PPAS Exam 2
1/148
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
149 Terms
NEUROLOGIC EXAMINATION → 13
mental status
cranial nerves
motor fx
cerebellar fx
sensory fx
reflexes
gait
headache
cognition
delirium
depression
anxiety
tardive dyskinesia
CRANIAL NERVES
I olfactory → smell
II optic → visual acuity, visual fields
III oculomotor, IV trochlear, VI abducent → eye muscles, pupil size, response to light
V trigeminal → face/jaw
VII facial → raise eyebrows, clench eyes, smile/frown, puff out cheeks
VIII acoustic/vestibulocochlear → inner ear (whisper, scratch, tuning fork)
IX glossopharyngeal, X vagus → gag reflex, swallowing
XI accessory → shrug shoulders, turn head to side
XII hypoglossal → stick out tongue
Cranial nerve symptoms & diagnoses → STROKE (4)
vision
facial asymmetry
slurred speech
difficulty swallowing
Cranial nerve symptoms & diagnoses → BELL’S PALSY (2)
facial paralysis
lower eyelid drooping
Cranial nerve symptoms & diagnoses → MYASTHENIA GRAVIS (2)
eyelid drooping
double vision
MOTOR FUNCTION: ASSESSING COORDINATION & BALANCE
FINE MOVEMENTS → 4
rapid finger tapping
finger to nose
alternate pat with hand & palm
observe at rest
MOTOR FUNCTION: ASSESSING COORDINATION & BALANCE
BALANCE
_____________, semi-tandem, tandem
Romberg test →
standing feet together
stand still & close eyes 20s
MOTOR FUNCTION: ASSESSING COORDINATION & BALANCE
GAIT → 4
standing
walking
turning
TUG (timed up and go test)
1. Stand with your eyes closed | A. Cranial Nerve II Optic |
2. Stick out your tongue | B. Cranial Nerve VII Facial |
3. Tap your thumb and finger together fast | C. Cranial Nerve VIII Vestibulocochlear |
4. Tell me the number I whispered | D. Cranial Nerve XI Accessory |
5. Smile | E. Cranial Nerve XII Hypoglossal |
6. Walk fast like you are catching a bus | F. Balance |
7. How many fingers am I holding up? | G. Fine motor movements |
8. Shrug your shoulders | H. Gait |
Match the technique/request to the nerve/function
F
E
G
C
B
H
A
D
MOTOR: REFLEXES classification
-
-
-
Altered with disease states → 5
2+ normal
0 absent
4+ hyperreflexia, may also have clonus
stroke, PN, ALS, MS, Thyroid disease
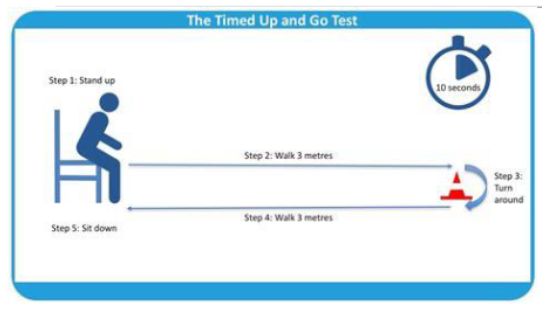
Timed Up and Go Test (TUG)
normal health elderly complete in _______
Score _____ = HIGH RISK FOR FALLS
</= 10s
>14
Stroke or TIA s/s
Balance
Eyes
Face (one side droop/numb)
Arms (one arm weak/numb)
Speech (slurred, unable)
Time (CALL 911! check clock to know what time sx first appeared)
HEADACHE reasons for emergent referral →
S → systemic s/s
N → neurologic
O → onset (thunderclap)
O → older (new onset >50 yo)
P → progression of existing headache disorder
Mental/Cognitive Status Screening Tools: MINI-COG
Orientation and registration: time, place, person, ___________, or items
Recall:
Perform task:
recognize words
3-5 words given, then after 5 min ask what they were
clock draw
MINI MENTAL STATE EXAM (MMSE)
Max score is 30
Mild AD →
Moderate AD →
Severe AD →
21-24
10-20
<10
DELIRIUM
MUST have … 2
then have either or … 2
acute/fluctuating, inattention
disorganized thinking, altered level of consciousness
HELPFUL QUESTIONS TO USE WITH CAM
Acute/fluctuating →
Attention →
Disorganized thinking →
Altered level of consciousness →
confusion → What day is it?
distraction, trouble keeping track → repeat the days of the week backwards
illogical, incoherent
drowsy, sleep, agitated, trying to escape
Which feature of the CAM did Mr. Williams exhibit when he was agitated and trying to “get out of here”?
