Traumatic Brain Injury Epidemiology, Pathology, and Clincial Considerations
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
Why study brain injury
}Serious and debilitating injury that permanently affects individual’s lives.
}Affects the lives of family members and can cause patients and their families to experience daily changes in emotion
}grief, guilt, anger, blame, denial and hopefully acceptance/hope.
}Discrete therapies (PT, OT, SLP) often spend more time with patient than any discipline, aside from nursing
}Therapies play important role throughout continuum of care
Acquired brain injury
uThis “basket” term describes any trauma that occurs to the brain after birth.
uAlthough traumatic injury is one form of acquired brain injury, acquired brain injury also encompasses damage from disease processes including: tumors, stroke, infection, or substance disease.
uAcquired brain damage can also occur from anoxia – or lack of blood supply to deliver needed oxygen the brain.
Causes of (non-traumatic) ABI
uMalignancy
uBenign mass
uAnoxia/Hypoxia
uCommonly from allergic response, asphyxiation, secondary result of TBI
uInfections
uMeningitis
uEncephalitis
uCerebral Vascular Accidents
uHemorrhage
uAneurysm
Ingestion of toxins
Traumatic brain injury
uAn injury that affects how the brain works. It may be caused by a:
uBump, blow, or jolt to the head
uPenetrating injury (such as from a gunshot) to the head
Consequences of brain inury
uMotor Impairments
uSensory Impairments
uAutonomic Impairments
uCognitive Impairments
uPersonality and Behavioral Changes
uLifestyle Consequences
Motor impairments of BI
Orthopedic complications, decreases in strength, impaired functional mobility, poor coordination, balance impairments, problems with fine motor and hand function, impairments in speech, etc.
Sensory impairments of BI
Taste, touch, hearing, vision, smell
Autonomic impairments of BI
Arousal, awareness, sleep disturbances
Cognitive impairments of BI
Memory, attention, difficulty learning, problem solving, planning, judgment and safety awareness
Personality and behvioral changes of BI
Social and coping skills, frustration, anger, denial, reduced insight, disinhibition, impulsivity, apathy, anxiety, depression
Lifestyle consequences of BI
Loss of independence
Unemployment and financial hardship
Lack of transportation
Lack of leisure and recreation opportunities
Difficulty with interpersonal relationships
Loss of roles
Epidemiology
u1.4-1.7 million new TBIs each year in US
uHistorically 75-80% mTBI
u15-30% with residual symptoms
uFrequency of moderate TBI increasing (19% in 1992, 37% 2002)
uTBI is a contributing factor to a third (30.5%) of all injury-related deaths in the United States
u52,000 deaths per year, 70-90,000 with residual deficits
u6-12% prevalence in adult population
u426 of 7288 subjects found to have TBI (5.8%)
u3,044 of 25,134 subjects found to have TBI (12.1%)
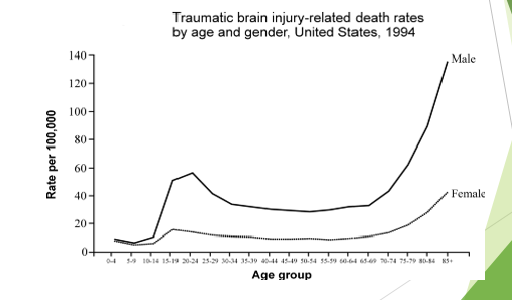
Risk factors and at-risk demographics
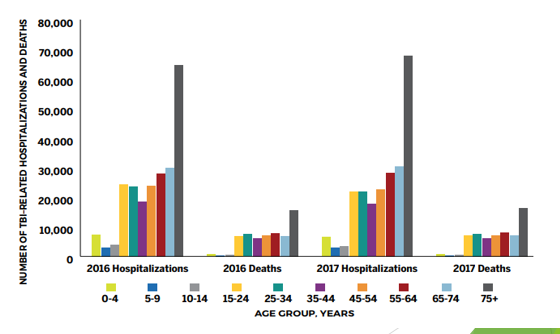
uThe very young (0-4 years old)
uThe very old
uAdolescent males
uLow health literacy
uLow SES
uAlcohol abuse + drug abuse
Estimated number of TBI hospitalizations by age
Risk factors and at-risk demographics
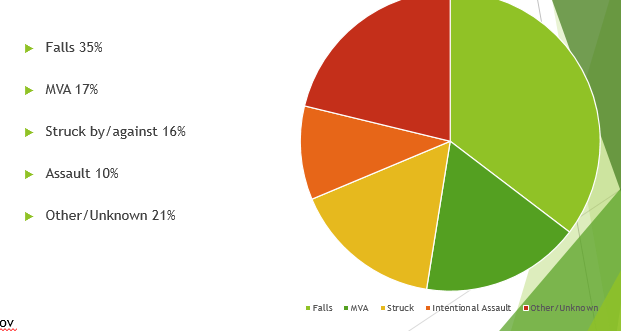
Etiology
u0-4 years: Up to 66% non-accidental trauma
u0-14 years: Up to 50% falls
u16-25 years: Up to 67% MVA
•26-35 years: Up to 50% MVA
•65+: Up to 60% falls
•85+: Up to 90% falls
TBI Cost
u2000 Census data
Direct costs of TBI: $9.22 billion/yr
Indirect costs (lost wages, productivity): $51.21 billion/yr
u2010 Census data
Combined direct/indirect costs: $76.5 billion
uSevere TBI accounts for nearly 90% of total TBI related costs
Primary injury
Closed head injury
Open head injury
Depressed skull fx
Compound skull fx
Basilar skull fx
Coup-Contrecoup injury
Intracranial pressure/elevated ICP
Brain herniations
Subarachnoid hemorrhage
Epidural hematoma
Subdural hematoma
Intraparenchymal hemorrhage
Diffuse axonal injury
Closed head injury
A closed head injury occurs when a person receives a traumatic blow to the head without a facture or displacement to the skull.
