Unit 4: Sensory Systems
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
What is the integration of sensory systems?
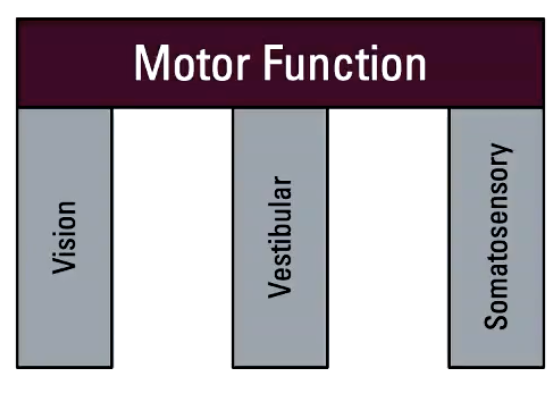
Movement is supported by 3 categories of sensory systems
Motor Function
Vision (see)
Vestibular (where body is in space)
Somatosensory (touch)
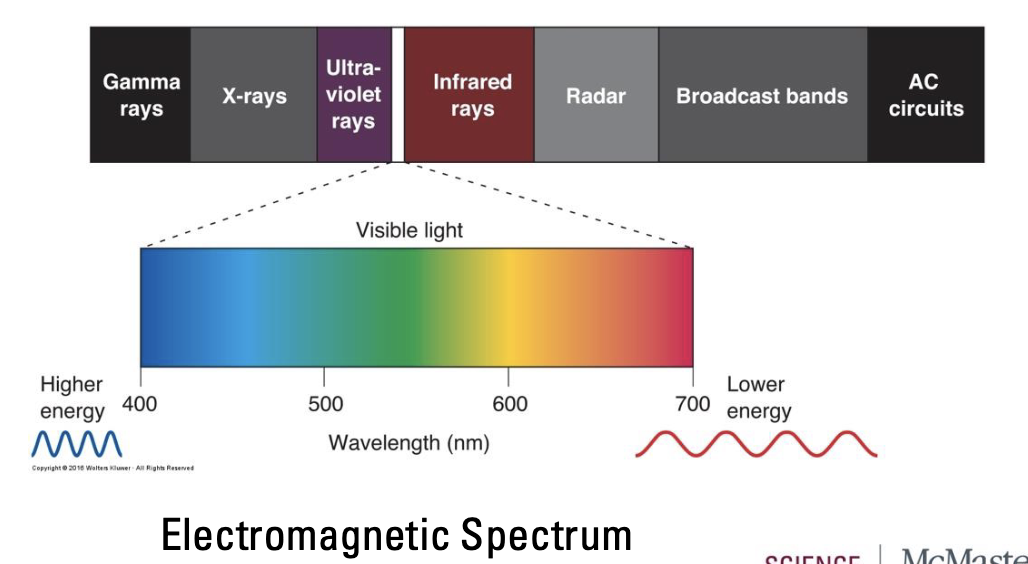
How do we see?
Neurons in the visual system create perception of world (images) based on electromagnetic radiation (light)
Eyes have evolved to only detect visible light (400-700nm)
Colour is not inherent in the world
Brain’s interpretation of wavelengths
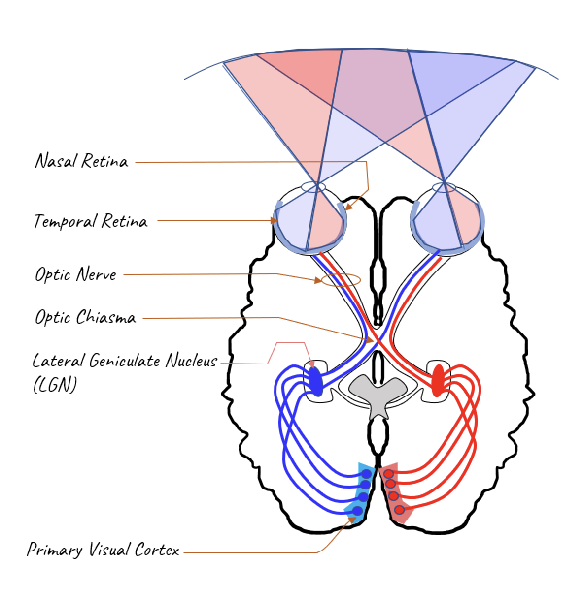
Visual Pathway
Retina → Thalamus → Primary visual cortex
What is retinofugal projection?
“Flees the retina”
Retina to Thalamus to Primary visual cortex
Retina – receives sensory information
Optic Nerve – before decussation
Optic Chiasm – decussation (partial)
Optic Tract – after decussation
Lateral Geniculate Nucleus (of the thalamus)
Primary Visual Cortex (V1 or Brodman’s 17)
**Remember: “N” before “T”
What is the primary visual cortex?
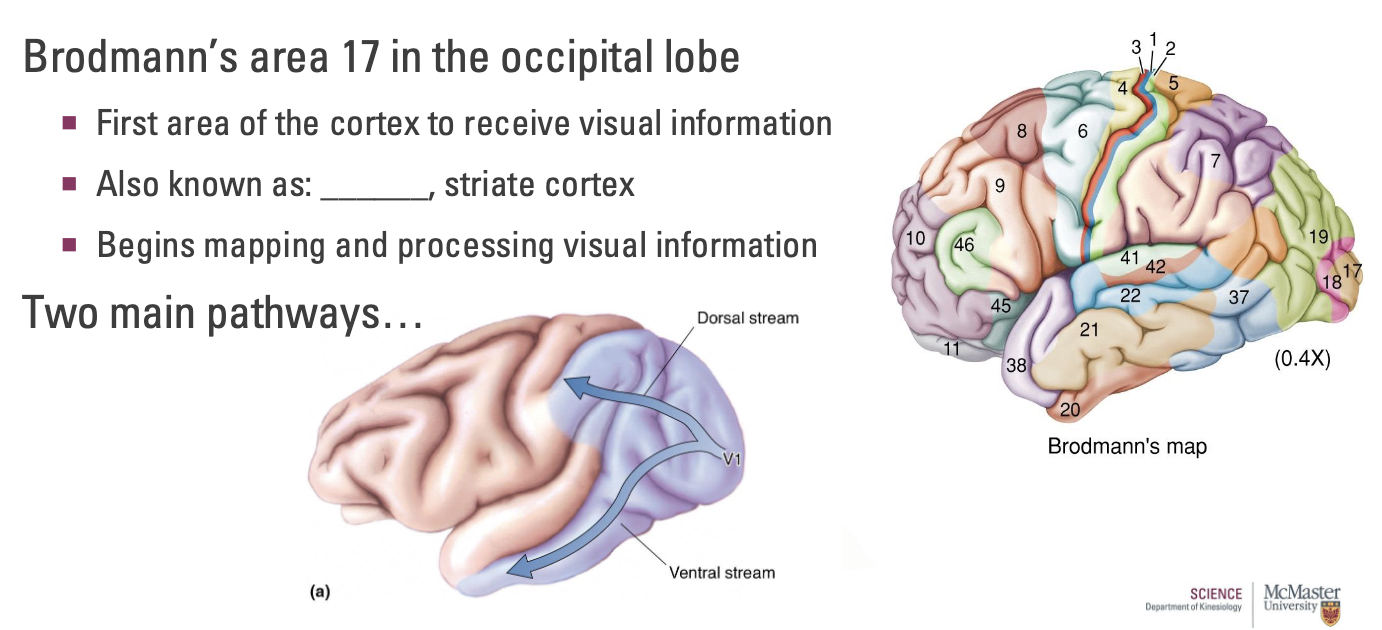
Brodmann’s area 17 in the occipital lobe
First area of the cortex to receive visual information
Also known as: V1, striate cortex
Begins mapping and processing visual information
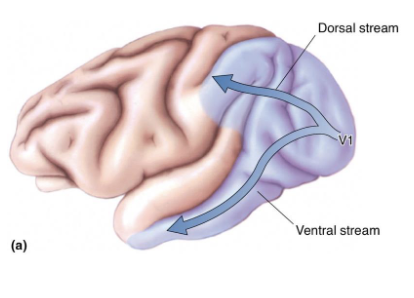
Two main pathways: Dorsal and ventral stream
What is the Dorsal Stream of V1?
Information passed toward the parietal lobe
Specialized processing of visual motions
Navigation – perceiving the direction and speed of objects helps us navigate safely
Directing eye movements – sense motion and quickly react to it
Motion perception – interpretation of moving objects
What happens if there is damage to Dorsal Stream of V1?
Case Study 1: Can see objects that aren’t moving, but once objects start moving, they become invisible.
Case Study 2: Told to pour coffee to fill a cup. Can see coffee on the bottom of the cup, but doesn’t register coffee filling up and coffee overflows.
What is the Ventral Stream in V1?
Information passed toward the temporal lobe
Specialized processing of vision other than motion
Object perception and facial recognition
Not only recognize features, but remembering faces (ex: babies recognizing parents faces)
What is the pathway for processing visual information?
Retina → Thalamus → Primary visual cortex
“maps” and processes visual information
Complex integration of parallel sensors and processing (colour, shape, motion, etc.)
What is the Vestibular System?
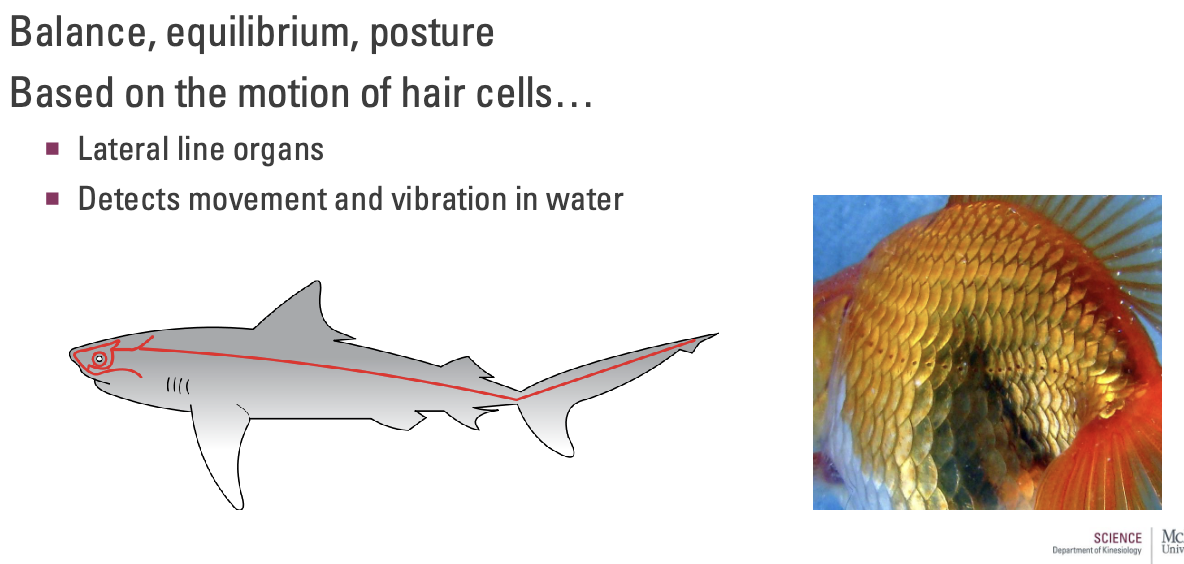
Balance, equilibrium, posture
Based on the motion of hair cells...
Lateral line organs (similar to fish)
Detects movement and vibration in water
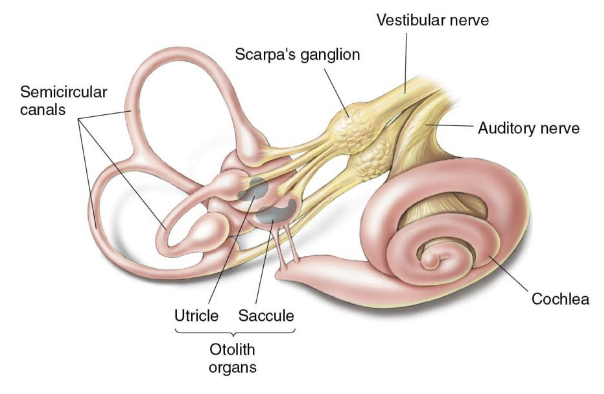
What is the Vestibular System in humans?
Humans = Vestibular labyrinth
Otolith organs – acceleration and tilt
Semicircular canals – head rotation
Both use hair cells to detect changes
~20,000 vestibular axons
Cell bodies in Scarpa’s ganglion
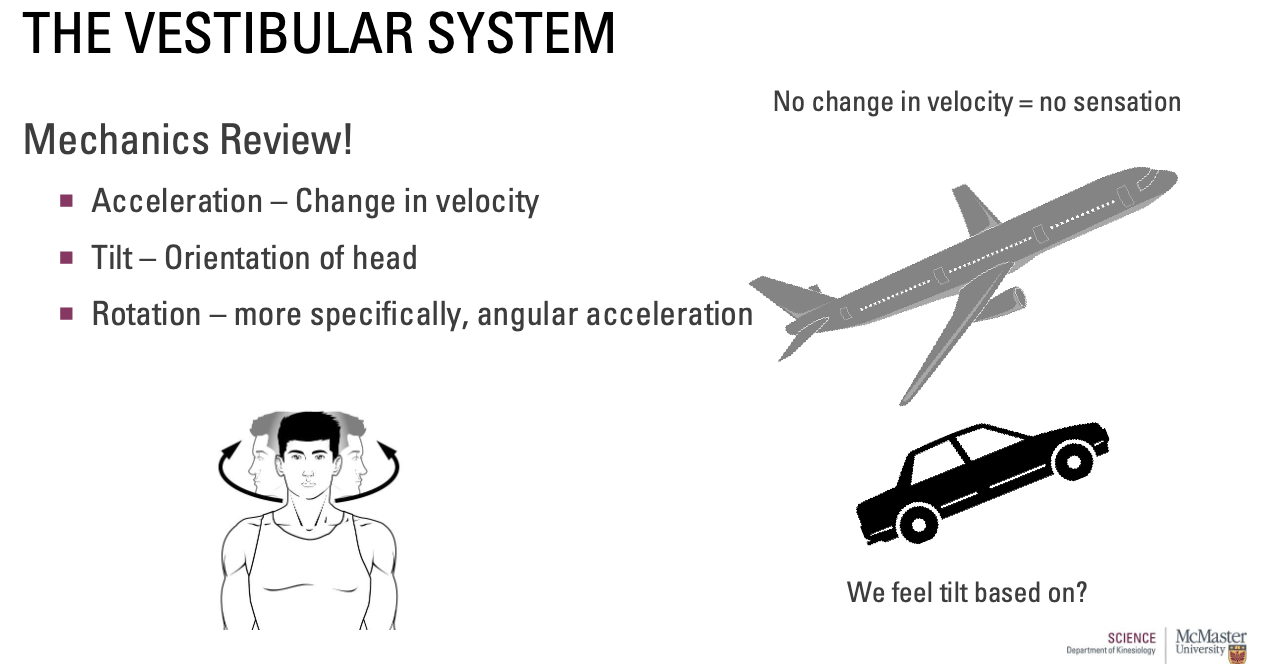
How does the Vestibular System relate to mechanics?
Acceleration – Change in velocity
Airplane at a consistent speed = no change in velocity = no sensation
Tilt – Orientation of head
Due to gravity
Rotation – more specifically, angular acceleration
Due to the semicircular canals
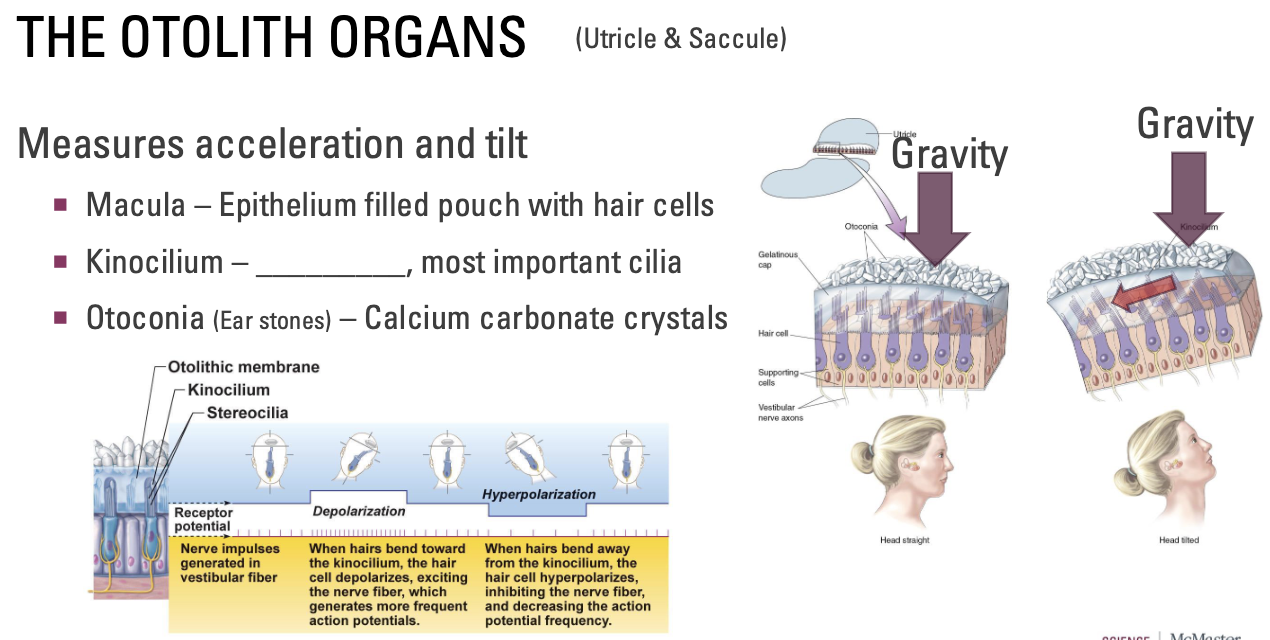
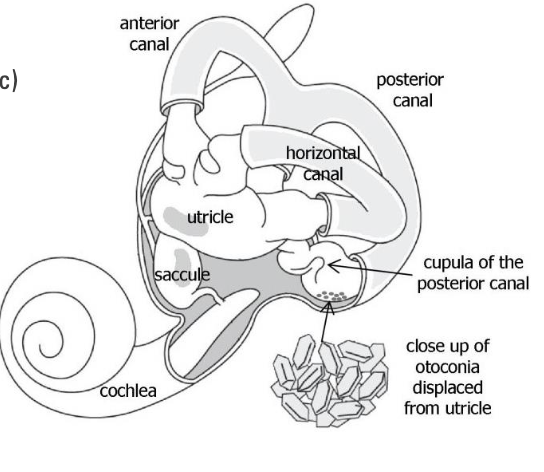
What are the Otolith Organs (Utricle and Saccule)?