A. Acute onset and fluctuating course
B. Inattention
C. Disorganized thinking
D. Altered level of consciousness
D
When Laura had delirium, she wanted to let the birds out of the wall with a hammer. Which feature of the CAM does this provide?
A. Acute onset and fluctuating course
B. Inattention
C. Disorganized thinking
D. Altered level of consciousness
C
COMPLEXITIES OF TRANSITIONS IN CARE
Multiple _________
Multiple (ever-changing) ____________
Multiple _________
Various _____
__________________
__________________
Lack of _____________
Inadequate ________ and __________
providers
therapeutic plans
comorbidities
EMRs
med discrepancies
poor communication
patient/family education
planning, goal setting
COMPLEXITIES OF TRANSITIONS IN CARE AFTER DISCHARGE
__________ for patients and their family about how and who should manage their care
Medication issues →
______________
misunderstanding
misunderstanding of instructions, adherence, DDIs, duplicate or omitted Rx
poor follow up w PCP
3 C’S OF MED RECS →
COLLECT best possible med hx
COMPARE what pt is actually taking w what is prescribed (identify discrepancies)
CORRECT any med discrepancies
PHARMACY RX REFILL INFORMATION
Advantages
Often _________ for medications
Provides information about _________
Disadvantages
Can be ______ to obtain
May be ________ (multiple pharmacies, OTCs)
only source
adherence
difficult
incomplete
OUTPATIENT EMR MEDICATION LIST
Advantages
May be easy to obtain and ______, especially if integrated EMR
Disadvantages
Cannot exchange their data ___________
Doesn’t work if patients are from practices that ___________
integrate
outside their own private network
dont use that EMR
HEALTH INFORMATION EXCHANGES
Advantages
May allow access to data from a _________ of healthcare systems
Data may be in a coded form that’s relatively _________
Disadvantages
_________ with a robust system in place
Most useful if ____________ the network
Only as accurate as the ________
variety
easy to use
few regions
everyone contributes
source it comes from
DISCHARGE MED LIST FROM RECENT HOSPITALIZATION
Advantages
If from same hospital, ________
May be easy to _________ into current chart
At one point in time, _________
Disadvantages
May be _________
Access limited to discharges from the ________
easiest to access
integrate
was accurate
out of data
same hosp
PATIENT/CAREGIVER’S VERBAL REPORT
Advantages
May be easy to obtain if patient ________ or family/caregiver available
Assesses patient/caregiver ________ of medications
Disadvantages
May be very _________ or _______
Not _______ in some cases (ex. delirium, family/caregiver not available)
communicative
knowledge
inaccurate, incomplete
available
MED LIST ON PAPER FROM PATIENT/CAREGIVER
Advantages
_____ to obtain
A bridge to a _________
Disadvantages
May be very ________ or ______
Often ___________
easy
long-term solution
inaccurate, incomplete
not available
TYPES OF MEDICATION DISCREPANCIES
Intended →
purposeful addition or omission of med(s)
TYPES OF MEDICATION DISCREPANCIES
Unintended →
omission
commission
diff dose/route/freq
therapeutic dup
Warfarin or aspirin held for a procedure
Example of …
intended
Metformin held at admission (use SSI while inpatient)
Example of …
intended
PPI continued at discharge for stress ulcer prophylaxis while pt was intubated
Example of …
unintended - commission
Patient requires 5 more days of prednisone for COPD exacerbation, not added to discharge med reconc
unintended - omission
Patient takes enalapril at home for BP but is substituted lisinopril upon admission per hospital formulary. His discharge instructions list both lisinopril & enalapril.
Example of …
unintended - duplication
Catapres TTS 0.1mg patch (patient was NPO during admission) continued at discharge instead of clonidine 0.1 mg tablet.
