve pressure
Lacunar Infarcts
Small (2-15 mm in diameter) subcortical stroke caused by occlusion of a single perforating branch of a large cerebral artery
cause of lacunar infarcts
hypertension
microatheroma
embolism
Subcortical structures involved with lacunar Infarcts
➢Basal ganglia
➢Thalamus
➢Internal capsule & corona radiata
➢Brainstem
Five Classic Lacunar Syndromes: Pure Motor Hemiparesis
Pure motor hemiparesis
➢ Most common
➢ Contralateral weakness
➢ Internal capsule
Five Classic Lacunar Syndromes: Pure Sensory
Pure sensory
➢ Contralateral numbness
➢ Thalamus
Five Classic Lacunar Syndromes: Sensorimotor
Sensorimotor
➢ Contralateral weakness & numbness
➢ Internal capsule & thalamus
Five Classic Lacunar Syndromes: Ataxic Hemiparesis
Ataxic hemiparesis
➢ Ipsilateral weakness and ataxia
➢ Gait deviation towards affected side
➢ Internal capsule or pons
Five Classic Lacunar Syndromes: Dysarthria Clumsy Hand
Dysarthria clumsy hand
➢ Facial weakness, dysphagia, & dysarthria
➢ Hand weakness especially with writing
➢ Any subcortical structure
Patient is a 63 year old male, hx HTN, DM, and Afib, who presents with left sided weakness and slurred speech.
LKW at 10 PM by his wife while getting ready for bed. About 5 minutes later, she noticed a left facial droop, left sided weakness, and unintelligible speech.
Patient arrives to the ED by EMS at 11 PM.
You are the receiving ED provider for this patient, what do you do?
