ANAESTHETICS
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
3 scores commonly used to assess risk
1. ASA scoring
2. SORT
3. P Possum
what is the ASA scoring in anaesthesia
ASA I: A normal healthy patient without any clinically significant past or present medical history.
ASA II: A patient with mild systemic disease.
OR if patient has a BMI between 30-40
ASA III: A patient with severe systemic disease, which is poorly controlled.=
ASA IV: A patient with severe systemic disease that is a constant threat to life.
ASA V: A moribund patient (dying) who is not expected to survive without the operation.
ASA VI: A declared brain-dead patient whose organs are being removed for donor purposes.
how is the SORT score used to determine risk in a surgery?
- it is used to predict risk of 30-day mortality in patients undergoing non-neurological and non-cardiac surgery.
- does not take into account intra operative variables
how is the P POSSUM score used to determine risk in a surgery?
- 12 physiological variables (patient factors like preoperative blood test results)
- 6 operative variables (surgical factors like blood loss)
- used to calculate 30 day mortality and morbidity post surgery
AIRWAYS - what devices can be used
Supraglottic airways e.g LMA I-gel
infraglottic airways - e.g endotracheal tube (ETT)
mask ventilation
types of ventilation
1. Non-Invasive Ventilation (NIV)Positive pressure via mask (e.g., CPAP, BiPAP); no airway needed.
2. Invasive VentilationPositive pressure via endotracheal/tracheostomy tube; requires airway insertion.
What happens to respiration during anaesthesia?
↓ FRC → leads to atelectasis and shunting
↓ Tidal volume and minute ventilation
↑ V/Q mismatch, ↓ oxygenation
Central respiratory drive suppressed
Mechanical ventilation often needed
to treat the atelectasis post op- do chest physio
CRITICAL CARE
- features on ward
- many staff to patient ratio
- special equipment to provide organ support
FLUID - what are the main types?
1. crystalloid
2. colloid (contains large insoluble molecules)
FLUID - what are the 4 Rs
- Routine maintenance
- Replacement
- Redistrubution
- Resuscitation
FLUID - what are our daily requirements
Water: 25–30 ml/kg/day
Sodium (Na): 1 mmol/kg/day
Chloride (Cl): 1 mmol/kg/day
Potassium (K): 1 mmol/kg/day
Glucose: 50–100 g/day
Urine output: 0.5 ml/kg/hr
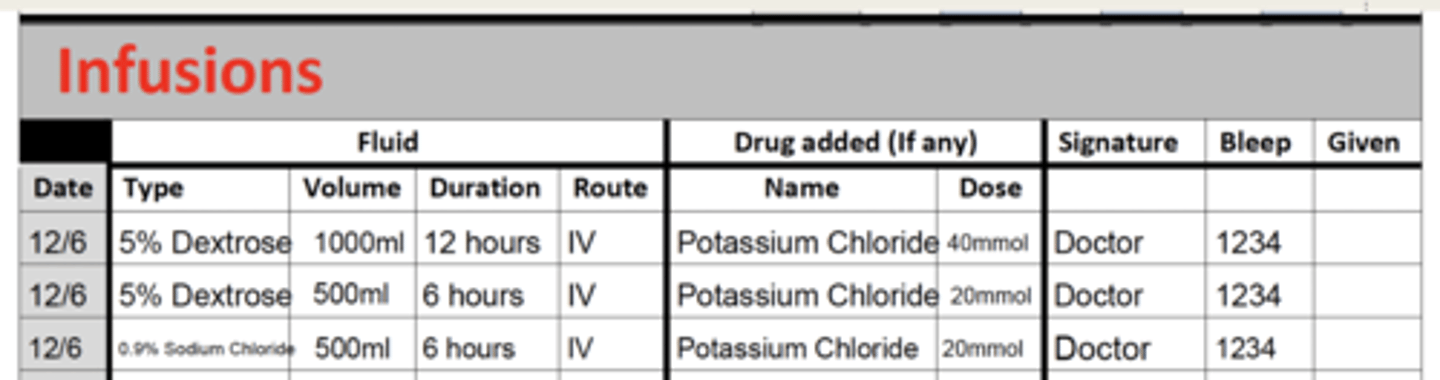
FLUID - how to prescribe maintenance fluids
- adults need around 2000 L of water
- need 50-100g of glucose
- 1mmol/kg/day of the electrolytes (potassium is only given in 20 or 40 mmol bags)
FLUID - how do you assess fluid status?
refer to the fluid status exam.
but the main things:
From end of bed – Look around for clues (e.g. urine bag, fluid restriction signs).
Speak to patient – Are they thirsty?
Measure the pulse – Tachycardia may indicate dehydration or fluid overload.
Test capillary refill time – >2 seconds indicates poor peripheral blood supply.
Assess skin turgor
Measure BP lying and standing – Postural drop >20 mmHg suggests dehydration.
Assess the JVP – Elevated in fluid overload, low in dehydration.