Example of …
unintended - diff dose/route/freq
PAIN CLASSIFICATION
Acute
Subacute
Chronic
<1m, identifiable cause, tx aimed at underlying cause
1-3m
>3m, not always identifiable, tx aimed to improve fx
NOCICEPTIVE PAIN
NEUROPATHIC PAIN
somatic → to body tissues, sharp/localized, visceral → arising from organs, dull/aching
PNS, CNS
PAIN ASSESSMENT
Past … hx
→
→
Query _________
___________ risk screening
___________ screening
___________ risk screening
________
med, social, family, psychiatric
ROS, basic 7 questions, QISS TAPED
phys exam
PDMP
substance abuse risk
mental health
rsp disease
pain
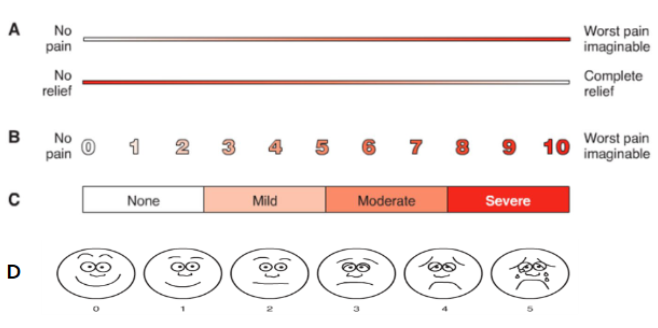
PAIN INTENSITY SCALES
A
B
C
D
visual analog scale
numeric rating scale
verbal scale
faces rating scale
_____________: brief, self-reported screening tool designed to help providers assess patients’ risk of opioid abuse before starting opioid therapy
opioid risk tool ORT
_______________: 17-item self report assessment of aberrant behavior for current opioid therapy
COMM assessment
PHARMACOTHERAPY BASED ON TYPE OF PAIN
1st line therapy → considerations for opioid use
Nociceptive
Neuropathic
Central sensitization
NSAIDs → only when other inadequate
TCA/SNRIs, antiseizure → ^
TCA/SNRIs, antiseizure → AVOID; often worsen
POPULATIONS AT GREATEST RISK FOR HARM FOR OPIOIDS → 6
sleep apnea/other
renal/hepatic insuff
older adults
preg women
depression/other
personal/family hx of AUD/SUD
When starting opioid therapy for acute or chronic pain, clinicians should prescribe _______ opioids
*TRY TO AVOID COMBINATION OF ER/IR PRODUCTS
IR
__________ should NOT be the 1st choice for an ER/LA opioid
methadone
Opioid Dosage
Lowest starting dose for opioid naive _____ MME for single dose
^ or _____ MME/day
Be cautious when increasing dosage to _____ MME/day
AVOID increasing to _____ MME/day
5-10
20-30
>/= 50
>/= 90
OPIOID TAPERING
______ of original dose _______
For long term opioid uses (>1 year) →
10% / week
10% / month
OPIOID FOLLOW UP
Within _________ of starting opioid therapy
CHRONIC =
1-4w
q 3m
PHARMACIST ROLES IN OPIOID SAFETY MONITORING
Screening for _________
Review of _______ data
Use of _________ or _______
Avoid __________
Proper utilization of _______
Arrangement of _______ for opioid use disorder
risk factors
PDMP
urine drug testing, random pill counts
co prescribing BZDs
naloxone
tx
NALOXONE WHEN FACTORS +RISK FOR OPIOID OVERDOSE
hx of _________
hx of _________
Higher opioid dosages (_____ MME/day)
Concurrent ________ use
overdose
SUD
>/= 50
BZD
OPIOID USE DISORDER TREATMENT
Opioid agonist →
Partial agonist →
PO or LA injectable →
methadone
buprenorphine
naltrexone
S/S OF INTOXICATION OR OVERDOSE → 6
miosis
-consciousness/drowsiness
-resp
bradycardia
euphoria
slurred speech
S/S OF WITHDRAWAL → 6
mydriasis
sweating
fever
NV, cramping
HTN, tachycardia
agitation
OPIOID CONVERSION FACTORS FOR MORPHINE MG EQUIVALENTS → 6
hydrocodone = 1
hydromorphone = 5
oxycodone = 1.5
fentanyl transdermal (mcg/hr) = 2.4
oxymorphone = 3
tramadol = 0.2
Calculate MME and TDD
Hydrocodone 5/325mg q6H
TDD = 20 mg hydrocodone
MME = 20
OPIOID TOLERANCE
incomplete cross-tolerance between opioids
reduce NEW opioid dose by ______ to accommodate
25-50%
OPIOID INDUCED HYPERALGESIA → treatment
-opioid dosage or opioid rotation
OA vs RA
both can cause morning stiffness
OA = larger joints
RA = small joints
All facilities that perform lab testing are regulated by
CLIA
What does CLIA stand for?