stoke alert
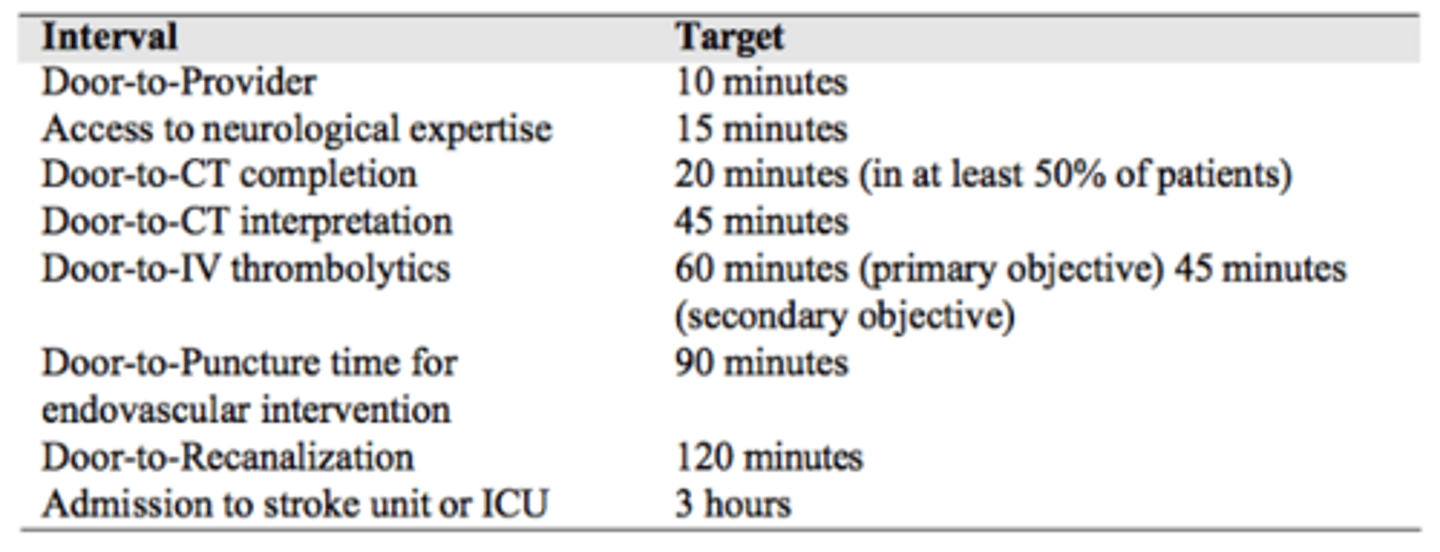
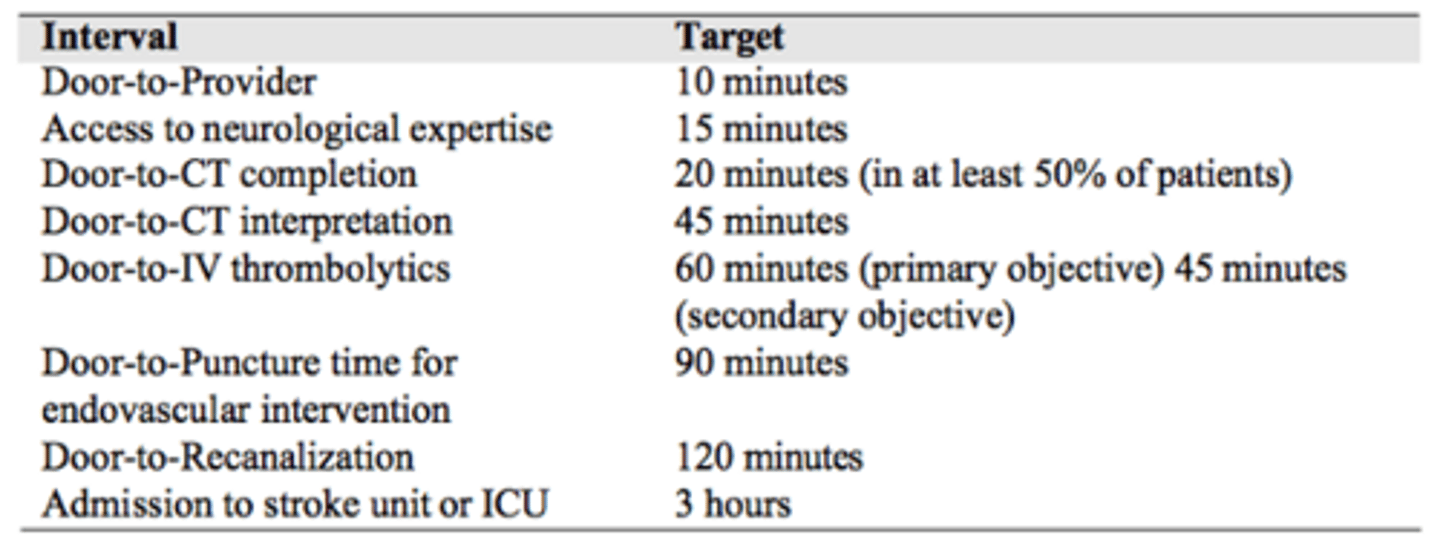
Acute Ischemic Stroke Diagnosis: Time is Brain
TPA OR TNK = most accepted med
and door to needle time <60 minutes
acute stroke diagnosis - time is brain
acute ischemic stroke management (last known well, time <4.5hrs)
Thrombolytics (tPA) should be considered to all patients with a LKW time <4.5 hours
BP goals:
- BP <220/110 for non-tPA candidates (incr cerebral perfusion)
- Blood pressure <185/110 for tPA candidates to lower the risk of hemorrhage
Patients with a LKW time <24 hours with the presence of a large vessel occlusion (LVO) should be considered for
thrombectomy
Acute Ischemic Stroke Management:
Door to puncture time is ____ minutes, while door to recanalization time is ____ minutes
Door to puncture time is 90 minutes, while door to recanalization time is 120 minutes
All post-thrombectomy patients will be monitored in the neuro ICU
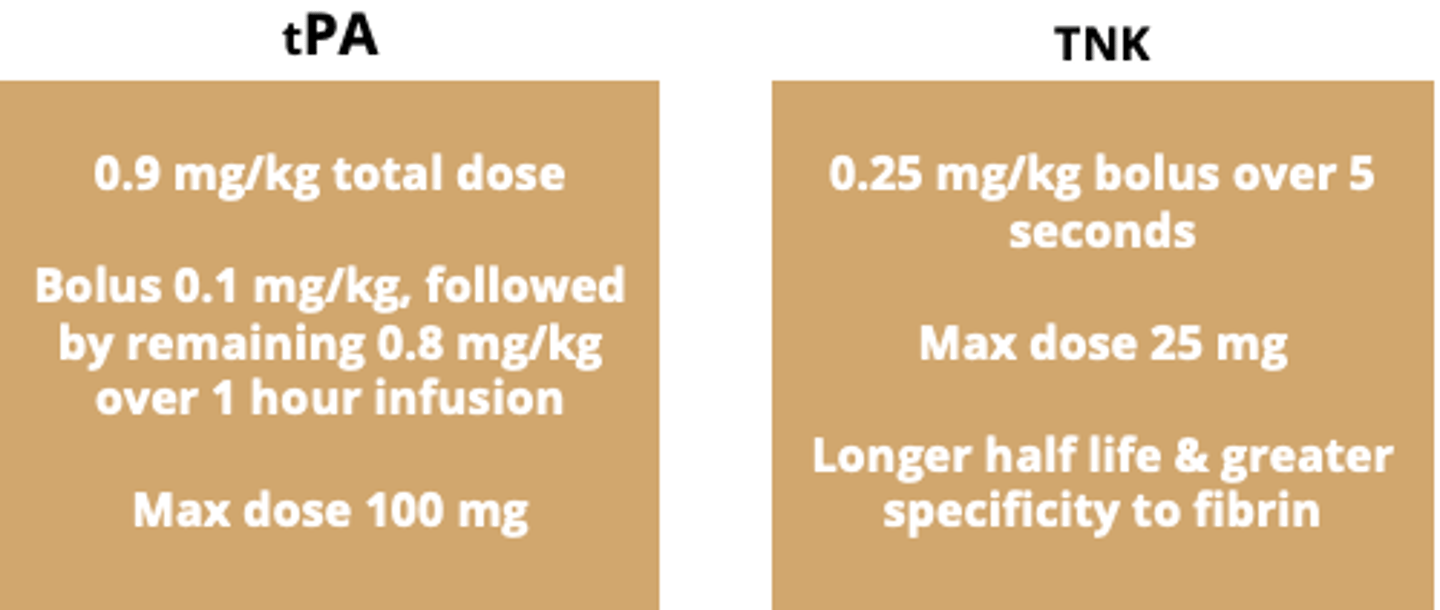
IV Thrombolytics (tPA vs TNK)
tPA = angioedema ipsilateral to the side of the stroke is a ADR (not well understood)
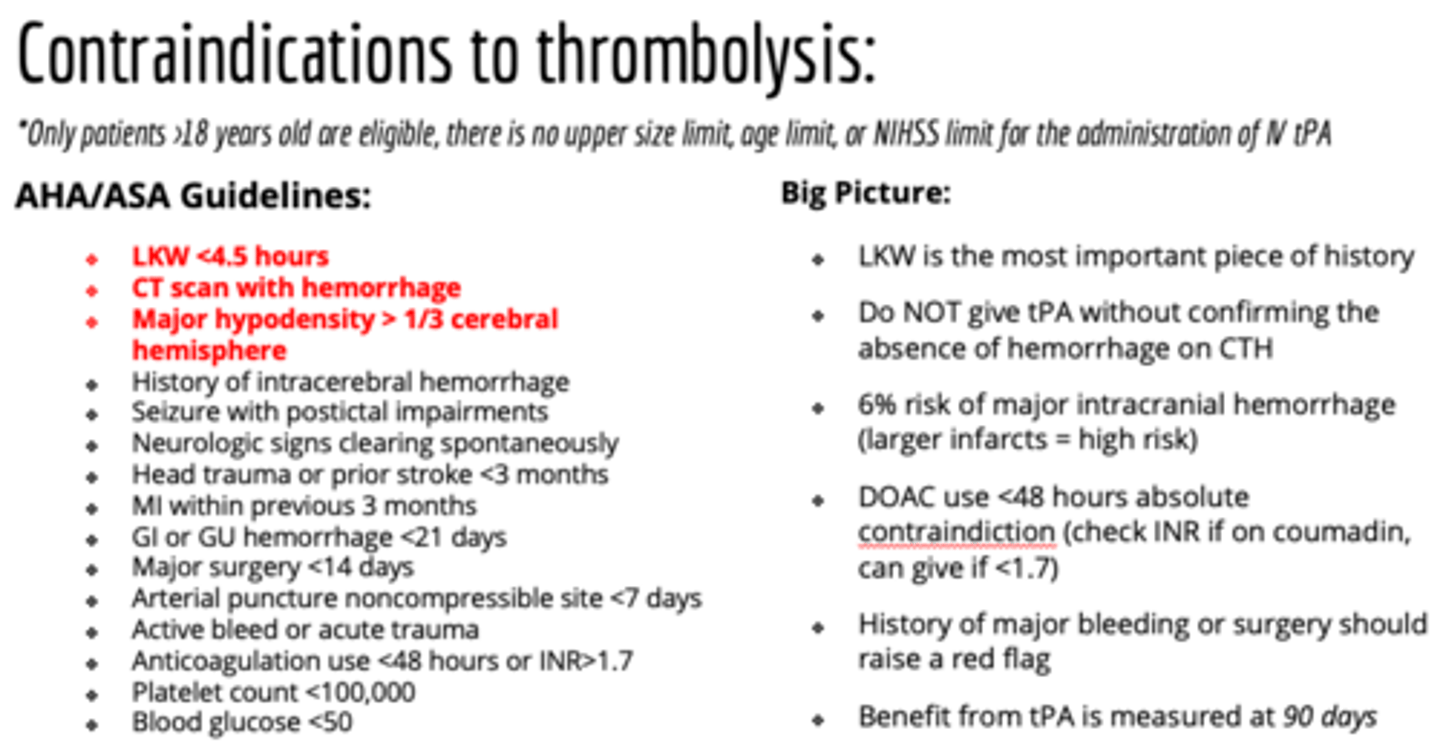
Thrombolysis: AHA/ASA Guidelines
*Only patients >18 years old are eligible, there is no upper size limit, age limit, or NIHSS limit for the administration of IV tPA
- LKW <4.5 hours give tPA/TNK. not normally done with LKW >4.5 hrs.
