pathooo urooo
1/120
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
121 Terms
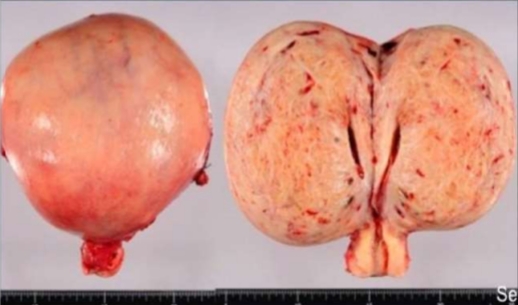
Adenomyosis
Def.:
• Presence of histologically benign endometrial tissue within the myometrium along with myometrial hypertrophy.
• The uterus is enlarged.
• cut section: diffuse thickness of uterine wall with areas of haemorrhages.
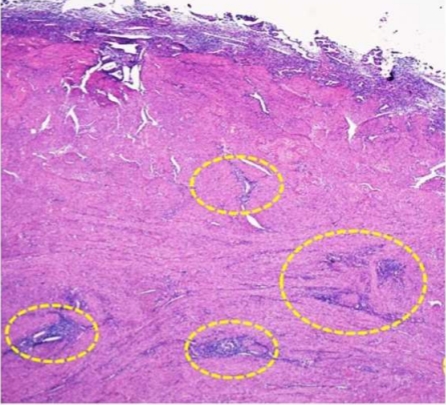
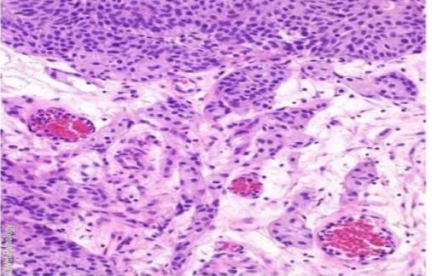
Adenomyosis
• Normal, benign endometrial islands composed of glands & stroma deep within the hypertrophied muscular layer
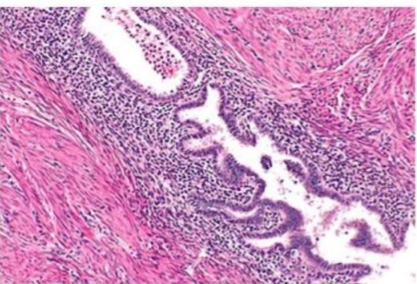
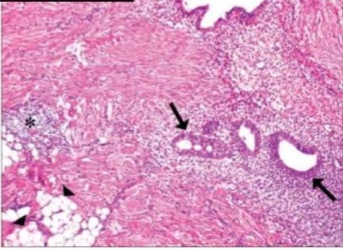
Adenomyosis
• Normal, benign endometrial islands composed of glands & stroma deep within the hypertrophied muscular layer
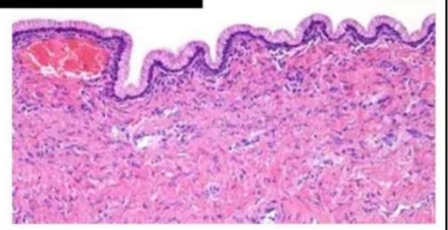
ENDOMETRIOSIS
Def.:
The presence of endometrial glands
and stroma in abnormal locations
outside the uterus.
Typically, the foci of endometriosis
appear as blue or brownish-black.
foci of
endometrial glands and stroma, old
or new haemorrhages, haemosiderin
laden macrophages and surrounding
zone of inflammation and fibrosis.
ENDOMETRIOSIS
Def.:
The presence of endometrial glands
and stroma in abnormal locations
outside the uterus.
Typically, the foci of endometriosis
appear as blue or brownish-black.
foci of
endometrial glands and stroma, old
or new haemorrhages, haemosiderin
laden macrophages and surrounding
zone of inflammation and fibrosis.

Endometrial Adenocarcinoma
- Morphology:
○ Macro:
-Polypoid/Cauliflower-Like Growth + Distended Uterus ⁃
Areas of Haemorrhage, Necrosis & Infiltration
Endometrial adenocarcinoma
o Micro:
Adenocarcinoma of Endometrial
Glands:
Endometrioid (most common)
• Numerous, Small, Back-to-Back Glands
•Irregular & Dysplastic Cells
• Little Stroma
may be well-differentiated,
moderately-differentiated or poorly
differentiated

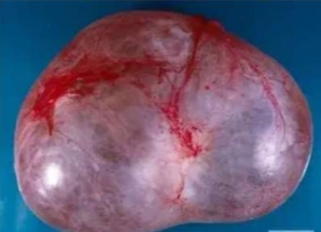
LEIOMYOMA/fibromyomas/ fibroids
The most common uterine tumours, of smooth muscle origin,
/A
occur within the myometrium (intramural or interstitia/, the serosa (subserosa/), or just underneath the endometrium (submucosa/)
often multiple, circumscribed, firm, nodular, grey-white masses of variable size.
characteristic whorled pattern.

LEIOMYOMA/fibromyomas/ fibroids
The most common uterine tumours, of smooth muscle origin,
/A
occur within the myometrium (intramural or interstitia/, the serosa (subserosa/), or just underneath the endometrium (submucosa/)
often multiple, circumscribed, firm, nodular, grey-white masses of variable size.
characteristic whorled pattern.

LEIOMYOMA/fibromyomas/ fibroids
The most common uterine tumours, of smooth muscle origin,
/A
occur within the myometrium (intramural or interstitia/, the serosa (subserosa/), or just underneath the endometrium (submucosa/)
often multiple, circumscribed, firm, nodular, grey-white masses of variable size.
characteristic whorled pattern.
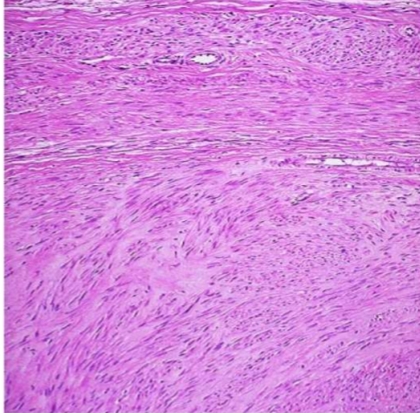
Leiomyoma
• MORPHOLOGIC FEATURES ME
whorled bundles of
smooth muscle cells + connective tissue
The smooth muscle cells are uniform in size and shape with abundant cytoplasm and central oval nuclei.
& Mitosis is infrequent
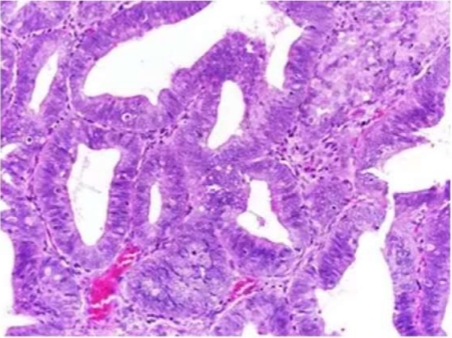
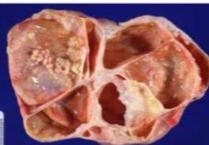
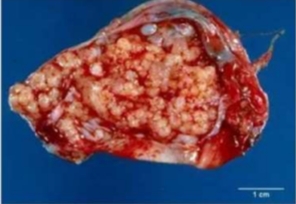
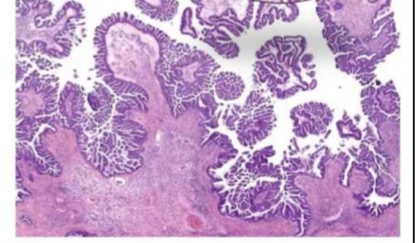
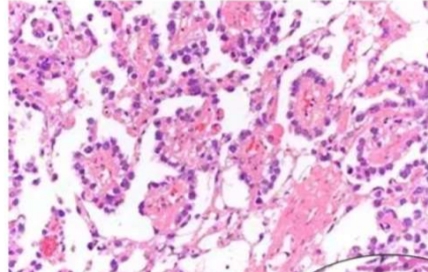
Serous Tumors: Benign Serous Cystadenoma
Gross:
•Unilocular or multilocular cysts, often with papillary projections;
•malignant forms may have solid areas.
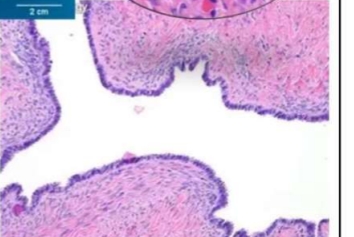
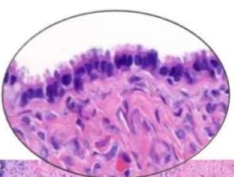
Microscopy:
•Papillary structures Lined by ciliated columnar epithelium; Psammoma bodies seen in malignant forms.
Serous Tumors: Benign Serous Cystadenoma
Gross:
•Unilocular or multilocular cysts, often with papillary projections;
•malignant forms may have solid areas.
Microscopy:
•Papillary structures Lined by ciliated columnar epithelium; Psammoma bodies seen in malignant forms.
Serous Tumors: Benign Serous Cystadenoma
Gross:
•Unilocular or multilocular cysts, often with papillary projections;
•malignant forms may have solid areas.
Microscopy:
•Papillary structures Lined by ciliated columnar epithelium; Psammoma bodies seen in malignant forms.
Serous Tumors: Benign Serous Cystadenoma
Gross:
•Unilocular or multilocular cysts, often with papillary projections;
•malignant forms may have solid areas.
Microscopy:
•Papillary structures Lined by ciliated columnar epithelium; Psammoma bodies seen in malignant forms.
Serous Tumors: Bordeline Serous Tumor
Gross:
•Unilocular or multilocular cysts, often with papillary projections;
•malignant forms may have solid areas.
Microscopy:
•Papillary structures Lined by ciliated columnar epithelium; Psammoma bodies seen in malignant forms.
Serous Tumors: Bordeline Serous Tumor
Gross:
•Unilocular or multilocular cysts, often with papillary projections;
•malignant forms may have solid areas.
Microscopy:
•Papillary structures Lined by ciliated columnar epithelium; Psammoma bodies seen in malignant forms.
Serous Tumors: Bordeline Serous Tumor
Gross:
•Unilocular or multilocular cysts, often with papillary projections;
•malignant forms may have solid areas.
Microscopy
•Papillary structures Lined by ciliated columnar epithelium; Psammoma bodies seen in malignant forms.

