T5 - IE3 - Pulmonology - Ostrom - Pathophysiology and Pharmacology of Chronic Obstructive Pulmonary Disease (COPD)
1/172
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
173 Terms
Asthma vs. COPD Chart
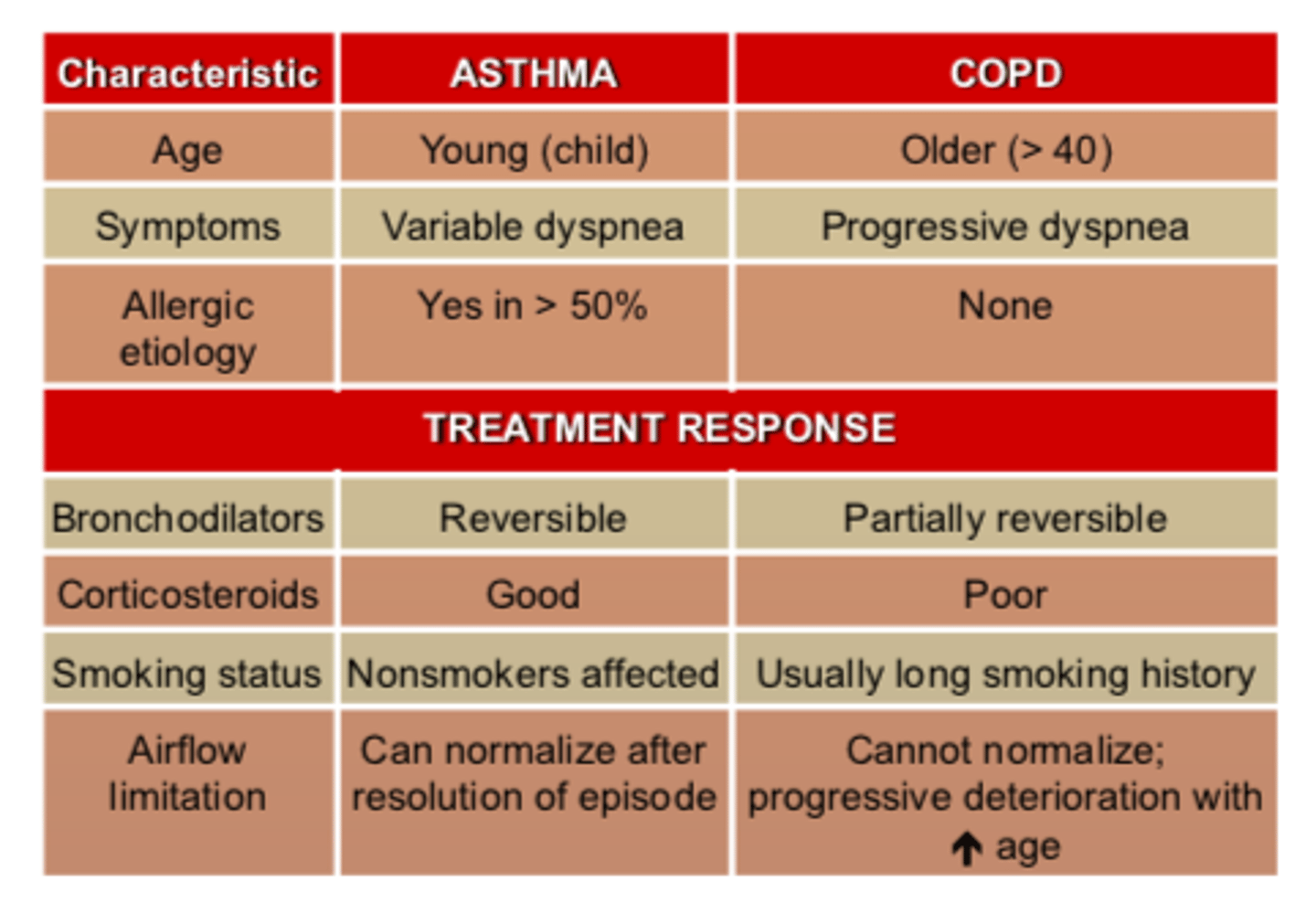
Asthma vs. COPD - treatment response: bronchodilators
Asthma: reversible
COPD: partially reversible
Asthma vs. COPD - treatment response: corticosteroids
Asthma: good
COPD: poor
Asthma vs. COPD - smoking status
Asthma: non-smokers affected
COPD: usually long smoking history
Asthma vs. COPD airway inflammation
Asthma: can normalize after resolution of each episode
COPD: cannot normalize - progressive deterioration with INCREASED age
In COPD - airway inflammation can ______ ____________, there is ____________ deterioration with increased age
- NOT normalize
- progressive (deterioration)
In COPD - airway inflammation: can NOT normalize, there is progressive ____________ with _________ age
- (progressive) deterioration
- INCREASED (age)
Asthma vs. COPD: Asthma is most often diagnosed in __________ or __________, while COPD is diagnosed ______ in life.
- childhood
- adolescence
- later (in life)
Asthma vs. COPD - smoking: Nearly all patients with COPD either _______ smoked or have a significant _____________ ________ ______ exposure, while asthma patients are more commonly non-smokers.
- (either) HAVE (smoked)
- (significant) environmental tobacco smoke (exposure)
Asthma vs. COPD - trigger signs: In general, asthma is acutely worsened by exposure to allergens, cold air and exercise.
COPD flare-ups are largely caused by _________ _______ ______ like pneumonia and influenza. COPD can also be made worse from exposure to ____________ _________.
- respiratory tract infections
- (exposure to) environmental pollutants
Asthma vs. COPD - trigger signs:
In general, asthma is acutely worsened by exposure to allergens, cold air and exercise.
COPD flare-ups are largely caused by respiratory tract infections like __________ and __________. COPD can also be made worse from exposure to environmental pollutants.
- pneumonia
- influenza
Asthma vs. COPD - trigger signs:
In general, asthma is acutely worsened by exposure to __________, ______ _____ and _________.
COPD flare-ups are largely caused by respiratory tract infections like pneumonia and influenza. COPD can also be made worse from exposure to environmental pollutants.
- allergens
- cold air
- exercise
Asthma vs. COPD - Treatment Goals: Different for each diseases. Asthma is treated to suppress __________ _________, whereas COPD is treated to reduce symptoms. Asthma pathology is ________, COPD is not.
- (to suppress) chronic inflammation
- reversible
Asthma vs. COPD - Treatment Goals: Different for each diseases. Asthma is treated to suppress chronic inflammation, whereas COPD is treated to __________ symptoms. Asthma pathology is reversible, COPD is _____ __________.
