Chiro Clinic OSCE Revision
1/53
Earn XP
Description and Tags
Everything from Med Exam, to Motion Palp.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
54 Terms
Cardiovascular Exam - Inspection (hands, fingers and nails)
Temperature - Observe the gradient from hands up along arms.
Colour - Observe for any cyanotic changes (blue), palmer erythema (red) or carotenemia.
Nail Beds - Assess the capillary return as well as observe any splintering haemorrhages
Clubbing - Shamroth’s sign looking for loss of diamond spacing.
Cardiovascular Exam - Inspection (Eyes)
Sclera - Observing for any jaundice (yellow) or anemia (excess whiteness on the eye lids)
Xanthlesama - Any yellow cholesterol deposits around the eyes
Cardiovascular exam - Inspection (face)
Malar flush - Any redness in the face which might be an indication of either pulmonary hypertension or mitral stenosis
Teeth infections - any signs of being a source of endocarditis (poor hygeine)
Tongue and Lips - any signs of central cyanosis
Cardiovascular exam - Inspection (Chest)
Scars: Scars may indicate defibrillator box or pacemakers
Cardiovascular exam - JVP
Patient lying supine, 30° angle on the table, have them look left to expose the right jugular vein (just posterior to SCM).
Measure the height of the pulsations in relation the the sternum.
Normal is above 3cm with 30° elevation.
If at height of sternum, pt may be hypovolemic
If at height of the jaw, pt may be hypervolemic
Cardiovascular Examination - Palpation (Neck)
Carotid pulse: Assessing the rate and character of the pulse as well as any vibrations which may indicate thrills (turbulent blood flow)
Cardiovascular examination - Palpation (Chest)
Assessing the 2LICS (Pulmonic) and 2RICS (Aortic) as well as the 5LICS (tricuspid) and the 5LICS in midclavicular line (mitral)
Heaves - feeling for any protrustions through the chest wall may be a sign of ventricular dilitation
Thrills - using ball of your hand, feeling for any vibrations which may indicate turbulent blood flow
Determine the location of the apex beat (PMI) location which will be where the Mitral valve is
Cardiovascular Exam - Auscultation
Diaphragm - begin at aortic area, noting cardiac rate and rhythm. S2 will be louder than S1 at aortic and pulmonic. Diaphragm will be better for Aortic and mitral regurgitation as well as any pericardial friction rubs.
Pulmonic inspiratory split - Ask the pt to breath in to identify inspiratory splitting of S2. A2 being the closure of the aortic valve, P2 being pulmonic valve closure. In expiration they will fuse into one sound.
Going further down - S1 will begin to get louder and S2 will diminish the further you go down the heart
Bell - Using the bell listen at tricuspid and mitral for any potential murmur of mitral stenosis
Respiratory Exam - Inspection (Fingers, Hands and Nails)
Temperature - Grading temperature starting at hands up along the arms
Colour - Observing any cyanosis (blue), nicotine stains, erythema (red) or Carotenemia (orange).
Nail Beds - Assessing capillary return as well as any splintering haemorrhages.