- CT scan with hemorrhage
- Major hypodensity > 1/3 cerebral hemisphere
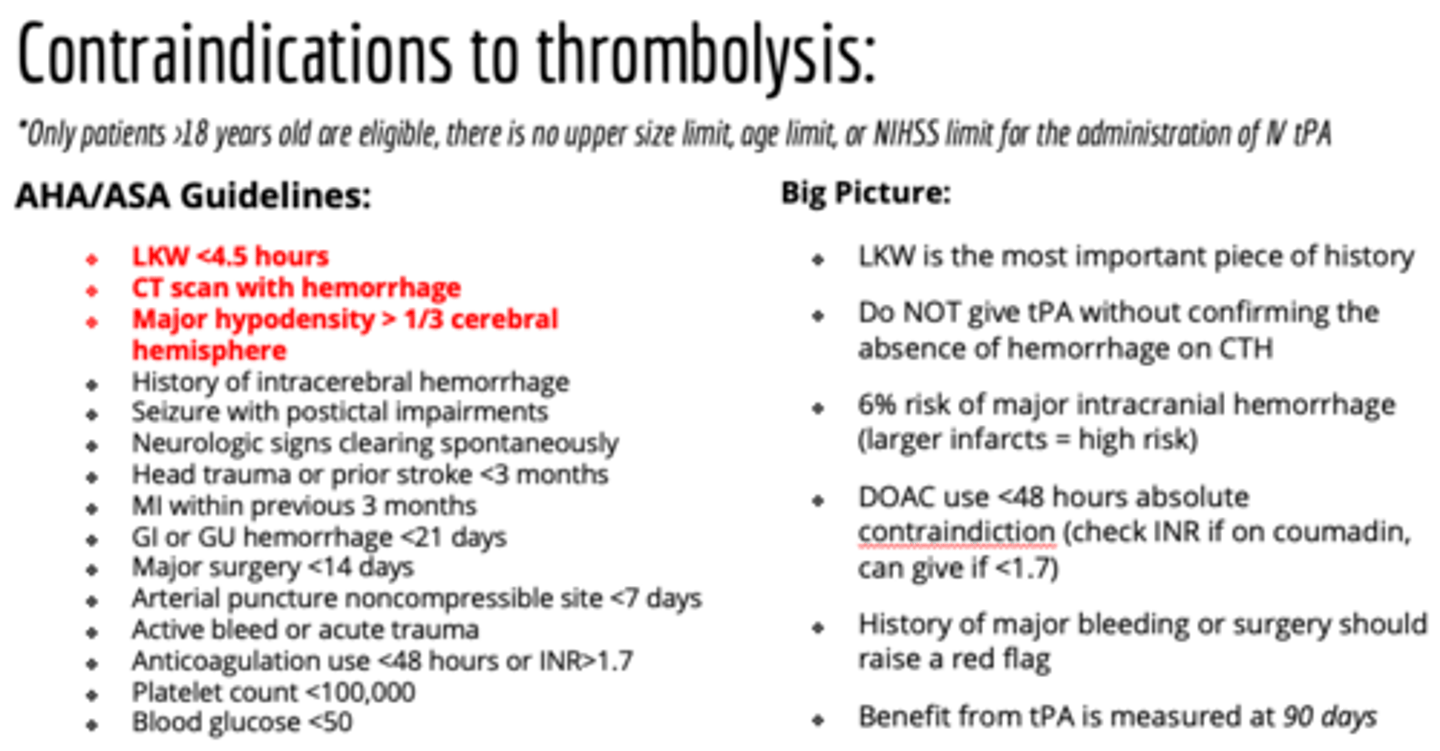
contraindications of thrombolysis (IV tPA) - big picture
- LKW is the most important piece of history
- Do NOT give tPA without confirming the absence of hemorrhage on CTH (blood in brain = do NOT give)
- Healthy brain tissue will not bleed, infarcted tissue has potential to bleed
- Hx of major bleed or surgery should raise a red flag
- Always check platelets & coags
- Reconsider tPA if symptoms resolving
Large Vessel Occlusion (LVO)
what vessels? % of strokes?
Occlusion of large cerebral artery
➢ICA
➢MCA (M1 or proximal M2 segment)
➢Basilar artery
15-20% of presenting strokes
Large Vessel Occlusion (LVO) associated with?