Measures acceleration and tilt
Macula – Epithelium filled pouch with hair cells
Kinocilium – Tallest, most important cilia
When fluid fills the hairs, we feel the small hairs (stereocillia) in relation to the big hair
Otoconia (Ear stones) – Calcium carbonate crystals
Tilt: Gravity pushes on otoconia → pushes on liquid → pushes on little hairs relative to this big hair → hair cells receive information and send down vestibular axons
Baseline of action potentials; firing rate increase/decreases depending on the amount of tilt
Cilia bend toward big hair = depolarization
Cilia bend away from big hair = hyperpolarization
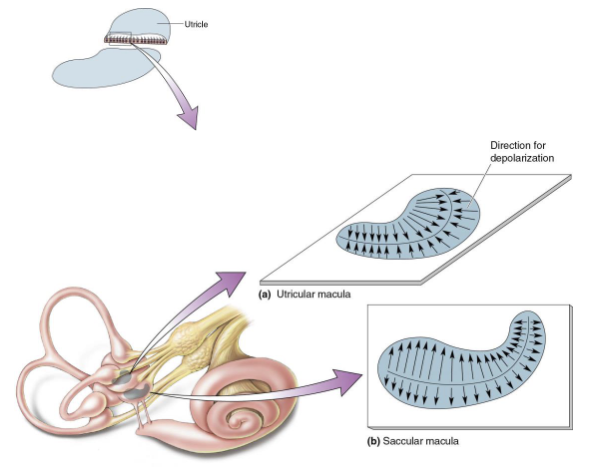
What is Macular Orientation?
Array of orientations within organ
Saccular macula – vertically oriented
Utricular macula – horizontally oriented
Allows measures of all possible linear movements
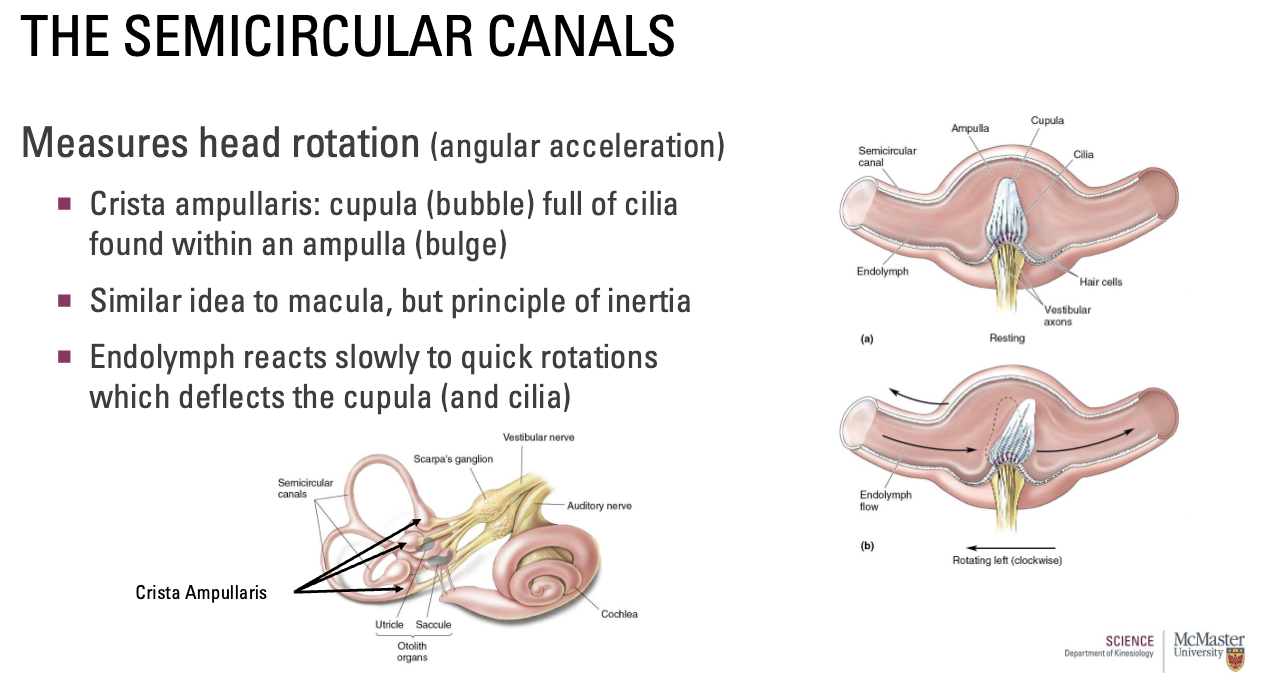
What are the Semicircular Canals?
Measures head rotation (angular acceleration)
Three semicircular canals on each side
Help sense all possible head rotation angles
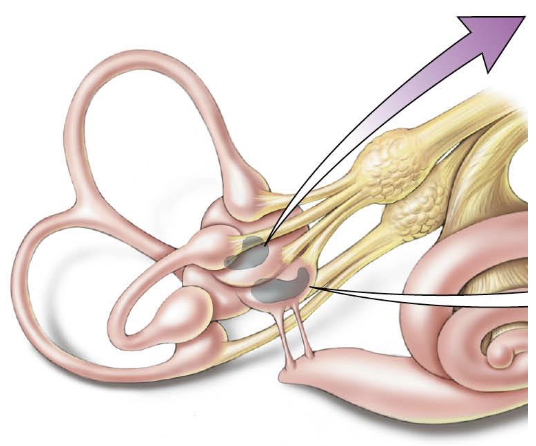
What are the Crista ampullaris?
Crista ampullaris: cupula (bubble) full of cilia found within an ampulla (bulge)
Similar idea to macula, but principle of inertia
Endolymph reacts slowly to quick rotations which deflects the cupula (and cilia)
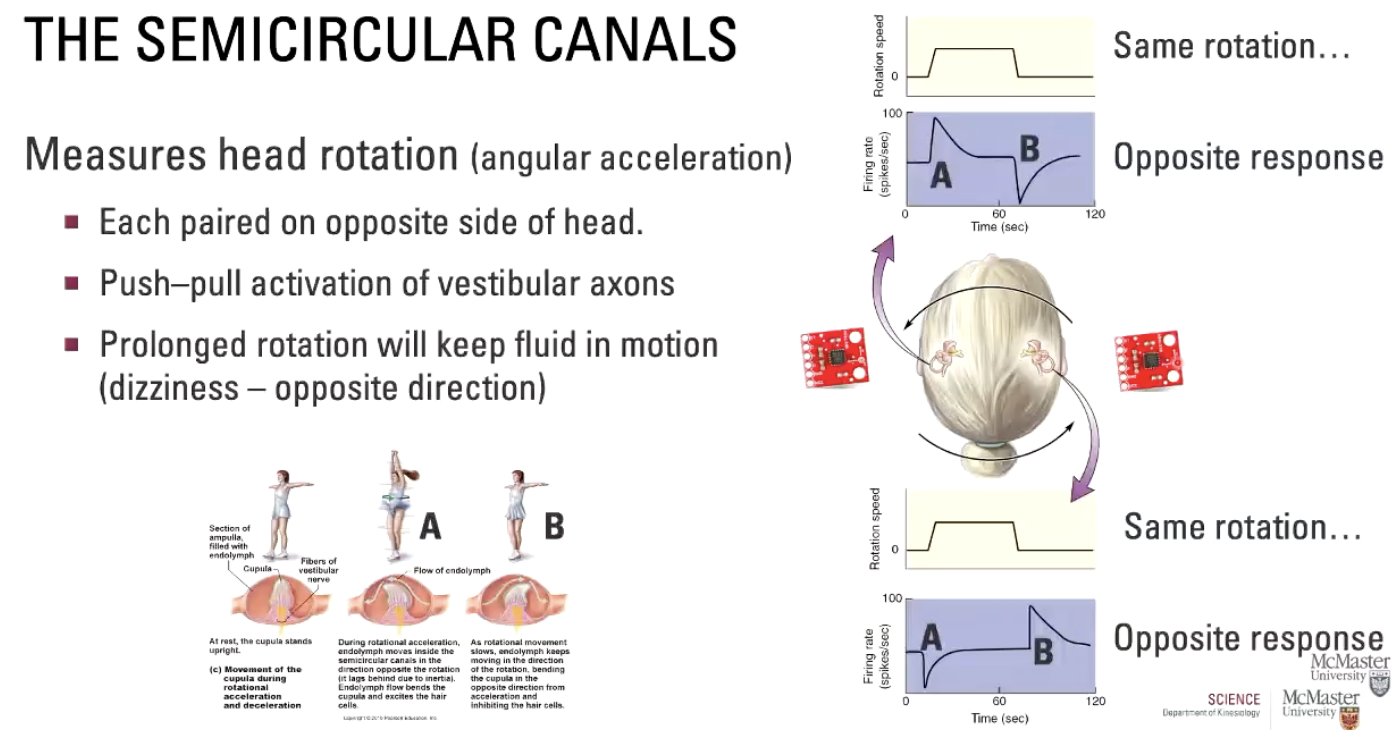
How are the Semicircular Canals organized?
Each paired on opposite side of head.
Push–pull activation of vestibular axons (same rotation but opposite response)
Prolonged rotation will keep fluid in motion (dizziness – opposite direction)
A → initiate movement, B → stop movement
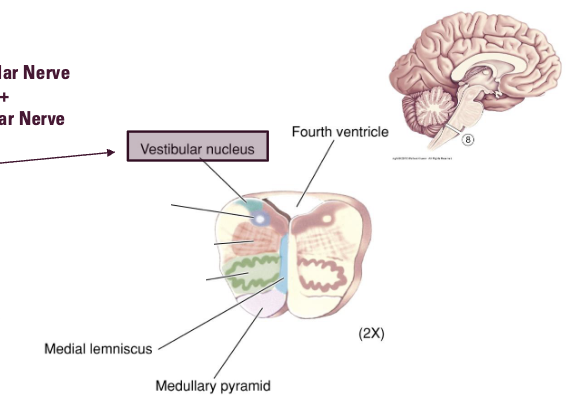
What are the Central Vestibular Pathways?
Pathways of vestibular information and reflexes to control head, body, eye movement
1) Otolith organs (Acceleration, tilt) + Semicircular canals (Rotation)
2) Vestibulocochlear nerve (VIII)
Bipolar neurons
Merges with auditory information
3) Vestibular nuclei
Dorsolateral regions of medulla
Integrate with other information (visual/motor)
4) Send out information above and below
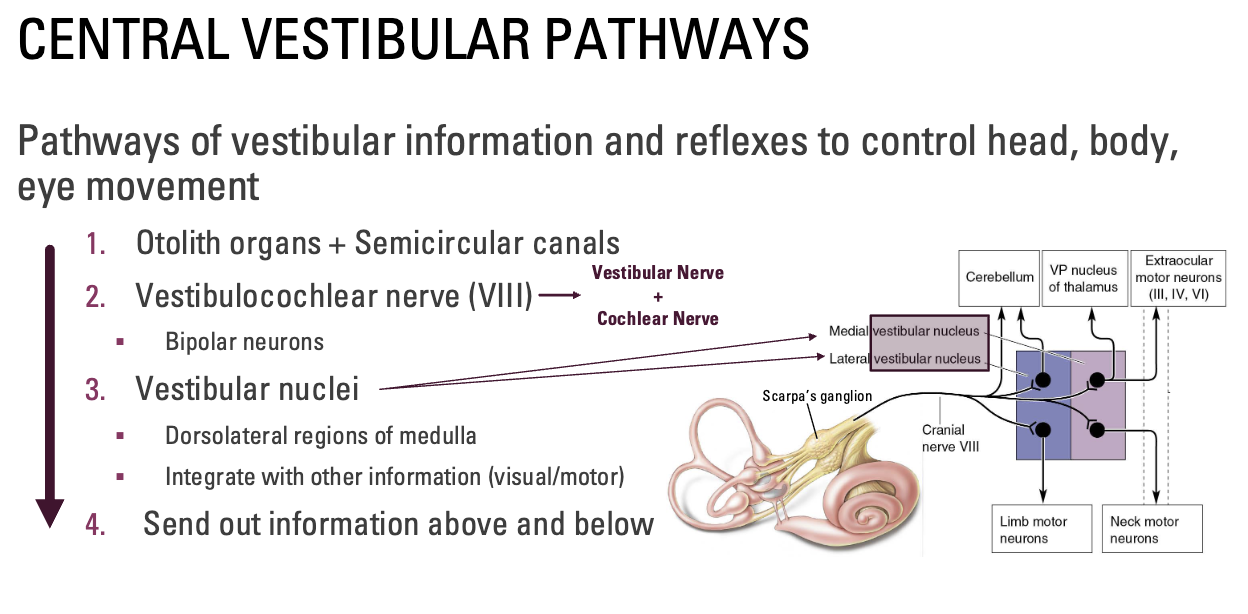
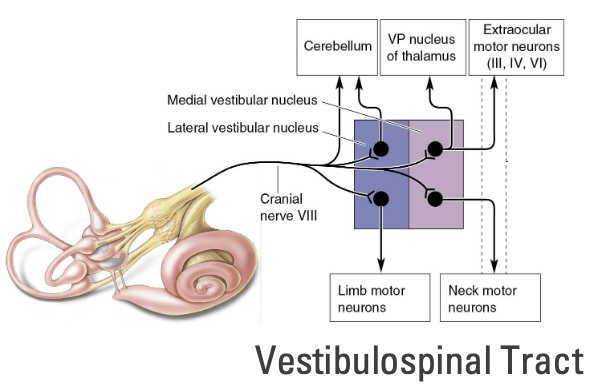
Where do the Central Vestibular Pathways send information out to?
1) Cerebellum
Vestibular sensations needed for coordinating movements
2) Thalamus (ventral posterior nucleus)
Then projects to Postcentral gyrus
Info received by the cortex maintains a representation of the body in space
3) Extraocular motor neurons
Reflexive eye movements
Primary goal: Maintain gaze
4) Limbs
Reflexive limbs movements
Primary goal: Keep body upright
5) Neck and trunk
Reflexive neck/trunk movements
Primary goal: Keep head upright
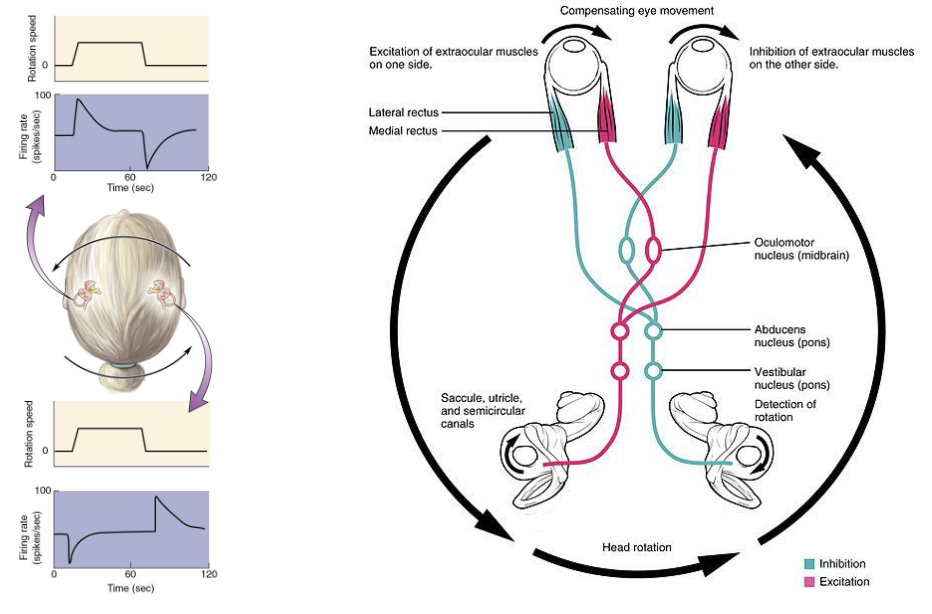
What is the Vestibulo-ocular Reflex (VOR)?
Function: To fixate line of sight on visual target during head movement
Mechanism: Senses rotations of head, commands compensatory movement of eyes in opposite direction
Ex: Seen in chickens due to their weak eyesight, this reflex helps them maintain gaze.
How do Vestibular Connections mediate horizontal eye movements?