Face – Do the eyes appear sunken?
Mucus membranes – Inspect mouth and tongue for moisture.
Auscultate the lungs – Pulmonary oedema in severe fluid overload; fine inspiratory crackles in the bases.
Look for pitting oedema – In sacrum and ankles; linked to fluid overload, right heart failure, and low protein states.
OBs Chart – Check fluid balance, BP and pulse trends, and possible pyrexia.
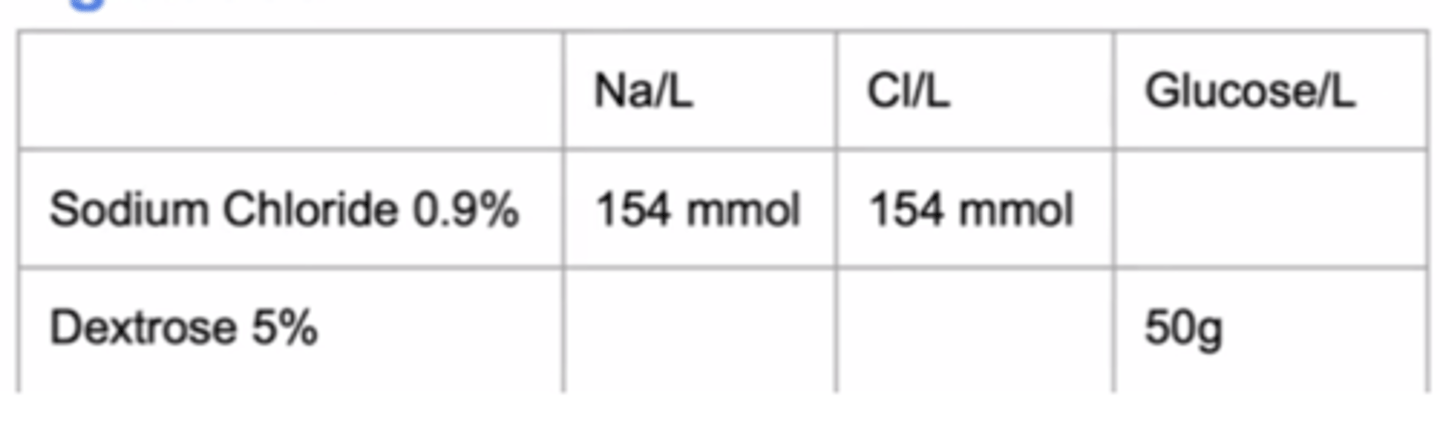
FLUID - what is in 1L 0.9% sodium chloride and 5% dextrose fluids
FLUID - in what cases do you need to adjust the amount of fluid (replace or redistribute)
- Electrolyte abnormality
- Vomiting/diarrhoea (dehydration)
- Kidney failure
- Heart failure
- Sepsis
- Fluid overload
FLUID - what do you prescribe in a resuscitation scenario (e.g SHOCK)
Administer 500 mL of 0.9% sodium chloride without potassium or Hartmann’s over 15 minutes (250 mL if there is left ventricular impairment). Reassess and repeat 250–500 mL over 15 minutes as needed, up to a total of 2000 mL.
PAIN - how do we treat pain medically?
"treat pain in a stepwise manner using multimodal analgesia with the WHO pain ladder":
1. simple analgesia (paracetamol)
usual dose: 1g every 4 hours
max 4 times a day
2. NSAID (ibuprofen)
usual dose: 400mg 3-4 times a day
cautions
1 dont take on empty stomach because of risk of peptic uclers
2 dont give if hypovolaemic (because impairs renal blood flow)
3 dont give if renal failure
4 dont give in asthma
5 dont give in heart disease (can increase risk of cardiac event)
3. weak opioid e.g codeine sulfate, dihydrocodeine
usual dose: 30mg 3-4 times a day
*some people are fast metabolisers and some people are slow metabolisers
side effects
- constipation (so give lactulose alongside)
- dizziness (so say to sit down when consuming)
- N/V
4. strong opioid (morphine, fentanyl)
alongside, always prescribe :
- oxygen
- PRN naloxone
- antiemetic
- regular laxative
** on the ward, morphine is always prescribed as PCA (patient controlled analgesia)
OTHER DRUGS
- antidepressants (amitriptyline)
- anticonvulsants (pregabalin, gabapentin)
- nitrous oxide
- tramadol
- ketamine
PRE-OP how do you assess fitness for surgery
can you climb one flight of stairs with no SOB, Pain etc?
PRE-OP what drugs do you stop/continue?