- reduce (symptoms)
- not reversible
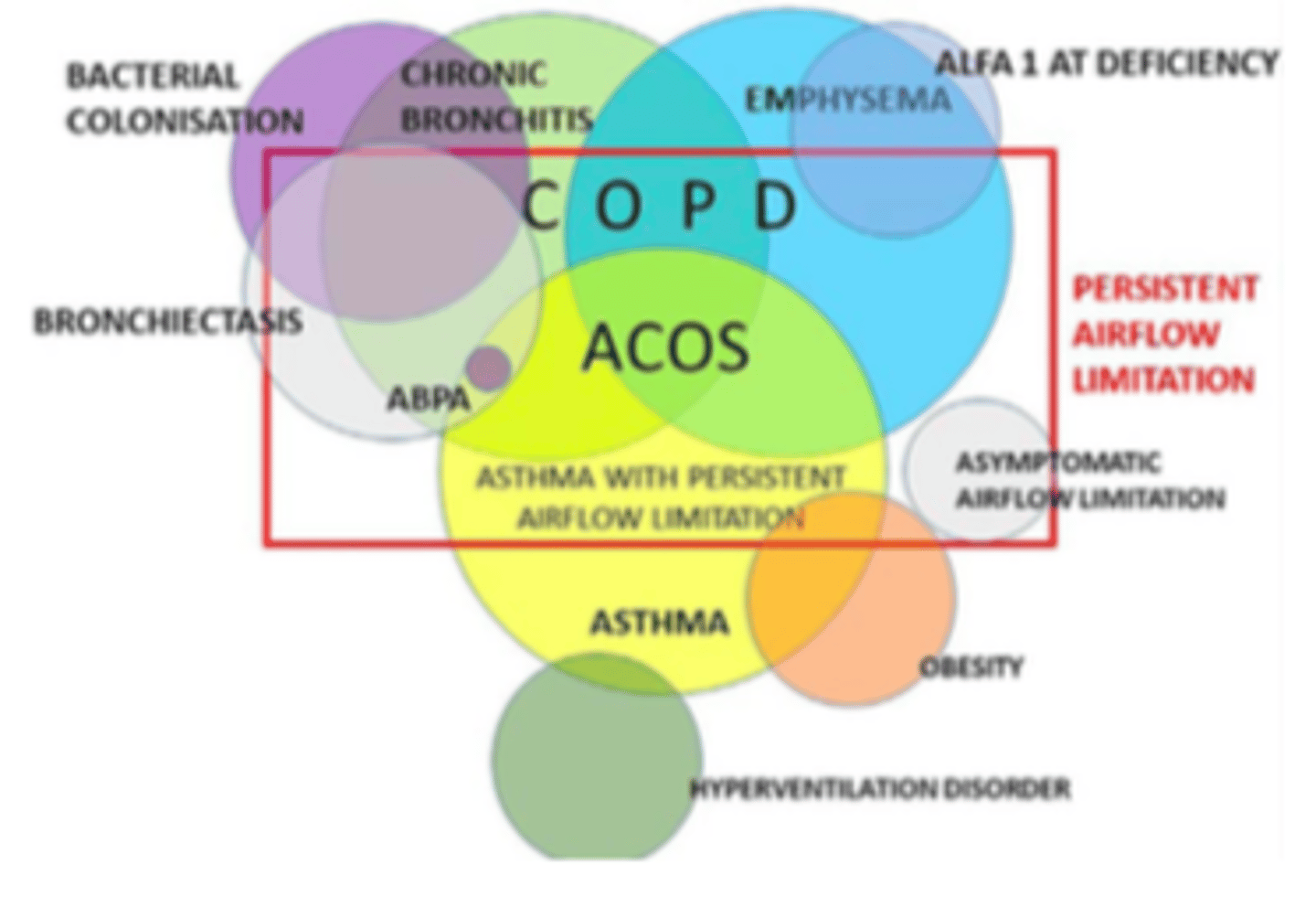
ACOS
asthma-COPD overlap symdrome
Asthma-COPD Overlap Syndrome (ACOS): is a ____ of both diseases; ________ ________ than either alone, so more _________ therapy needed
- mix (of both)
- more serious (than either alone)
- aggressive (therapy needed)
ACOS is still poorly understood
Asthma-COPD Overlap Syndrome (ACOS): still _________ understood, diagnosis is still __________
- poorly (understood)
- (still) evolving
Asthma-COPD Overlap Syndrome (ACOS) diagram
COPD Pathophysiology - Progressive ____ of airflow in lungs resulting in ______________ that is not fully reversible. Primarily caused by chronic inflammation.
- (Progressive) loss
- bronchoconstriction
COPD Pathophysiology - Progressive loss of _______ in lungs resulting in bronchoconstriction that is _____ _______ reversible. Primarily caused by ________ inflammation.