Serous Tumors: Serous carcinoma
Gross:
•Unilocular or multilocular cysts, often with papillary projections;
•malignant forms may have solid areas.
Microscopy:
•Papillary structures Lined by ciliated columnar epithelium; Psammoma bodies seen in malignant forms.
Serous Tumors: Serous carcinoma
Gross:
•Unilocular or multilocular cysts, often with papillary projections;
•malignant forms may have solid areas.
Microscopy:
•Papillary structures Lined by ciliated columnar epithelium; Psammoma bodies seen in malignant forms.
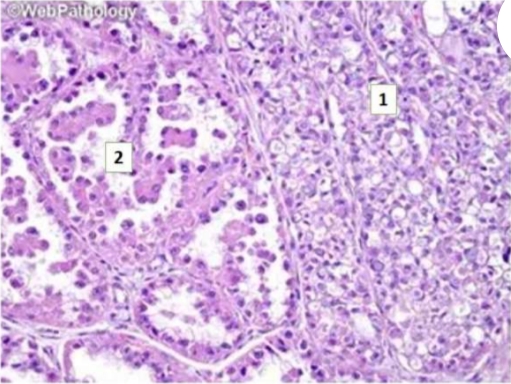
•Mucinous Tumors:
Gross:
•Large, multilocular cysts
filled with thick, gelatinous
material; malignant forms
may show necrosis.
Microscopy:
•Glandular structures lined by
Lined by mucin-secreting
columnar epithelium;
•may be associated with
pseudomyxoma peritonei
•Mucinous Tumors:
Gross:
•Large, multilocular cysts
filled with thick, gelatinous
material; malignant forms
may show necrosis.
Microscopy:
•Glandular structures lined by
Lined by mucin-secreting
columnar epithelium;
•may be associated with
pseudomyxoma peritonei
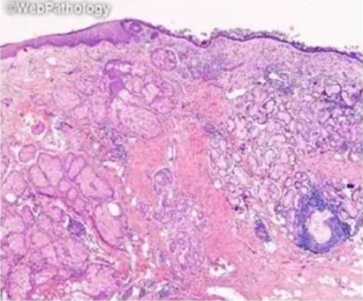
•Clear Cell Carcinoma: Microscopy:
•Clear cells, •Hobnail cells

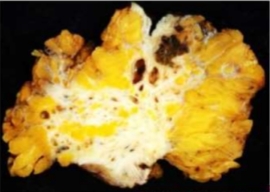
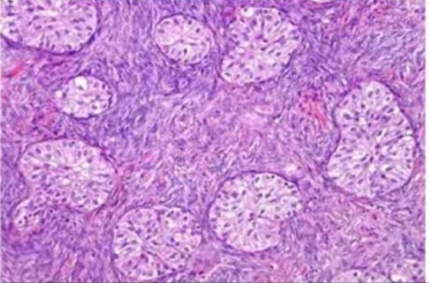
•Brenner Tumor
Gross:
sharply demarcated, solid, yellow
white cut surface
Microscopy:
•mature transitional
epithelium (urothelium) arranged in
sharply defined solid clusters,
nests and trabeculae of within a
dense fibromatous stroma
•Brenner Tumor
Gross:
sharply demarcated, solid, yellow
white cut surface
Microscopy:
•mature transitional
epithelium (urothelium) arranged in
sharply defined solid clusters,
nests and trabeculae of within a
dense fibromatous stroma

B. Germ Cell Tumors (15-20%)
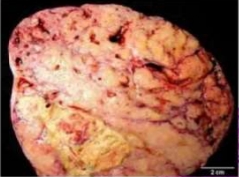
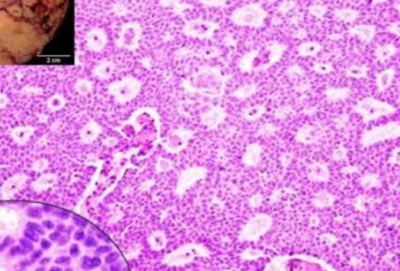
Dysgerminoma
Gross:
solid mass. Grey white, homogenous
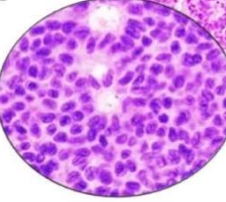
Microscopy:
monomorphic tumor ells arranged
in diffuse sheets, & separated
by delicate fibrous septae
contain lymphocytes (T cells), plasma
cells
B. Germ Cell Tumors (15-20%)
Dysgerminoma
Gross:
solid mass. Grey white, homogenous
Microscopy:
monomorphic tumor ells arranged
in diffuse sheets, & separated
by delicate fibrous septae
contain lymphocytes (T cells), plasma
cells
B. Germ Cell Tumors (15-20%)
Yolk Sac Tumor
Microscopy:
papillary structure is contained
within a cystic space lined by
flattened cells (Glomeruloid),
=Schiller-Duval body
a hallmark of yolk sac tumor
B. Germ Cell Tumors (15-20%)
Yolk Sac Tumor
Microscopy:
papillary structure is contained
within a cystic space lined by
flattened cells (Glomeruloid),
=Schiller-Duval body
a hallmark of yolk sac tumor

