Skill Station 1 - Supraglottic Airway insertion
1/34
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
35 Terms
What should be done first before any patient interventions?
don the appropriate PPE for AGMP (aerosol generating medical procedures)
What is the appropriate PPE for SGA and gastric port suctioning?
full droplet
airborne precautions with N95 mask
What is the order in which the PPE should be donned?
H - wash hands
G - gown
M - mask
E - eye protection
G - gloves
What are some indicators that the current airway interventions are insufficient and that an SGA should be used?
ETCO2 is too low/not changing
waveform is not normal
no chest rise and fall
What are the ALS PCS indications for a supraglottic airway?
patient requires ventilatory/respiratory assistance
other interventions (e.g., NPA, OPA, re-positioning) are not effective
What are the ALS PCS conditions for a supraglottic airway?
patient’s own gag reflex is absent
What are the ALS PCS contraindications for a supraglottic airway?
esophageal disease (e.g., esophageal varices)
caustic (e.g., bleach, lye) ingestion
oropharynx trauma
foreign body obstruction
What is the necessary equipment required for supraglottic airway and gastric port suctioning?
medical tape
water-based lubricate
pillow/blanket/towel for repositioning
SGA device
syringe with enough air to inflate SGA
C-collar if needed
What should be tested/confirmed before inserting the SGA into the patient’s airway?
does the cuff (if applicable) inflate
patient weight
patient height
inspect that SGA is not damaged/missing pieces
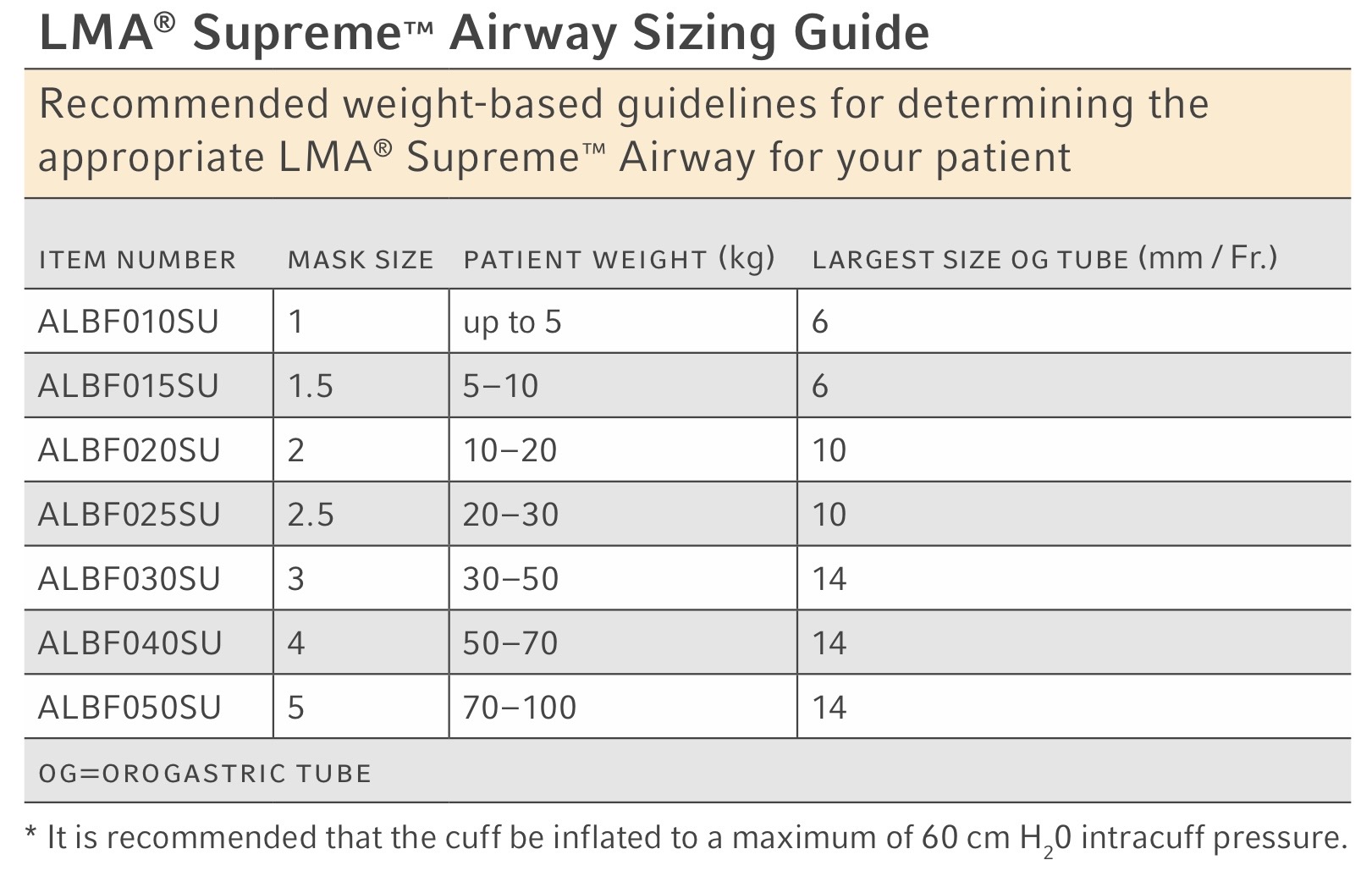
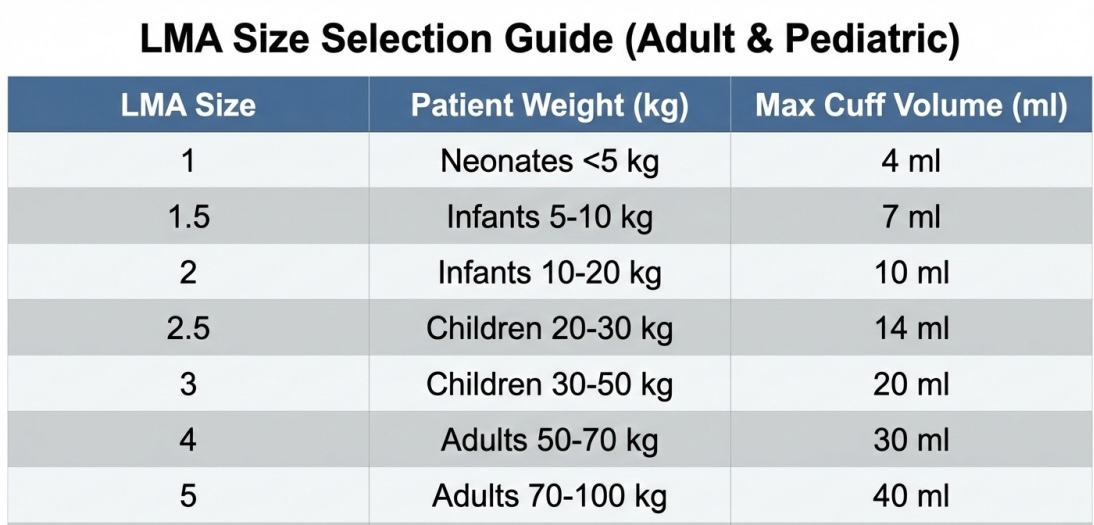
What is the sizing guideline of LMAs?
1 = up to 5 kg (max 6 mm OG tube)
1.5 = 5-10 kg (max 6 mm OG tube)
2 = 10-20 kg (max 10 mm OG tube)
2.5 = 20-30 kg (max 10 mm OG tube)
3 = 30-50 kg (max 14 mm OG tube)
4 = 50-70 kg (max 14 mm OG tube)
5 = 70-100 kg (max 14 mm OG tube)
How should the patient’s face be held while inserting the SGA?
chin lift with non-dominant hand (if no trauma)
colleague can hold c-spine if there is trauma
apply C-collar
What is an alternative method to sizing LMAs?