- airflow (in lungs)
- not fully (reversible)
- chronic (inflammation)
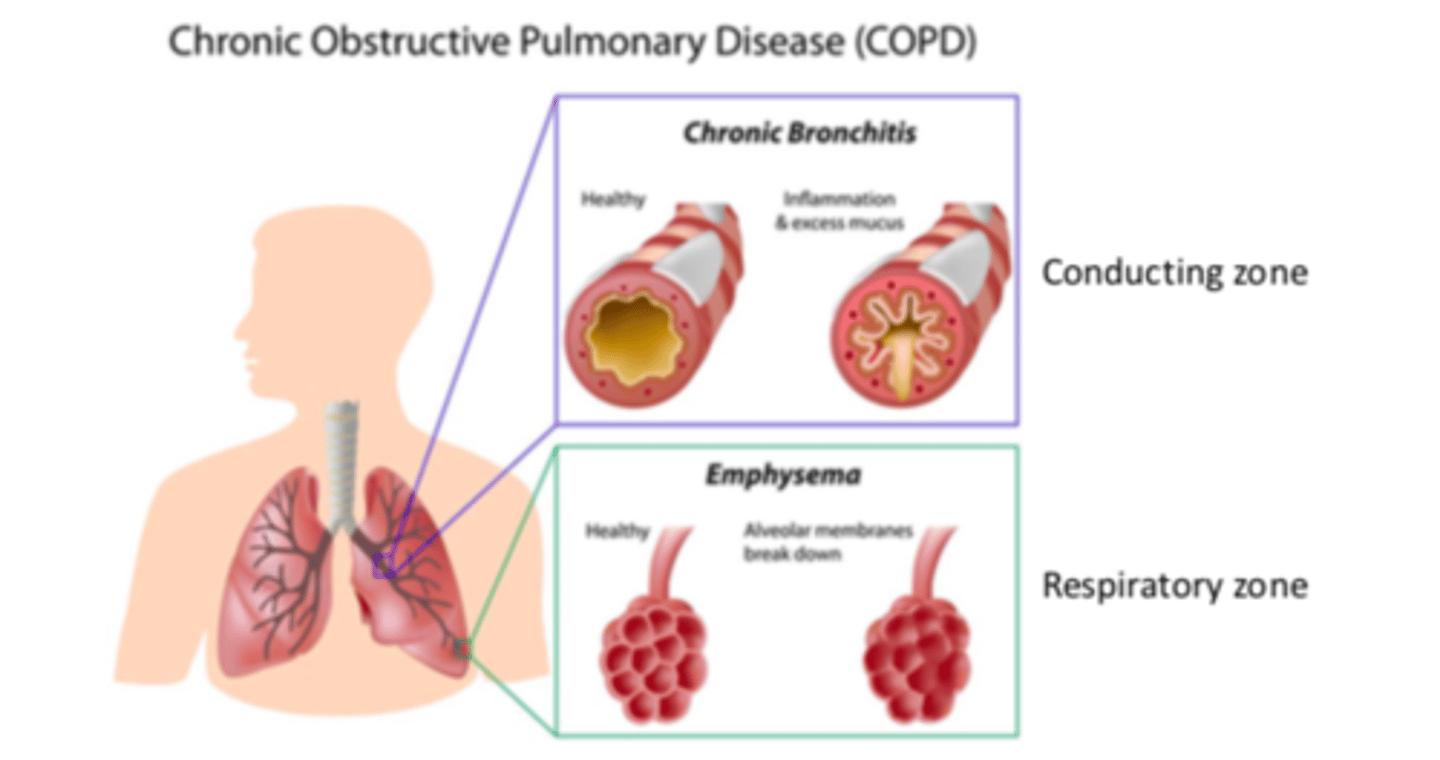
COPD Pathophysiology - two common forms
Bronchitis
Emphysema
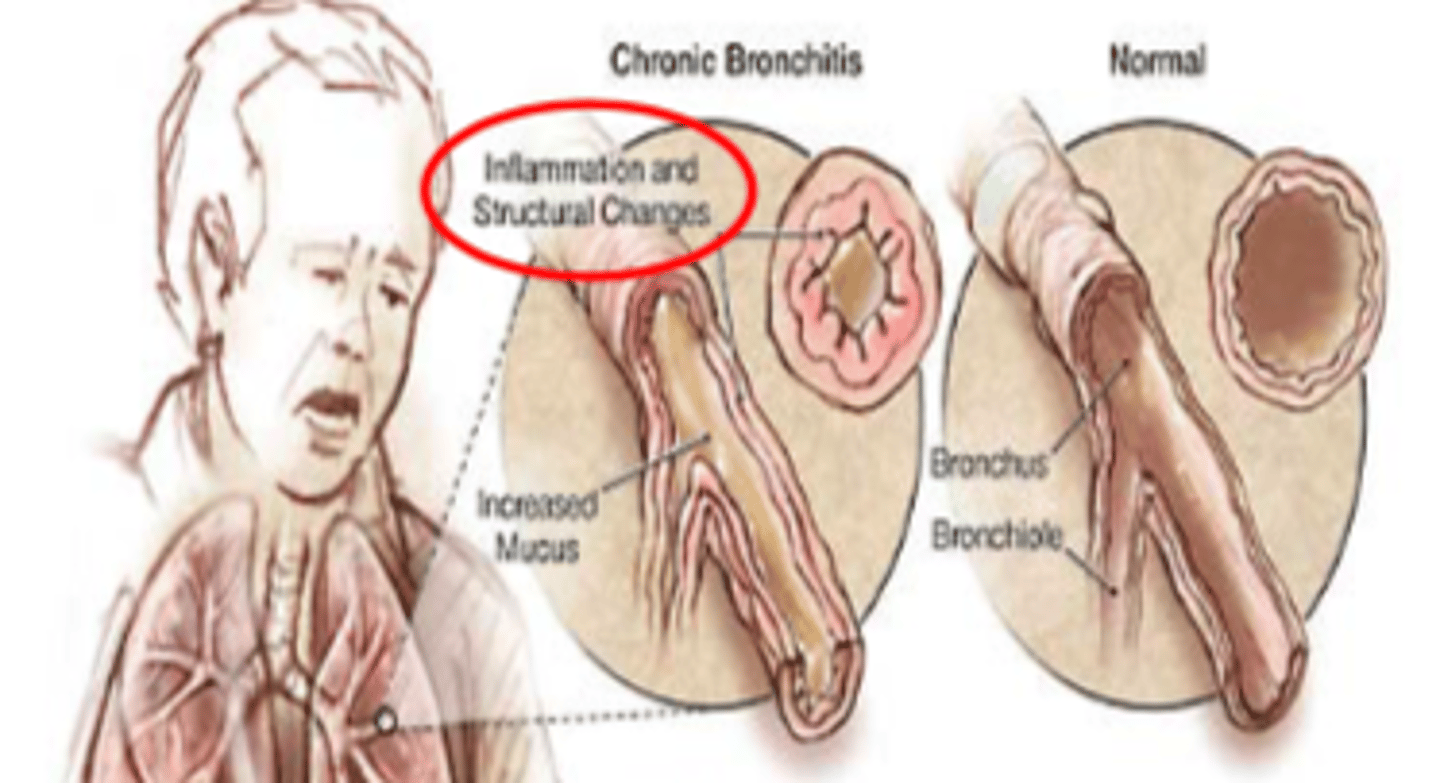
COPD Pathophysiology - two common forms: bronchitis
fixed obstruction of airways
- inflammation
- mucus production
conducting zone blocked
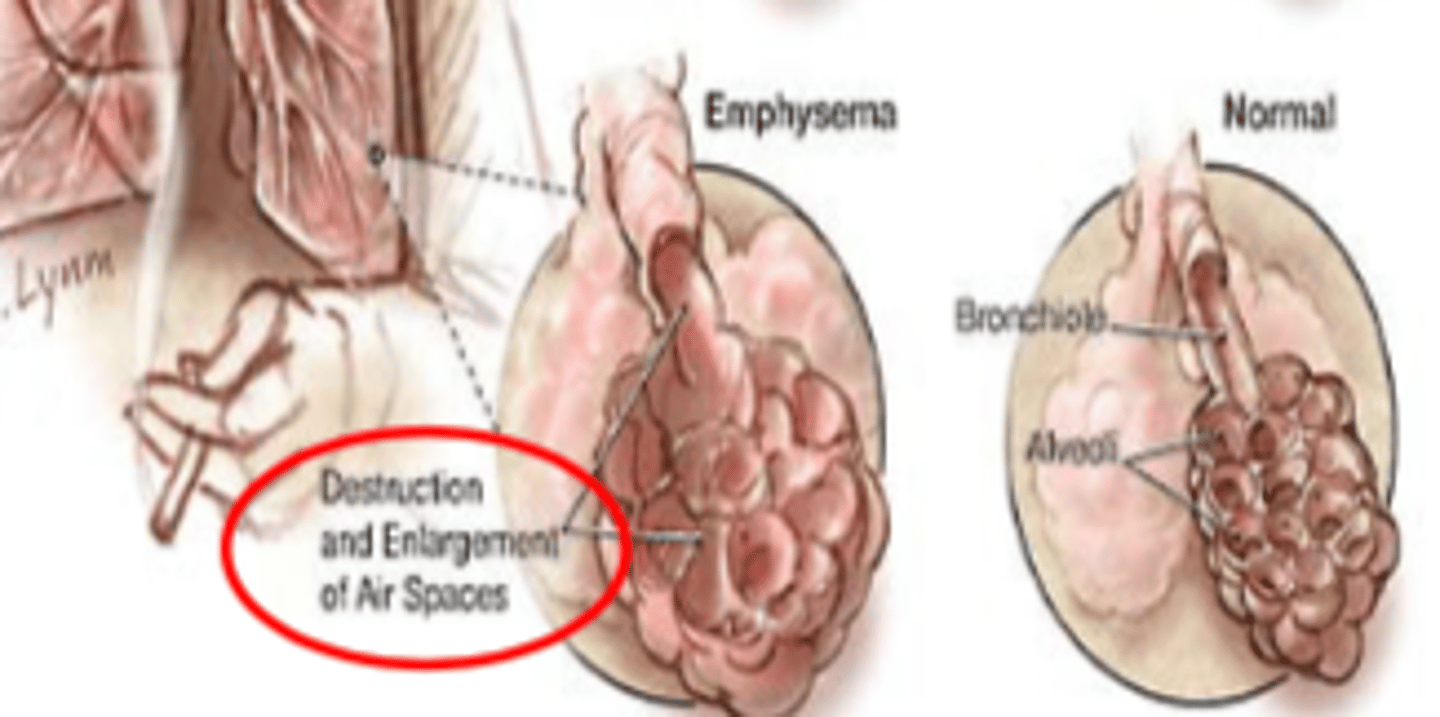
COPD Pathophysiology - two common forms: emphysema
destruction of alveolar architecture
loss of respiratory zone
COPD - bronchitis: _________ ______ of airways
- fixed obstruction (of airways)
Inflammation and/or mucus production
COPD - bronchitis: fixed obstruction of airways from the results of ___________ and/or _________ production
- inflammation
- (and/or) mucus (production)
COPD - emphysema: __________ of alveolar architecture
- destruction (of alveolar architecture)
Loss of respiratory zone
COPD - bronchitis: _____________ zone is blocked
- Conducting (zone)