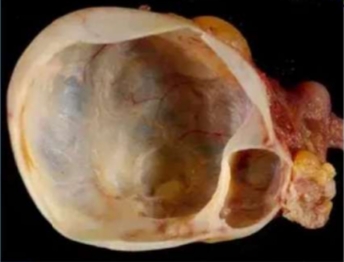
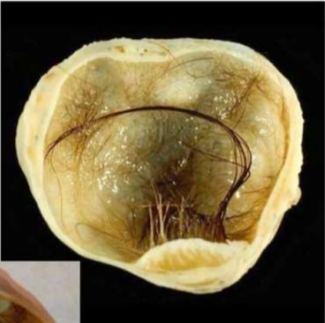
Mature Teratoma (Dermoid Cyst G/A
• unilocular cvst. lined by the skin
& filled with paste-like sebaceous secretions and desquamated keratin admixed with masses of hair
• Generallv. in one area of the cvst wall. solid prominence is seen (Rokitansky's protuberance) where tissue elements such as tooth, bone, cartilage and various other odd tissues are present.
Mature Teratoma (Dermoid Cyst G/A
• unilocular cvst. lined by the skin
& filled with paste-like sebaceous secretions and desquamated keratin admixed with masses of hair
• Generallv. in one area of the cvst wall. solid prominence is seen (Rokitansky's protuberance) where tissue elements such as tooth, bone, cartilage and various other odd tissues are present.
. Mature Teratoma (Dermoid Cyst)
Multiple Mature
ME:
Tissues in one tumour & Encapsulated
Ectodermal derivatives are most prominent: lining of the cyst wall is stratified squamous epithelium and its adnexal structures such as sebaceous glands, sweat glands and hair follicles.
• Tissues of mesodermal and endodermal origin are also commonly present.
. Mature Teratoma (Dermoid Cyst)
Multiple Mature
ME:
Tissues in one tumour & Encapsulated
Ectodermal derivatives are most prominent: lining of the cyst wall is stratified squamous epithelium and its adnexal structures such as sebaceous glands, sweat glands and hair follicles.
• Tissues of mesodermal and endodermal origin are also commonly present.
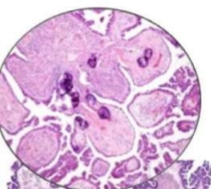
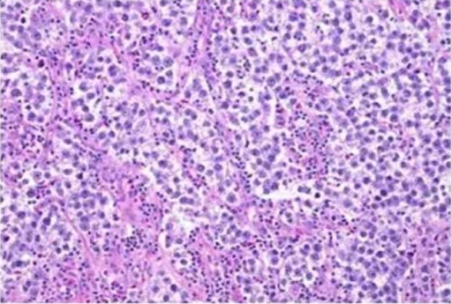
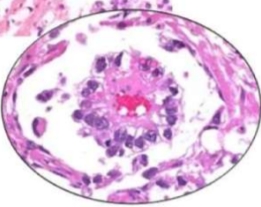
Granulosa Cell Tumor
• all ages.
• secrete oestrogen.
GIA
• small, solid, partly cystic and usually unilateral tumour.
• Cut section of solid areas is yellowish-brown M/E
• granulosa cells are arranged in micro- and macrofollicular, trabecular, bands and diffuse sheets.
• rosettelike structures called:
Call-Exner bodies: central rounded pink mass surrounded by a circular row of granulosa cells having grooved nuclei with coffee-bean appearance.
Granulosa Cell Tumor
• all ages.
• secrete oestrogen.
GIA
• small, solid, partly cystic and usually unilateral tumour.
• Cut section of solid areas is yellowish-brown M/E
• granulosa cells are arranged in micro- and macrofollicular, trabecular, bands and diffuse sheets.
• rosettelike structures called:
Call-Exner bodies: central rounded pink mass surrounded by a circular row of granulosa cells having grooved nuclei with coffee-bean appearance.
Granulosa Cell Tumor
• all ages.
• secrete oestrogen.
GIA
• small, solid, partly cystic and usually unilateral tumour.
• Cut section of solid areas is yellowish-brown M/E
• granulosa cells are arranged in micro- and macrofollicular, trabecular, bands and diffuse sheets.
• rosettelike structures called:
Call-Exner bodies: central rounded pink mass surrounded by a circular row of granulosa cells having grooved nuclei with coffee-bean appearance.

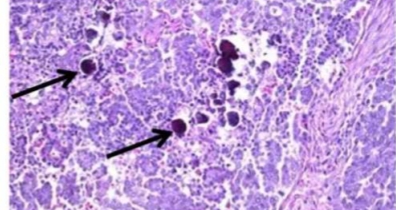
Krukenberg Tumor:
•Bilateral ovarian metastases by
transcoelomic spread from gastric, colon,
appendix and breast carcinoma;
GIA
• moderately large, rounded or kidney shaped,
firm, multinodular masses in both ovaries.
ME
• mucin-filled signet ring cells which may lie
singly or in clusters
Krukenberg Tumor:
•Bilateral ovarian metastases by
transcoelomic spread from gastric, colon,
appendix and breast carcinoma;
GIA
• moderately large, rounded or kidney shaped,
firm, multinodular masses in both ovaries.
ME
• mucin-filled signet ring cells which may lie
singly or in clusters

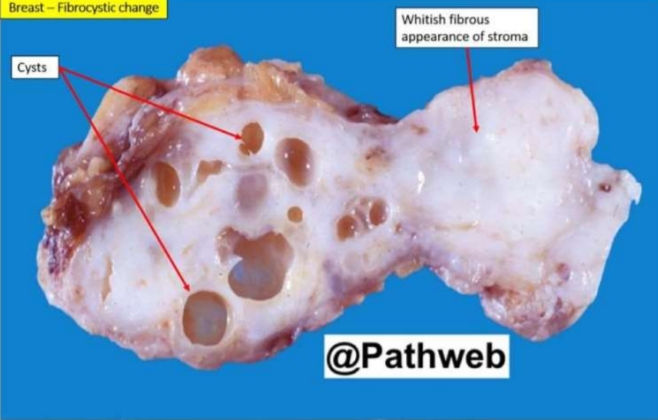
Fibrocystic changes
G/A
○ Grey-white Scar Tissue (Fibrosis) ○ Multiple Cystic Lesions.
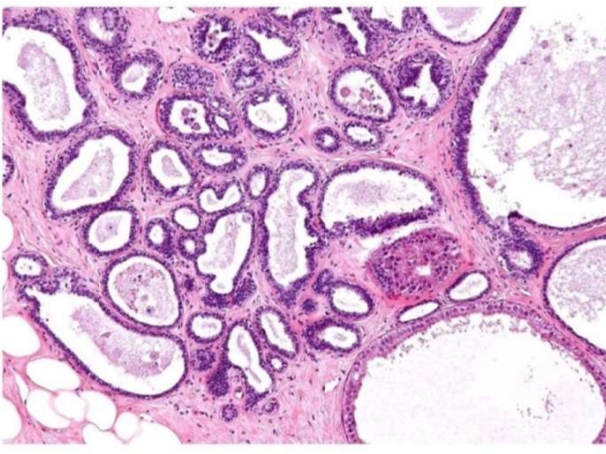
FIBROCYSTIC CHANGE - Morphology:
M/E
o Non Proliferative: 1. Cyst formation
• lining flattened or atrophic.
• Frequently, there is apocrine metaplasia 2. Fibrosis surrounding the cysts and
variable degree of stromal lymphocytic infiltrate.
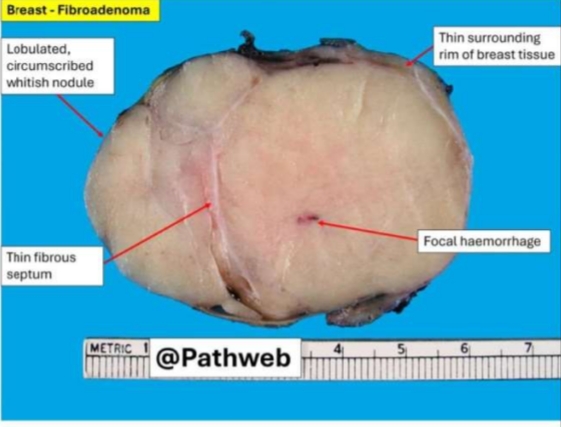
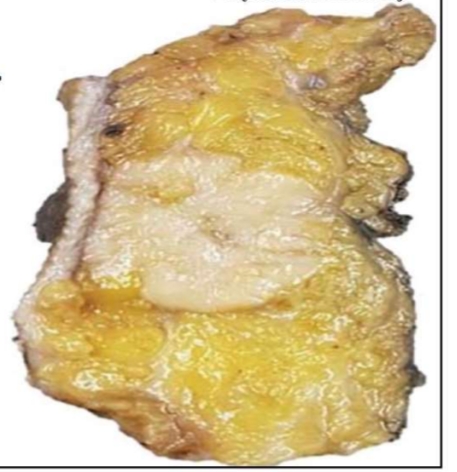
Fibroadenoma “breast mouse”
Capsulated, Firm,
Homogenous, Grey, Nodular/lobulated Tumour, Without Cysts.
Lobulated, circumscribed Without Cysts.