large core infarcts resulting in significant clinical deficits
Large Vessel Occlusion (LVO): Mechanical thrombectomy =
definitive treatment
Mechanical Thrombectomy inclusion criteria
➢LKW within 24 hours
➢NIHSS 6 or greater
➢Presence of LVO
Mechanical Thrombectomy Timing
➢LKW <6 hours straight to thrombectomy
➢LKW 6-24 hours obtain CT perfusion
Mechanical Thrombectomy Risks
➢Reperfusion injury
➢Iatrogenic dissection
➢Distal embolization
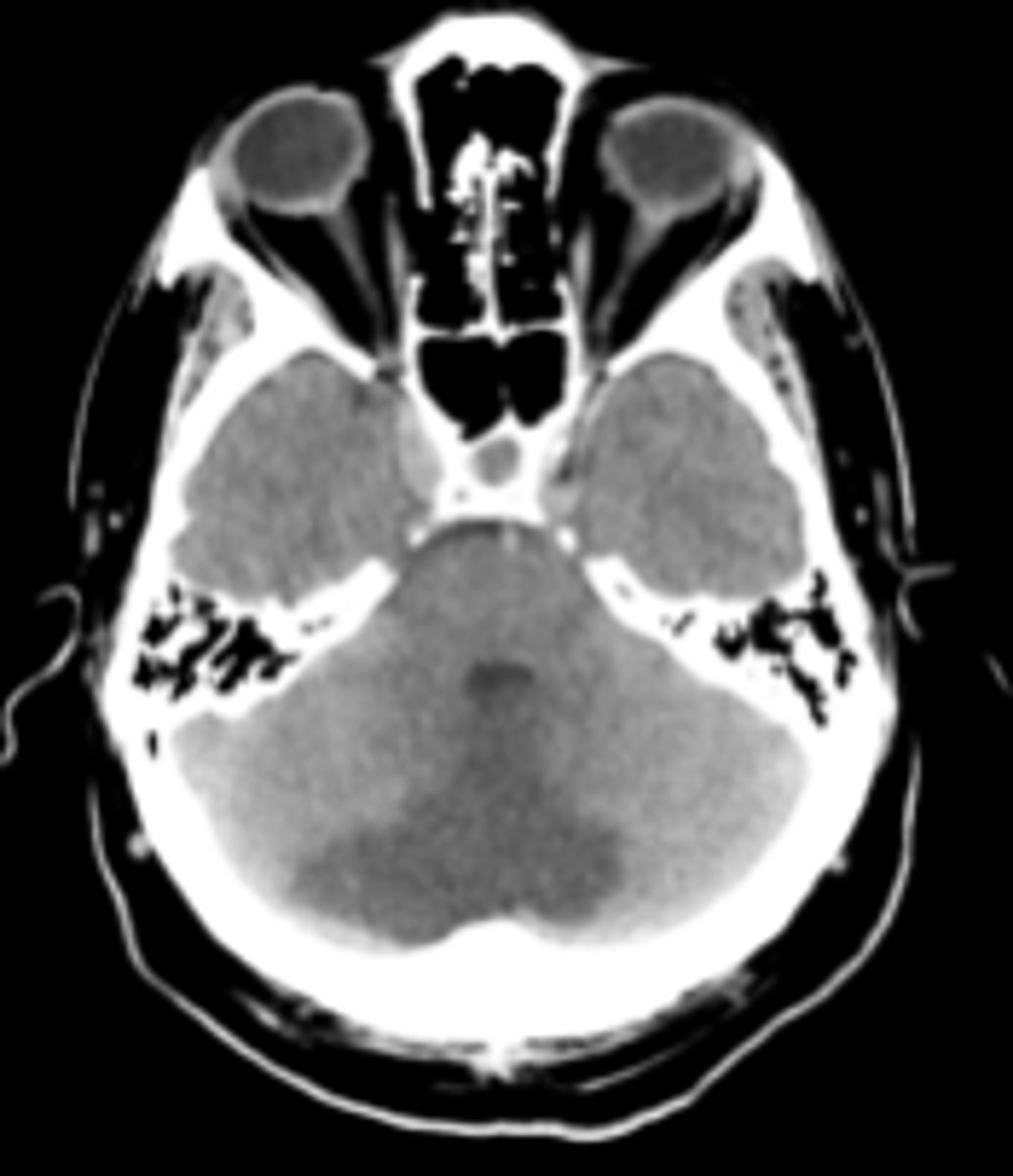
Patient is a 58 year old male with PMH of HTN, who presents with a sudden onset severe headache, not relieved with ibuprofen. His wife reports he later awoke in the middle of the night with a worsening more diffuse headache. Patient took 325 mg of aspirin x 3 for pain (LOTS). He suddenly projectile vomited, prompting his wife to activate EMS.
On arrival to the ED, patient is complaining of a 10/10 headache unlike any prior headache. On exam, he looks ill-appearing and lethargic.
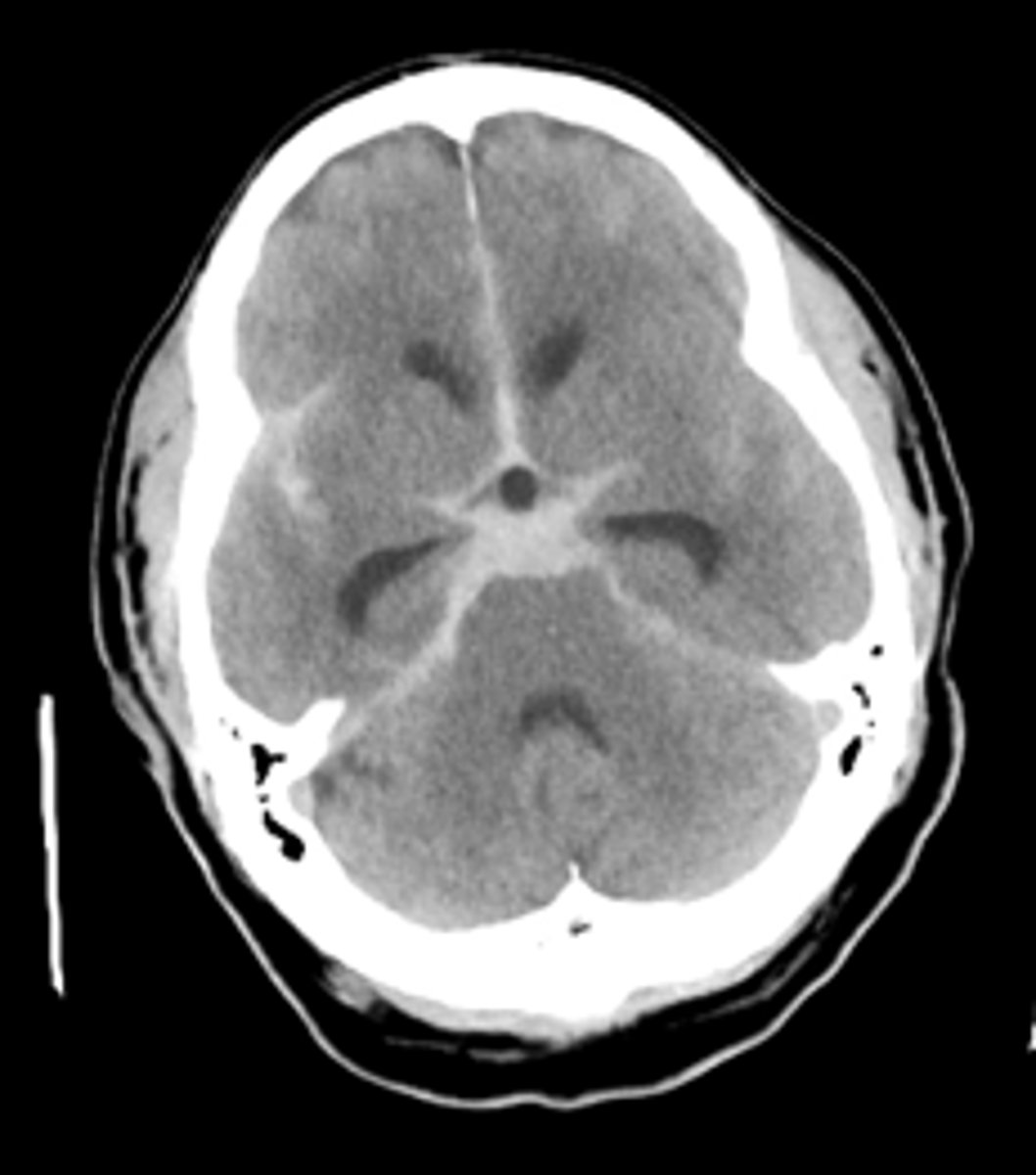
You are the neurology PA on call overnight, what is the first study you order?