A. complete laboratory insurance amendments
B. cruise line international association
C. complete laboratory improvement act
D. clinical laboratory improvement amendments
D
What is a “waived test”?
A. Simple lab exam/procedure with high risk of error
B. Simple lab exam/procedure with low risk of error
C. Complex lab exam/procedure with high risk of error
D. Complex lab exam/procedure with low risk of error
B
Which form must be completed to apply for a CLIA waiver?
CMS - 116
In which setting can POCT be performed?
A. community
B. emergency department
C. home
D. all of the above
D
How much is the Biennial Certificate of Waiver Fee?
$248
Yes or No
Can pharmacists charge for CLIA waived services?
yes
To perform POCT in ANY state, you must
A. have a CLIA certificate of waiver
B. follow manufacturer’s instructions for the test
C. both of these
D. only one of these
C
Which organization approves devices as “CLIA-waived”
A. CMS
B. CDC
C. DHHS
D. FDA
D
T or F:
POCT are classified by their complexity as simple, moderate, or high
T
T or F:
You must obtain additional training to provide POC testing
F
SCOPE OF PRACTICE
3 regulatory entities →
state pharmacy practice acts
federal pharmacy law
PREP Act (public readiness and emergency preparedness act)
What can we do in Arkansas?
2017 → “Statewide Protocol” + Naloxone
2019 → Nicotine Replacement Therapy NRT
2021 → Oral Contraceptive Therapy
2022 → Flu/Strep/COVID Test & Treat
2023 → HIV PrEP/PEP Therapy
Act 284
Act 651
Act 408
Act 503
Act 314
ACT 408 (ORAL CONTRACEPTIVE THERAPY)
Can ONLY prescribe ______ birth control
REQUIRED completion of ___________ approved by AR BoP
Patient assessment algorithm →
PO
training program
preg, BP, OC eligibility screening
ACT 314 (HIV PrEP / PEP Therapy)
PrEP (PRE EXPOSURE) options → 2
Descovy (emtricitabine/TAF)
Truvada (emtricitabine/TDF)
ACT 314 (HIV PrEP / PEP Therapy)
PEP (POST EXPOSURE) options → 4
Emtriva (emtricitabine)
Isentress (raltegravir)
Tivicay (dolutegravir)
Truvada (emtricitabine/TDF)
Viread (TDF)
Which require completion of training program approved by AR BoP? (select all that apply)
A. “Statewide Protocol” + Naloxone
B. NRT
C. Oral contraceptive therapy
D. Flu/Strep/Covid test and treat
E. HIV PrEP/PEP therapy
C, E
ACT 314 (HIV PrEP / PEP Therapy)
PrEP (PRE EXPOSURE)
Inclusion criteria → 3
EXCLUSION criteria → 4
18+, +risk, -HIV Ag/Ab test result w/in past 7d or -POC HIV test
interested in Apretude (cabotegravir IM), s/s acute HIV infxn, CrCL <30, +HIV test
ACT 314 (HIV PrEP / PEP Therapy)
PrEP (PRE EXPOSURE) TX ALGORITHM
Descovy vs Truvada preference
Descovy → regular NSAID use, -BMD, NOT approved for female @birth
Truvada → preg/breastfeeding, cis-female or trans-male
ACT 314 (HIV PrEP / PEP Therapy)
PEP (POST EXPOSURE)
Inclusion criteria → 3
EXCLUSION criteria → 4
13+, exposure to +HIV source, exposure to unknown HIV status
<13 yo, exposure >72h, +HIV test, -renal fx
ACT 314 (HIV PrEP / PEP Therapy)
PEP (POST EXPOSURE)
Adult dosing →
PREGNANT patients →
Pediatric dosing →
Truvada + Tivicay/Isentress
Truvada + Isentress
>/= 40kg Truvada + Isentress; <40 kg Viread + Emtriva + Isentress
POCT & Treat: Influenza
Documentation must be maintained for _____
2 yr
INFLUENZA & STREP A CRITICAL THRESHOLDS
Critically unstable & refer
BP
RR
O2
adult <90 SBP or <60 DBP; age 3-9 <70 + (age x 2) SBP
adult >25; <18 yo >20
<90%
INFLUENZA ELIGIBILITY CRITERIA TO USE PROTOCOL
Age _____
____________
Symptoms _______
No hx of ______ to influenza tx
Has NOT used antiviral therapy for influenza within _____
____________
3+
not preg
<48h
allergic rxn
30d
not immunocompromised
Which flu treatment contains milk proteins and is NOT recommended in pts w/ underlying respiratory disease?