Fibroadenoma “Breast mouse”
Capsulated, Firm,
Homogenous, Grey, Nodular/lobulated Tumour, Without Cysts.
Lobulated, circumscribed Without Cysts.
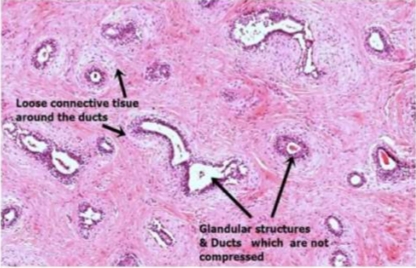
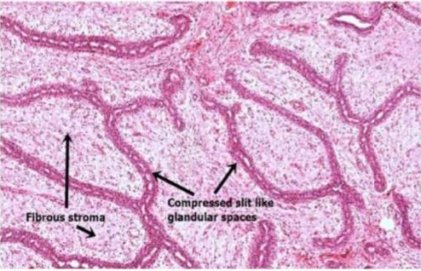
Fibroadenoma “Breast Mouse”
Fibrous tissue comprises most of a fibroadenoma,.
The arrangements between fibrous overgrowth and ducts may produce two types of patterns in the same tumour
⁃ Intracanalicular pattern :stroma compresses the ducts ---slit-like clefts lined by ductal epithelium or
⁃ Pericanalicular pattern: encircling masses of fibrous stroma around the patent or dilated
ducts.
Fibroadenoma “breast mouse”
Fibrous tissue comprises most of a fibroadenoma,.
The arrangements between fibrous overgrowth and ducts may produce two types of patterns in the same tumour
⁃ Intracanalicular pattern :stroma compresses the ducts ---slit-like clefts lined by ductal epithelium or
⁃ Pericanalicular pattern: encircling masses of fibrous stroma around the patent or dilated
ducts.

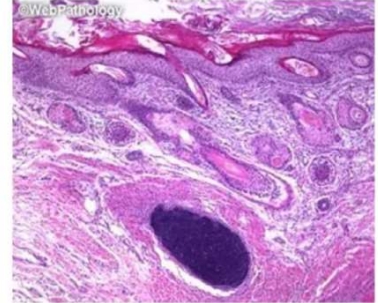
Paget’s disease
Gross picture:
Nipple eczema or ulceration. Excoriation of the areola. There may or may not be a palpable mass.

Paget’s disease
Gross picture:
Nipple eczema or ulceration. Excoriation of the areola. There may or may not be a palpable mass.

Paget’s disease
Gross picture:
Nipple eczema or ulceration. Excoriation of the areola. There may or may not be a palpable mass.
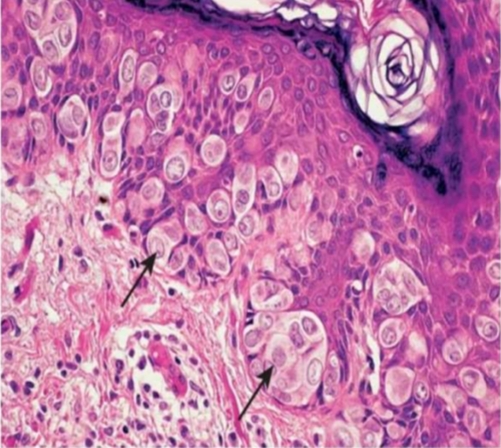
• Microscopic picture:
• The basal layer of epidermis
is infiltrated by large
malignant cells with:
a) Clear cytoplasm. & Large
hyperchromatic nuclei
(Paget's cells).
•The underlying carcinoma
may be:
a) Intraductal.
b) Invasive carcinoma.

Nipple Retraction

Peau d’orange

Ulceration
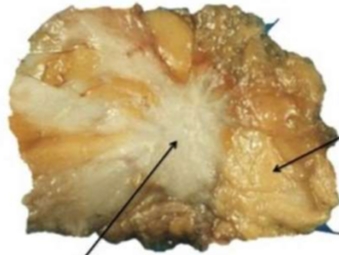
Invasive Ductal carcinoma no special type
• Gross picture:
-Shape: non-capsulated, irregular and spiky.
-Consistency: hard.
-Size: variable usually >1 cm.
-Colour: Grayish white.
-Mobility: Early mobile but late fixed.
The cut surface:
• Greyish white,
• Concave (due to retraction of excessive
fibrosis)
• The tumor gives a gritty sensation during
cutting
Invasive ductal carcinoma no ductal type
• Gross picture:
-Shape: non-capsulated, irregular and spiky.
Consistency: hard.
-Size: variable usually >1 cm .
-Colour: Grayish white.
-Mobility: Early mobile but late fixed. The cut surface:
• Greyish white,
• Concave (due to retraction of excessive fibrosis)
• The tumor gives a gritty sensation during cutting.
Poorly circumscribed, firm to hard mass with irregular, infiltrative margins (crab-like).
Cut section is whitish and gritty. (arrow in the middle)
B. Invasive Breast Carcinoma
Invasive Ductal Carcinoma of No Special Type (|BC-NST)
-Diffuse sheets, well-defined nests, and cords of malignant ductal cells.
-Sheets are separated by productive dense stromal fibrosis (Desmoplastic reaction,
B. Invasive Breast Carcinoma
Invasive Ductal Carcinoma of No Special Type (|BC-NST)
-Diffuse sheets, well-defined nests, and cords of malignant ductal cells.
-Sheets are separated by productive dense stromal fibrosis (Desmoplastic reaction,
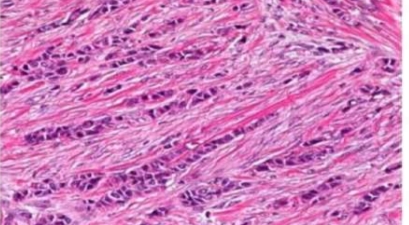
Invasive lobular carcinoma:
• The tumor cells are small to medium-sized regular, and uniform ,with little cytological abnormalities.
• They grow singly in the form of linear cords (Indian File fibrous stroma.

Invasive lobular carcinoma:
• The tumor cells are small to medium-sized regular, and uniform ,with little cytological abnormalities.
• They grow singly in the form of linear cords (Indian File fibrous stroma.
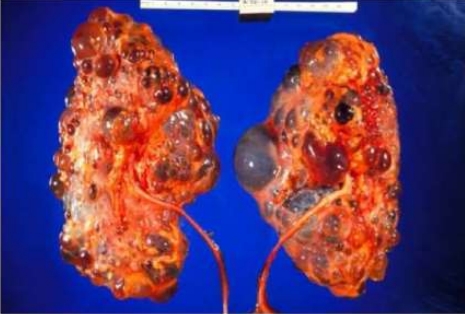
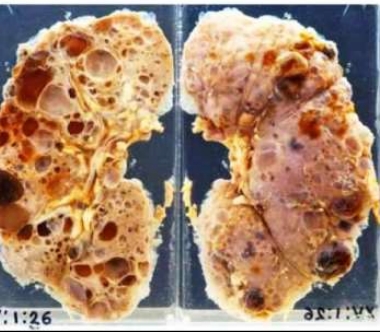
POLYCYSTIC KIDNEY DISEASE
Bilateral, large cystic kidney
o Some areas of Haemorrhage
o Some normal kidney tissue between cysts
- Cysts:
o = Bulging, filtrate-filled pouches of kidney.
o Caused by a Nephron not connecting to any collecting duct - (le: Filtrate has nowhere to go → Expands & Expands)
In AR (childhood type) all tubules are affected & in AD (Adult type, many tubules are affected)
POLYCYSTIC KIDNEY DISEASE
Bilateral, large cystic kidney
o Some areas of Haemorrhage
o Some normal kidney tissue between cysts
- Cysts:
o = Bulging, filtrate-filled pouches of kidney.
o Caused by a Nephron not connecting to any collecting duct - (le: Filtrate has nowhere to go → Expands & Expands)
In AR (childhood type) all tubules are affected & in AD (Adult type, many tubules are affected)
POLYCYSTIC KIDNEY DISEASE
Bilateral, large cystic kidney
o Some areas of Haemorrhage
o Some normal kidney tissue between cysts
- Cysts:
o = Bulging, filtrate-filled pouches of kidney.
o Caused by a Nephron not connecting to any collecting duct - (le: Filtrate has nowhere to go → Expands & Expands)
In AR (childhood type) all tubules are affected & in AD (Adult type, many tubules are affected)

Minimal Change disease
- Pathologic features: *Electron microscopy: fusion (effacement) of the foot processes of epithelial cells (Podocytes)
SGS - FOCAL SEGMENTAL
GLOMERULOSCLEROSIS:
⁃ Very Similar to Minimal Change Disease, but in young Adults
*Pathologic features:
Microscopic picture:
○
starts in the juxtamedullary glomeruli.
○ Affects parts (segmental) of some (focal)
glomeruli of nephron
○ Foot processes of podocytes damaged
○ hyalinosis (hyaline/ glassy view on histology, -> scar tissue (glomerulosclerosis