Example: Rotating head left but maintaining eyes on a fixed point
Excite the red side (contract) and inhibit the blue side (relax)
(Vestibular nucleus - medulla/pons)
What are the peripheral vestibular changes with age?
Peripheral changes – likely occur first
Otolith organs
Loss of cilia
Alterations in otoconia (size and shape)
Semicircular Canals
Loss of cilia, to a greater extent than otolith organs
Greater impact in VOR and fall risk
What are the central vestibular changes with age?
Central changes – likely occur later (after 60 years of age)
Vestibular nuclei – slow loss of neurons
Cerebellum – slow loss or change in connectivity
Together, this leads to a reduction in sensory information necessary to control head, eyes, and body and maintain balance
Add this to a multitude of changes to other sensory structures (vision, touch, proprioception) and loss of muscle strength = Increased fall risk
What is BPPV (most common)?
Benign Paroxysmal Positional Vertigo
Benign = harmless in the long-term
Paroxysmal = Sudden onset/recurrence of symptoms (<60sec)
Vertigo = Sensation of spinning/dizziness
Vertigo itself is a symptom (not an illness)
Caused by:
Ear stones (otoconia) migrating into semi-circular canals
Disrupting the cupula located in ampulla
Treatment:
Often resolves on own, but...
Specific head manoeuvres can reposition debris out
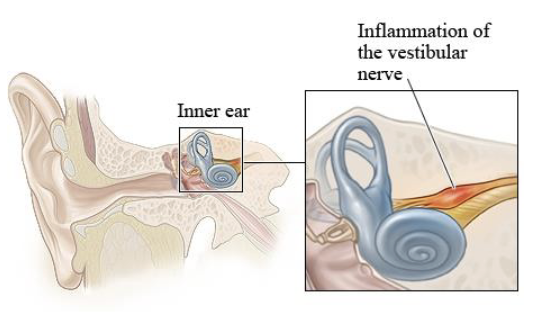
What is Vestibular Neuronitis (second most common)?
Caused by:
Inflammation of the vestibular nerve
Symptoms:
Sudden vertigo that can last for several days
Does not affect hearing
Treatment:
Anti-nausea medication until inflammation reduces
Steroids to reduce inflammation
Physical therapy/activity can help the body compensate (help with balance training)
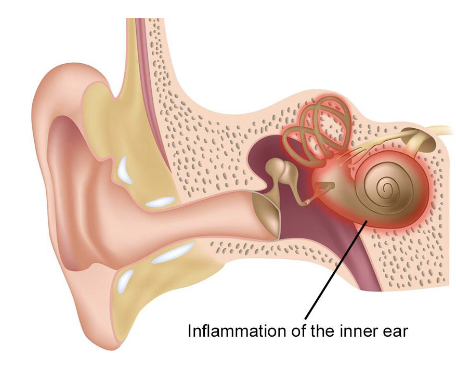
What are Labyrinthitis?
Caused by:
Inflammation of the entire inner ear due to infection
Symptoms:
Sudden vertigo that can last for several days
Does affect hearing
Treatment:
Treat infection
Anti-nausea medication until inflammation reduces
Physical therapy/activity can help the body compensate
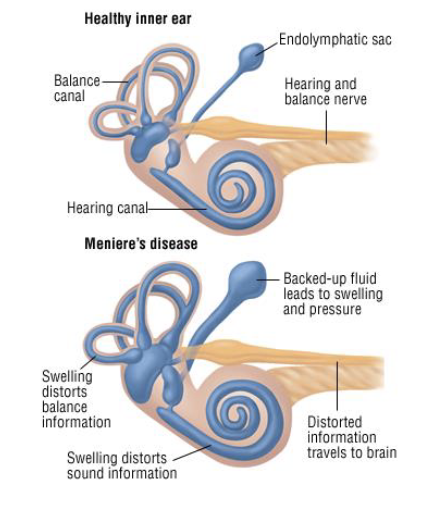
What is Meniere’s Disease?
Caused by:
Excessive fluid build up in inner ear
Unknown why this occurs
Symptoms:
Sudden episodes of: tinnitus, hearing loss, and/or vertigo
Each episode can last minutes to hours
May occur in clusters, then subside for years
Treatment:
No cure; managing symptoms
Can lead to permanent hearing loss, but rare
What does Somatosensory system respond to?
Distributed all over body
Responds to many kinds of stimuli
Subgrouped into 4 senses:
Touch
Pain
Temperature
Proprioception
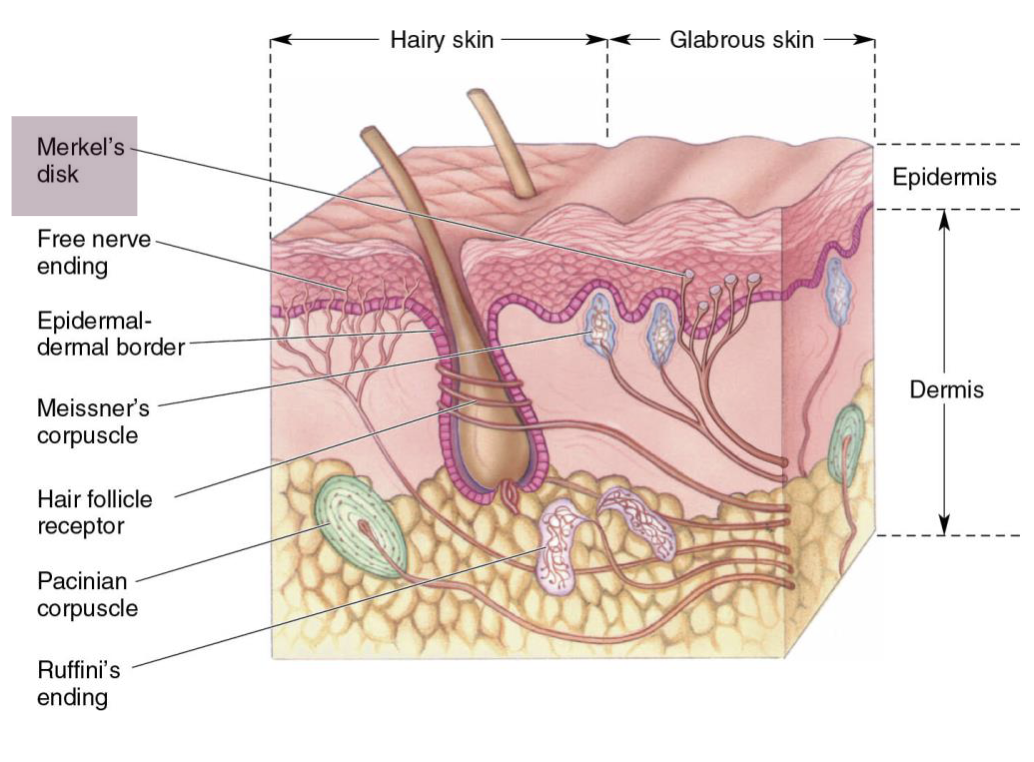
What are mechanoreceptors in skin?
Most somatosensory receptors are mechanoreceptors
Receptive to physical distortion
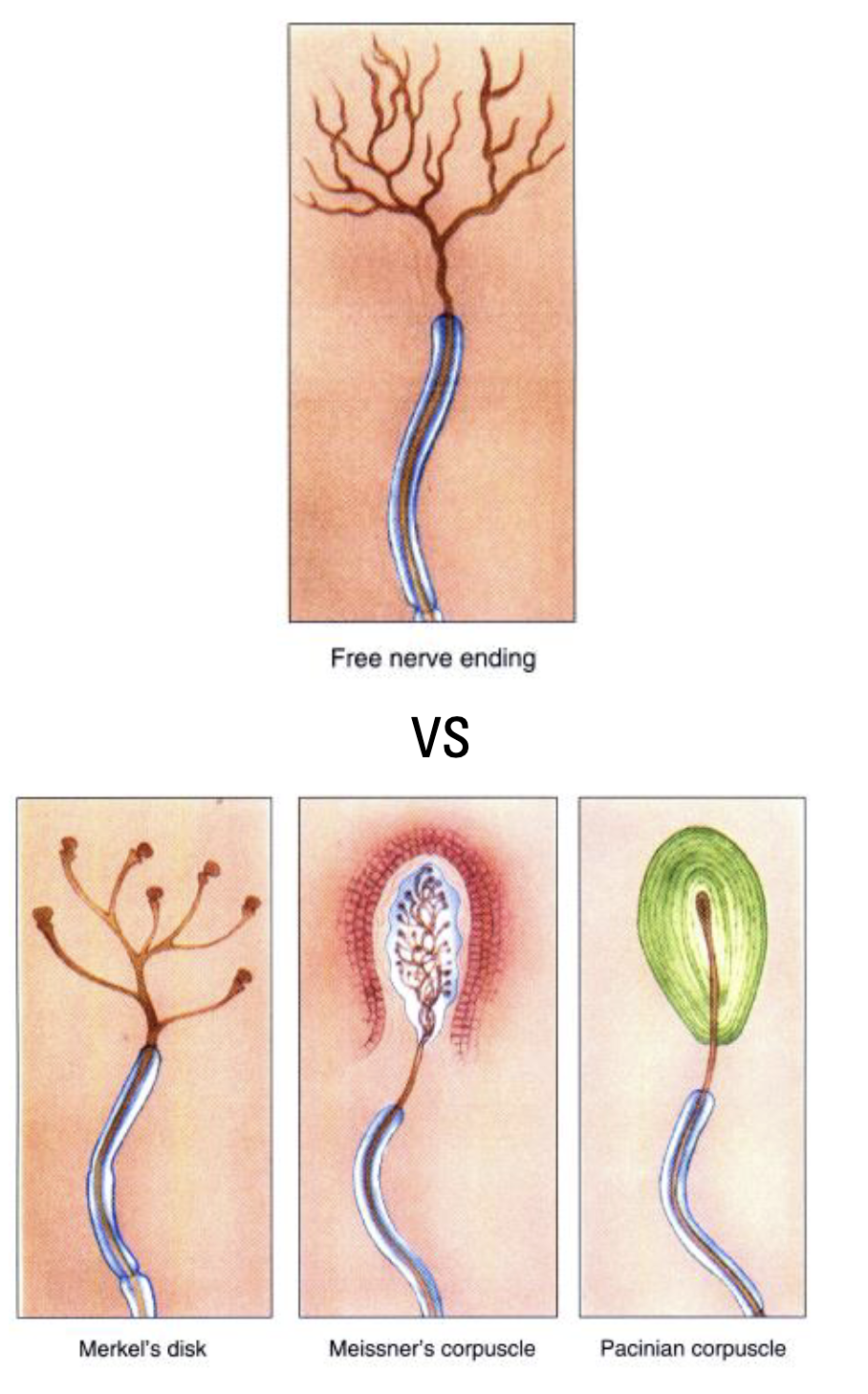
4 primary receptors in skin
Pacinian corpuscles
Meissner's corpuscles
Ruffini’s endings
Merkel's disks
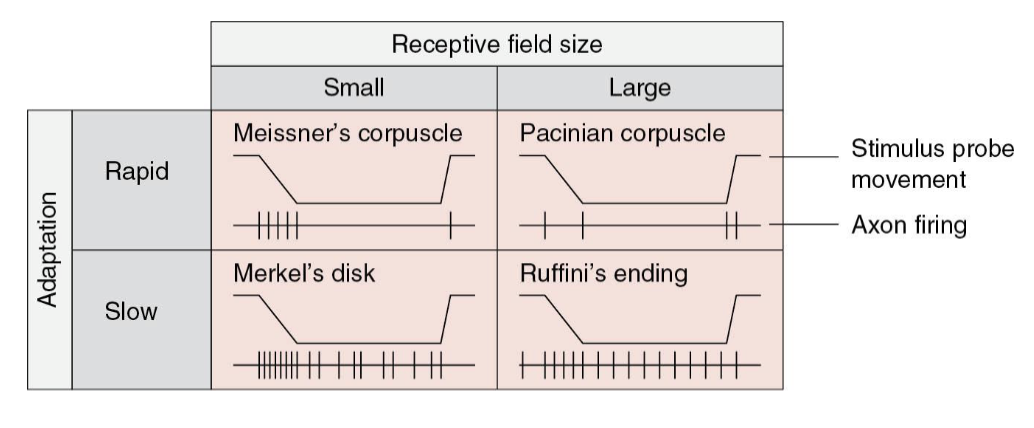
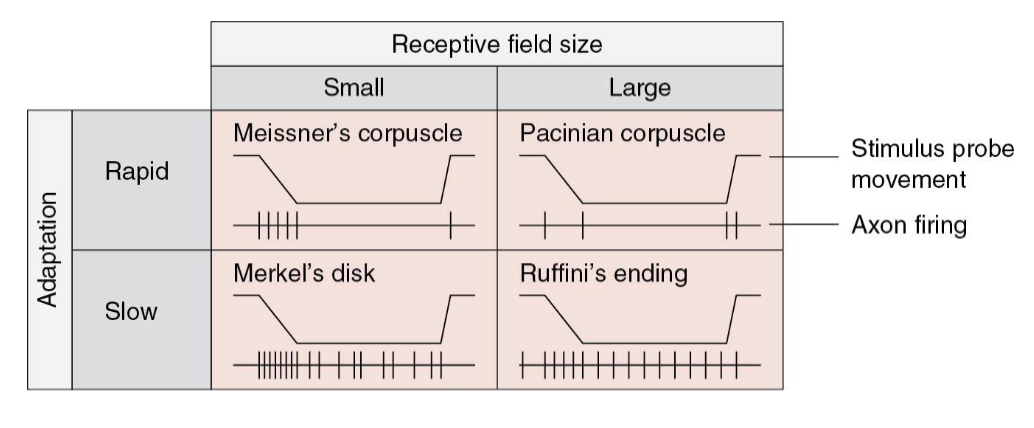
Vary in terms of:
Receptive field (large vs. small)
Adaptation (rapid vs. slow)
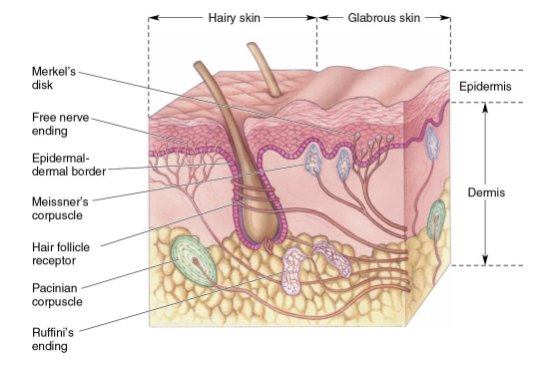
Which two mechanoreceptors in skin are likely measuring a small receptive field?
Merkel’s disk and Meissner’s corpuscle (closer to surface)
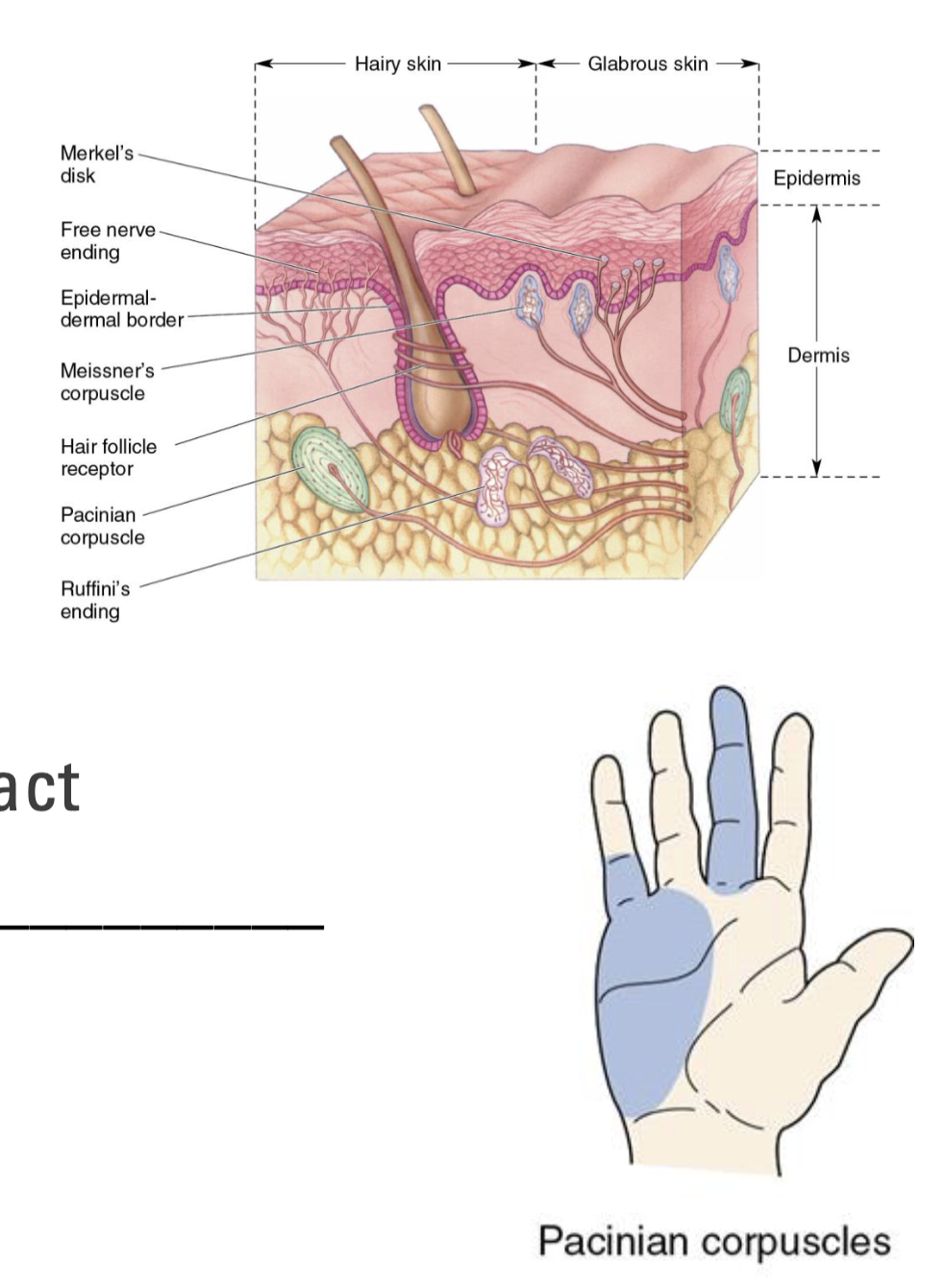
What are Pacinian Corpuscles?