palatal-crocoid distance
oral airway comparison

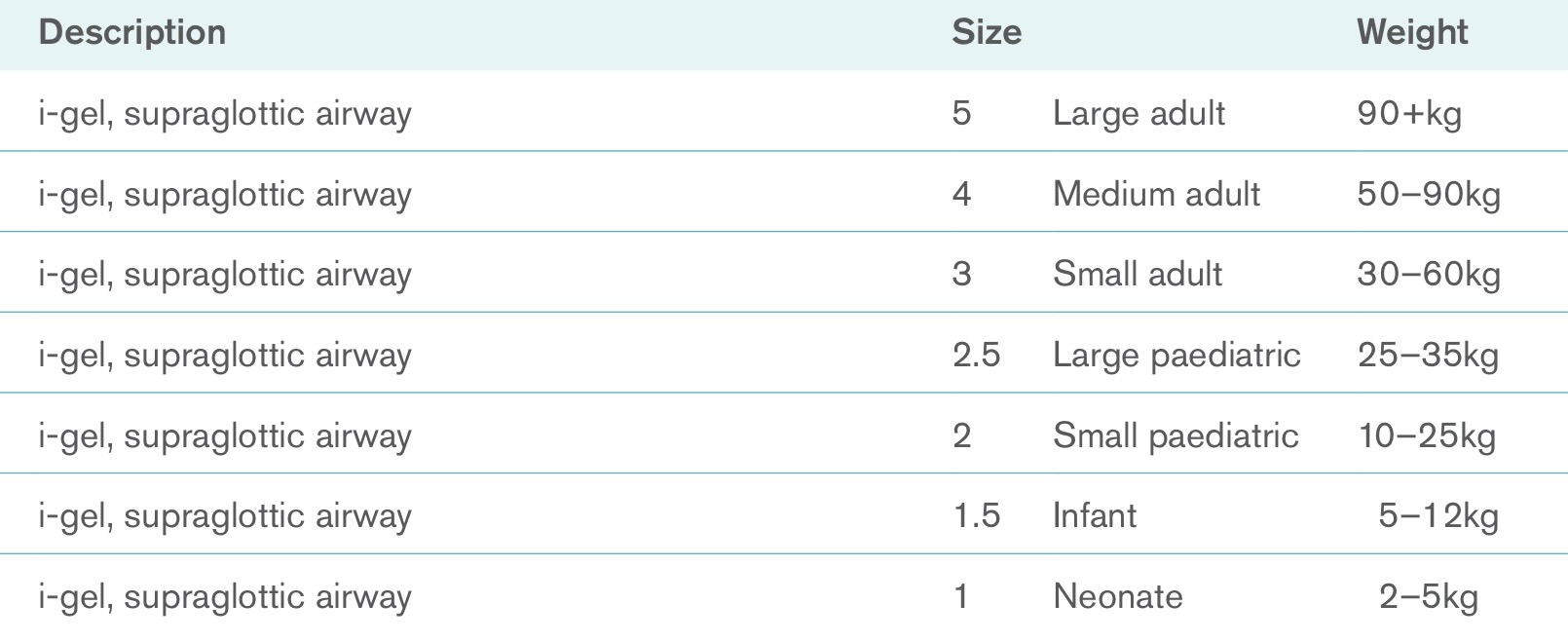
What is the sizing guideline of iGel?
5 (large adult) = 90+ kg
4 (medium adult) = 50-90 kg
3 (small adult) = 30-60 kg
2.5 (large pediatric) = 25-35 kg
2 (small pediatric) = 10-25 kg
1.5 (infant) = 5-12 kg
1 (neonate) = 2-5 kg
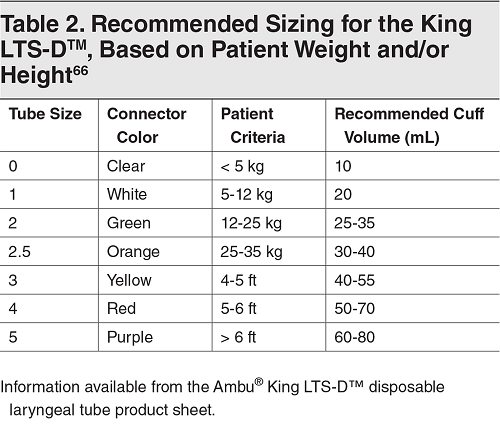
What is the sizing guideline of KingLTs?
clear = < 5 kg
white = 5-12 kg
green = 12-25 kg
orange = 25-35 kg
yellow = 4-5 ft
red = 5-6 ft
purple = > 6ft
What position should the patient be placed in if using an iGEL?
sniffing position
What position should the patient be placed in if using an LMA?
sniffing position
What position should the patient be placed in if using an KingLT?
neutral spine
Where should lubrication be applied to the iGel?