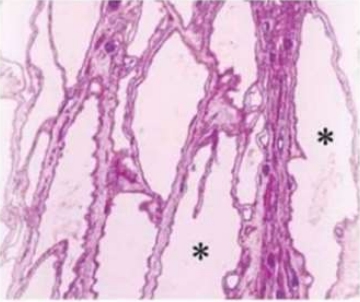
3- MGN- MEMBRANOUS GLOMERULONEPHRITIS:
- MGN = >50% of Adult Nephrotic Syndrome
*Pathologic features:
Microscopic picture:
diffuse hyaline thickening and formation of spikes
giving hair comb appearance of the basement membrane.
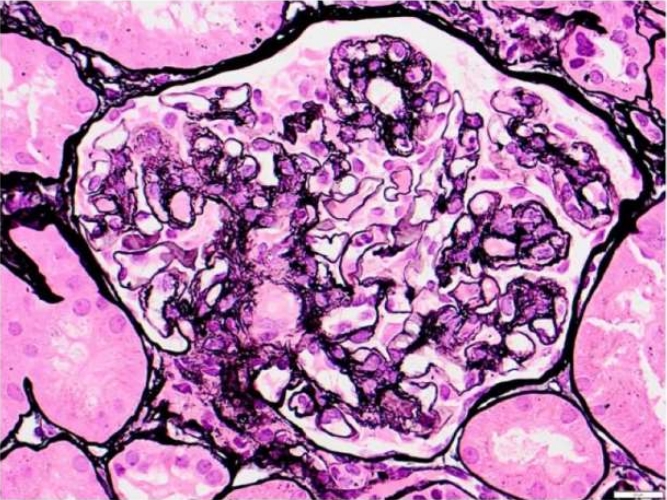
4- Membranoproliferative glomerulonephritis:
65% present as nephrotic & 35% mixed
nephrotic & nephritic
*Pathologic features:
Microscopic picture:
D Enlarged hypercellular lobulated glomeruli
due to mesangial proliferation.
2 Thickened capillary walls with double
contour / tram track appearance
Best demonstrated by silver or PAS stain
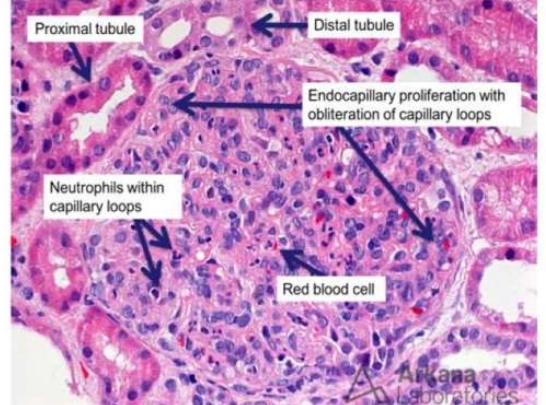
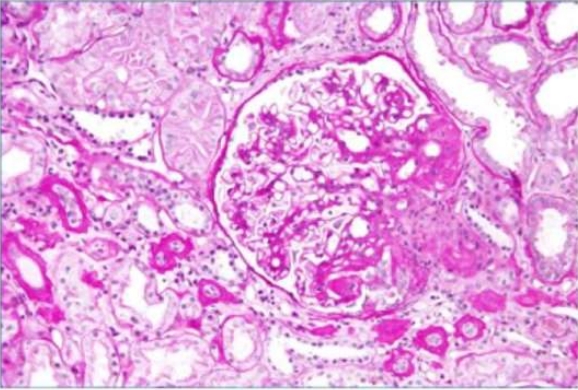
1- PSGN - POST-STREPTOCOCCAL GLOMERULONEPHRITIS:
THE Childhood cause of Nephritic Syndrome
Pathological features: icroscopic picture:
-Glomeruli: diffusely swollen and cellular (proliferation of endothelial cells + leucocytic nfiltration).
-Convoluted tubules : cloudy swelling and fatty hange of lining cells,.
-Collecting tubules: casts in their lumen (mainly lood casts).
-Interstitial tissue: edematous, hyperemic and shows leucocytic infiltration.
1- PSGN - POST-STREPTOCOCCAL GLOMERULONEPHRITIS:
THE Childhood cause of Nephritic Syndrome
Pathological features: icroscopic picture:
-Glomeruli: diffusely swollen and cellular (proliferation of endothelial cells + leucocytic nfiltration).
-Convoluted tubules : cloudy swelling and fatty hange of lining cells,.
-Collecting tubules: casts in their lumen (mainly lood casts).
-Interstitial tissue: edematous, hyperemic and shows leucocytic infiltration.
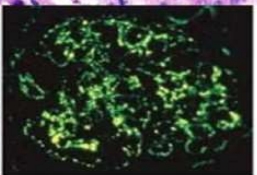
Immunofluorescence: Granular (hump-like) deposits
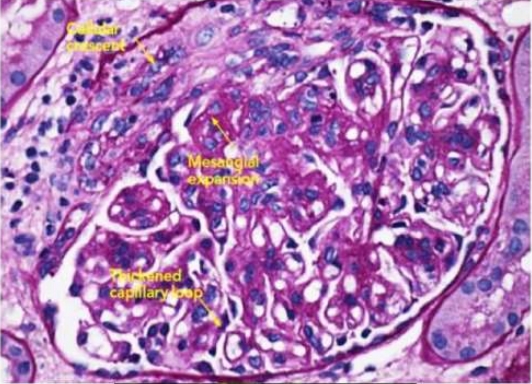
Rapidly progressive glomerulonephritis: (Crescentic glomerulonephritis)
• *Pathological features:
Microscopic picture:
1- Glomeruli: show crescent formation due to proliferation of the parietal layer of the Bowman's capsule.
2- compressed capillary tufts that become
replaced by fibrous tissue.
3-Thrombosis in the capillary loops and adhesions between the tuft and the capsule.
4-Focal tubular necrosis & interstitial inflammatory cellular infiltration. Tubular lumen contains red cells, hyaline and cellular casts.
Rapidly progressive glomerulonephritis: (Crescentic glomerulonephritis)
• *Pathological features:
Microscopic picture:
1- Glomeruli: show crescent formation due to proliferation of the parietal layer of the Bowman's capsule.
2- compressed capillary tufts that become
replaced by fibrous tissue.
3-Thrombosis in the capillary loops and adhesions between the tuft and the capsule.
4-Focal tubular necrosis & interstitial inflammatory cellular infiltration. Tubular lumen contains red cells, hyaline and cellular casts.
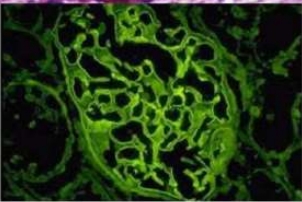
*Immunofluorescence: According to cause,
in Goodpasture's syndrome:
linear pattern deposits of antibodies along GBM
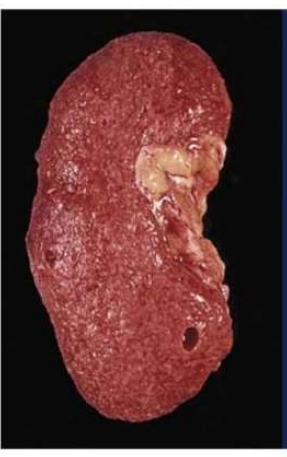
Chronic slowly progressive glomerulonephritis
[End stage Kidney]
*Pathological features:
Gross picture:
1. The kidneys are small in size
and firm.
2. The surface is finely granular,
and the capsule is adherent and
difficult to strip with decortication.
3. The cut surface shows that the
cortex is narrowed and not
demarcated from the medulla. The
peri pelvic fat is increased.
Chronic slowly progressive glomerulonephritis
[End stage Kidney]
*Pathological features:
Gross picture:
1. The kidneys are small in size
and firm.
2. The surface is finely granular,
and the capsule is adherent and
difficult to strip with decortication.
3. The cut surface shows that the
cortex is narrowed and not
demarcated from the medulla. The
peri pelvic fat is increased.
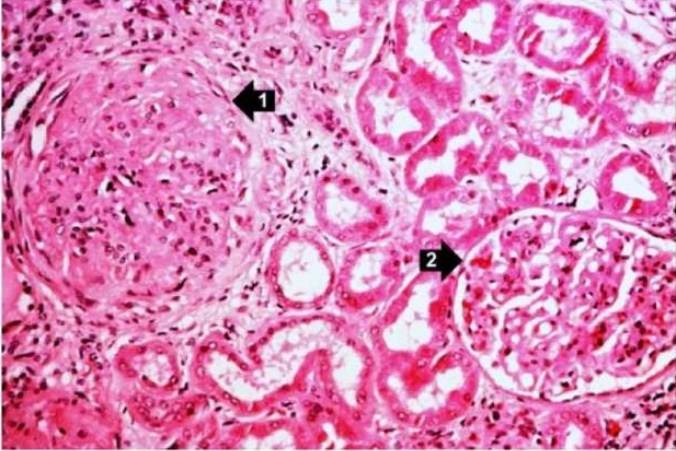
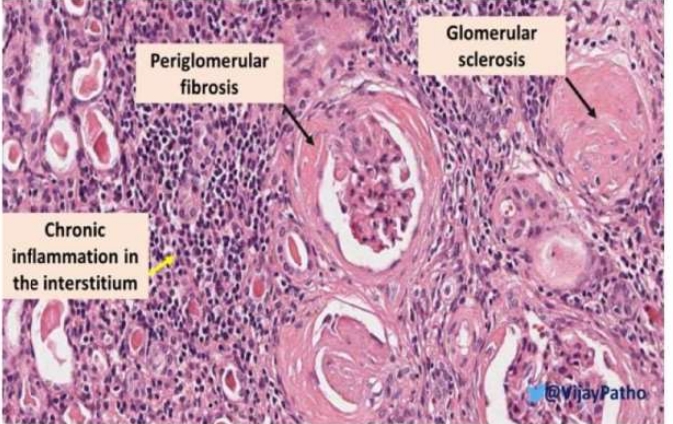
Chronic slowly progressive glomerulonephritis:
Microscopic picture:
1. Glomeruli : sclerosed.
2. Tubules:
contains hyaline and granular casts & are:
Some are atrophied & others show
compensatory hypertrophy, dilatation and
cyst formation
3. Interstitial fibrosis and infiltration by
chronic inflammatory cells.
4. Thick Medium sized and small arteries