COPD - emphysema: loss of __________ zone
- respiratory (zone)
Destruction and enlargement of air spaces
COPD - emphysema: __________ and ________ of air spaces
- destruction
- enlargement (of air spaces)
COPD - emphysema vs. normal lungs figure
COPD - chronic bronchitis: ___________ and ____________ changes
- inflammation
- structural (changes)
COPD - chronic bronchitis vs. normal lungs figure
COPD - Chronic Bronchitis and Emphysema Zone Figure
COPD Molecular / Cellular Pathophysiology Pathway Figure
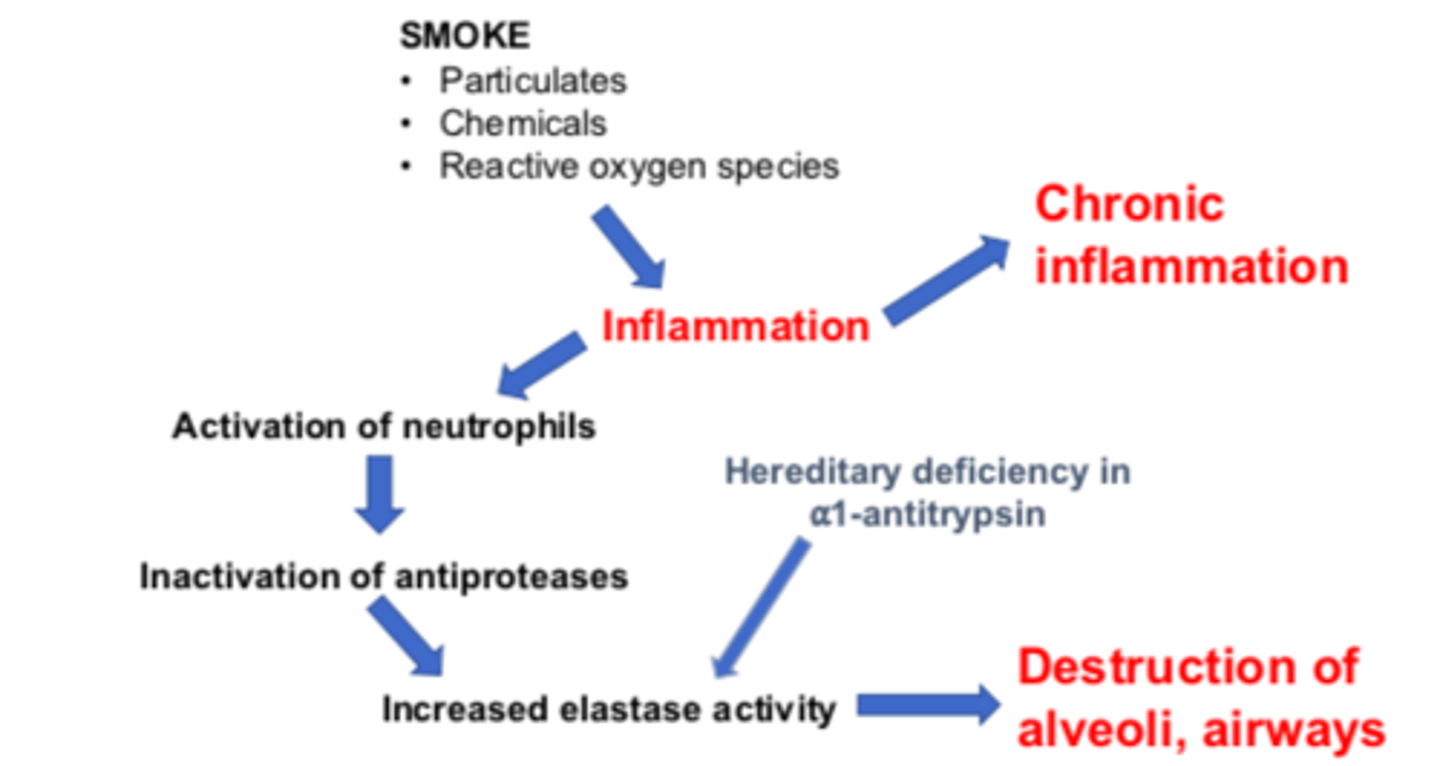
COPD Molecular / Cellular Pathophysiology Pathway: smoke exposure
particulates
chemicals
reactive oxygen species
These lead to inflammation and progress to chronic inflammation
COPD Molecular / Cellular Pathophysiology Pathway:
Step 1: smoke exposure (particulates, chemicals, reactive oxygen species) leads to ___________
- (leads to) inflammation
Step 2: Inflammation will lead to chronic inflammation and activation of neutrophils.