Closed head injuries are quite dangerous because secondary swelling occurs within the brain, either from edema or bleeding. Resulting compression causes further injury (secondary injuries).
Brain swelling may manifest by liquid or brain tissue swelling through any available openings, including the eye sockets.
This affects the cranial nerves controlling the eye muscles with resultant eye muscle impairment.
If Cranial Nerve III is compressed the pupil will appear dilated.
Medical personnel can initially assess intracranial pressure through pupil size.
ER personnel sometimes term this condition as a “blown pupil” (herniation or cranial compression).
Open head injury
}An open head injury occurs when an individual receives an impact from an outside force severe enough to cause to fracture or displace the skull.
}Positives: More room for swelling decreases risk of secondary compression injury
}Negatives: The brain is exposed and vulnerable to infections and/or further injury.
}If the skull is fractured or displaced, bone fragments from the skull can enter the brain and cause further injury.

Types of skull fx in open brain injury
Depressed skull fx
Compound skull fx
Basilar skull fx
Depressed skull fx
The broken piece of skull bone moves in towards the brain (open or closed head injury)
Compound skull fx
The scalp is cut and the skull is fractured
Basilar skull fx
The skull fracture is located at the base of the skull (neck area) and may include the opening at the base of the skull.
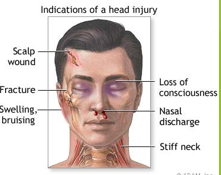
Patients may exhibit Raccoon eyes, or bruising around their eye orbits, or Battle’s sign – bruising behind the ears, or CSF leaking through the eyes and nose.
Why is brain injury so dangerous?
The brain is closed system with little room for edema uThe brain is a closed vault containing
ubrain tissue
ucerebral spinal fluid (CSF)
ublood supply.
uAny injury to the skull, brain tissue, arteries, or CSF causes cerebral swelling with accompanying blood pressure increases. This results in an increase in intracerebral pressure.
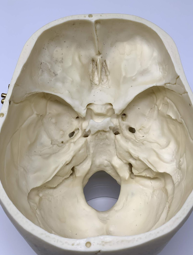
Skull landmarks
uThe base of the skull is rough, with many bony protuberances
uThese ridges can result in injury to the temporal and frontal lobes of the brain during rapid deceleration
udefinition: when the head slows or stops suddenly and the brain continues to move
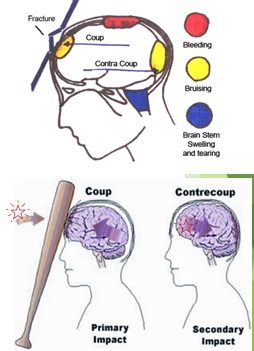
Coup-contrecoup injury
}Any blow to the skull causes damage to the brain at the site of the impact – COUP injury…
}…as well as damage to the brain due to “rebound” when the brain secondarily impacts the opposite side of the skull (CONTRE-COUP injury).
}This phenomenon occurs when the force impacting the head is not only great enough to cause damage at the site of impact, but also is able to move the brain severely enough that damage occurs to the opposite side of the brain as well.
Intracranial pressure
uNormal: 0 - 15 mmHg.
u>20mmHg usually gets intervention
u>25-30mmHg is fatal if prolonged, except in children, who can tolerate higher pressures for longer times.
uSustained leads to more brain damage
Be aware that when patients have higher levels of ICP, actions like coughing, agitation, or confusion can further raise their levels.
Often patients are placed into a medically induced and “therapeutic coma” to avoid this.
Sx of an elevated CP
uCranial nerve palsies
uHeadache with nausea/vomiting
uMental status changes
uConfusion, agitation, lethargy
uTherapists need to work closely with nurses and doctors in the ICU and notify the nurse in charge with any of these signs occur.