Largest and deepest mechanoreceptor in skin
Get compressed and detect pressure and vibration
Large receptive field
Rapid adapting
React quickly to initial contact, but not sustained contact
Best at detecting finer textures and high frequency vibrations
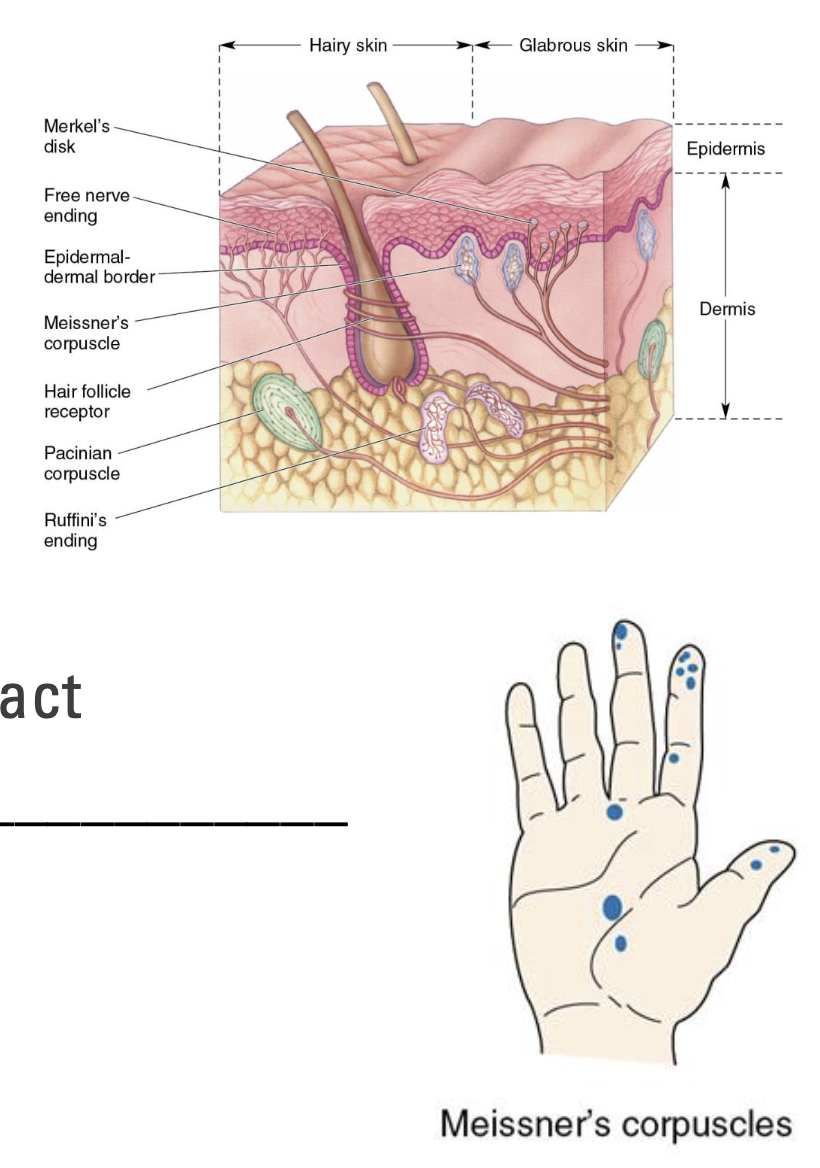
What are Meissner’s Corpuscles?
Small receptors in upper dermis; common in fingers
Detect fine touch and pressure
Small receptive field
Rapid adapting
React quickly to initial contact, but not sustained contact
Best at detecting heavier textures and lower frequency vibrations
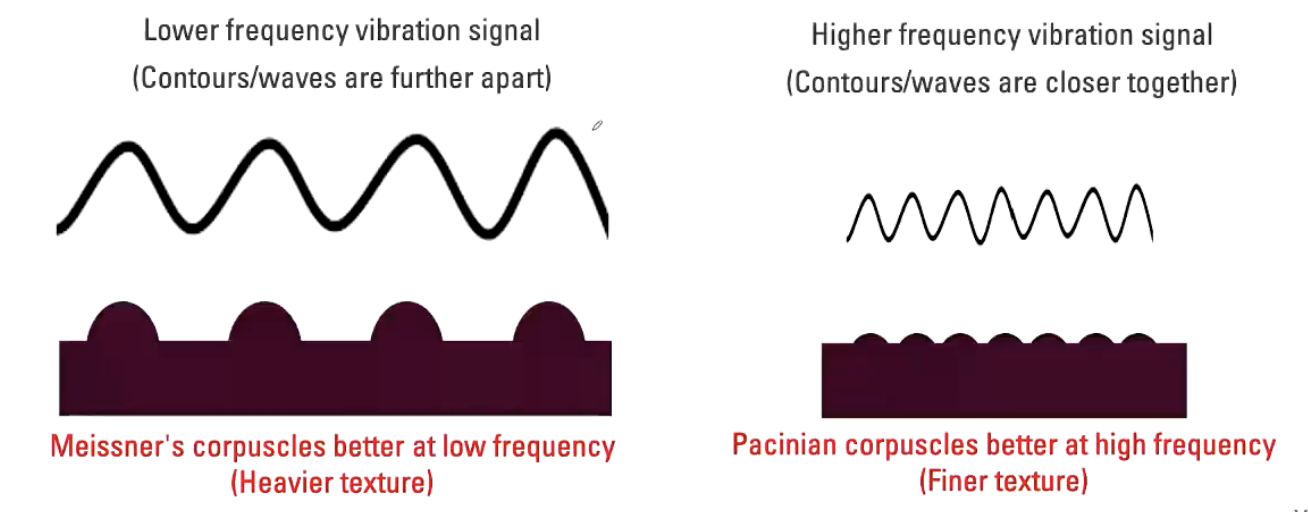
Explain rapid adapting mechanoreceptors and vibrations.
Lower frequency vibration signal (Contours/waves are further apart)
Meissner's corpuscles better at low frequency (Heavier texture)
E.g. Moving fingers across keys on a keyboard
Higher frequency vibration signal (Contours/waves are closer together)
Pacinian corpuscles better at high frequency (Finer texture)
E.g. Moving hand across the surface of smooth table
What are Ruffini Endings?
Large receptors in the dermis layer
Detect stretch and deformation
Large receptive field
Slow adapting
React to sustained deformations
Best at detecting grip/position
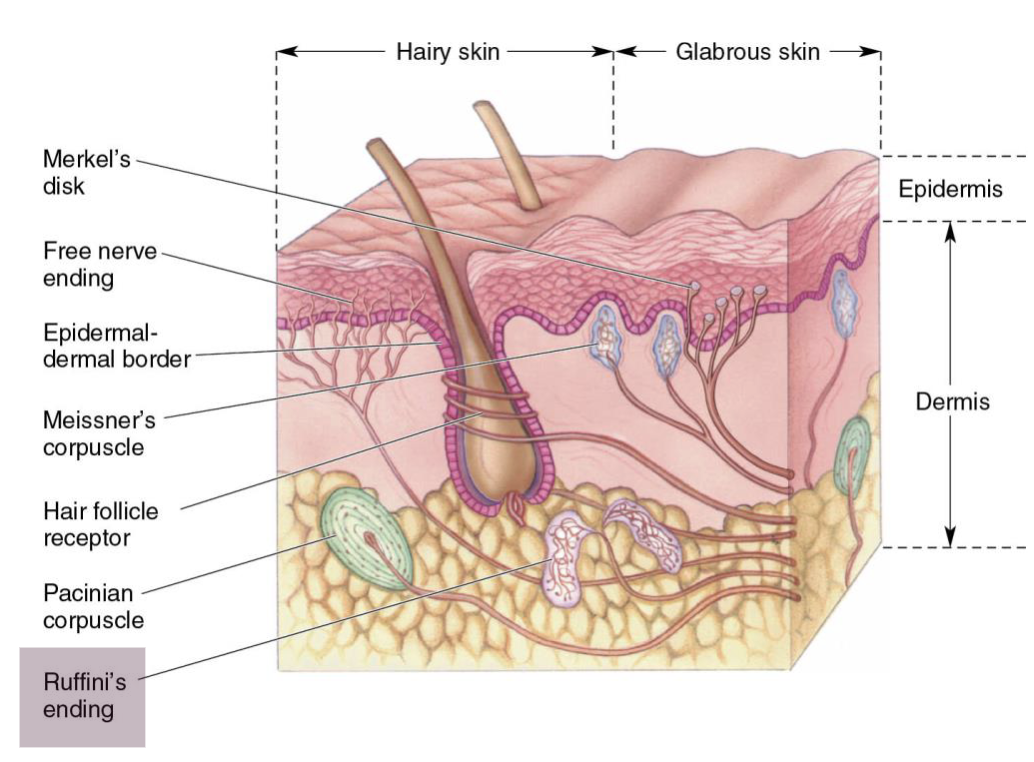
What are Merkel’s Disks?
Small receptors in epidermis, common in fingers
Detect fine touch and pressure
Small receptive field
Slow adapting
React to sustained deformations
Best at static discrimination of shapes/textures
What is the receptive field size and adaptation rate?
We can combine all 4 into a 2x2 chart
Most things we feel involve some input from all
Examples:
Catching a football? Pacinian corpuscle
Reaching into your backpack to find your favourite pen? Merkel’s disk
Holding someone’s hand? Ruffini’s ending
Petting your dog? Pacinian corpuscle
Holding guitar cord? Merkel’s disk
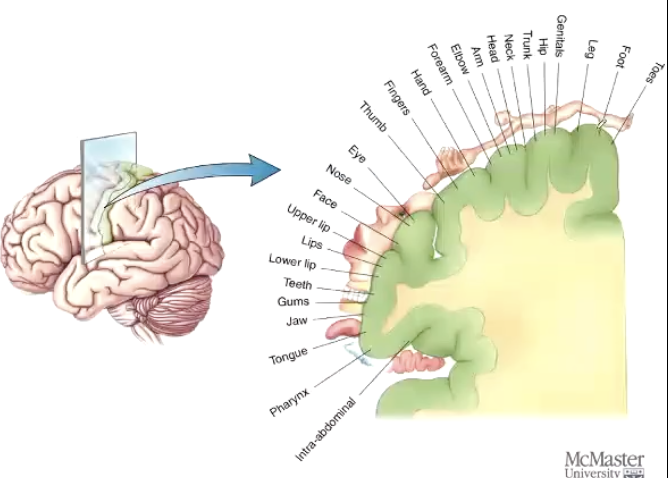
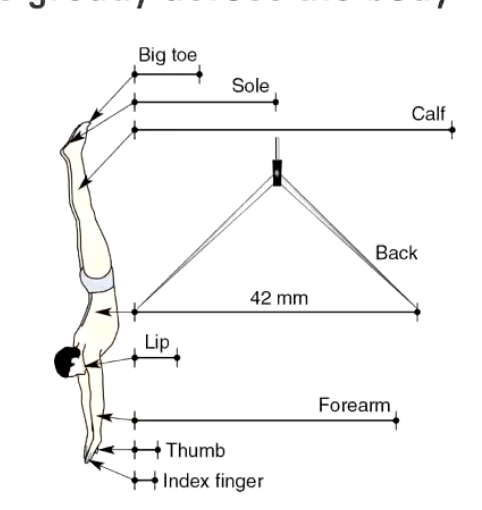
What is Two-Point Discrimination?
Sensitivity to discriminate small points varies greatly across the body
More sensitive in important places
Accomplished by:
Greater density of mechanoreceptors
Smaller field size (2 M’s - Meissner/Merkel)
Greater brain tissue devoted to those areas
Could barefoot running or walking be better than “shod”?
Improve sensory information coming from the feet
Could this improve/speed up the rapid mechanical receptor time period?
Can we train our fast adaptors?
Highly debated!
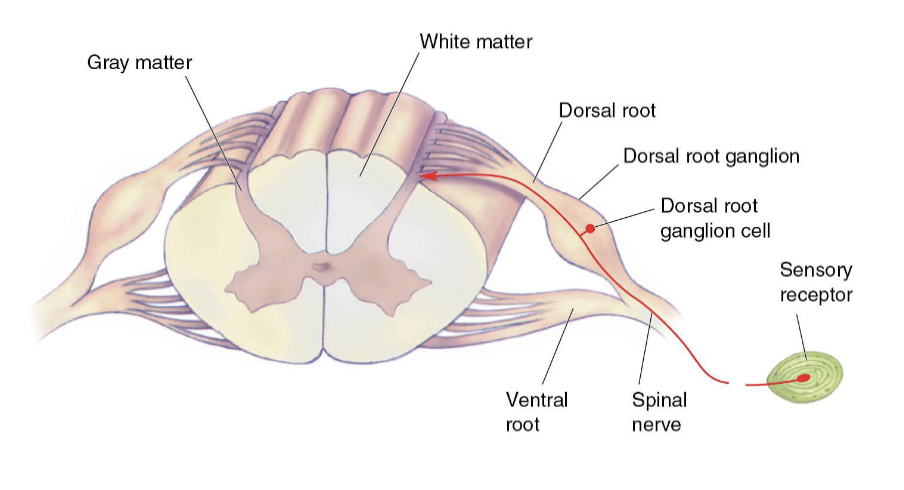
What is the path to the brain, beginning with an axon?
Primary Afferent Axon
AKA: First order neuron; Sensor to spinal cord
Enters spinal cord at dorsal root
Cell bodies lie in dorsal root ganglion
Pseudo-unipolar neurons
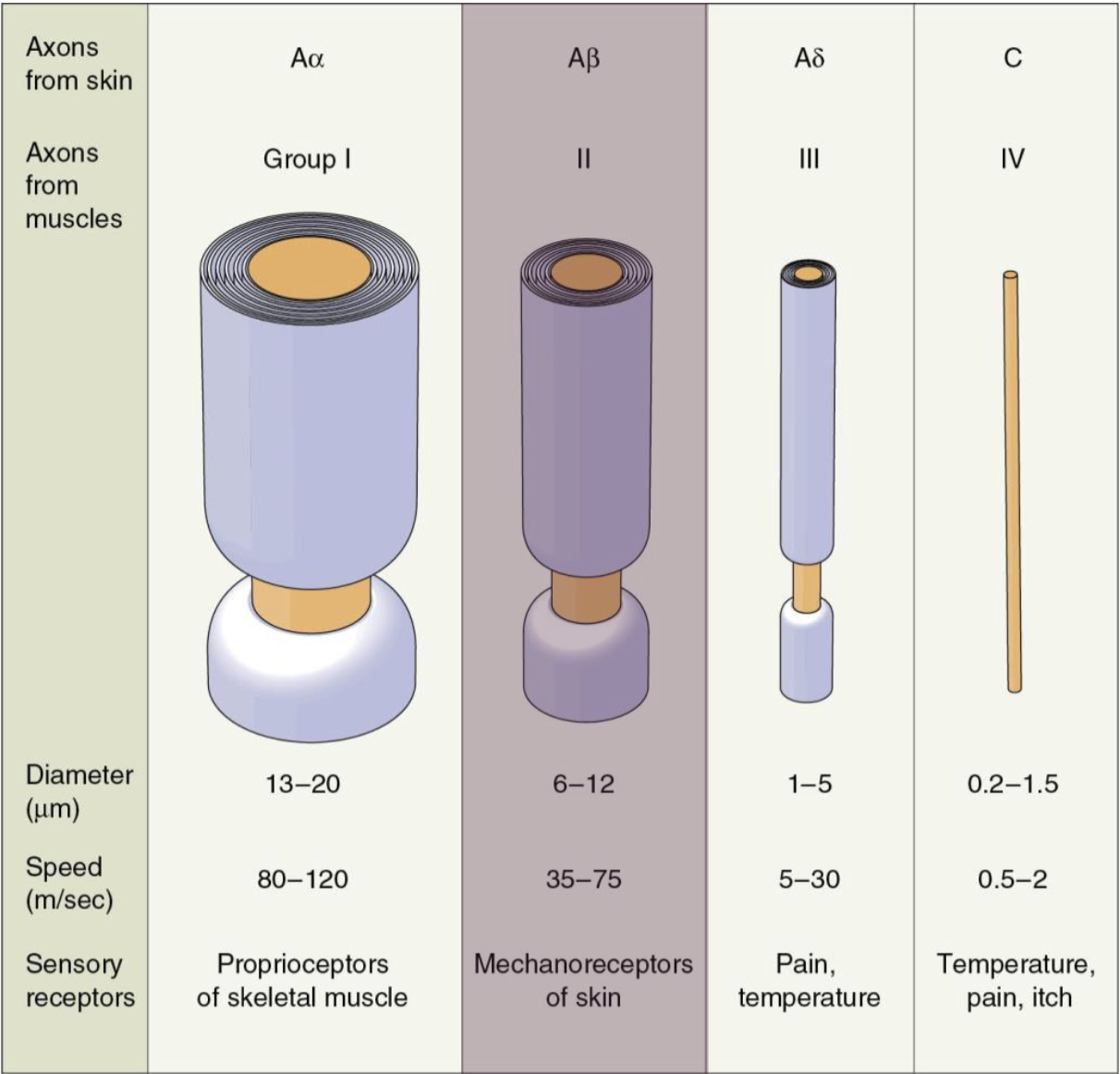
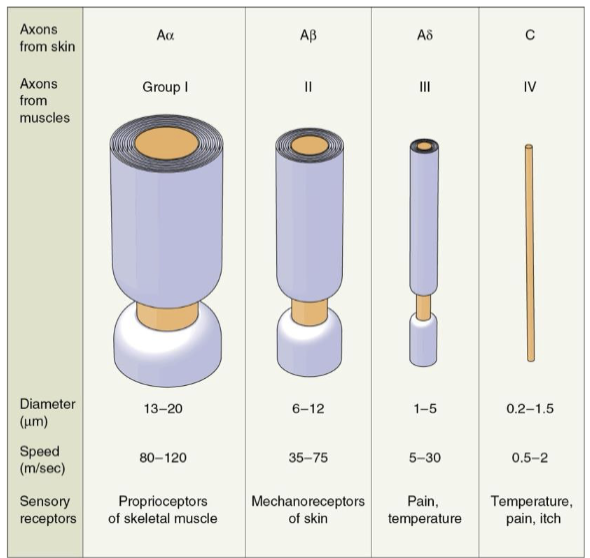
Four types of primary afferent axons:
Aα (proprioception), Aβ (touch), Aδ (pain), C axons (slow pain/itchy)
Aβ mediates touch
What are the various sizes of primary afferent axons?