COPD Molecular / Cellular Pathophysiology Pathway:
Step 1: smoke exposure (particulates, chemicals, reactive oxygen species) leads to inflammation
Step 2: Inflammation will lead to ________ __________ and activation of _________.
- chronic inflammation
- (and activation of) neutrophils
Activation of neutrophils lead to inactivation of antiproteases
COPD Molecular / Cellular Pathophysiology Pathway:
Step 2: Inflammation will lead to chronic inflammation and activation of neutrophils.
Step 3: Activation of neutrophils lead to ___________ of antiproteases
- inactivation (of antiproteases)
HDAC
Histone deacetylase.
Histone deactylase (HDACs)
An enzyme that removes acetyl groups from a histone tail, allowing histones to wrap the DNA more tightly promoting repression of gene transcription.
COPD Molecular / Cellular Pathophysiology Pathway:
Step 2: Inflammation will lead to chronic inflammation and activation of neutrophils.
Step 3: Activation of neutrophils lead to inactivation of ____________
- (inactivation of) antiproteases
Step 4: Inactivation of antiproteases cause increased elastase activity
COPD Molecular / Cellular Pathophysiology Pathway:
Step 3: Activation of neutrophils lead to inactivation of antiproteases
Step 4: Inactivation of antiproteases cause ___________ __________ activity
- increased elastase (activity)
This leads to destruction of alveoli, airways
COPD Molecular / Cellular Pathophysiology Pathway:
Step 4: Inactivation of antiproteases cause INCREASED elastase activity.
Hereditary deficiency of ___-_________ also causes INCREASED elastase activity
Step 5: Increased elastase activity causes DESTRUCTION of _________ and ____________
- α1-antitrypsin
- (causes DESTRUCTION of) alveoli
- airways
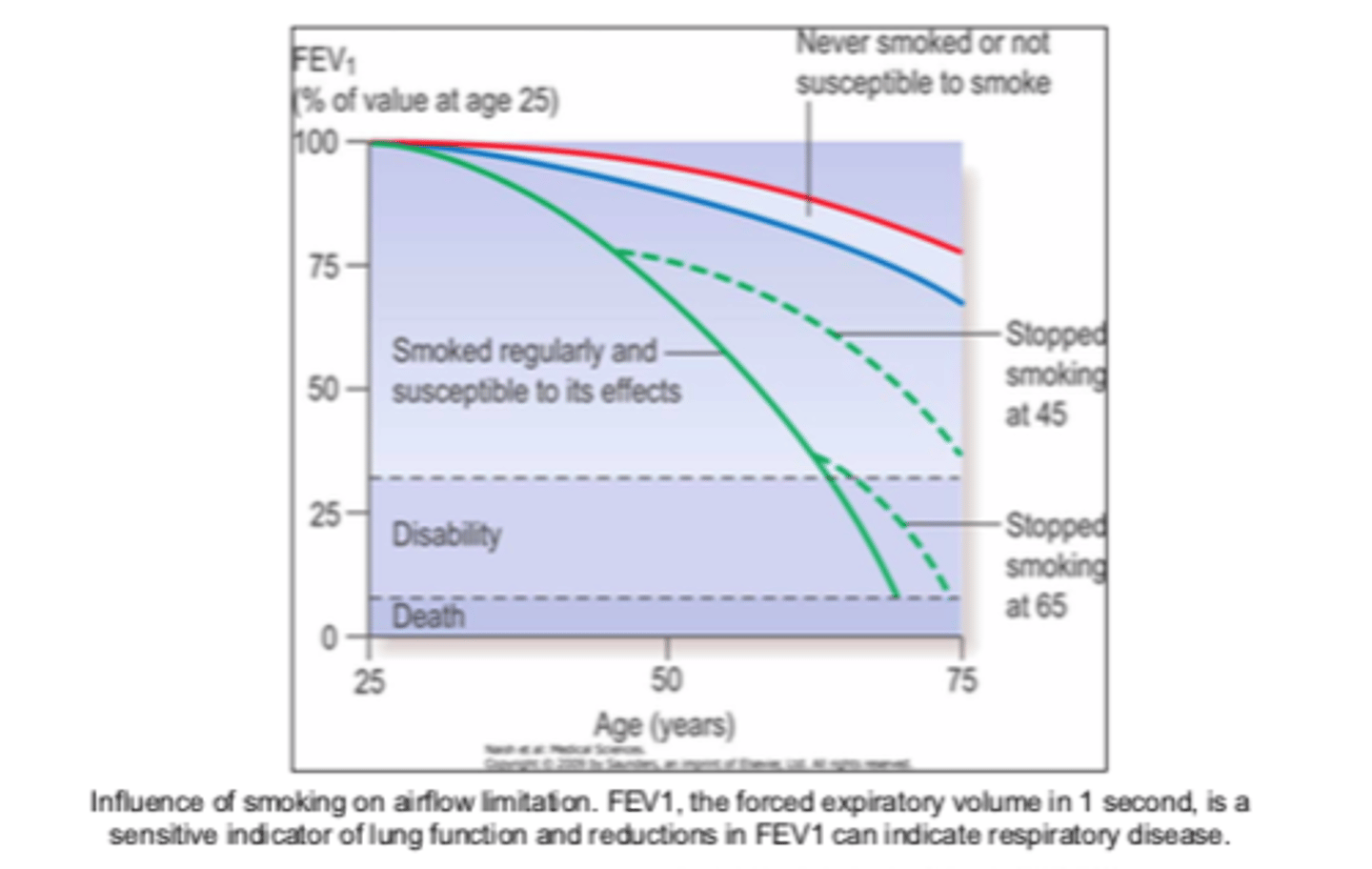
Smoking causes ________, but there is hope if you ________
- (causes) COPD
- (if you) quit
ALWAYs counsel on smoking cessation
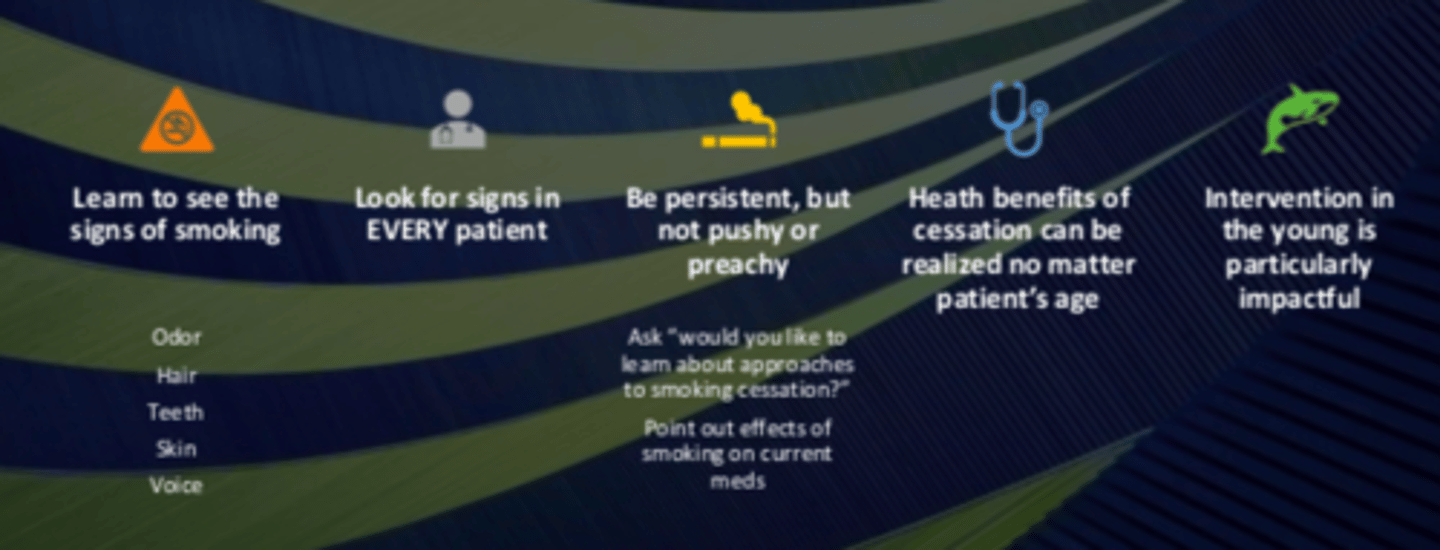
Promoting tobacco cessation: advise patient to ____ / _______ second-hand smoke
- quit / avoid (second-hand smoke)
Promoting tobacco cessation: assess patient's willingness to quit