zanamivir (Relenza)
TAMIFLU (OSELTAMIVIR)
USE IN CAUTION WITH …
Chronic _______ disease
Severe ______ impairment
________ impairment (dose adjust)
________ disease
cardiac
hepatic
renal
resp
STREP A PHARYNGITIS ELIGIBILITY CRITERIA
Age _____
______________
Centor score _____
Has not used ABx for sore throat or URI within ______
_________ is positive
______________
3+
not preg
2+
30d
GAS POCT
not immunocompromised
STREP A PHARYNGITIS TREATMENT
1st line
2nd line (or PCN allergy)
3rd line (if PCN allergy or exclusions to 1st/2nd line)
amox, pen V
cephalexin
azithromycin
MEDICARE (REVIEW)
covers → payment to
Part A
Part B
Part C “Medicare Advantage”
Part D
hospital/hospice → hospital
outpt med → provider
outpt med, ± Rx → commercial payer
Rx → PDP
PHARMACISTS are not currently recognized as providers under Medicare _______, which limits ability to bill for clinical services
part B
____________ is the process of verifying a healthcare professional’s qualifications
___________ is the process of granting permission to perform specific services within an organization or payer network
These processes are essential for pharmacists to participate in medical billing and payer networks
credentialing
privileging
Who can we bill medical claims for our clinical services?
AR BCBS
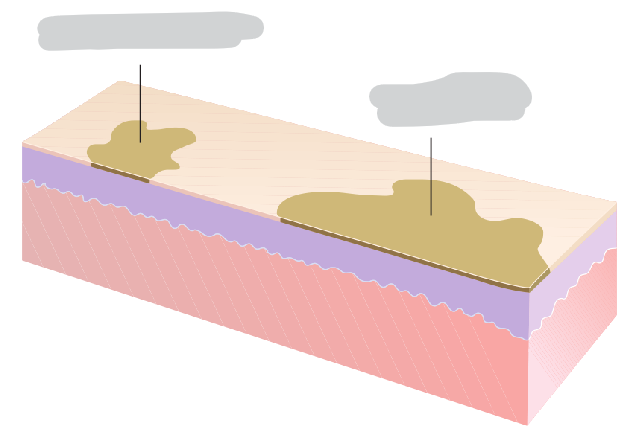
Macule vs Patch
patch (5cm+) > match

PAPULE
small, ______ lesion
raised
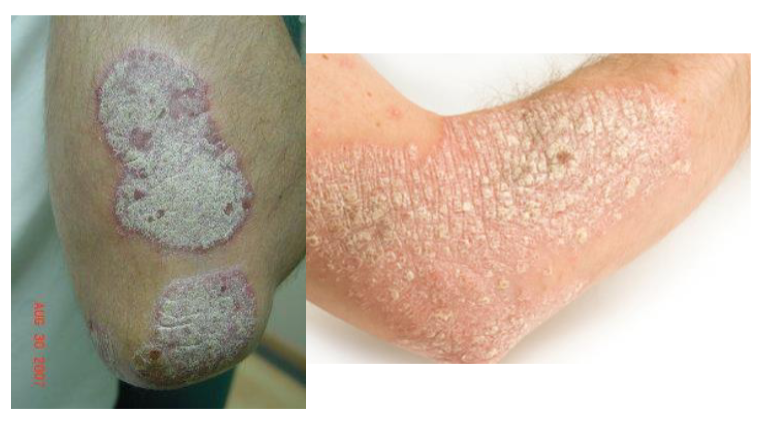
PLAQUE
raised, >_____ in diameter
1.5 cm

__________: thickening or roughening of the skin (leather bark like)
lichenification

Nodule
_____ cm in length AND depth
>1.5

skin lesion =
secondary to ______
usually ______
wheal
edema
erythematous

Skin lesion =
Nodule containing liquid
cyst

skin lesion =
filled with ______ serous fluid
vesicle
clear

skin lesion =
bulla