Clubbing - Shamroth’s sign looking for loss of diamond spacing.
Respiratory Exam - Inspection (face)
Respiratory Rate - Noting respiratory rate (norm. 12-20 Breaths/min)
Respiratory Effort - Any usage of accessory Muscles
Malar Flush - Any signs of redness from pulmonary hypertension or mitral stenosis
Teeth infections - Observing teeth for dental hygiene. Decay may be a sign of endocarditis
Tongue and lips - assessing for any central cyanosis
Respiratory Exam - Inspection (Eyes)
Sclera - Looking for any signs of jaundice (yellow) or Anaemia (excess whitening)
Xanthelasma - Yellow cholesterol deposits around the eye
Respiratory Exam - Inspection (Chest)
Respiratory effort - retraction of interspace
Scars - defibrillator box or pacemaker
Skeletal abnormalities - kyphoscoliosis, pectus excavatum or barrel chest
Symmetry of respiratory movements
Tracheal Deviation
Respiratory Exam - Palpation (Neck)
Cervical nodes - Feeling for any enlargements of the cervical nodes
Tracheal Deviation - Observe if the trachea deviates at all by palpating the sternal notch
Respiratory Exam - Palpation (Chest)
General Tenderness - palpate across the chest wall for any general tenderness
Lateral Expansion - Have thumbs at aronud level of T10. Ask pt to inhale and exhale and observe the range, symmetry and distance between your thumbs
AP Expansion - Inspect expansion front and back, feeling for symmetry
Supraclavicular and Axillary nodes - Feeling for any enlargements or tenderness
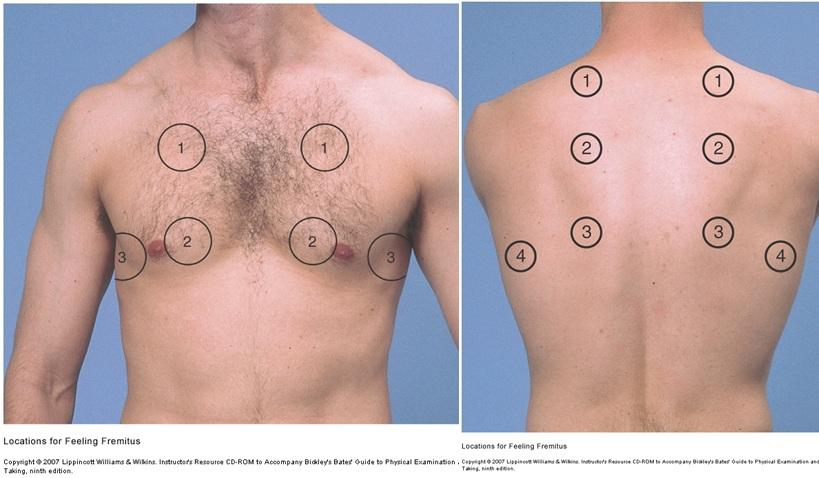
Respiratory Exam - Palpation (Posterior and Anterior Wall)
Tactile Fremitus - Instruct Pt to say ‘99’ in each of these areas. Feeling for any increased vibration (excess tissue ie. mass or consolidation) or decreased vibration (Excess air ie. asthma/emphysema)
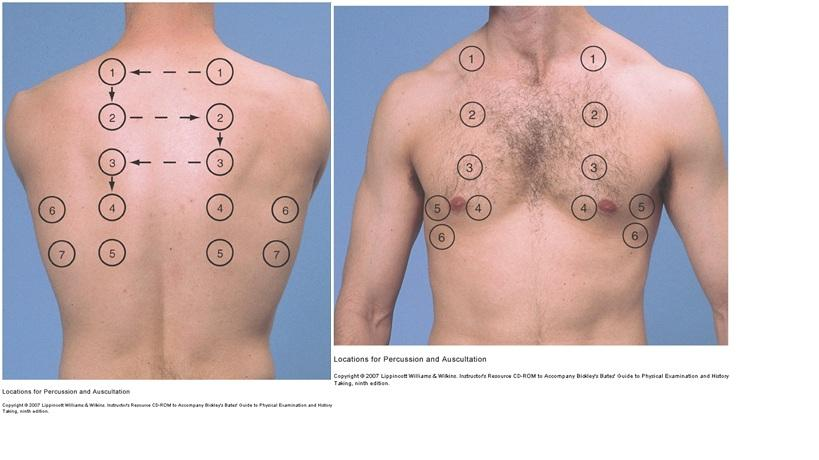
Respiratory Exam - Percussion
Intercostal spaces - Percussion along intercostal spaces in a ‘ladder’ pattern listening for changes
Normal Lungs are resonant - hyperresonance may signify COPD or asthma from air trapped in alveoli
Abnormal dullness - underlying dullness or pleural effusion
Diaphragm excursion - Instruct pt to breath out and percuss to find higher level of diaphragm. Then instruct to breath in and measure the lower point. Distance between them should be 3-5cm
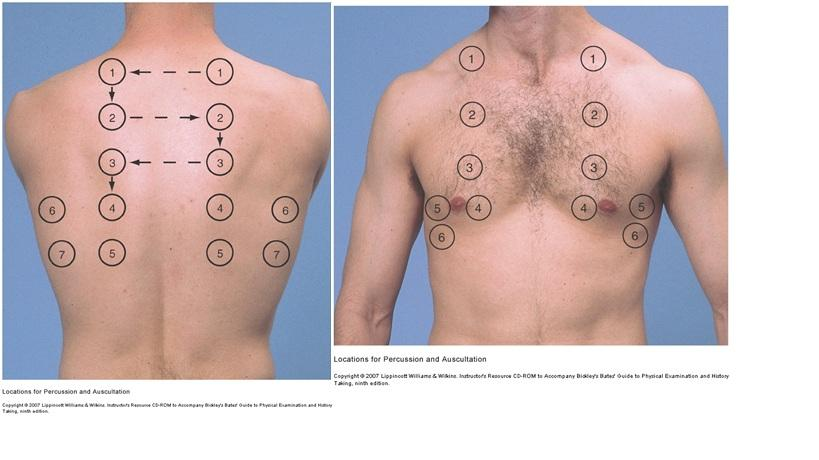
Respiratory exam - Auscultation (breath sounds)
Begin by asking pt to clear airway by coughing
Listening for:
Adventitious breath sounds - crackles, ronchi, wheezing
Sounds generated from breathing
Vesicular - Soft and low pitched
Bronchovesicular - intermediate pitch and intensity
Bronchial - harsh and high in pitch
Respiratory exam - Auscultation (Vocal Fremitus)
Bronchophony - instruct pt to say 99. Should sound muffled. If clear, suspect increased tissue
Egophony - Instruct Pt to say E. Will change to sound like an A if consolidated tissue
Whispered pectoriliquy - Pt to whisper 1,2,3. Should only faintly hear it. Underlying consolidation if heard clearly