Fluids of the brain are
uNon-compressible so once pressure begins to build intracerebral pressure (ICP) increases rapidly. This is a life threatening problem!!
uHigher ICP leads to less cerebral perfusion or a lower CPP (cerebral perfusion pressure). This, in turn can cause more damage to brain tissue.
Normally, if the ____ _____ _____ _____, then cerebral vessels will ____, to maintain an even perfusion pressure
Systemic blood pressure rises
If the ____ _____ ____, then the vessels will _____ to allow better flow, with the same goal in mind
Systemic pressure falls
Dilate
uThese mechanisms often fail after brain injury.
uSome compensation occurs through blood & CSF moving from the brain into the spinal column; but too much pressure can lead to brain tissue herniation or a midline shift. This causes more brain damage!!
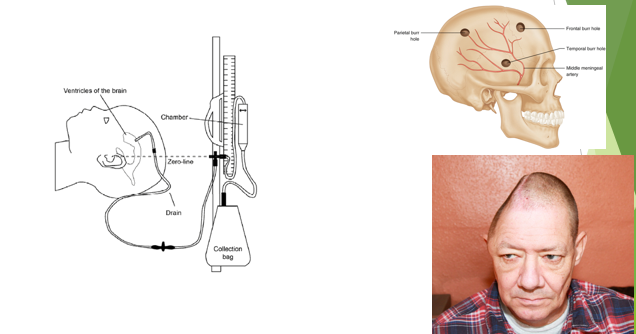
Intervention for elevated ICP
Midline shift and brain herniation
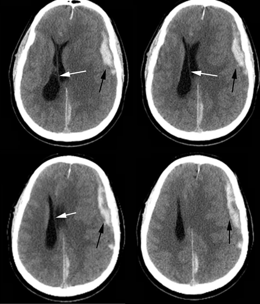
Where does the brain shifts
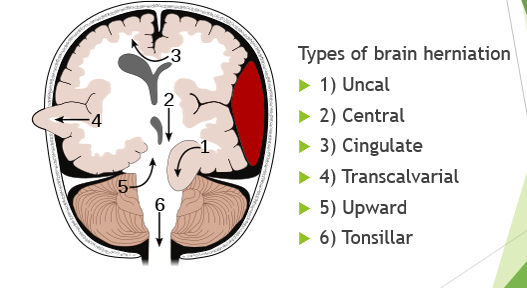
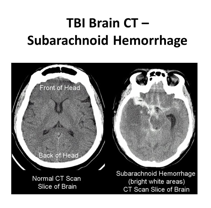
Subarachnoid hemorrhage
uMost frequent lesion in TBI
uBleeding into subarachnoid space
uBetween dura and pia mater
uTypically diffuse, but can be focal
uMultiple secondary effects with large SAH
Epidural hematoma
u= an accumulation of blood between the skull and the dural membrane.
uSeen in 2-4% of TBI
uBetween dura and skull
uMost commonly middle meningeal artery
uOverall mortality of 10%
<10% when treated early
Epidural hematoma fun facts
uTypically caused by a focused blow to the head with a blunt object like a baseball, hammer, or baseball bat.
uIn 85-95% of patients, this type of trauma is accompanied by an overlying fracture of the skull.
uBlood vessels in close proximity to the fracture are the sources of the hemorrhage.
uBecause the underlying brain is usually minimally injured, prognosis is excellent if treated quickly and aggressively.
uOutcome from surgical decompression and repair is related directly to patient's preoperative neurologic condition.
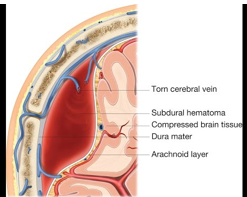
Subdural hematoma
uSeen in 12-29% of TBI
uCollection of blood between dura and arachnoid membrane
uTorn bridging veins
uMay be missed on initial imaging
Can form later
Symptoms often delayed
uMortality rate 40-60%
*If a patient develops sudden lethargy, confusion, headache, dizziness…tell medical team
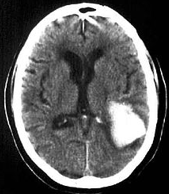
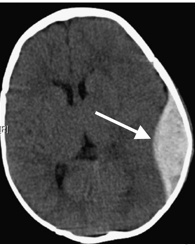
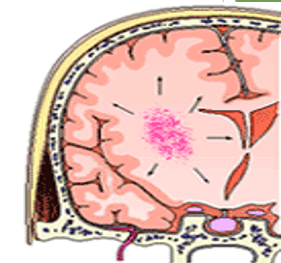
Intraparenchymal hemorrhage
uSevere contusion, laceration or penetrating injury
uFocal
uMay present as coup-contre coup
uSuborbital, anterior temporal lobe
uBlood pools in white matter of brain.
uBrain trauma can cause several severe IPHs, and can result in white matter shear injury—extensive loss of axons w/extensive brain injury.
uThis can cause diffuse axonal injury.