distal tip (without clogging or inhibiting ventilation)

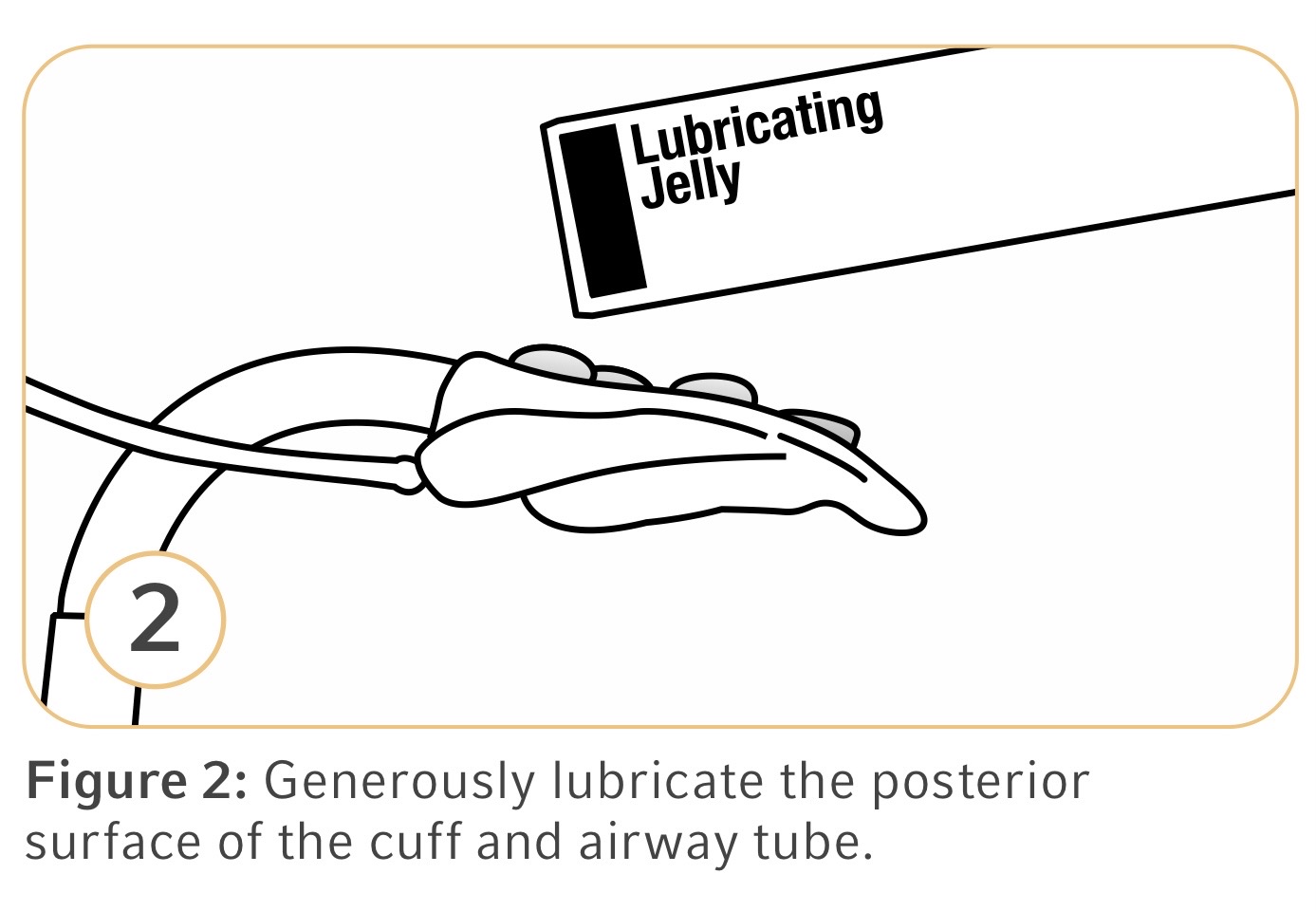
Where should the lubrication be applied on the LMA?
posterior surface of the cuff and airway tube
How should the SGA be held?
within the dominant hand
How should the KingLT be inserted?