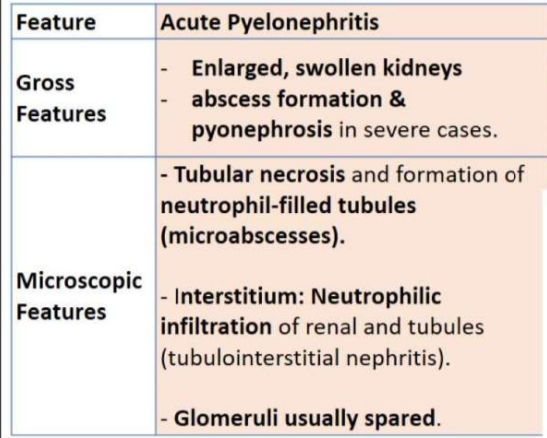
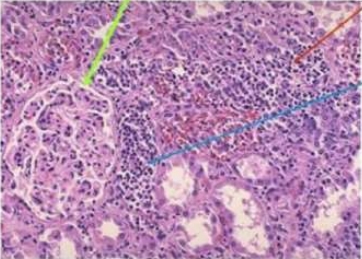
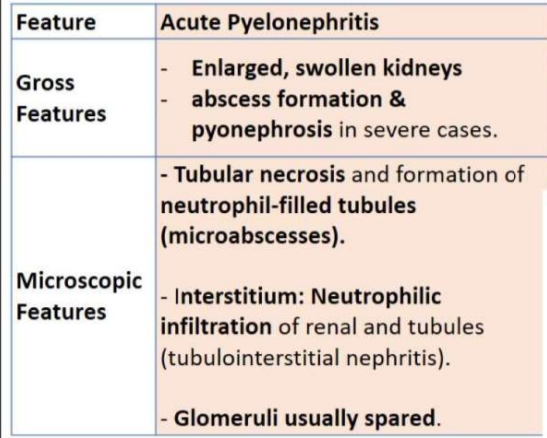
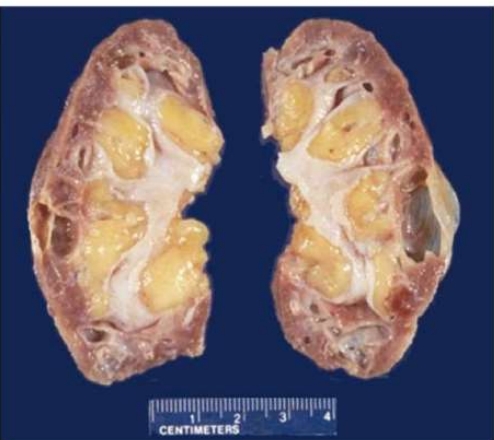
Chronic Pyelonephritis
Tubular atrophy and dilation, with thyroidization (dilated tubules filled with eosinophilic material resembling thyroid colloid).
- Interstitium: Chronic inflammatory infiltrates & Fibrosis
Glomeruli may show ischemic changes due to scarring.
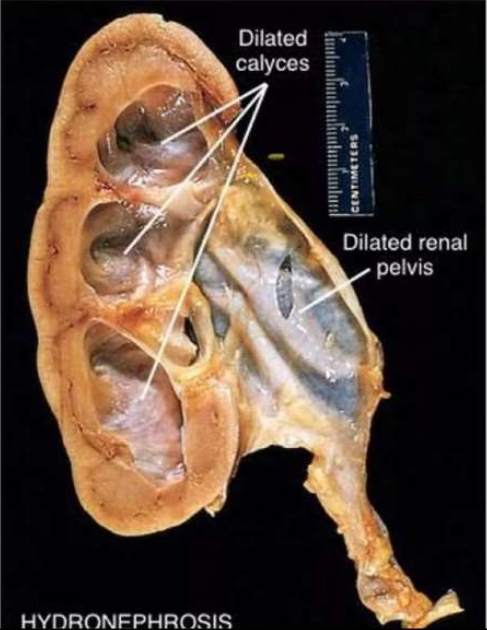
Hydronephrosis
Morphology:
1- Enlarged kidney
2- Urine stasis: infection and stone formation.
3- Pyonephrosis and pyelonephiritis: hematuria &pyuria.
4- Bilateral hydro ureter & hydronephrosis: ends by CRF.
5- Bladder wall trabeculation... diverticulosis in cases of Bladder neck or uretheral obstruction.
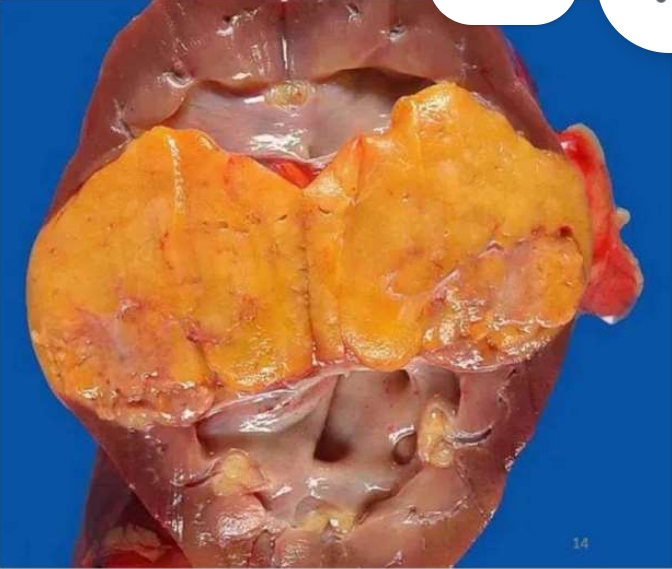
Angiomyolipoma (AML)
Gross Pathology
Well-circumscribed, non
encapsulated mass
Yellow-tan color due to abundant fat
content
Heterogeneous cut surface, with
areas of:
Yellow (adipose tissue)
Pink to tan (smooth muscle
component)
Red-brown (vascular component)
May show hemorrhagic areas
(spontaneous rupture and bleeding
in larger tumors >4 cm)
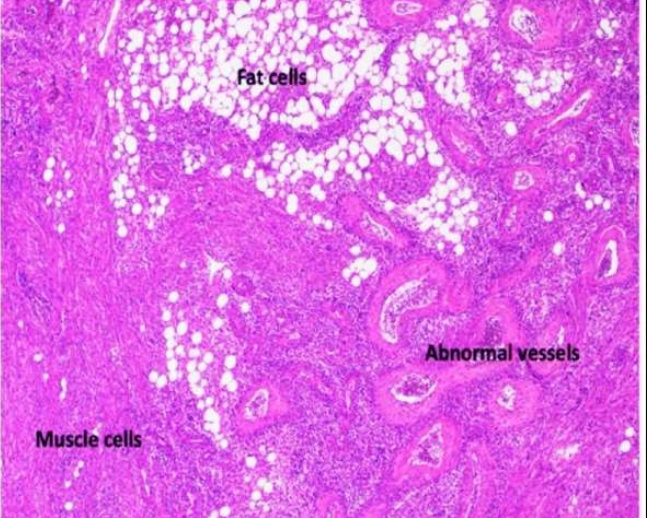
Angiomyolipoma (AML)
• Microscopic Pathology
The three characteristic components are:
1.Adipose Tissue
1. Mature adipocytes (variable quantity)
2. Can predominate in some cases (lipomatous
variant)
2.Smooth Muscle Cells
1. Spindle or epithelioid smooth muscle cells
arranged in bundles
2. May show nuclear atypia (not a sign of
malignancy in AML)
3.Thick-Walled Blood Vessels
1. Irregular, dysmorphic blood vessels with
thickened walls
2. Lack of elastic fibers, making vessels prone
to rupture and hemorrhage