Stages:
Pre-contemplation
Contemplation
Preparation
Action
Maintenance
Relapse
Try to move patients along one stage
Promoting tobacco cessation: if ready to quit
establish a quit date
provide self-help materials
offer nicotine replacement therapy and/or non-nicotine medications
Promoting tobacco cessation - if ready to quit: offer _______ ________ therapy and/or ___-________ medications
- nicotine replacement
- non-nicotine
Promoting tobacco cessation - if ready to quit: recommending a smoking cessation program
Combination of medications plus a smoking cessation program is more effective than either alone
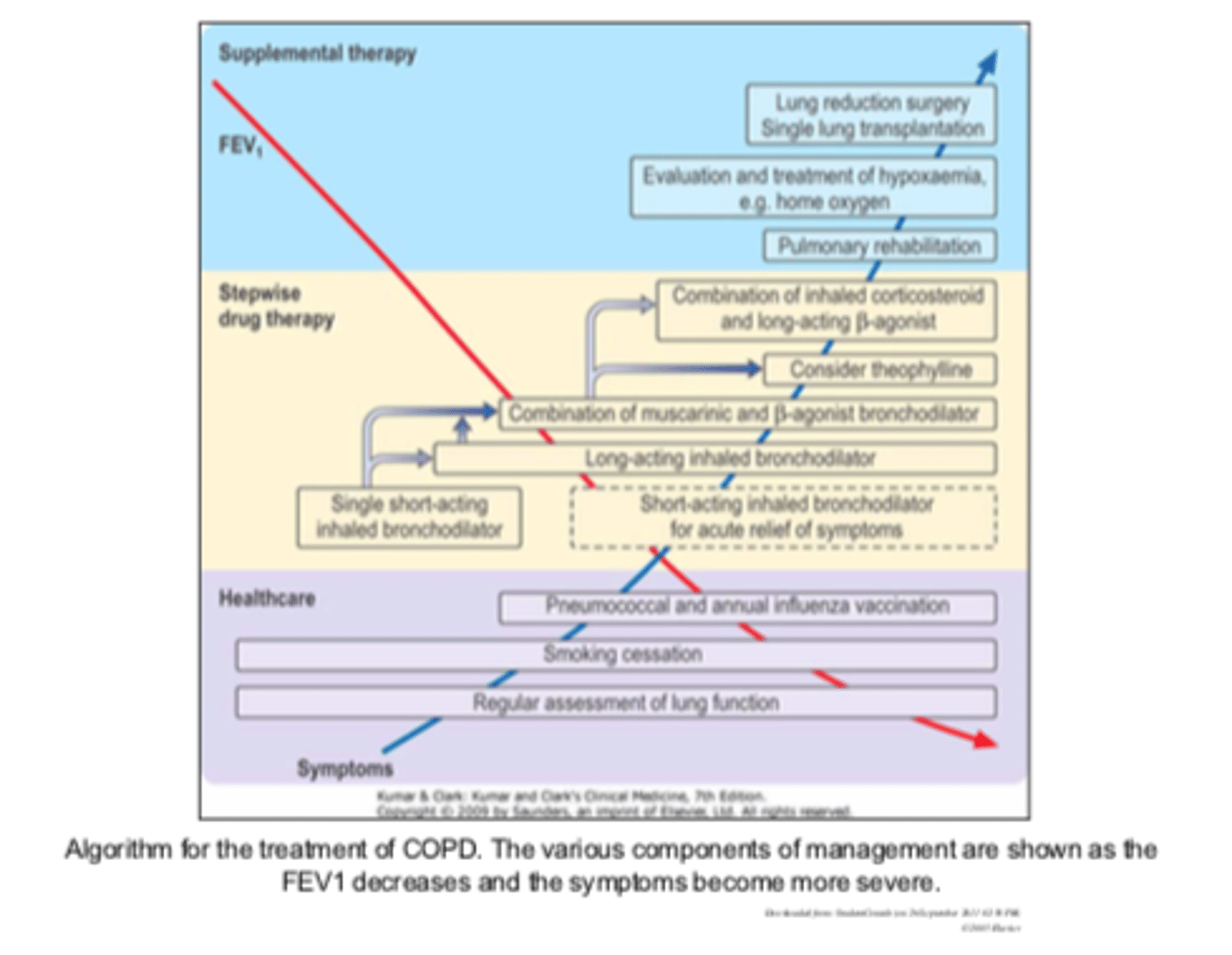
Algorithm for the treatment chart
Long Acting Inhaled Anticholinergics: improved selectivity through __________ application by ________ or _______ inhalation
- topical (application)
- nasal
- oral (inhalation)
Long Acting Inhaled Anticholinergics: __________ systemic adverse effects with recommended dosing regimen
- minimal (systemic adverse effects)
Increased risk of urinary retention, especially with BPH
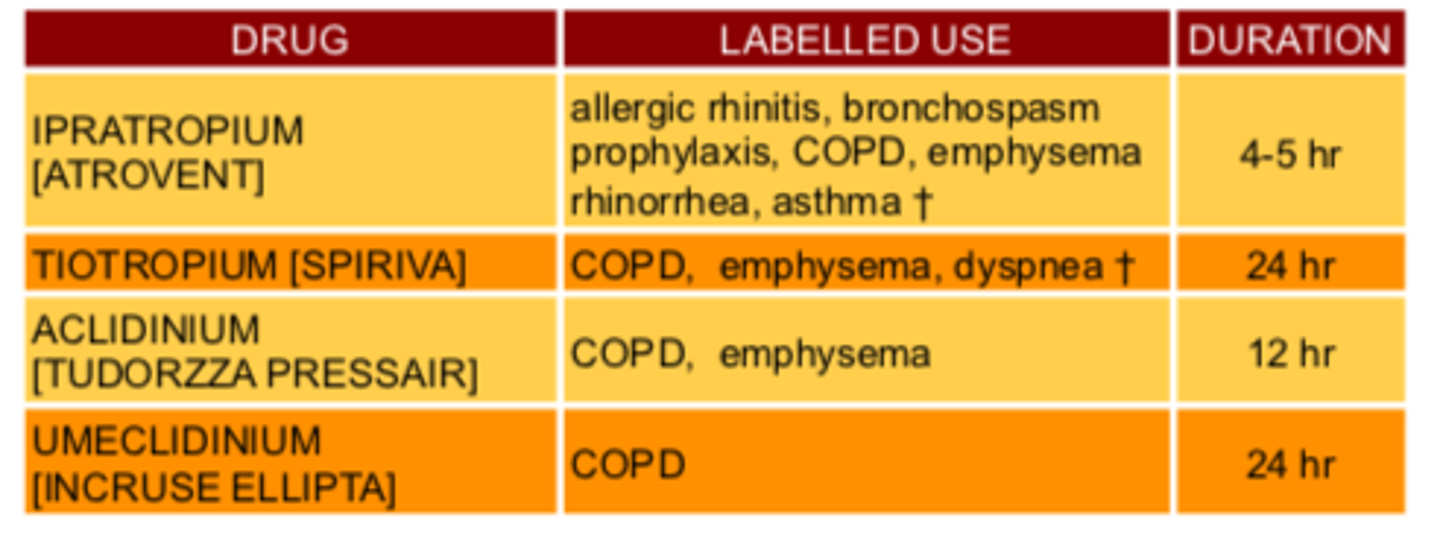
Long Acting Inhaled Anticholinergics Drugs
Ipatropium
Tiotropium
Aclidinium
Umeclidinium
Ipatropium
ATROVENT
ATROVENT
ipatropium
tiotropium
SPIRIVA
aclidinium
TUDORZZA PRESSAIR
TUDORZZA PRESSAIR
aclidinium
umeclidinium
INCRUSE ELLIPTA
INCRUSE ELLIPTA
umeclidinium
Long Acting Inhaled Anticholinergics Chart
Counseling - anticholinergics: avoid activities requiring ________ alertness or __________ until drug effects are ____________
- mental (alertness)
- coordination
- realized
May cause dizziness, mydriasis, and blurred vision
Counseling - anticholinergics: may cause _________, __________, and _________ vision
- dizziness
- mydriasis
- blurred (vision)
Avoid medication contact with eyes
Counseling - anticholinergics: Inhalation form may cause...
headaches
dry mouth
respiratory tract infections (including bronchitis)
urinary retention,
urinary tract infections
sinusitis
Counseling - anticholinergics: Report symptoms of ___________ (anaphylaxis, rash, angioedema, urticaria), eye pain, blurred vision, excessively dry nasal passages, or nose bleeds