45 degree angle/corner of the mouth
tip should be placed behind the base of the tongue
rotate tube to midline as it reaches posterior pharynx
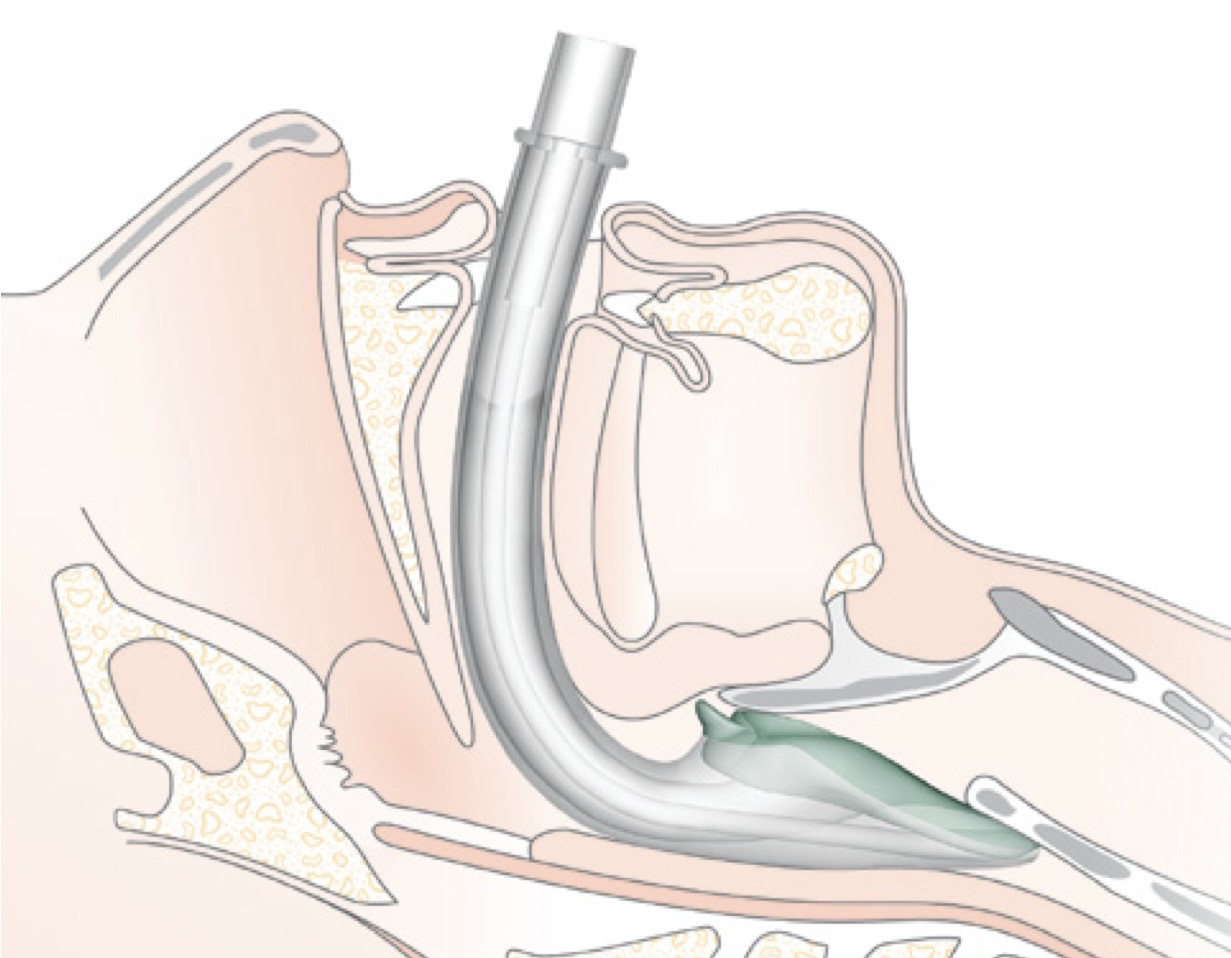
How should the LMA be inserted?
grip it like a pencil
insert until index finger has gone as far as possible past the hard palate
use non-dominant hand to feed LMA in until resistance is felt
How should iGEL be inserted?
hold from tip of the stiffer part of the upper iGEL
advance tube until the base of the connector is aligned with teeth/gums (or resistance is felt)
What are the inflation guidelines for the LMA?
1 = 4 mL
1.5 = 7 mL
2 = 10 mL
2.5 = 14 mL
3 = 20 mL
4 = 30 mL
5 = 40 mL
What are the inflation guidelines for the KingLT?
clear = 10 mL
white = 20 mL
green = 25-35 mL
orange = 30-40 mL
yellow = 40-55 mL
red = 50-70 mL
purple = 60-80 mL

What should be done after the SGA is inserted into the patient’s airway (and inflated, if applicable)?
remove the syringe (if applicable)
attach the BVM (with filter)
What is the primary way to confirm ventilation?