Abdominal Exam - Inspection (Nails and hands)
Leukonychia - White spotting on nails
Koilonychia - Spoon shaped nails
Clubbing - Shamroth’s Sign
Palmer erythema (redness) or pallor (whiteness)
Asterixis - Jerking hands while asked to hold position
Abdominal Exam - Inspection (Arms and Face)
Bruising & ecchymoses (Black/purple brusing)
Petechia - pinpoint spots caused by capillary bleeding
Hair Loss
Bronzing or Jaundice
Sclera Jaundice
Abdominal Exam - Inspection (Mouth, Teeth and Gums)
Pigmented Lesions
Fetor Hepaticus - Sweet breath of severe liver disease)
Gum hypertrophy
Aphthous ulcers - Sign of underlying systemic disease
Candidiasis - Fungal infection, curd patches in the mouth
Glossitis - Smooth, red tongue
Leucoplakia - White-coloured tongue thickening, pre-malignant
Abdominal Exam - Inspection (Torso)
Supraclavicular nodes - enlarged or tender
Gynaecomastia (male breast prominence)
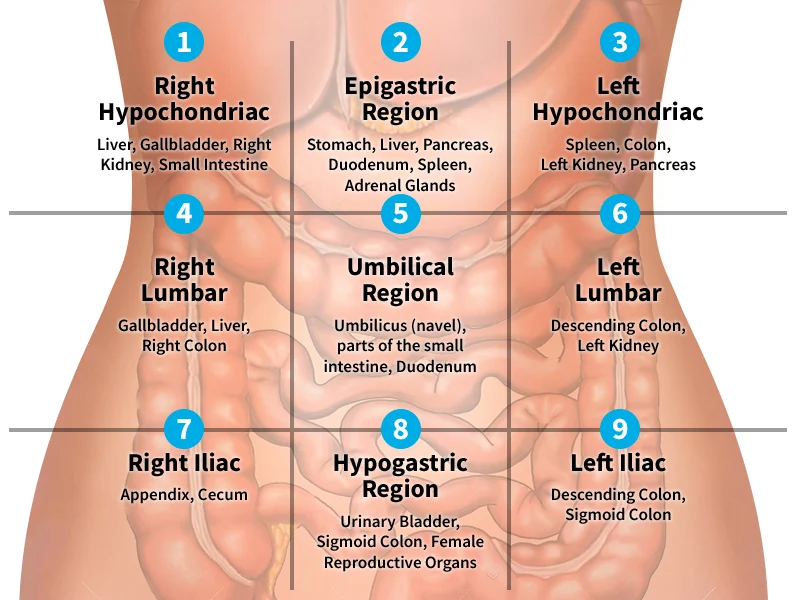
Inspect the abdomen for size, shape, symmetry, lesions, colour and movement
Abdominal Exam - Auscultation
Bowel Sounds - Listening to each region/quadrant for any abnormal bowel sounds (high pitched sounds)
Bruits - Listen for bruits over each of the following:
- Abdominal Aorta
- Renal (L&R)
- Common Iliac (L&R)
Abdominal Exam - Percussion
Percuss over each of the quadrants listening for tympany (Hollow) or dullness (fluid or oragn)
Percuss liver span - Along midclavicular line, go up until tympany turns to dullness to identify bottom of liver. Begin at the nipple line and go down till lung dullness turns to liver for top of the liver.
Abdominal Exam - Palpation
Light Touch - Ask patient to flex the knees and mouth breath. Using a light dipping motion, go through each region observing for tenderness, or increased resistance. Observe patients face too for apprehension
Deep touch - Pressing harder for any masses or tenderness. Watch for any signs of peritonitis
Palpate each of the following structures:
- Liver: one hand under and move soft tissues surrounding rib 11 & 12. One hand on top just under ribs and lateral to transverse abdominus
- Spleen: Standing on Pt’s right side, reach across, scoop under and press up on left lower rib cage. Other hand under left costal margin feeling for any enlarged spleen. Would typically be unable to palpate otherwise.
- Aorta: Deep in upper abdomen feeling for width (should be less then 3cm), and assess for any thrills
- Kidneys: Below ribs, place hands on top and below patient to ballot each kidney. Typically unable to palpate
Abdominal Exam - Special Tests (appendicitis)
McBurney’s Point - pain found 2 inches from ASIS toward umbillicus
Rebound Tenderness - Press down on an area of tenderness. Ask the Pt if the pressing down hurts more or removing the hand hurts more. Positive if hurts more when hand removed
Rosving’s sign - Press down onto lower left quadrant. Positive if pain refers to lower right quadrant
Psoas sign - Ask patient to raise their leg. Make them resist hip extension. Positive will be pain illicited.