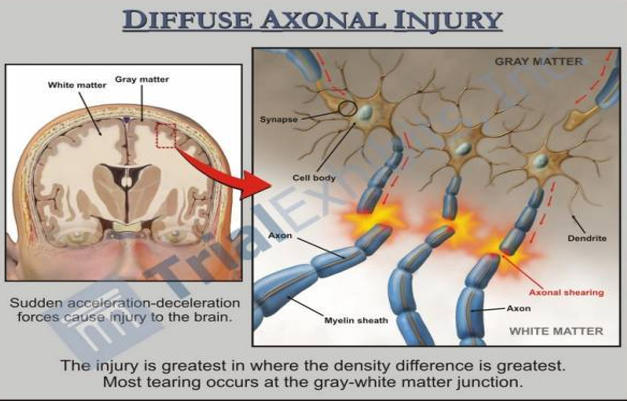
Diffuse axonal injury
uCan accompany any type of brain injury (open or closed), and is caused by the shaking/strong rotation of the head that occurs with impact
uDamage to the brain occurs when the less mobile brain lags behind the movement of the skull, causing brain structures to tear
uOften with extensive tearing of the white matter tracts.
uSecondary injury occurs with release of white blood cells intended for repair, causing further damage due to effects on both healthy and unhealthy tissue.
uCan lead to temporary, permanent, localized, or widespread brain damage, coma, or death.
uCan only be diagnosed through MRI.
uFunctional impairments vary depending on where the shearing occurred.
Diffuse axonal injury summary
uFound in 13.9-72% of TBI
uCommon in deceleration injuries
uPrimary injury
uShearing with rotational forces
uSecondary injury
uMechanical stress leads to metabolic cascade and cell death
uLocal ion flux and Ca+ deregulation lead to cytoskeletal dysfunction and reactive axonal swelling
uGrading
I.Scattered, microscopic evidence of axonal damage
II.Includes corpus callosum
III.Involvement of the pons
The pons is directly involved in maintenance of consciousness
Secondary injury
uFocal
Hypoxia/Ischemia
Herniation
uDiffuse
Hypoperfusion
Hypotension
Elevated ICP
Excitotoxicity
Apoptosis
u1 or more typically present in >30% severe TBI
uSignificant determinants in prognosis
Many signs are clinically apparent during therapy
Common medical complications in TBI (secondary)
uHydrocephalus
uSympathetic Storming
uSeizures
uICU Acquired Weakness (ICUAW)
uCIP
uCIM
uHeterotopic Ossification (HO)
Hydrocephalus
•Signs and sx (similar to those of SDH [subdural hemorrhage], elevated ICP)
•Decreased level of consciousness
•Headache
•Nausea
•Vomiting
•Cognitive changes
•Papilledema
•Decreased vision
•Magnetic gait
•Incontinence

Sympathetic storming—Paroxysmal sympathetic hyperactivity
uDysfunction of the autonomic nervous system
u15-33% of severe TBI
•Signs and Symptoms
•Intermittent agitation
•Diaphoresis
•Hyperthermia
•Hypertension
•Tachycardia
•Tachypnea
•Extensor posturing
•Pupillary dilatation
What to do with sympathetic storming/Paroxysmal Sympathetic Hyperactivity
uIdentify, minimize triggers
uMonitor vital sign response to treatment
uReport exaggerated response, symptoms of unchecked autonomic activity
Seizures
•Signs and Symptoms
•Vary depending type and location of seizure
•May include:
•Motor
Myoclonic jerks
Sustained contractions
•Autonomic signs or symptoms
•Somatosensory or special sensory symptoms
•Absence seizures
frequently missed clinically
ICU aquired weakness
Critical illness polyneuropathy
Critical illness myopathy
Critical illness polyneuropathy
uAxon-loss neuropathy affecting patients who are significantly medically compromised
uDistal > proximal
uMotor and sensory
uTypically symmetrical
uMay note muscle wasting
Thenar muscles
Tib anterior
Quadriceps
Critical illness myopathy
uDefinition: Acute primary myopathy causing weakness and paralysis in individuals with critical illness
Proximal > distal muscle weakness
Sensation spared
Reflexes diminished
Heterotopic ossification
u“Clinically relevant” H.O. varies between 8-22% in individuals with TBI
uLength of coma and ventilation, surgical fixation of fractures, autonomic dysregulation, spasticity strongly associated with increased H.O. risk.
uMost common location in TBI is hip, followed by shoulders, elbows, knees.
uCan lead to worse outcomes depending on joint