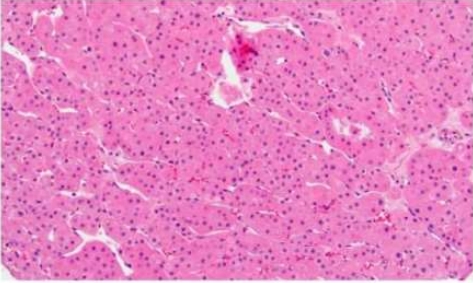
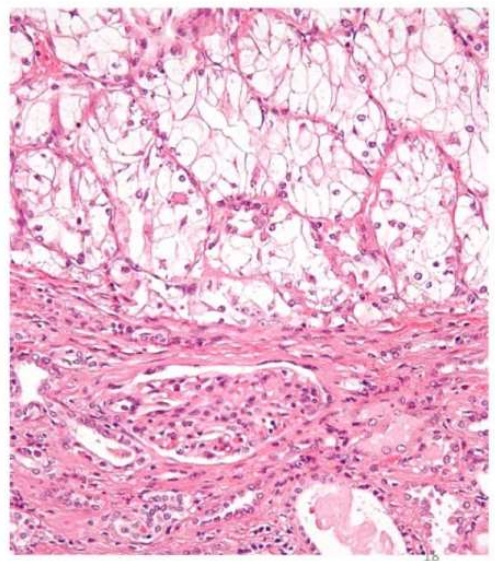
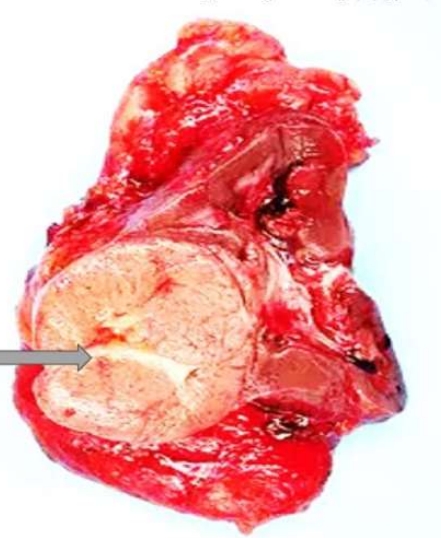
Renal Oncocytoma
• Benign epithelial tumor
• Originates from intercalated cells of the collecting duct
• Gross Pathologic Features:
• Well-circumscribed, mahogany-brown mas • Central stellate scar (not always present
• No necrosis or hemorrhage
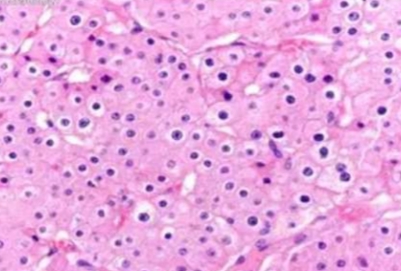
• Microscopic Pathologic Features:
• Large polygonal cells with abundant eosinophilic, granular cytoplasm (due to numerous mitochondria
• Round, uniform nuclei with prominent nucleoli
Renal Oncocytoma
• Benign epithelial tumor
• Originates from intercalated cells of the collecting duct
• Gross Pathologic Features:
• Well-circumscribed, mahogany-brown mas • Central stellate scar (not always present
• No necrosis or hemorrhage
• Microscopic Pathologic Features:
• Large polygonal cells with abundant eosinophilic, granular cytoplasm (due to numerous mitochondria
• Round, uniform nuclei with prominent nucleoli
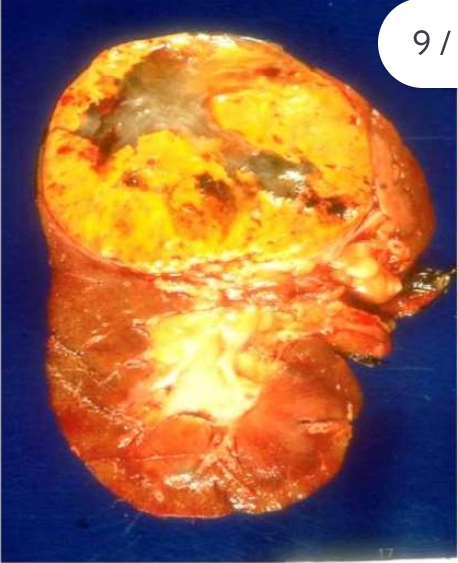
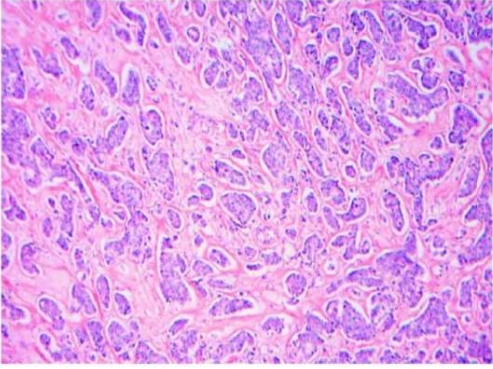
Renal Cell Carcinoma
. Clear Cell Renal Cell Carcinoma (ccRCC) (Most common subtype: 70-80% of RCC cases
Origin: it arises from the epithelium of the convoluted tubules.
Incidence: usually common in males more than 40 years of age.
Gross Pathologic Features:
• Well-circumscribed, golden-yellow mass (due to lipid content
• Areas of hemorrhage, necrosis, and cystic degeneration (variegated cut surface
• Typically located in the upper pole of the kidney • Typically located in the upper pole of the kidney
1.Clear Cell Renal Cell Carcinoma (ccRCC)
• Microscopic Pathologic Features:
• Tumor cells Round to polygonal cells with clear cytoplasm & distinct cell membranes
• Nuclei varv from low-grade (small round nuclei) to high-grade (large, pleomorphic nuclei)
• Delicate, branching vasculature chicken-wire pattern
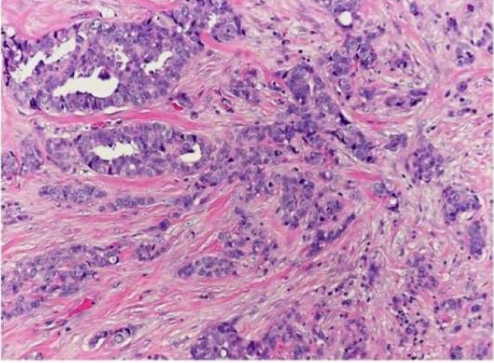
2. Chromophobe Renal Cell Carcinoma
• (5-7% of RCC cases)
• Gross Pathologic Features:
• Tan or pale, well-circumscribed mass with a central scar (15%)
• Usually lacks necrosis and hemorrhage
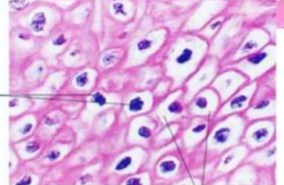
Chromophobe Renal Cell Carcinoma Microscopic Pathologic Features:
. Large polygonal cells with pale, eosinophilic cytoplasm and distinct cell borders (plant cell-like appearance)
. Perinuclear halos and coarse cytoplasmic granules
• Nuclei are irregular, often described as raisinoid
Chromophobe Renal Cell Carcinoma Microscopic Pathologic Features:
. Large polygonal cells with pale, eosinophilic cytoplasm and distinct cell borders (plant cell-like appearance)
. Perinuclear halos and coarse cytoplasmic granules
• Nuclei are irregular, often described as raisinoid