All A’s are myelinated
Larger + myelination = faster
Aα proprioceptors are faster than Aβ mechanoreceptors for quick reflexes
C’s are NOT myelinated
Smaller and slower
What is the path to the brain, into the spinal cord?
Two Aβ branches:
Directly ascending the spinal cord to the brain
Synapses with second-order sensory neuron (for reflexes)
Most second-order sensory neurons lie in the dorsal horn
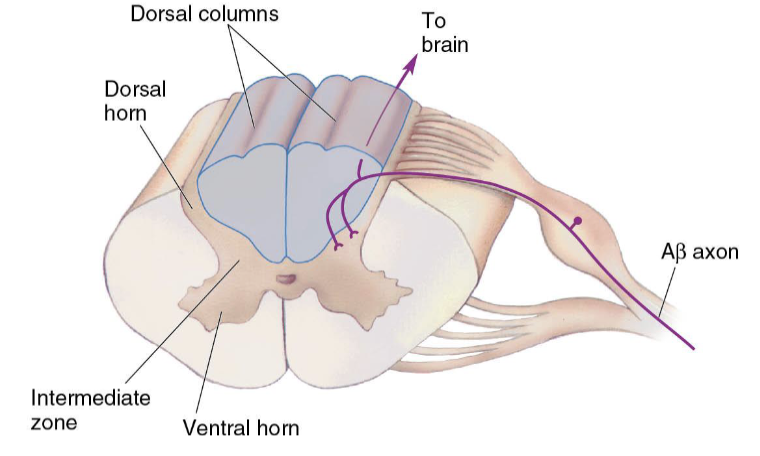
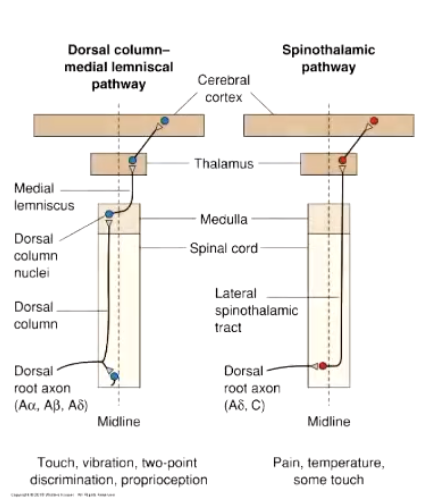
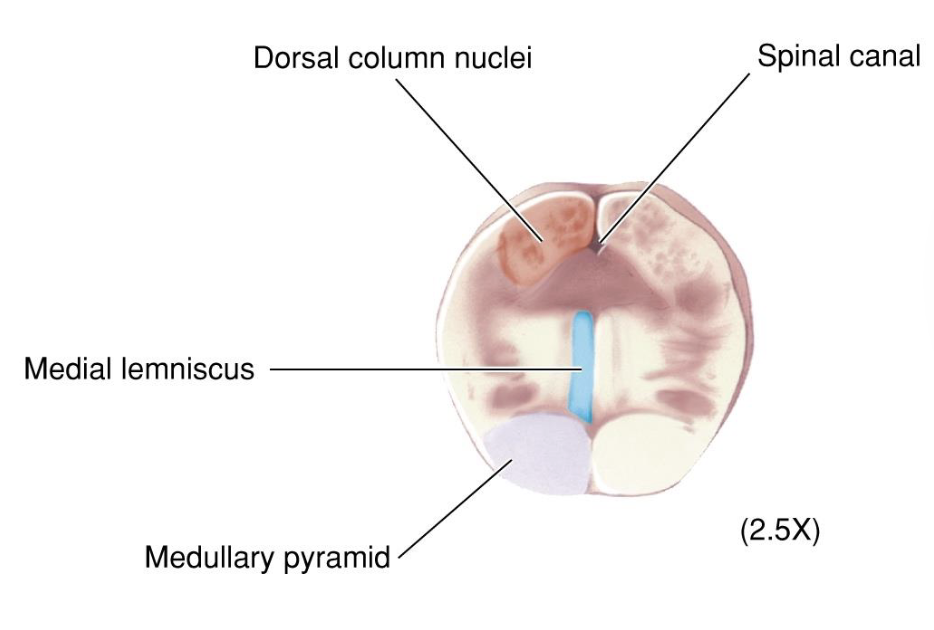
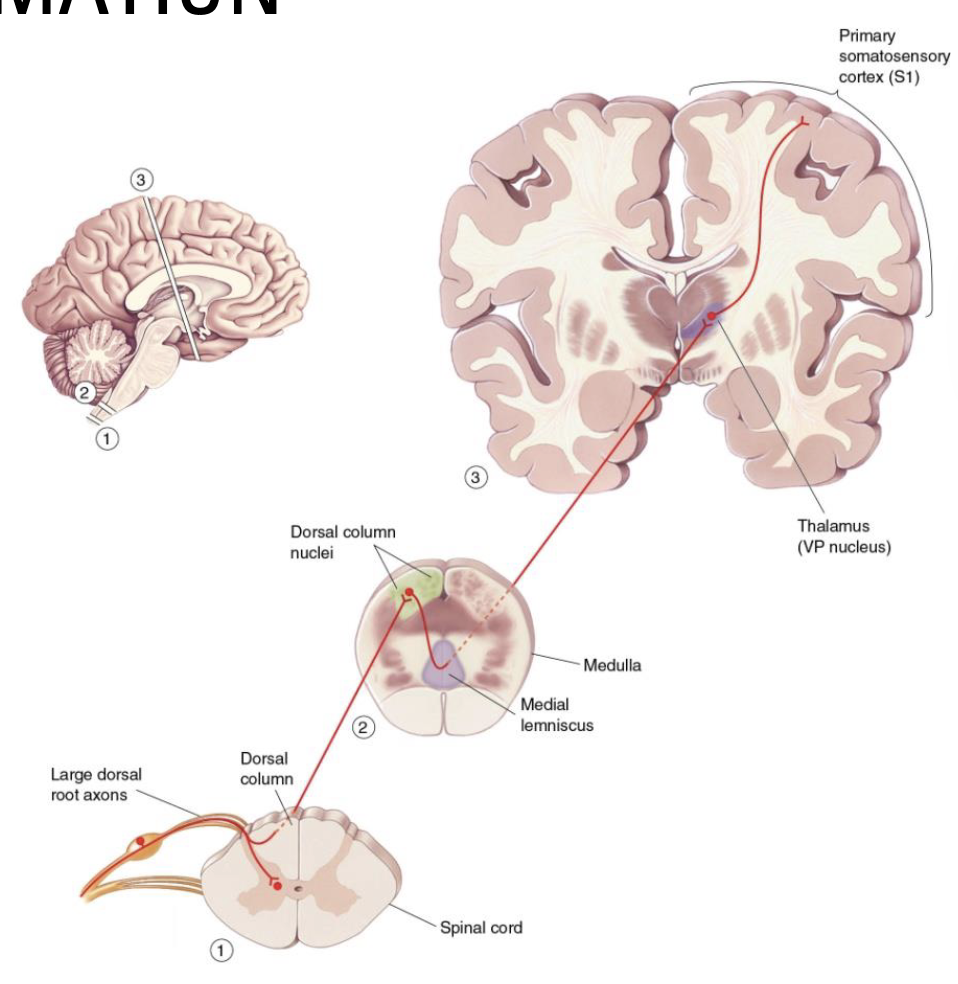
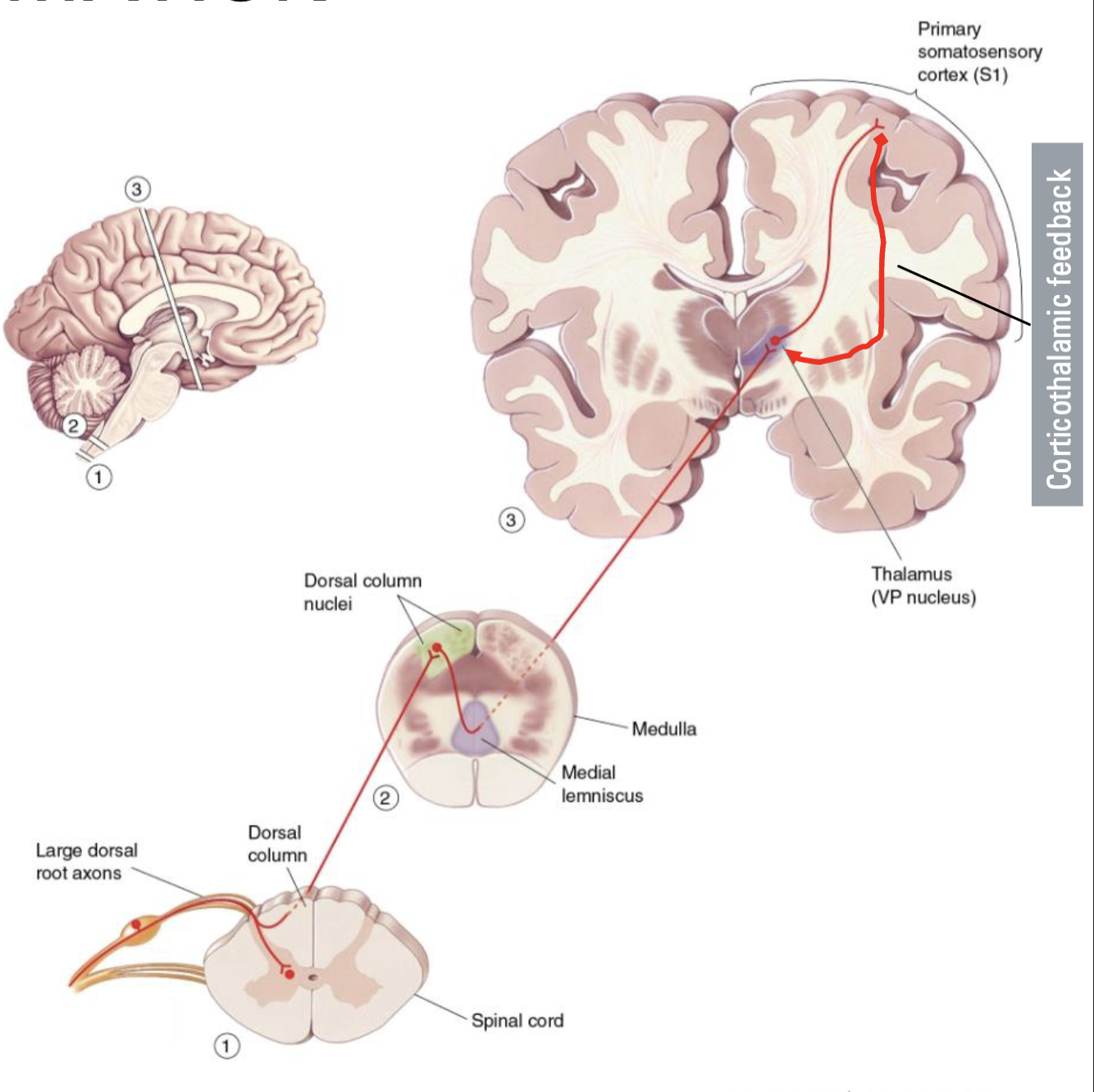
What is the Dorsal Column (Touch Information)?
Dorsal Column-Medial Lemniscal Pathway (DCML)
Ascending branch goes up the dorsal column
Synapse on the dorsal column nuclei in medulla
Dorsal column nuclei axons decussate and ascend the medial lemniscus
Synapse in the VP nucleus of the thalamus
Neurons in the VP nucleus project to somatosensory cortex
Terms: Ipsilateral (Same side) vs. Contralateral (Opposite side)
What is the DCML?
DCML = 3 neuron pathway with 3 synapse points required to reach S1
These exist for a reason other than simply passing along information
We can assume information is altered at each synapse
Adjacent inputs can be inhibited to enhance tactile stimuli
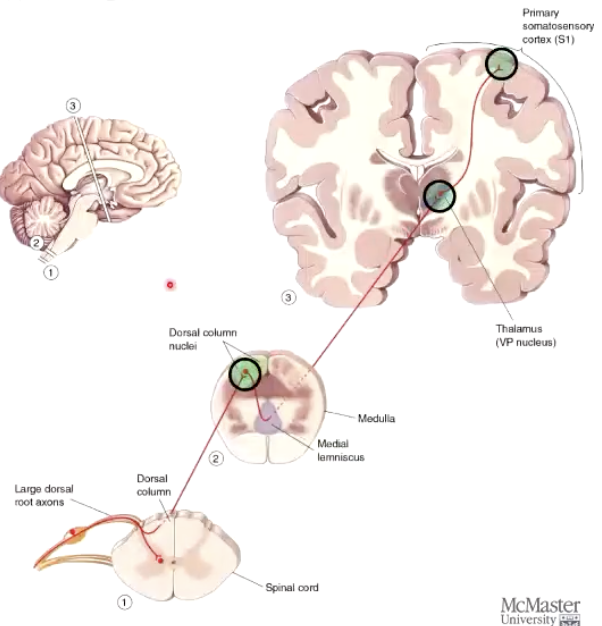
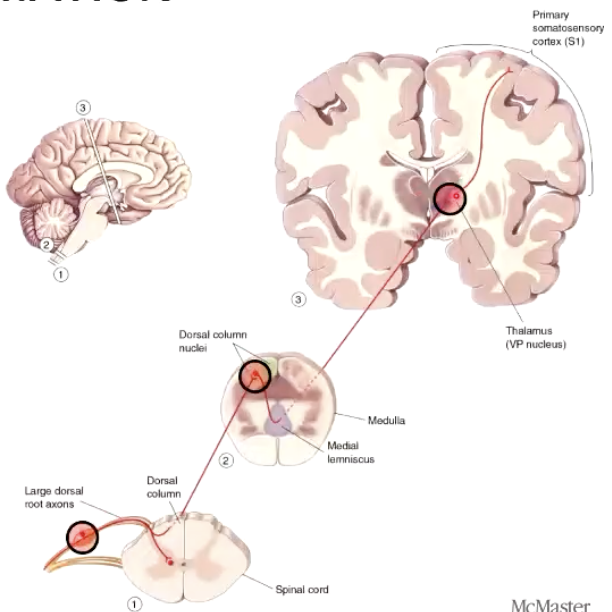
What are the 3 neurons, and 3 synapses of DCML?
3 neurons (Red)
First-order, second-order, third-order
3 synapses (Green)
First to second, second to third, third to cortex
No synapse until it reaches medulla
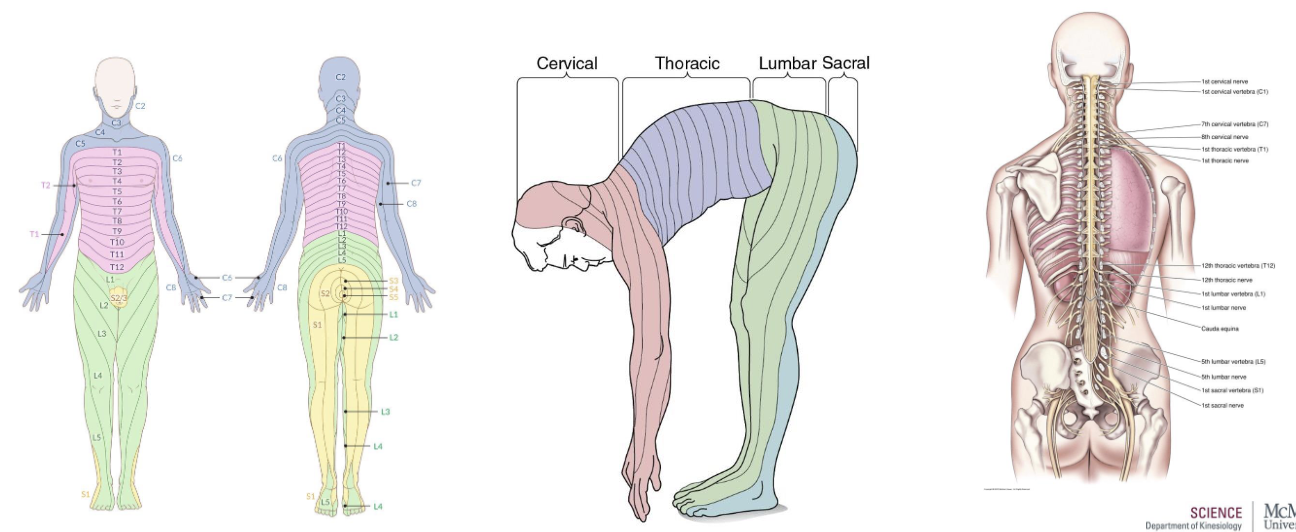
What is the segmental organization of spinal cord?