- hypersensitivity
Counseling - anticholinergics: advise patient on proper _________ technique, depending on __________ ______
- inhalation (technique)
- delivery device
SABAs for bronchodilation drugs
albuterol (VENTOLIN)
levalbuterol (XOPENEX)
pirbuterol (MAXAIR)
terbutaline
SABAs for bronchodilation: "____________" with _____ onset-intermediate duration
- "relievers"
- quick (onset-intermediate)
~6 hour
SABAs for bronchodilation: _________ smooth muscle
- relax (smooth muscle)
Stabilize mast cells preventing histamine release in response to allergen
SABAs for bronchodilation: stabilize ______ _______ preventing ___________ release in response to allergen
- (stabilize) mast cells
- histamine (release)
SABAs for bronchodilation: _________ route preferred
- inhaled (route preferred)
Also given PO, SC, IV
SABAs for bronchodilation - side effects
N/V
headache
Increased BP, HR
Arrhythmias
Convulsions
Coma
Respiratory & Vasomotor Collapse
Tremor via β2 receptors in skeletal muscle
Short-lived hyperglycemia
SABAs for bronchodilation: routine monitoring of ____________ function
- pulmonary (function)
LABA drugs for maintenance
Salmeterol (SEREVENT)
Formoterol (FORADIL)
Indacaterol (ARCAPTA NEOHALER)
salmeterol
SEREVENT
SEREVENT
salmeterol
formoterol
FORADIL
FORADIL
formoterol
LABAs for maintenance: ___________ _______ onset-long duration
- "preventers" slower (onset)
12+ hour duration
LABAs for maintenance: used for ____________ or _________-________ asthma
- nighttime
- exercise-induced (asthma)
Usually prescribed for 2x daily administration
LABAs for maintenance: usually prescribed for _____ daily administration
- 2x (daily administration)
Aerosol or powder
Counseling: β2AR Agonists - warn patient to report symptoms of ___________ _____________
- (symptoms of) paradoxical bronchospasm
Counseling: β2AR Agonists - instruct patent to report need for __________ _____ or _______ of drug to provide symptomatic relief
- increased frequency
- amounts (of drug)
Counseling: β2AR Agonists - advise patients to report symptoms of...