ETCO2 capnography
What are secondary ways to confirm successful ventilation?
auscultation of lungs during bag squeezes (4 points - apexes and bases)
auscultation of abdomen to make sure there is no air entry within the stomach
compliance of bag squeezes (must ask if there is any resistance)
What are the troubleshoots for KingLT insertion?
assess the depth of the tube and gently, slowly withdraw tube until changes are noted in ventilations
add more air to cuff
consider changing the size of the KingLT
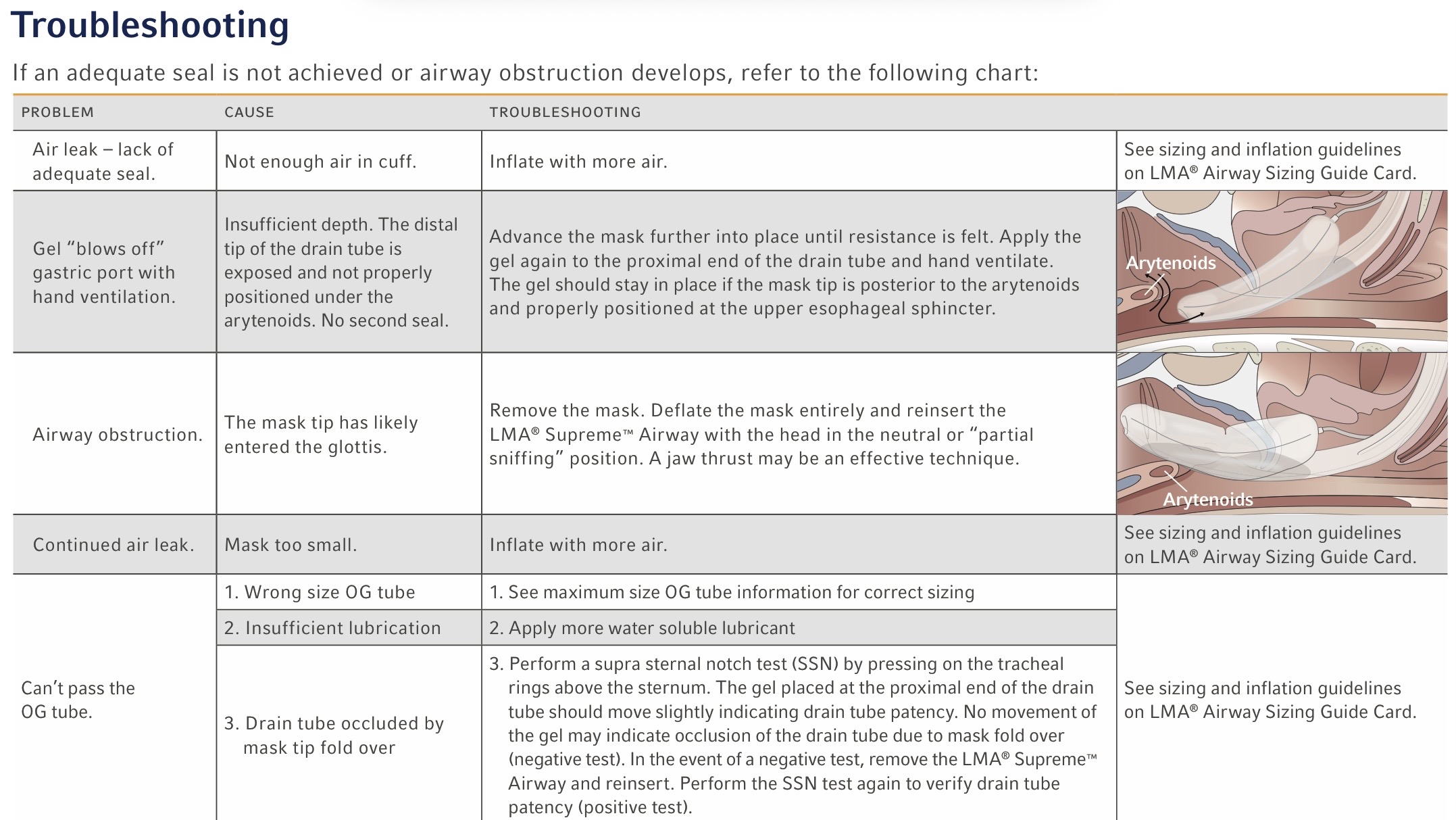
What are the troubleshoots for the LMA?
edge might be twisted (deflate and reinflate, rotate to each side, reinflate)
add more air to the cuff
consider changing size of LMA
What is the final step of applying an SGA?
securing it with medical tape
What are the negative consequences of using a KingLT that is too small?
the distal balloon can obstruct the larynx
What are the negative consequences of using a KingLT that is too large?
distal balloon could rupture esophagus
ventilation opening could be placed too low in the esophagus
What are the negative consequences of improper volume inflation of the SGA?
ischemia of soft tissue
overinflation of the balloon causing rupture
What should be done with the SGA if used in a cardiac arrest scenario and the patient sustains a ROSC?
the airway should only be removed as the gag reflex becomes stimulated
(remember the conditions for use: absent gag reflex)