Dermatomes diagram – The distribution/mapping of spinal nerves
Comes from an evolutionary standpoint (all 4s → bipedalism)
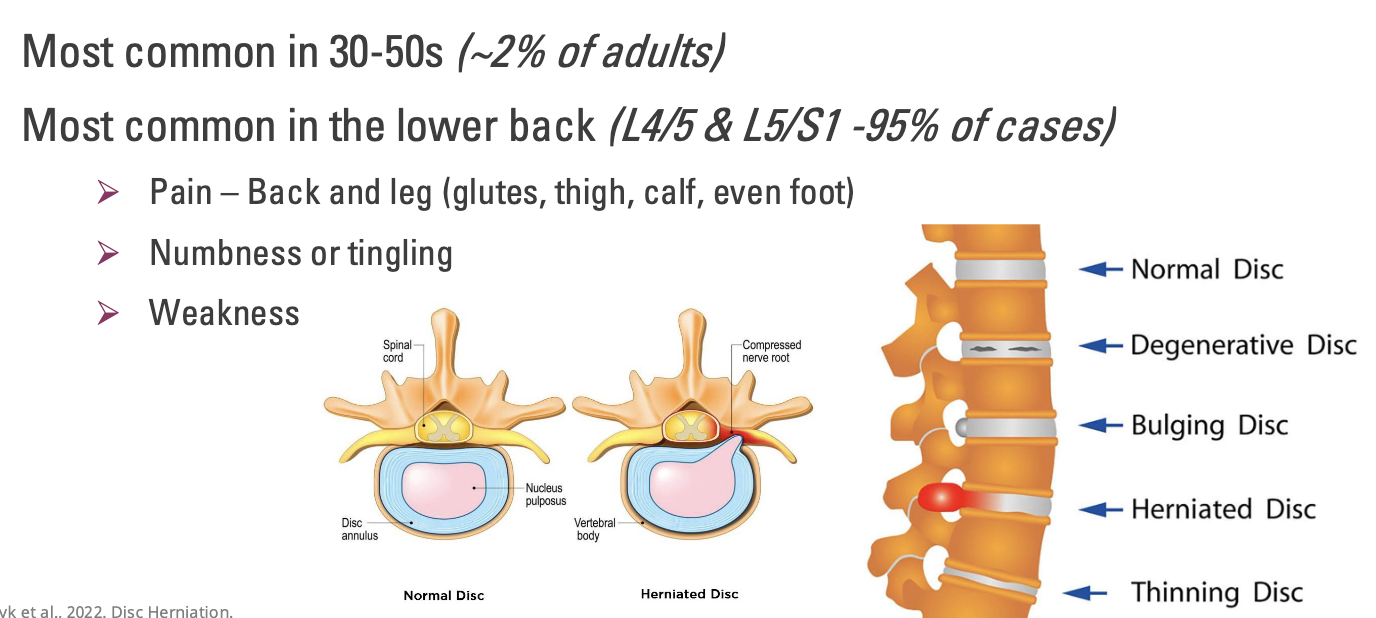
What is a Herniated Disc?
Most common in 30-50s (~2% of adults)
Most common in the lower back (L4/5 & L5/S1 -95% of cases)
Pain – Back and leg (glutes, thigh, calf, even foot)
Numbness or tingling
Weakness
**Reported as pairs, because we talk about the disc in between the 2 vertebra
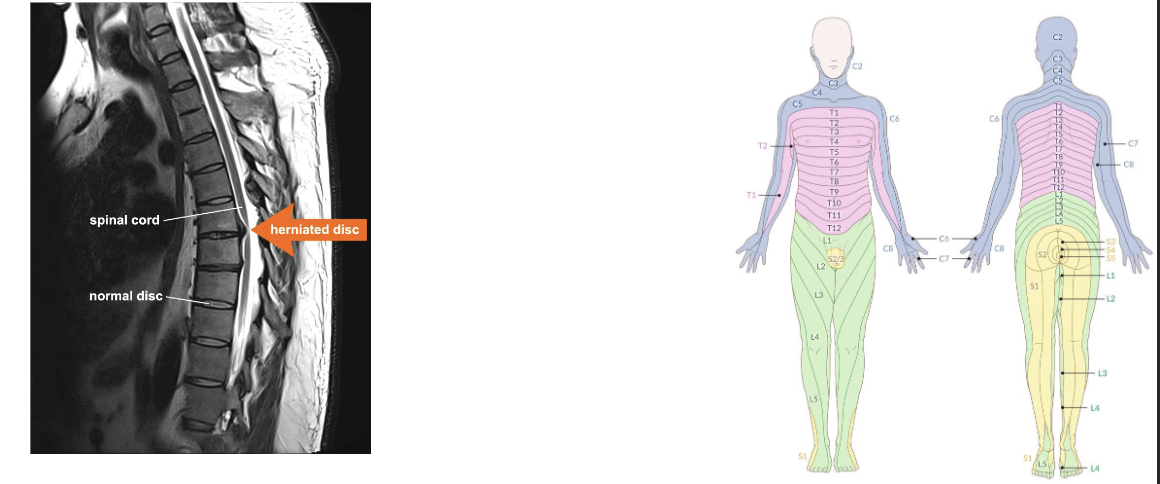
How to test for Herniated Disc?
Physical exam, Imaging, and/or even nerve tests for diagnosis
Herniated discs cause localized and radiating pain by compressing the spinal cord or nerve roots, with pain location often indicating the affected level
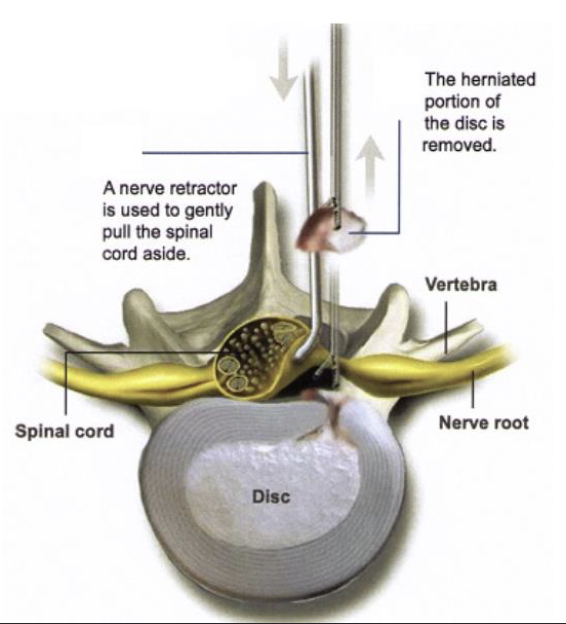
What are treatment options for Herniated Disc?
1. Rest, physical therapy, pain medications
85% resolve in 8-12 weeks
2. Surgical – Discectomy/Microdiscectomy
Conservative failed to resolve
Progressive/debilitating pain, numbness, and weakness
Why is lateral inhibition (overlapping neurons) important for touch information?
Inhibit adjacent inputs to enhance tactile sensitivity
Increases contrast to allow for more precise/finer location of sensation
Graph: Purple shows frequency of APs
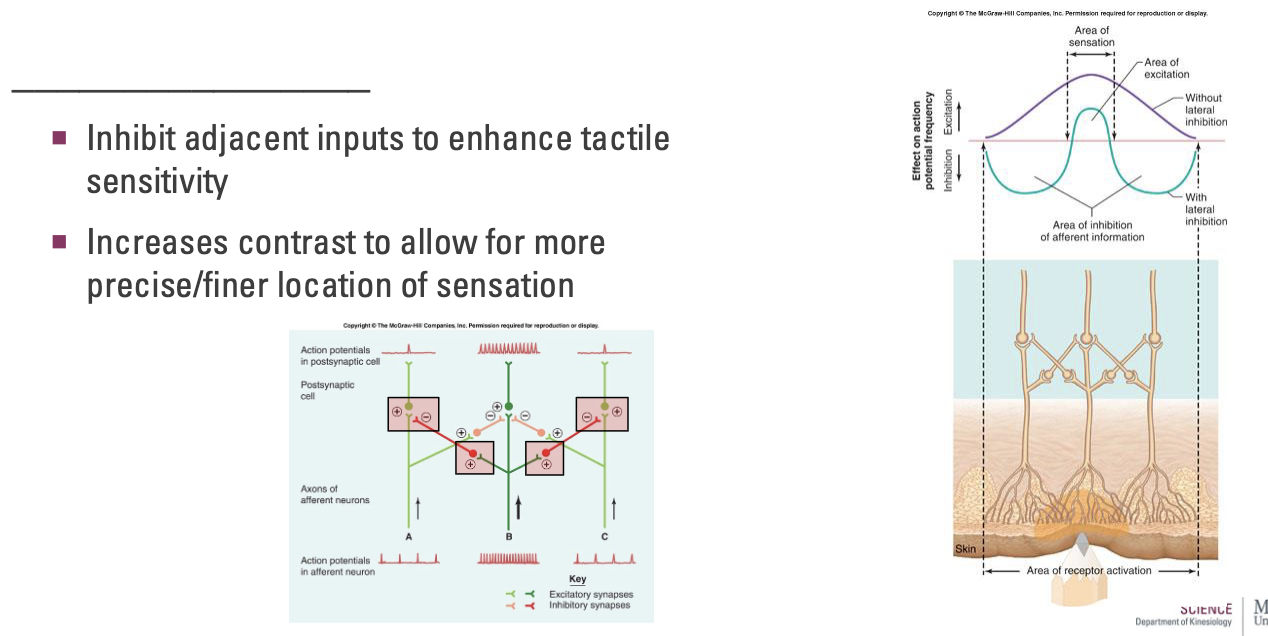
What is Sensory gating?
Corticothalamic feedback influences sensory processing
Cortex helps to filter irrelevant or repetitive information
“Feel what you want to feel”
However, these complex pathways remain unclear
May be related to many cognitive disorders...
Ex: Schizophrenia (extreme), ADHD (less extreme)
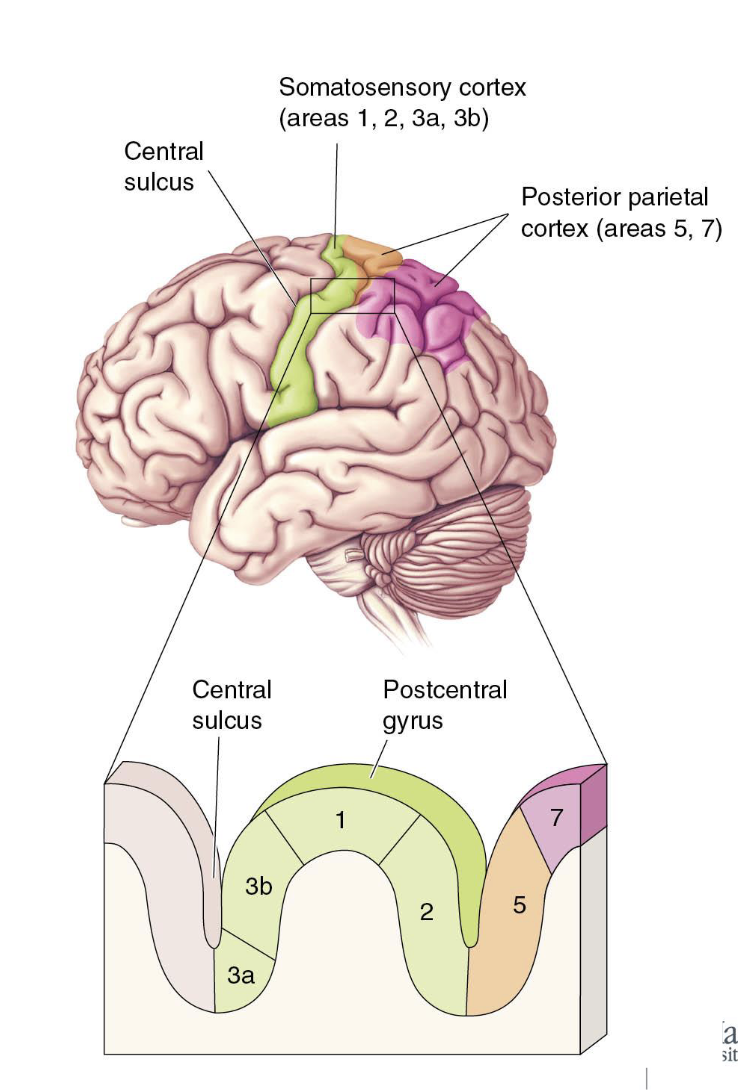
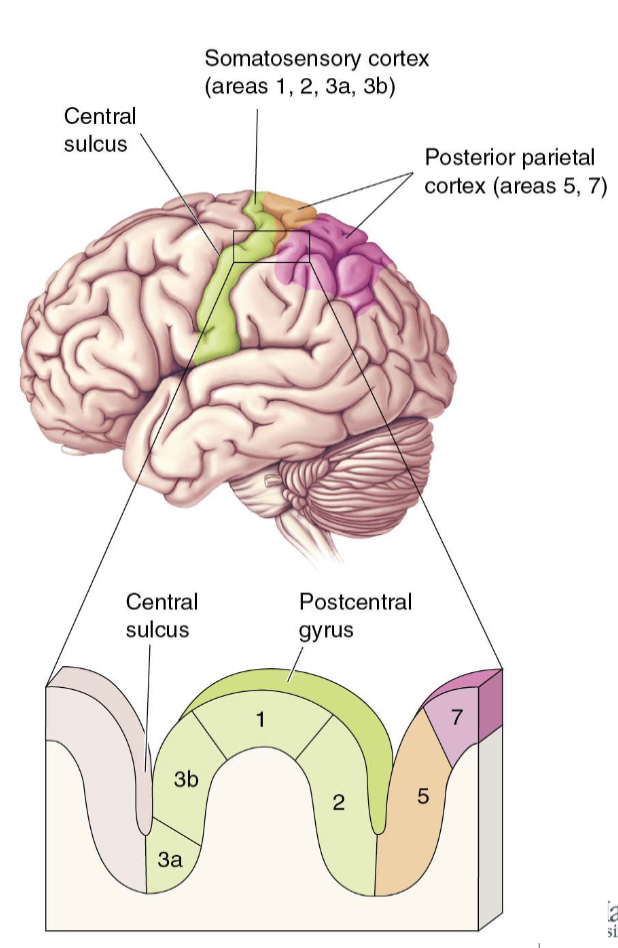
How do we know 3b is the primary input site?
Primary somatosensory cortex = 3b
Receives inputs from VP nucleus
Highly responsive to somatosensory input
Damage impairs sensation
Electrical stimulus creates sensations
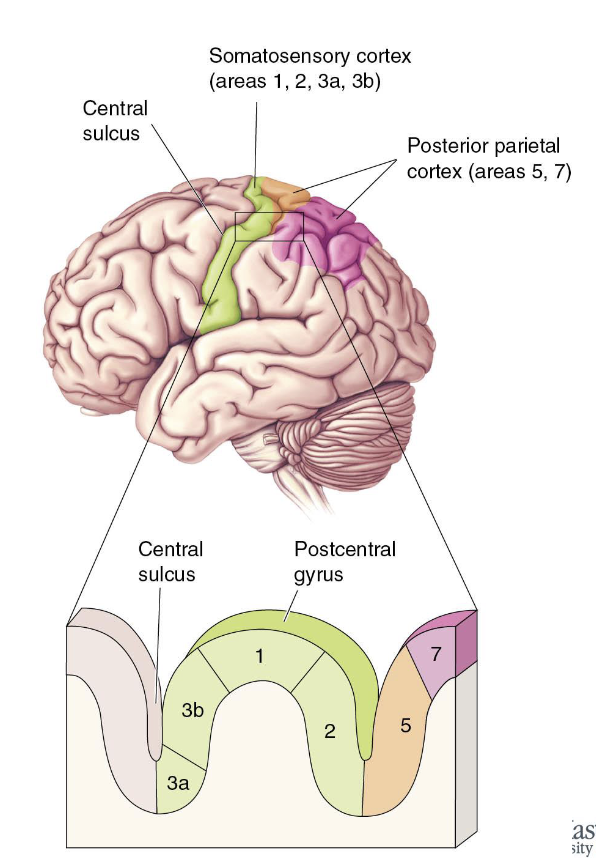
What are the areas adjacent to 3b?
Somatosensory 3a
Dense thalamus input, but more body position
Somatosensory 1 & 2
Receives information from 3b
Generally related to texture, size, and shape
What is the contribution of Wilder Penfield?