Abdominal Exam - Special Tests
Murphy’s Sign - Deep pressure under the liver on inspiration sign of acute cholecystitis
Valsalva test - sign of hernia
Shifting Dullness - Assesses for ascites. Percuss border of tympany and dullness then instruct pt to roll over toward you. Percussive notes will stay relatively the same in average patients.
Peripheral Vascular and lymphatic system Exam - inspection
Neck - Observing the neck vessels as well as any enlarged nodes
Hands and Feet - Swelling, colour or hair loss
Peripheral Vascular exam - palpation
Temperature gradient - assess along the arms
Contact each of the following pulses and assess their rate, character and any thrills:
- Radial, Ulnar and brachial
- Carotid
- Abdominal aorta
- Femoral, popliteal, posterior tibial and dorsalis pedis
Peripheral Vascular exam - Auscultation
Listen for bruits at the radial, carotid, abdominal aorta and dorsalis pedis for any turbulent sounds (whooshing)
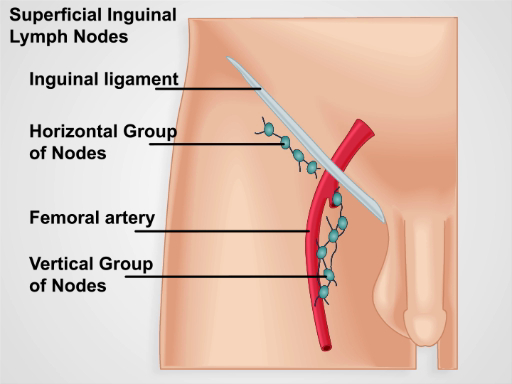
Lymphatic Exam - Palpation
Palpate each of the lymph nodes for any enlargements or tenderness:
- Epitrochlear, Axillary
-Submental, Submandibular, Tonsillar, Pre-auricular, post-auricular, suboccipital, anterior cervical chain, supraclavicular and posterior cervical chain
- Inguinal: Horizontal and vertical chain
Peripheral vascular Exam - Special Tests
Capillary Reperfusion - check nails on feet and hands
Allen Test - Hold arm up and out to side, occluding radial and ulnar artery, clench fist then observe paleness changing to red when releasing either radial or ulnar artery.
Leg elevation - Patient supine, lift their leg up and instruct them to pump their calf, observe whiteness in leg. Swing their leg around and instruct them to sit up and observe colour come back to foot
Eye Exam - inspection
Sclera and conjuctiva - observe for any colour changes
Cornea and lens - Hold pen light on an angle looking for an opacities through the lens
Pupil Size
Eye Exam - Palpation
Nasolacrimal Gland duct - Palpate and observe any swelling or excess tearing
Eye Exam - Visual Function
Visual Acuity - Have patient stand 6 metres away from snellens chart. Cover one eye and instruct them to read it out. Same for other eye
Visual Fields - Stand in front of patient, cover one eye and you close yours. Mimic the visual field and wiggle your finger asking them when they can see it
Light Reflex - Direct and Consensual reflex when light shined in the eye
Accomodation - Have them look at tip of pen, then wall, back to pen. Observe for convergence
6 Directions of gaze - Make a H in the air watching their eyes. Looking for nystagmus.
Eye exam - Opthalmoscopy
Ensure Left hand, left eye while looking at their left eye. Vice Versa
Red Reflex - Red glow when first looking through ophthalmoscope
Optic Disc - follow retinal vessels centrally to the disc. Observe:
- Colour, Size and shape
- Clarity of disc margin
- Physiological cup - should be cup to disc ratio 3:1
- Swelling (paplidema)
Retina - Observe it’s colour
Macula and Fovea - Ask patient to look directly into the light to see fovea and surrounding macula shape and colour
Ear Exam - Inspection
General Appearance
Lesions, lumps or discharge
Ear Exam - Palpation
Auricle, Tragus and mastoid process for any tenderness or swelling
Auricle Tug test for otitis externa
Ear Exam - Otoscopy
Ear Canal - Any Wax, discharge, Foreign bodies, redness and swelling
Ear Drum - Observe the pars flaccida, pars tensa, cone of light and malleus
Ear Exam - Auditory Acuity
Whispered voice - whisper in one ear while other is covered. Get pt to repeat back what is said
If this is failed go onto:
Weber test - hold tuning fork on head, ask if it’s heard equally on both side
Rinne Test - Place tuning fork on mastoid. when they can no longer hear it through bone, move it to the ear ask if they can still hear it.