CT dry scan... looks like "clown nose", star of death
subarachnoid hemorrhage
(worst HA of life)
Subarachnoid Hemorrhage
- Neurologic Emergency with significant morbidity and mortality
- Presence of blood within the subarachnoid space between the arachnoid membrane and the pia mater
- Blood coats the arachnoid villi and obstructs CSF outflow leading to hydrocephalus and elevated intracranial pressure
SAH epidemiology
Worldwide incidence of 2 to 16 per 100,000 people
More common in women, peak age range 50-60 years
Approximately 5% of the population harbors an intracranial aneurysm and 20-30% of the population will have multiple aneurysms
90% of aneurysms develop within the anterior circulation, with the ACOMM being the most common site for aneurysm formation
SAH - categorized into? causes? *know*
Categorized into traumatic and non-traumatic
➢Trauma is the most common cause of SAH
➢Aneurysm rupture is the most common cause of non-traumatic SAH
SAH Clinical Presentation
--Sudden onset severe headache, unlike prior headaches
--Often described as WHOL or “thunderclap” headache
--Nausea & vomiting
--Photophobia
--Neck stiffness & pain (blood irritating meninges)
--Loss of consciousness
--Seizures
SAH Diagnostic Imaging? what first then what follows?
#1 Non-Contrast CTH
➢Acute blood appears hyperdense w/in subarachnoid space
➢Hydrocephalus from intraventricular hemorrhage (IVH)
CTA Head and Neck
➢Vessel imaging to detect aneurysm
➢Negative CTA should not rule out the presence of an aneurysm if the clinical suspicion is high
Lumbar Puncture: High volume RBCs (thousands), RBC turn yellow (Xanthochromia) within 12 hours from recirculation of CSF
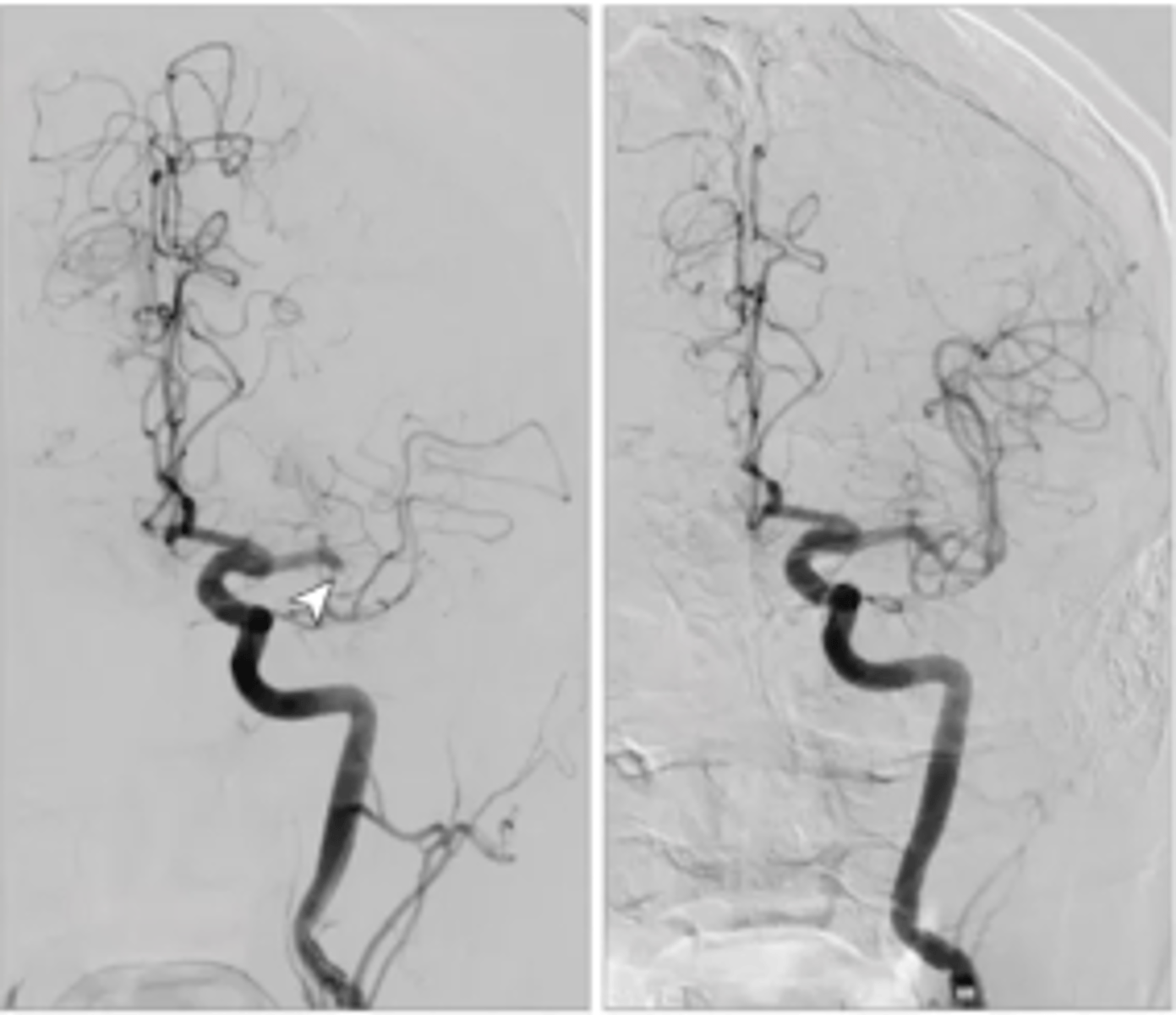
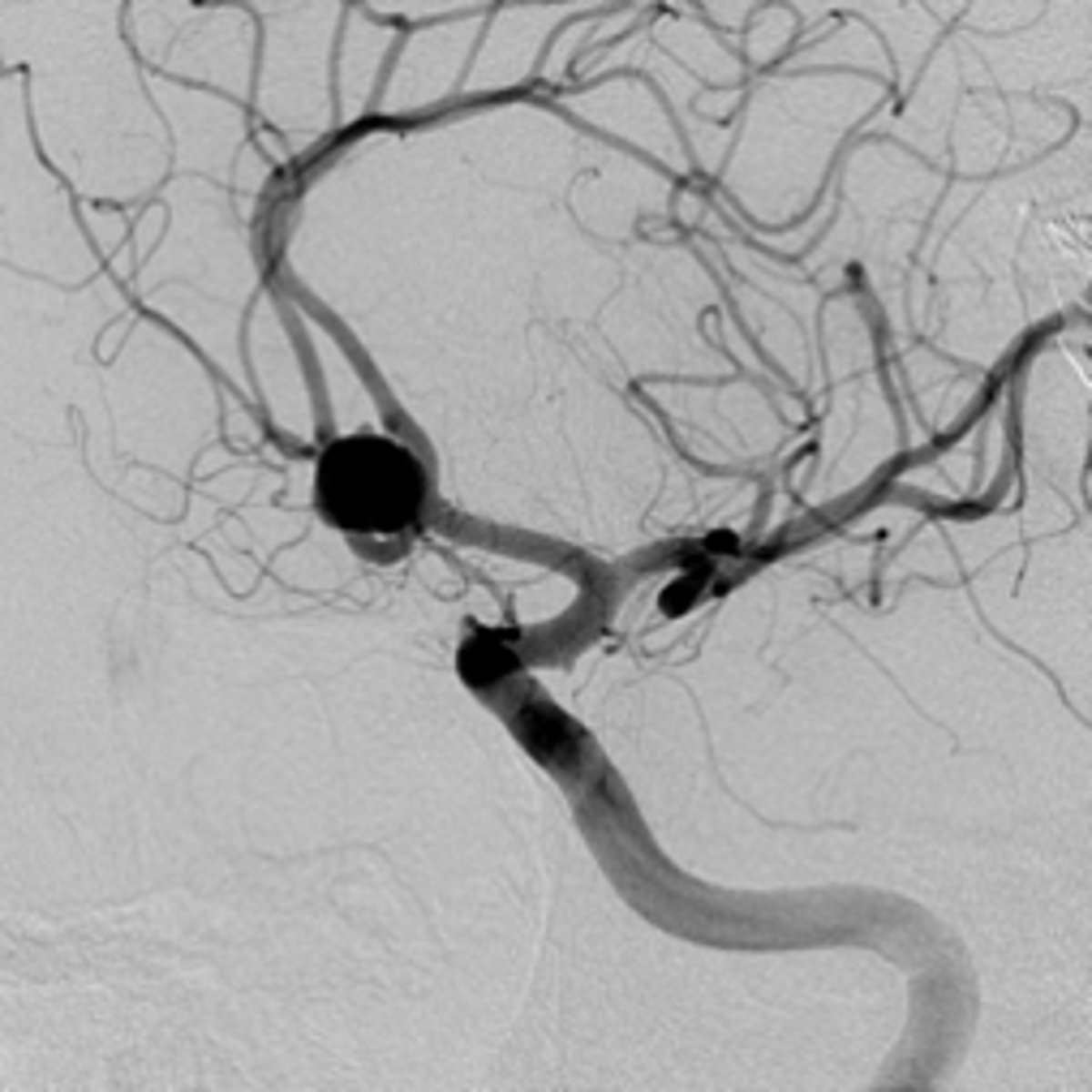
Digital Subtraction Angiography (DSA)
Digital Subtraction Angiography (DSA)
Gold standard for detection of aneurysm and surgical planning (urgent to ID aneurysm --> surgery)... visualize --> surgery
Image:
- ICA --> MCA and ACA
- black dot = aneurysm in ACOM area
Aneurysmal SAH Treatment
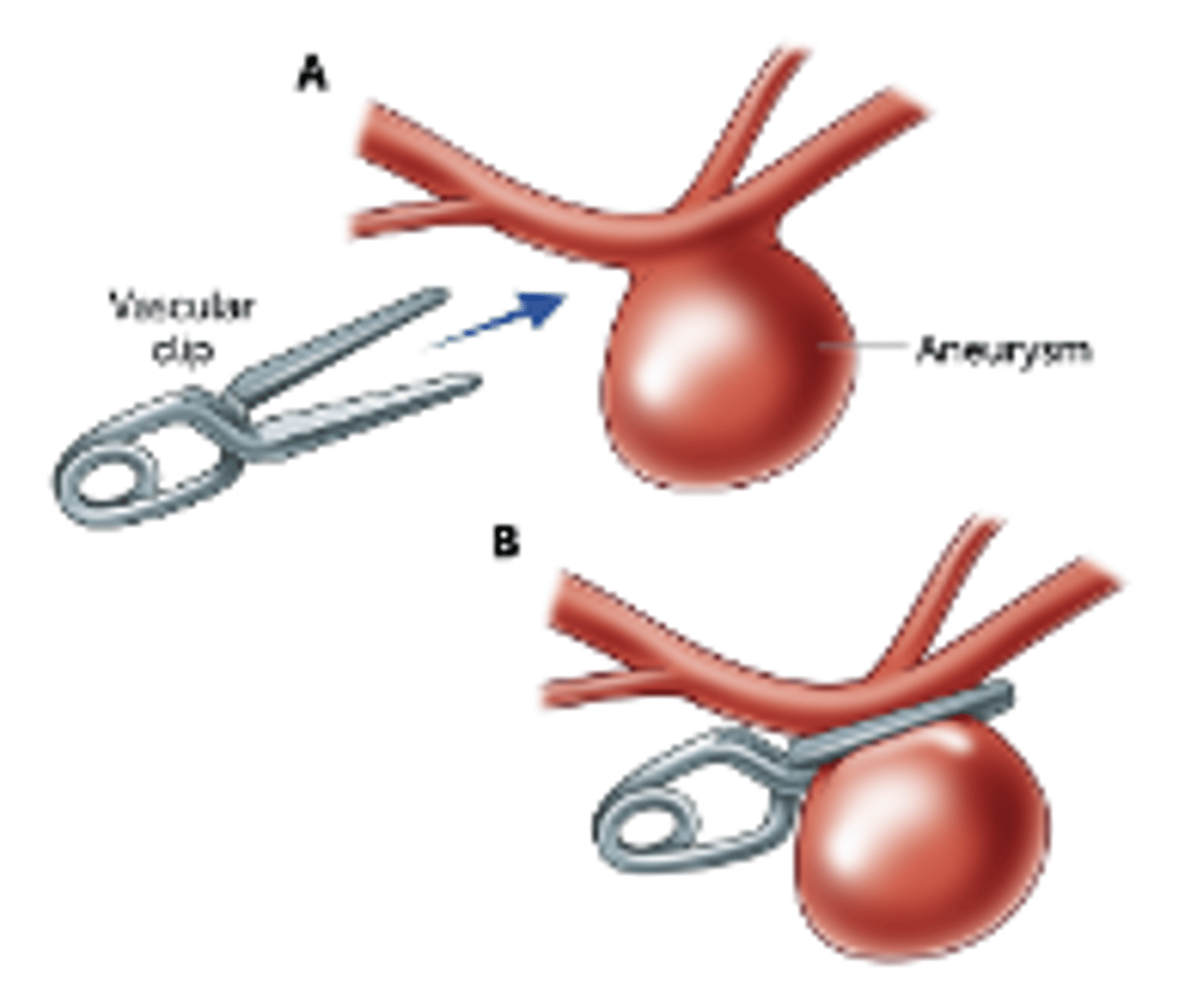
Surgical Clipping
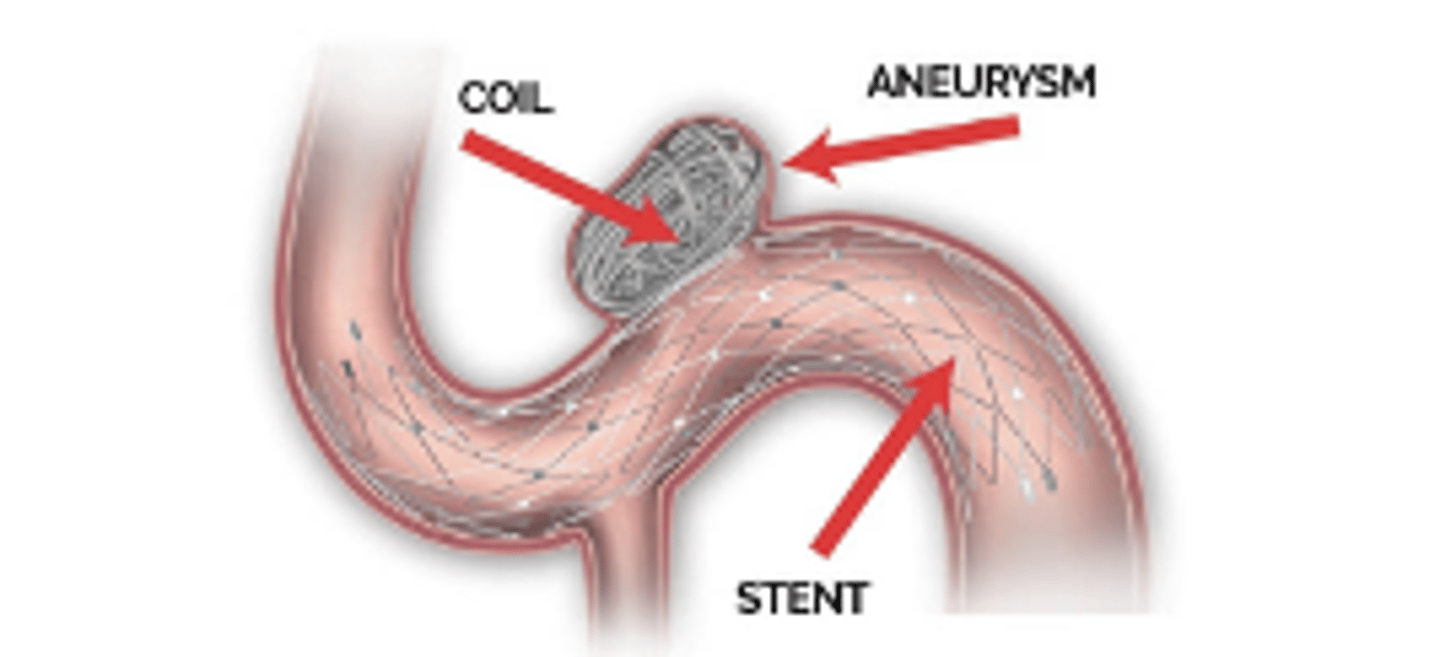
Endovascular Coiling
Aneurysmal SAH Treatment - Surgical Clipping
Surgical Clipping
➢Physically place a clip on the aneurysm neck
➢Invasive requiring craniotomy
➢Best for wide neck aneurysms
Aneurysmal SAH Treatment - Endovascular Coiling
Endovascular Coiling
➢Diverts blood flow to decrease stress on vessel wall
➢Less invasive
➢Wide neck aneurysms require stent and DAPT