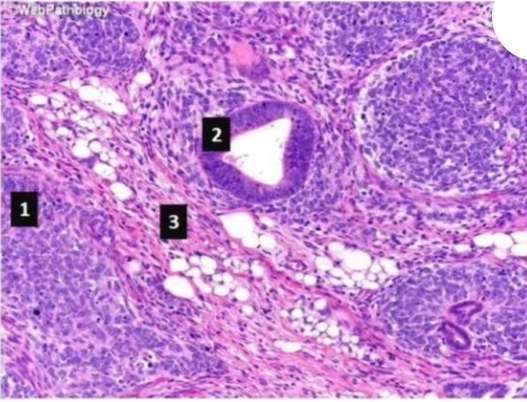
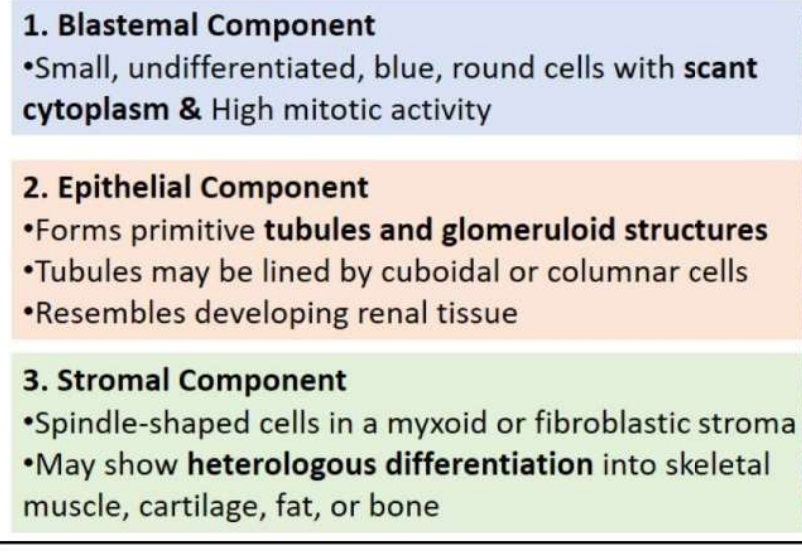
Wilms Tumor (Nephroblastoma)
• Gross Pathology
• Large, well-circumscribed mass that
can occupy the entire kidney
• Soft, gray-tan cut surface
• Areas of necrosis, hemorrhage, and
cystic degeneration are common
• Unilateral in most cases
& can be bilateral in syndromic cases

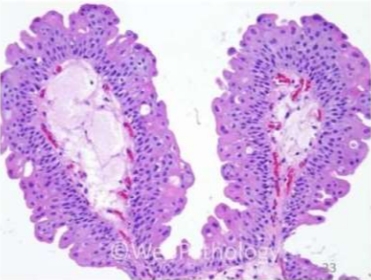
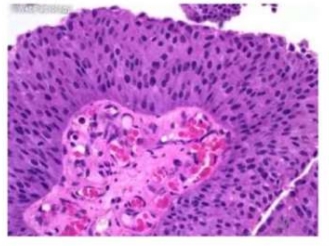
Urothelial Papilloma
• Benign tumor
. Gross Pathology:
• Small, exophytic lesion, usually <1 cm
. Located most commonly in the bladder
• Papillary, with a delicate fibrovascular core
• Microscopic Pathology:
• Orderly architecture with normal thickness of urothelium (3-7 layers)
No cytologic atypia
• Thin fibrovascular cores
Urothelial Papilloma
• Benign tumor
. Gross Pathology:
• Small, exophytic lesion, usually <1 cm
. Located most commonly in the bladder
• Papillary, with a delicate fibrovascular core
• Microscopic Pathology:
• Orderly architecture with normal thickness of urothelium (3-7 layers)
No cytologic atypia
• Thin fibrovascular cores
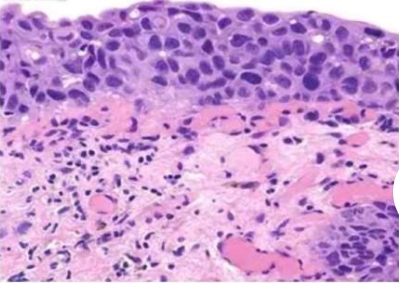
Urothelial Carcinoma in Situ (CIS)
•Flat, high-grade neoplasm confined to the
urothelium.
• Microscopic Pathology:
• High-grade cytologic atypia with disorganized
architecture
• Enlarged, hyperchromatic nuclei with prominent
nucleoli
• Frequent mitotic figures, including atypical forms
• Lack of maturation from basal to superficial layers

Exophytic Papillary Bladder Carcinoma
Gross Pathology:
• Multifocal exophytic Papillary masses with soft, friable appearance

Endophytic Infiltrative Bladder Carcinoma
Gross Pathology:
• Ulcerative mass infiltrating bladder hemorrhage
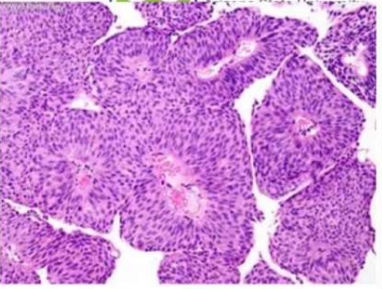
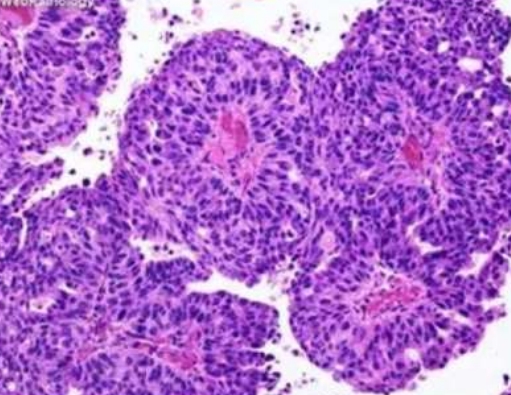
4. Low-Grade Papillary Urothelial Carcinoma
Microscopic Pathology:
• Papillary structures with very thin
fibrovascular core.
• Each papilla is covered by malignant
transitional epithelium (more than seven
layers) with:
• mild cvtologic atvpia
• Preserved polarity and architecture
• Nuclei are slightly enlarged, with irregular
contours but without prominent nucleoli
.
Low mitotic activity
4. Low-Grade Papillary Urothelial Carcinoma
Microscopic Pathology:
• Papillary structures with very thin
fibrovascular core.
• Each papilla is covered by malignant
transitional epithelium (more than seven
layers) with:
• mild cvtologic atvpia
• Preserved polarity and architecture
• Nuclei are slightly enlarged, with irregular
contours but without prominent nucleoli
.
Low mitotic activity
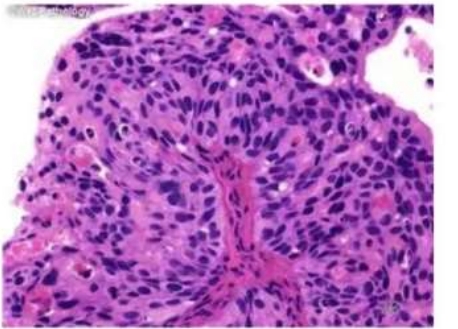
5. High-Grade Urothelial Carcinoma
Microscopic Pathology:
Marked nuclear atypia, loss of polarity, and frequent mitoses
• High nuclear-to-cvtoplasmic ratio
• Irregular, hyperchromatic nuclei with prominent nucleoli
• Invasive component often present, infiltrating the lamina propria or muscularis propria
• Variants: Micropapillary, sarcomatoid, plasmacytoid, nested
5. High-Grade Urothelial Carcinoma
Microscopic Pathology:
Marked nuclear atypia, loss of polarity, and frequent mitoses
• High nuclear-to-cvtoplasmic ratio
• Irregular, hyperchromatic nuclei with prominent nucleoli
• Invasive component often present, infiltrating the lamina propria or muscularis propria
• Variants: Micropapillary, sarcomatoid, plasmacytoid, nested
High-Grade Urothelial Carcinoma
• Microscopic Pathology:
Invasive component
Lamina Propria