American-Canadian neurosurgeon
Discovered stimulating parts of the cortex could evoke vivid and specific memories, including sounds and smells
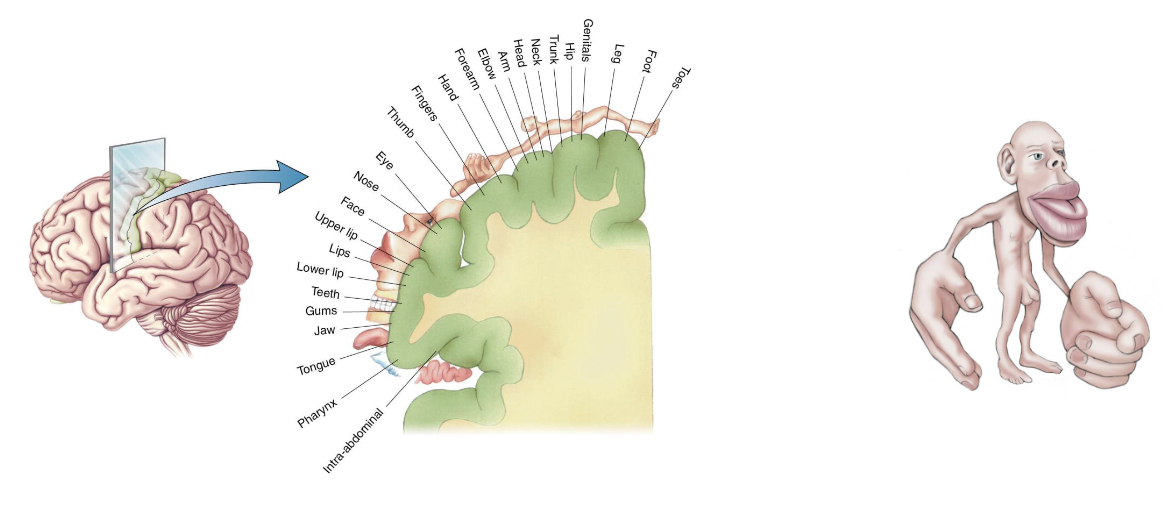
What is Cortical Somatotopy, Homunculus?
Mapping of the somatosensory cortex
Homunculus represents the density of sensory input
What is the Posterior Parietal Cortex?
Allows for the processing of basic sensory information and integration with other senses
Posterior parietal cortex 5 (orange)
Sensory integration for the planning and organization of movement
Posterior parietal cortex 7 (pink)
Sensory integration for object recognition and spatial relationships
What is pain and nociception?
Nociceptors: receptors of painful stimuli
Activated by stimulus that may damage tissue
Strong mechanical stimulation, temperature extremes, oxygen deprivation, chemicals; even substances released by damaged cells (lactic acid, histamine, etc.)
Nociception ≠ pain
Nociception = sensory process that provides the signals that MAY trigger pain
Pain = sore, aching, throbbing sensations we “feel”; can be influenced by past experiences
Nociception can exist without pain
Pain can exist without nociception
What are types of Nociceptors?
Free nerve endings, which bring the sensation of pain to CNS
Types of Nociceptors
Mechanical nociceptors - Respond to damage such as cutting, crushing, or pinching
Thermal nociceptors - Respond to temperature extremes
Chemical nociceptors - Respond to histamine and other chemicals
Polymodal nociceptors - Respond equally to all kinds of damaging stimuli
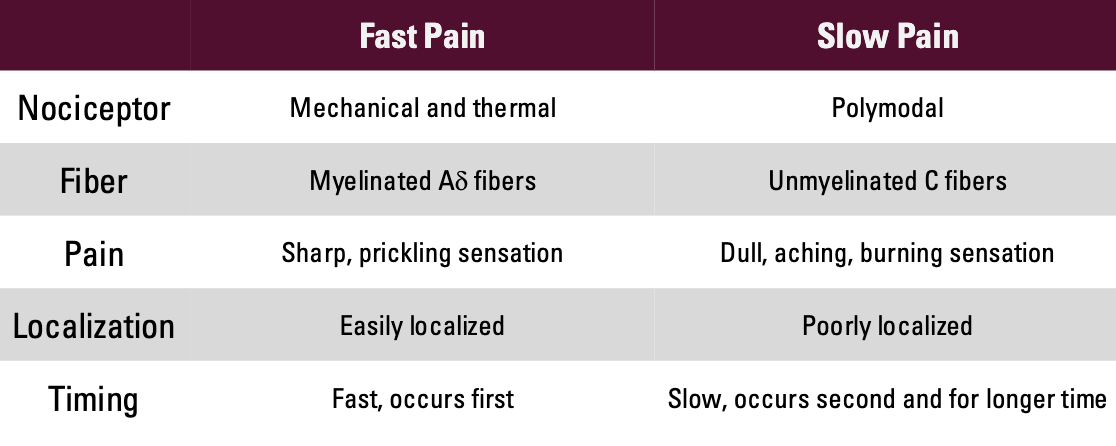
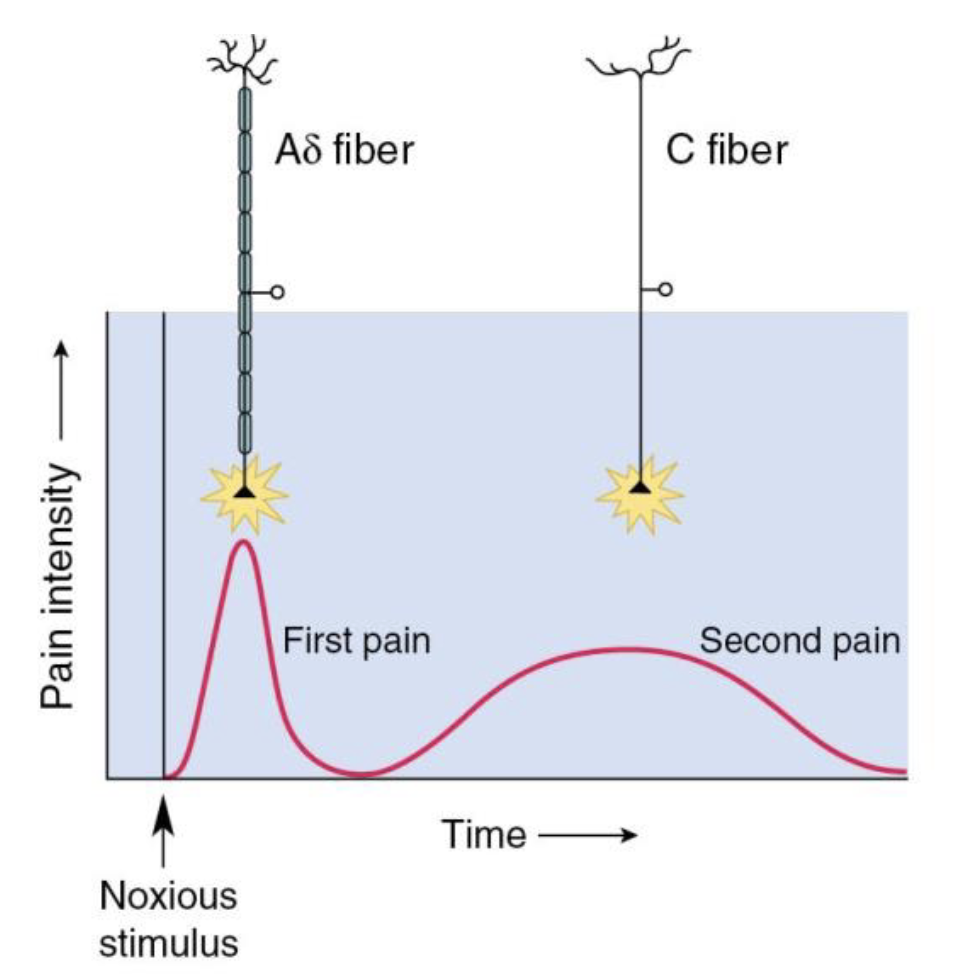
How do different types of pain involve different types of fibers?
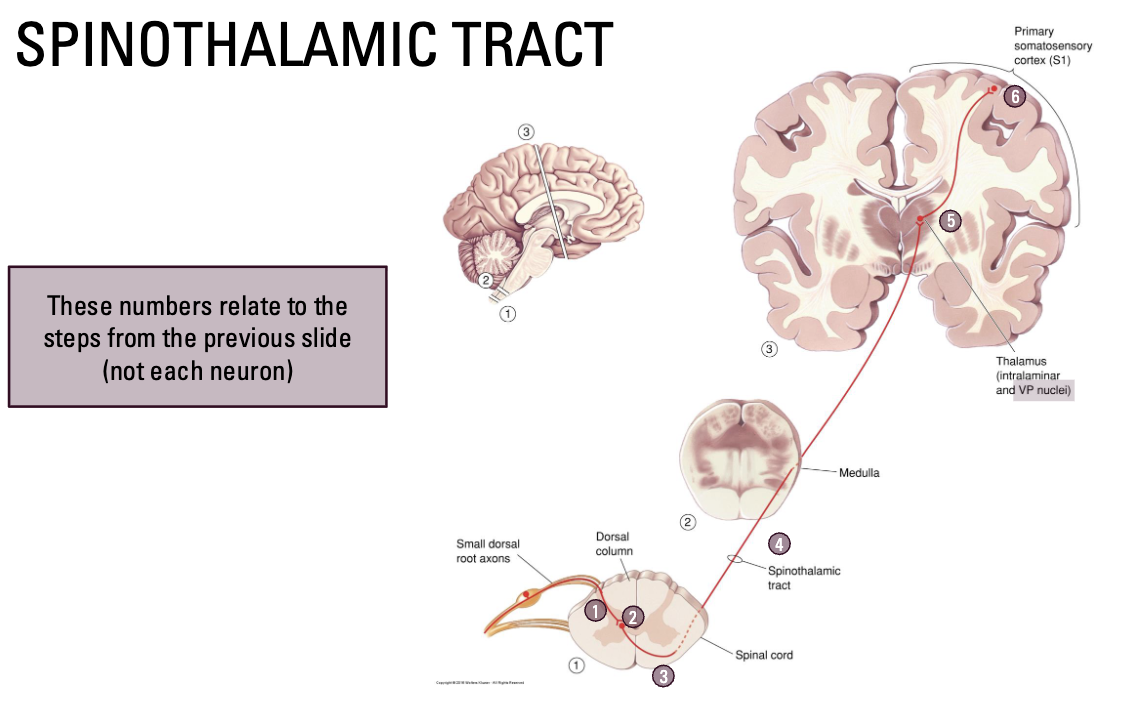
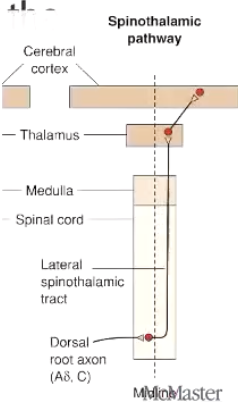
What is the Spinothalamic Tract?
To carry nociceptive information to brain
Cell bodies in dorsal root ganglion
Axons enter dorsal horn of spinal cord
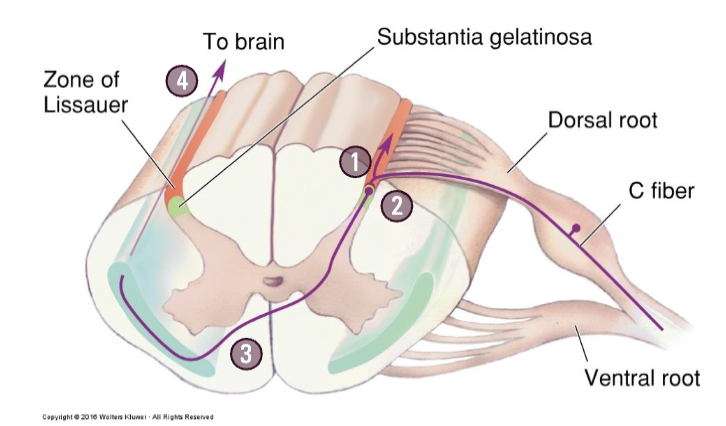
What is the pathway of carrying nociceptive information through Spinothalamic Tract?
Enter zone of Lissauer (ascend or descend slightly)
Synapse in the substantia gelatinosa (in the dorsal horn)
Second order neurons in the spinal cord immediately decussate
Ascend to the brain in the ventrolateral surface of the spinal cord
Synapse with VP nucleus (and other areas) in the thalamus
Information then projected the somatosensory cortex
NOTE: Pain is complex and can be difficult to localize in the brain. It is also highly integrated with medial structures related to emotion/memory
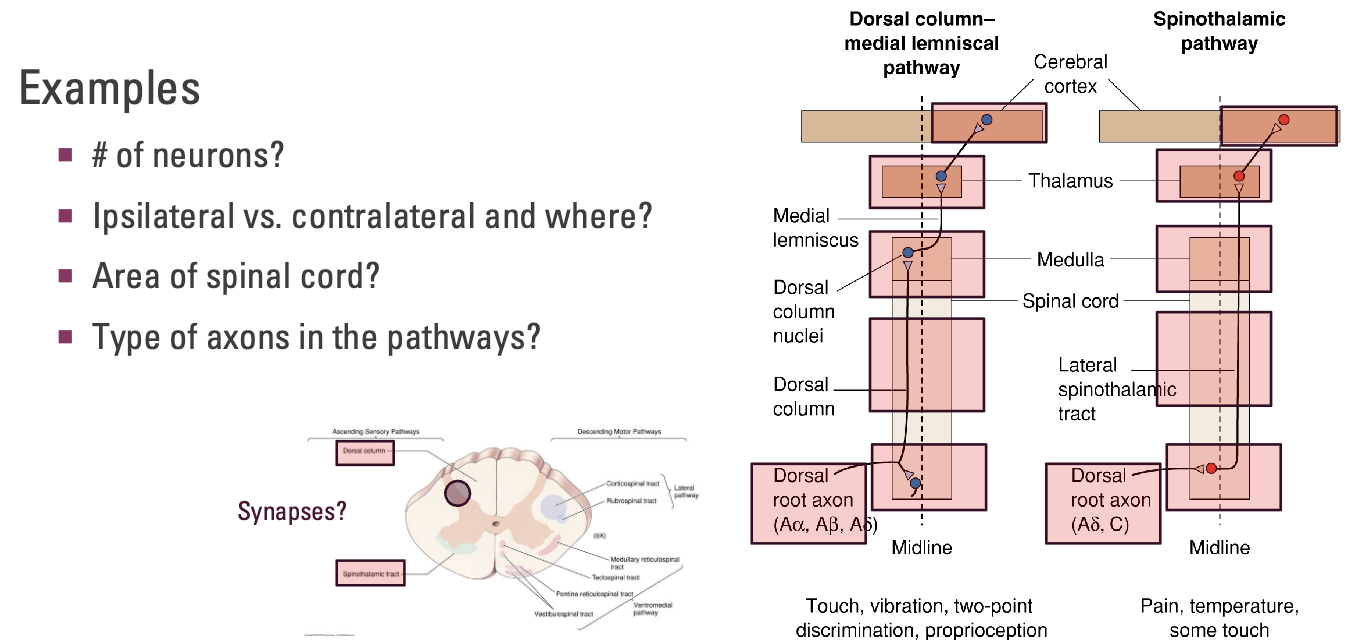
How can you compare the 2 major ascending pathways?
# of neurons?
DCML: 3
STT: 3
Ipsilateral vs. contralateral and where?
DCML: Ipsilateral to start, contralateral at medulla
STT: Contralateral immediately and stays contralateral
NEXT TEST
Area of spinal cord?
DCML: Dorsal column
STT: Lateral spinothalamic tract
Type of axons in the pathways?
DCML: Aα (proprioception), Aβ (touch), Aδ (pain)
STT: Aδ (pain), C axons (slow pain/itchy)
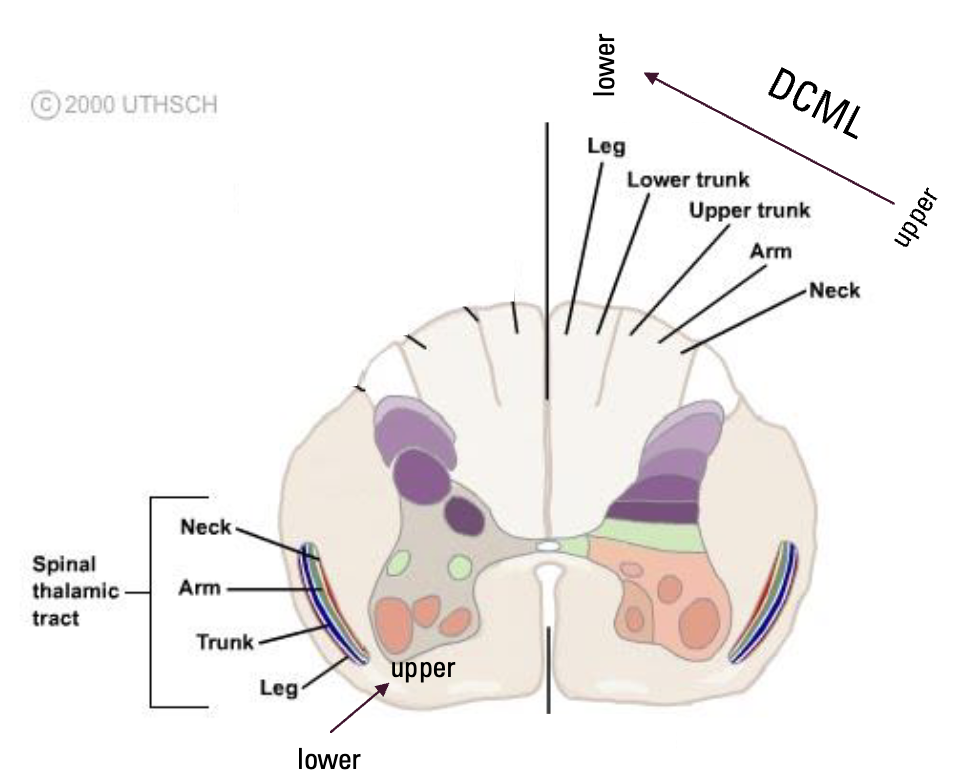
What is the general organization of these pathways?