atrial fibrillation
supraventicular tachycardia
hypokalemia
Counseling: β2AR Agonists - side effects
Palpitations
Chest pain
Tremors
Headache
Dizziness
Nervousness
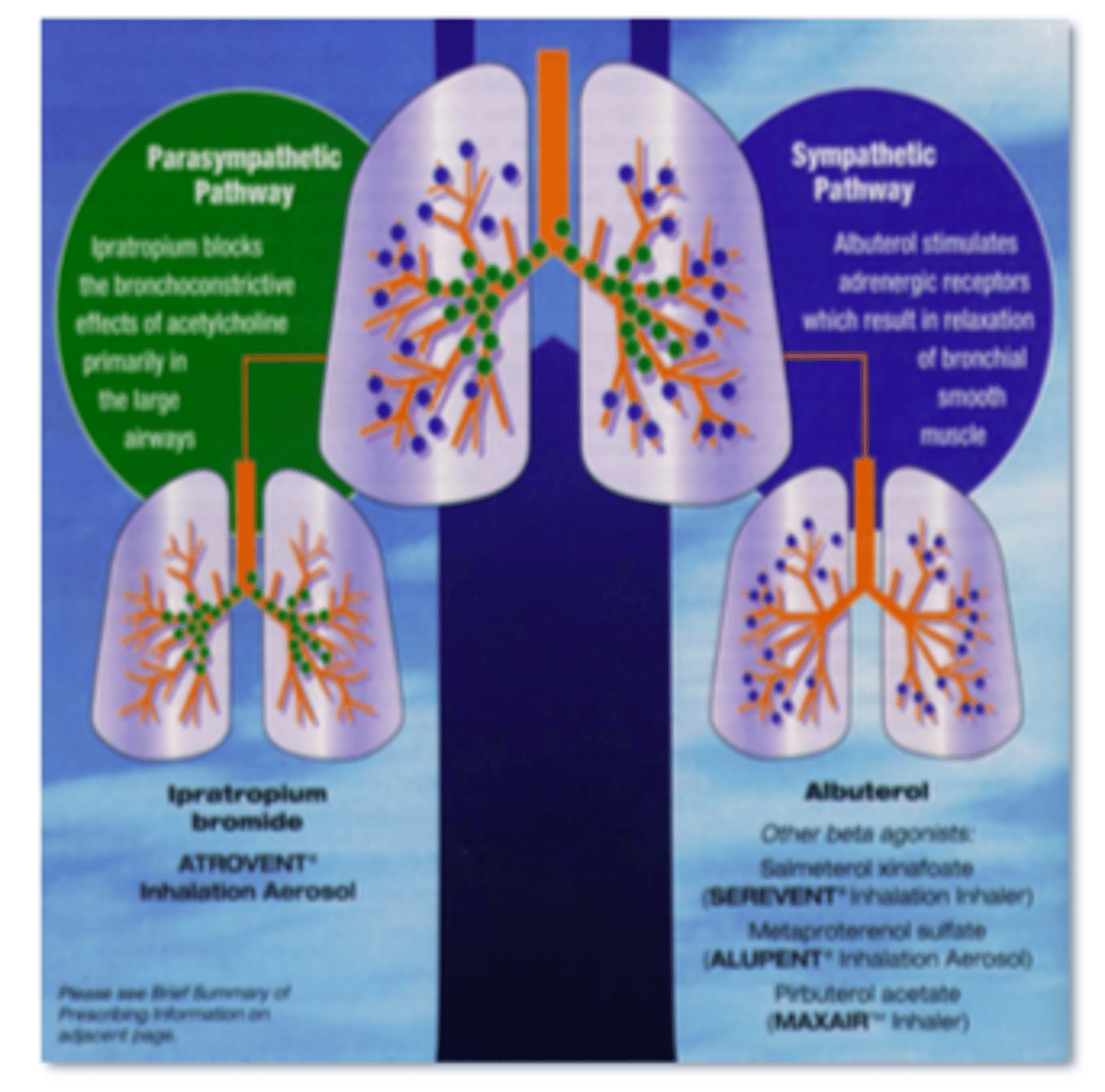
Combination LABA & Anticholinergic for COPD Figure
Parasympathetic: inhibits bronchoconstriction
Sympathetic: causes bronchodilation
ICS Corticosteroid Drugs
Beclomethasone dipropionate (BECLOVENT)
Budesonide (RHINOCORT)
Fluticasone propionate (FLOVENT)
Mometasone (NASONEX)
Ciclesonide (ALVESCO)
beclomethasone dipropionate
BECLOVENT
budesonide
RHINOCORT
fluticasone propionate
FLOVENT
ciclesonide
ALVESCO
ICS mono-therapy is _____ __________ for COPD
- NOT appropriate (for COPD)
Smokers can be resistant to _________________ therapy
- corticosteroid (therapy)
Oxidative / carbonyl stress from smoking may inhibit HDAC2 from unwinding thus increased inflammatory gene transcription and steroid resistance
Smokers: corticosteroid resistance
Oxidative / carbonyl stress from smoking may inhibit HDAC2 from unwinding thus increased inflammatory gene transcription and steroid resistance
Smokers - corticosteroid resistance: Oxidative / carbonyl stress from smoking may inhibit __________ from unwinding thus increased __________ gene transcription and steroid resistance
- HDAC2
- inflammatory (gene transcription)
This leads to inflammation in COPD
Combined corticosteroid & LABA drugs
Fluticasone / Salmeterol (ADVAIR DISCUS)
Budesonide / Formoterol (SYMBICORT)
Mometasone / Formeterol (DULERA)
fluticasone / Salmeterol
ADVAIR DISCUS
budesonide / formoterol
SYMBICORT
mometasone / formoterol
DULERA