Patient is a 78-year-old female with a PMH of smoking and HTN, who presents with acute onset headache, vomiting, and AMS.
Upon arrival to the ED, patient opens eyes to pain, pupils equal and reactive, does not follow any commands, not moving left side of body.
You are paged to the bedside to evaluate this patient in the ED. What is the first thing you do?
get a CT ! worried abt a focal neurological deficit
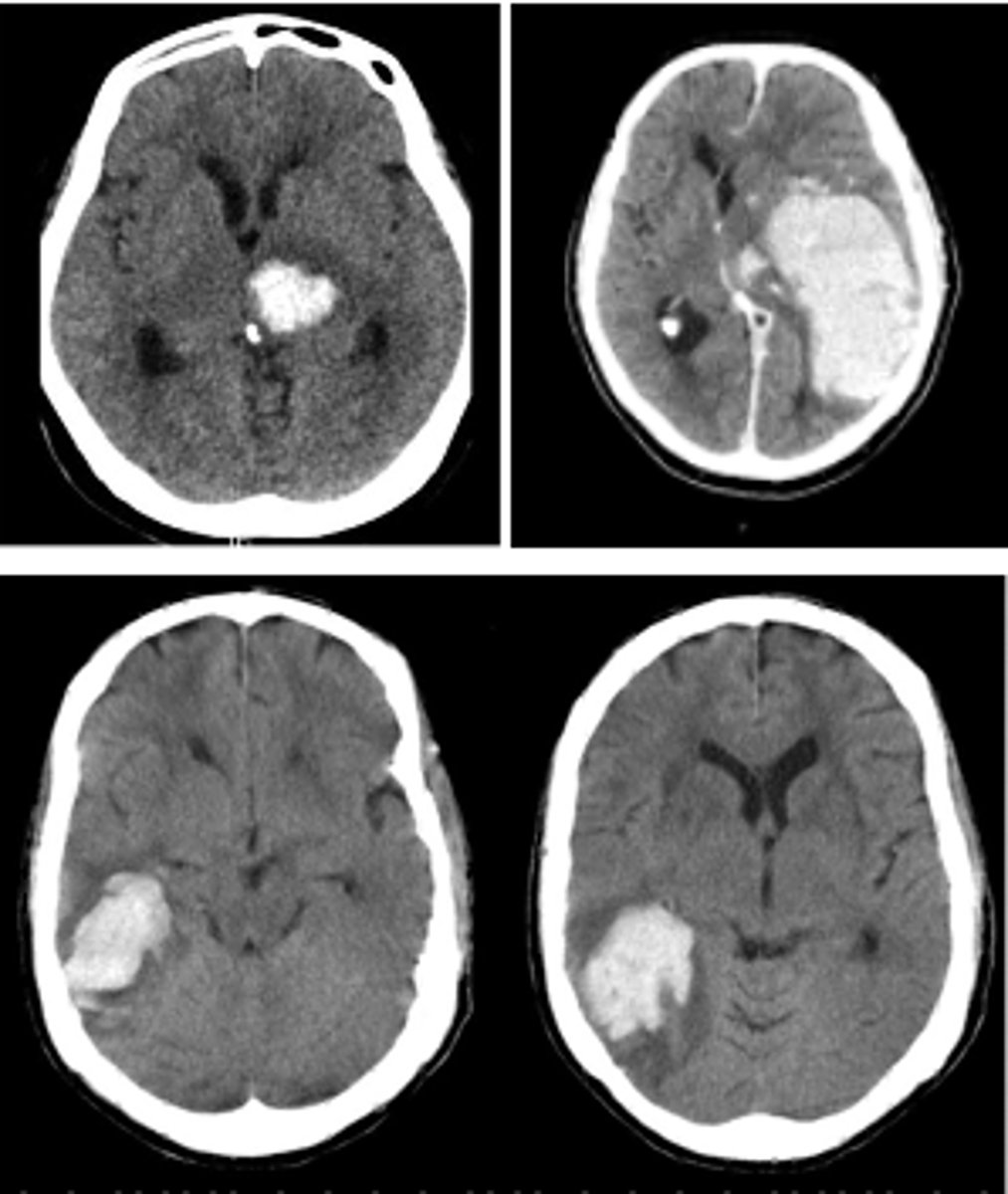
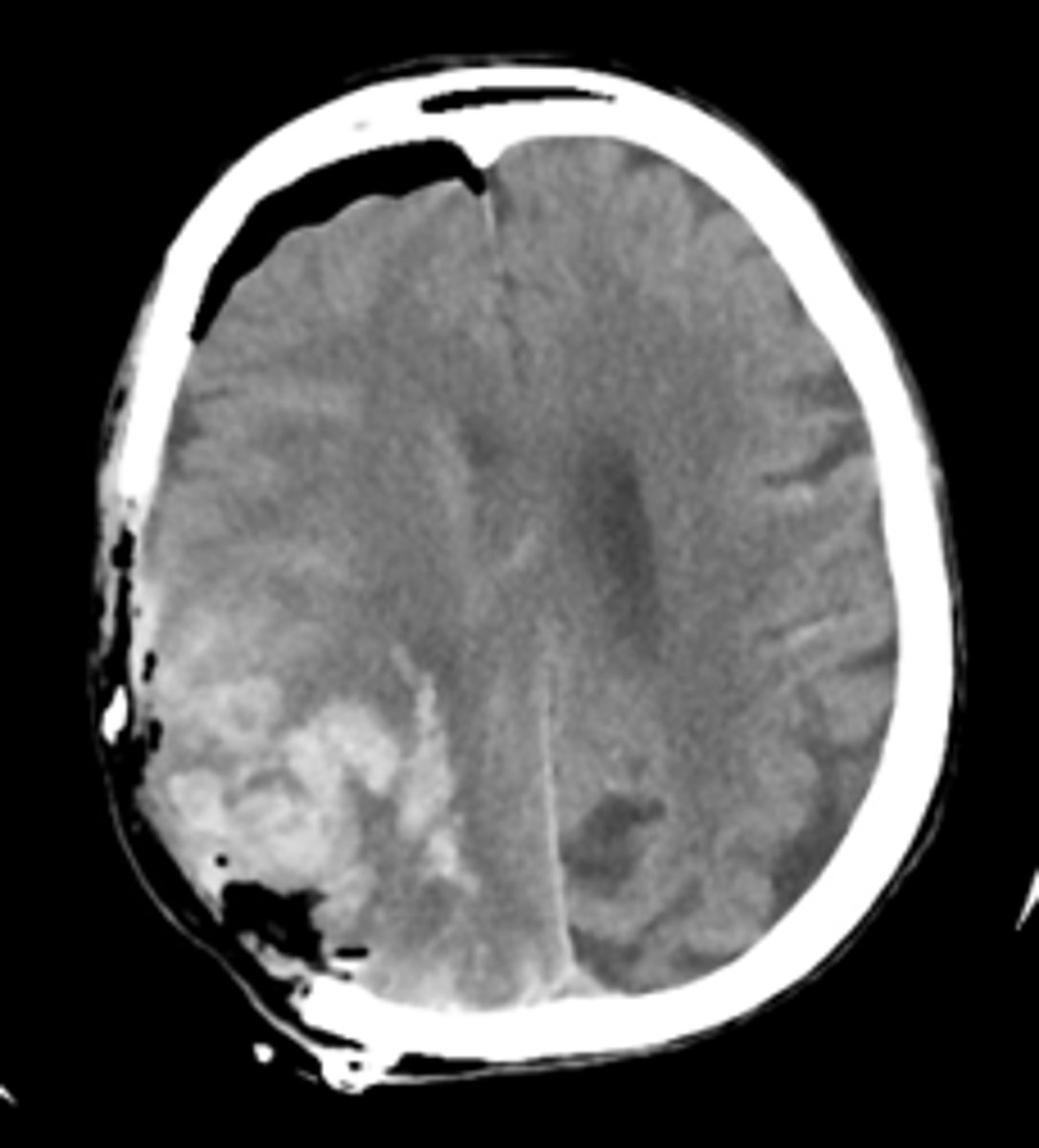
Intraparenchymal Hemorrhage (IPH)... Spontaneous bleeding into the brain parenchyma
Intraparenchymal Hemorrhage (IPH)
- Spontaneous bleeding into the brain parenchyma.
- Acute neurologic emergency that requires prompt treatment to prevent secondary brain injury.
IPH epidemiology
- Accounts for 10-15% of all strokes, but carries the highest mortality rate.
- Rate expected to double in the next 50 years from aging population and use of anticoagulation.
IPH Etiology
SMASHU
Stroke - obeys vascular territory
Medication - anticoagulation or tacrolimus
Amyloid - older patients, lobar ICH
Systemic - malignancy, vasculitis, APLS
Hypertension - subcortical ICH (deeper vessels more susceptible)
Unknown
IPH Management/Treatment: Golden Hour
HOB @ 30 degrees
Reversal of antiplatelet or anticoagulation
- ASA or Plavix: DDAVP & platelets
- Warfarin: Vitamin K
- DOAC: PCC
Strict blood pressure control
- SBP<140 if aneurysm suspected or large ICH
- SBP<160 otherwise
Hypertonics for cerebral edema (dehydrate brain, less edema)
- Mannitol (sugary solution)
- 23.4% saline (salty solution)
Stability scan
- 6 hours
- 24 hours - start DVT ppx
Neurosurgery consult
EVD placement for IVH & hydrocephalus OR for hemicraniectomy
Decompressive hemicraniectomy (DHC)
health disparities of stroke
➢Stroke disparities are widespread across the world
➢Epidemiological studies in the United States show that stroke risk and mortality is higher amongst ethnic minorities compared to white populations
➢Morbidity associated with stroke places an enormous emotional and financial burden on families & caretakers
➢Annual stroke recurrence rates have declined since the 1960s (6.1% to 5%), and are expected to be as low as 2.3% in the next 10 years from secondary stroke prevention
what can we do to help the health disparities of strokes?
- Understand chronic disease as a major cause of disability and death
- Encourage behavior changes, implement antihypertensive therapy, and control lipids
- Recruit minority populations into stroke trials
- Emergency Neurological Life Support Certification !!!