DCML
Upper body tracts more lateral
Lower body tracts more medial
Spinothalamic
Upper body tracts more deep
Lower body tracts more superficial
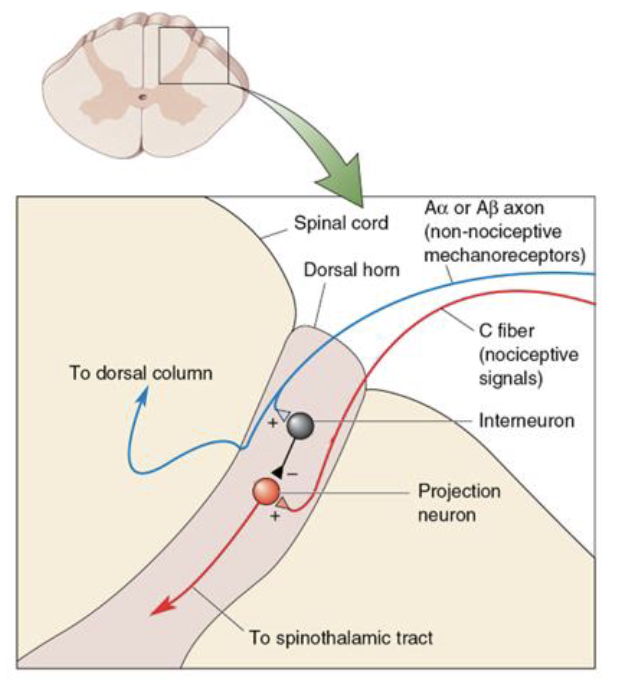
Pain Regulation - Afferent Regulation
Pain can be reduced by the activity of mechanoreceptors
Gate control theory of pain
Neurons in the spinothalamic tract may be inhibited by Aα or Aβ sensory nerves (touch) in the dorsal horn of the spinal cord.
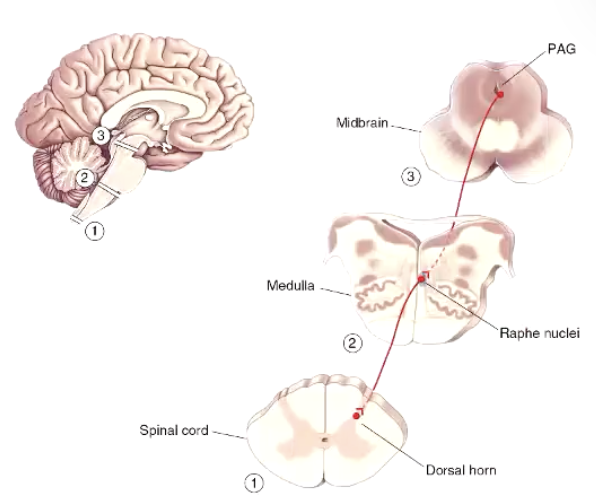
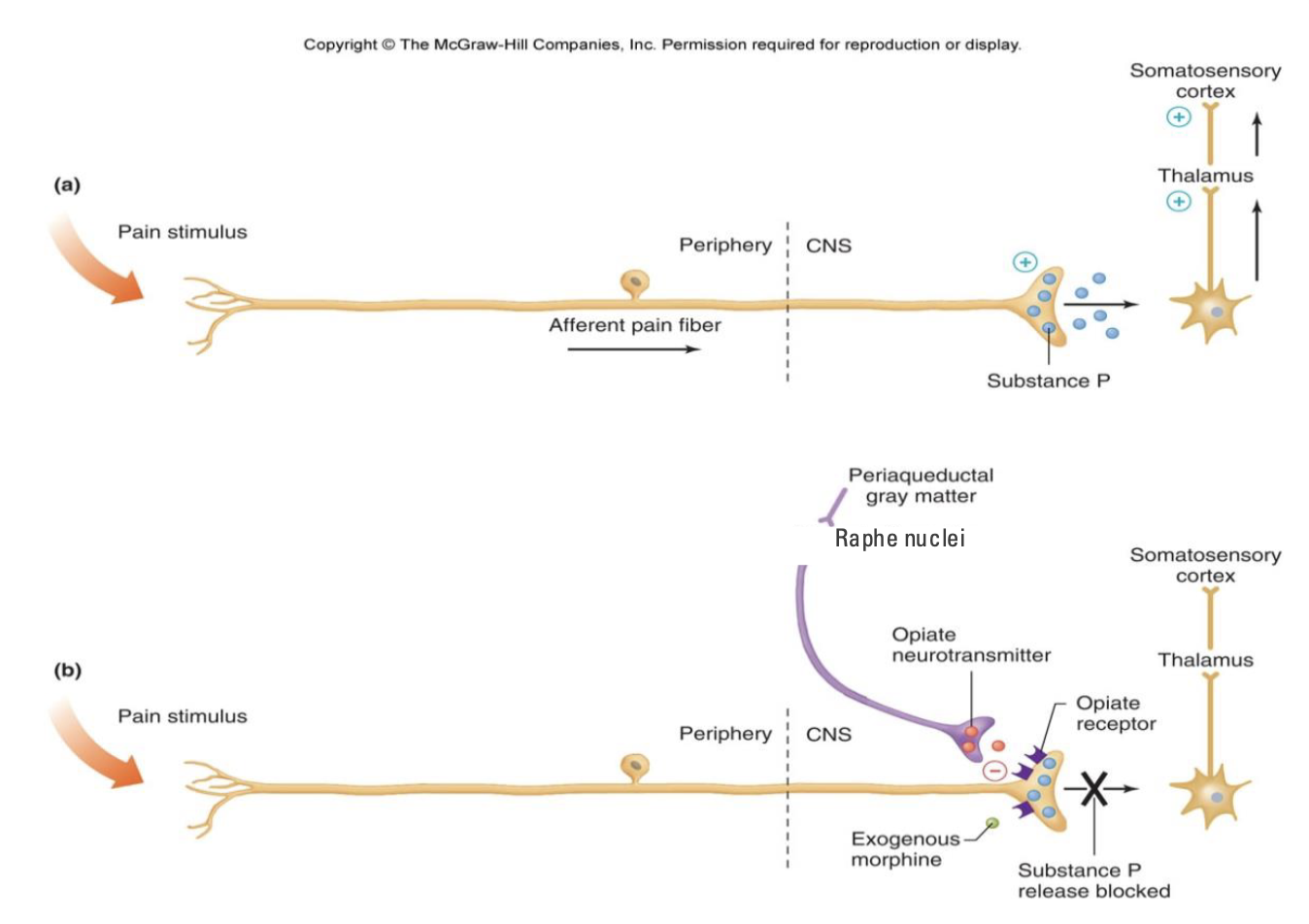
Pain Regulation - Descending Regulation
Brain can do powerful things when it comes to controlling pain!
Strong emotion, stress, etc. can suppress pain
Periaqueductal gray matter (PAG) - in medulla
Receives input from many areas in cortex (often emotional)
Neurons descend to medulla (Raphe nuclei)
Neurons descend to spinal cord to depress activity
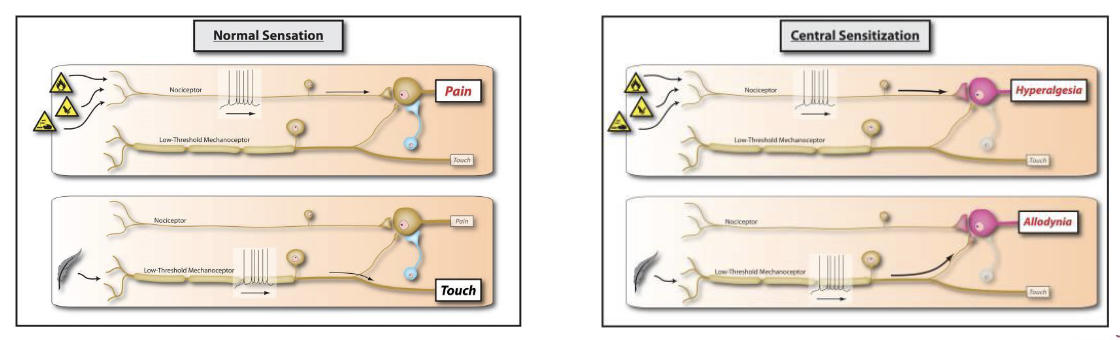
Hyperalgesia
Reduction in the pain threshold, increased sensitivity, or spontaneous pain
Primary Hyperalgesia: super-sensitivity within the damaged area
Secondary Hyperalgesia: super-sensitivity in the surrounding area
Primary changes occur peripherally:
Inflammation = bodies attempt to eliminate injury and stimulate healing
A variety of neurotransmitters, peptides, lipids, etc. are released which can attach to receptors in/around injury to lower their threshold for activation
Hyperalgesia vs. Allodynia:
Allodynia is a similar concept, but pain response from stimuli that would normally not cause pain
Central Sensitization
Amplification of neural signaling (e.g., nociceptive information) within the CNS that elicits pain hypersensitivity or even normal stimuli (allodynia)
Changes in the synapses and potentially the organization of interconnecting neurons may increase excitability/reducing inhibition of pain pathways
Contributions are difficult to identify and treatments difficult to target
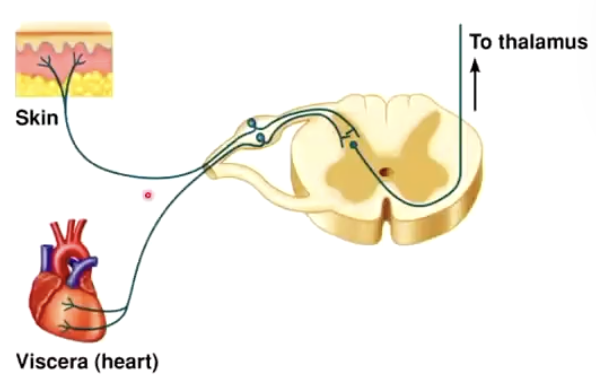
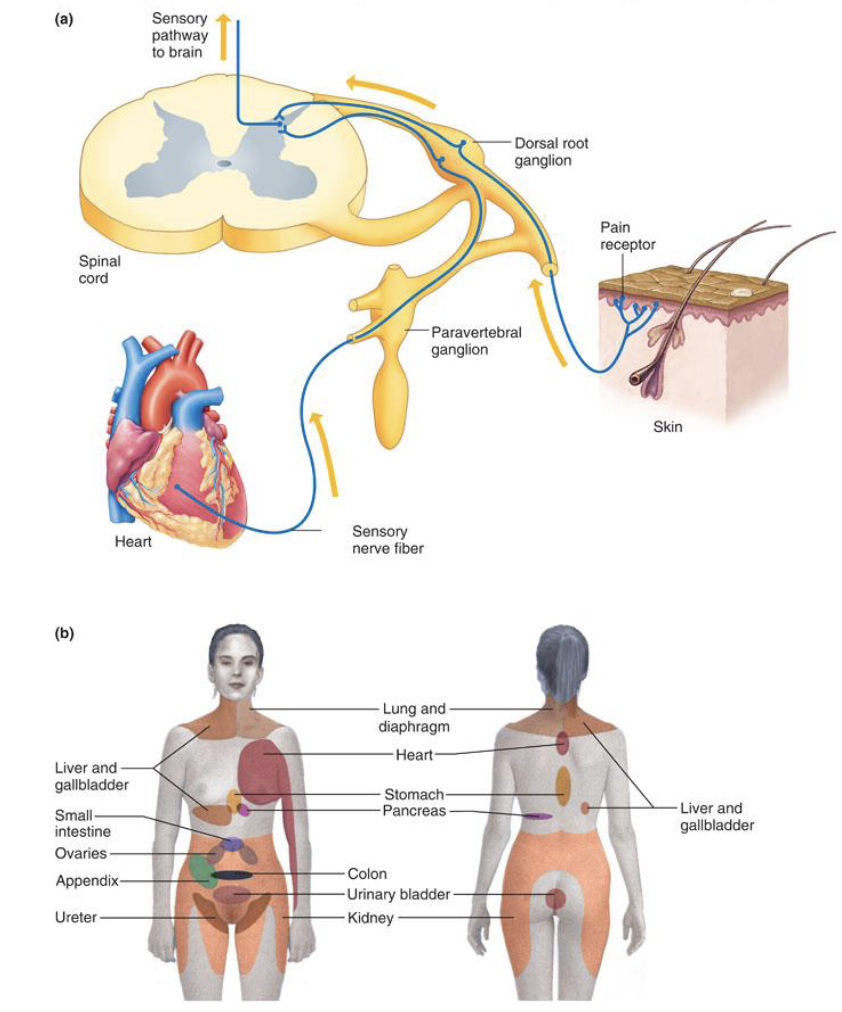
What is referred pain?
Cross-talk between sensory neurons
Convergence of visceral and somatic afferent neurons (in dorsal root ganglion)
Ex: Chest and left arm pain before heart-attack
Issue here?
In STT, the signal should synapse, then cross over and go up to the brain
More accurate diagram:
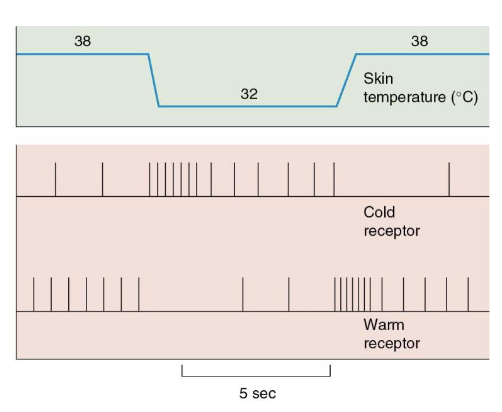
What is temperature?
Thermoreceptors
Varying sensitivities to hot and cold temperatures
Cold (Aδ & C fibers) and hot (C fibers)
Adapt to long durations of stimuli
Follow the same pathway as pain
What is proprioception?
Our perception of the location and movement of our body
Allows us to control limb and joint position for optimal movement
Group I neurons
Two primary receptors:
Muscle spindle – amount of stretch in a muscle
Golgi tendon organ – amount of force
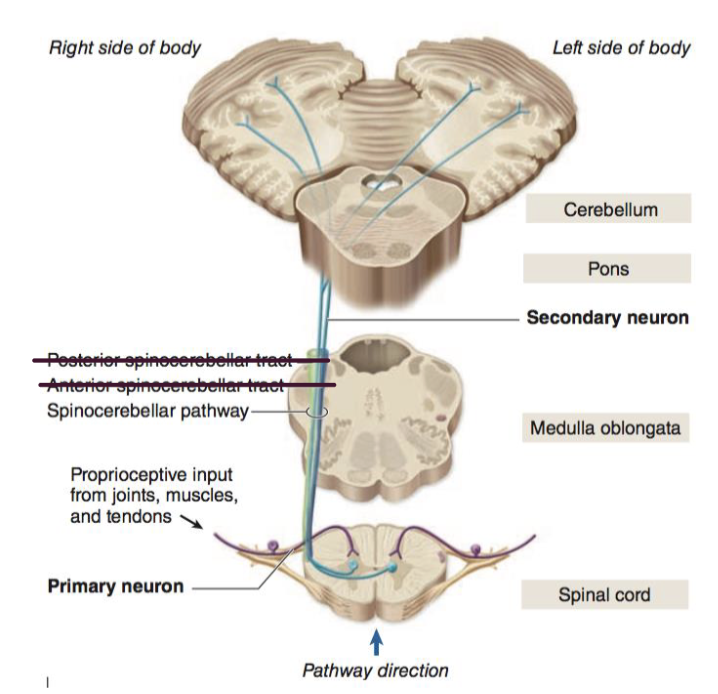
Conscious vs. Unconscious proprioception
Conscious proprioceptive information
Dorsal column medial lemniscus pathway
Unconscious proprioceptive information
Spinocerebellar tracts – To cerebellum
Spinal interneurons – Spinal reflexes
While holding a dime for a period of time between your fingers, you are able to feel the contours along the edge. The most important receptor for this type of sensory information is the...
A. Messner’s corpuscle
B. Merkel’s disk
C. Pacinian corpuscle
D. Ruffini’s endings
B. Merkel’s disk
You stub your right toe on your bedpost and the free nerve endings immediately send nociceptive information to the brain through the spinothalamic tract. What side of the body (spinal cord/brain) will this information be when it: i) is ascending the spinal cord at the level of thecervical spine, ii) reaches the brain.
A. i) left, ii) left
B. i) left, ii) right
C. i) right, ii) right
D. i) right, ii) left
A. i) left, ii) left
Which of the following statements is NOT true about the dorsal column medial lemniscal pathway?
A. The body of the second order neuron is found within medulla
B. It contains 3 neurons (first, second, and third order)
C. Decussation occurs immediately after the axon enters the spinal cord
D. The body of the first order neuron is within the dorsal root ganglion
C. Decussation occurs immediately after the axon enters the spinal cord