- antihypertensive
most drugs you CONTINUE, but ACE inhibitors, you STOP the morning of
- anticoagulants
- mostly you STOP these, but depends why they are on them
e.g warfarin stop 5 days before and go on LMWH
- if on DAPT, discuss with cardiology
diabetes drugs are a bit complex:
metformin
OD or BD: take as normal
TDS: miss lunchtime dose
assumes only one meal will be missed during surgery, eGFR > 60 and no contrast during procedure
( so metformin generally given the morning dose)
gliclazide (sulfonylureas)
omit the morning of the surgery
steroids
increase steroid dose peri-op to prevent addisonian crisis
PRE-OP when do you stop eating or drinking?
eating - 6 hours before
drinking - 2 hours before
milk counts as solid food lol
PRE-OP tests
if minor op - no routine tests are really needed
UBEXS
- urine (e.g pregnancy)
- bloods - group and save in case of transfusion requirement! (important!)
following are not needed usually, but can be useful if indicated:
- ECG
- X-ray
- Special tests e.g echo?
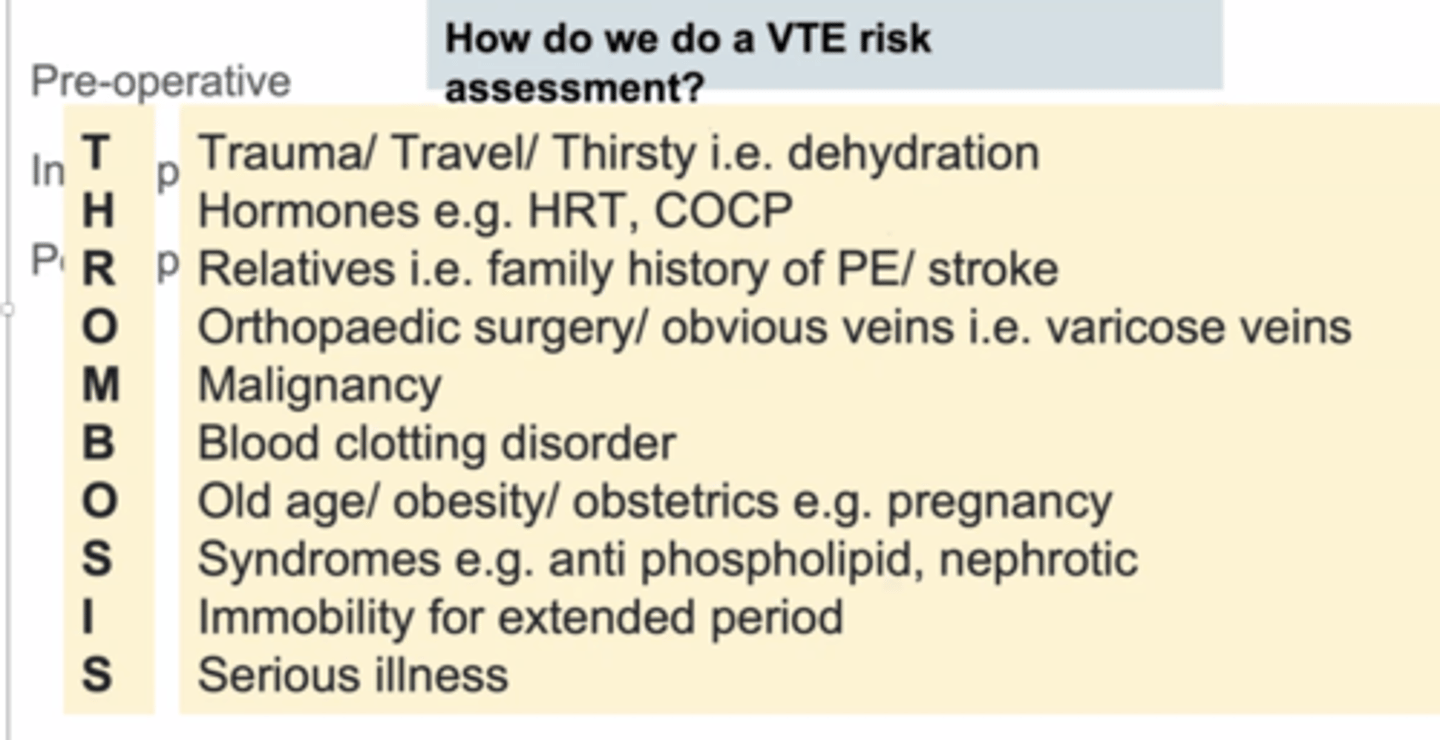
PRE-OP - how do you do a VTE risk assessment?
INTRA-OP what is the triad of drugs
Hypnosis -
- propofol (IV) or
- sevofluorane (inhaled)
- use ketamine in haemodynamically unstable patients.
Analgesia
- fentanyl (used during induction of anaesthesia)
- morphine (used during maintenance of anaesthesia)
Muscle relaxation
- depolarising agents e.g suxamethonium (initially cause muscle contraction and then cause muscle relaxation)
- non-depolarising agents e.g rocuronium (competitively inhibit acetylcholine receptors)
what is the RYR1 mutation
this is a gene that can cause malignant hyperthermia triggered by certain anaesthetic agents. It results in sustained muscle contraction, increased metabolism, and a rapid rise in body temperature
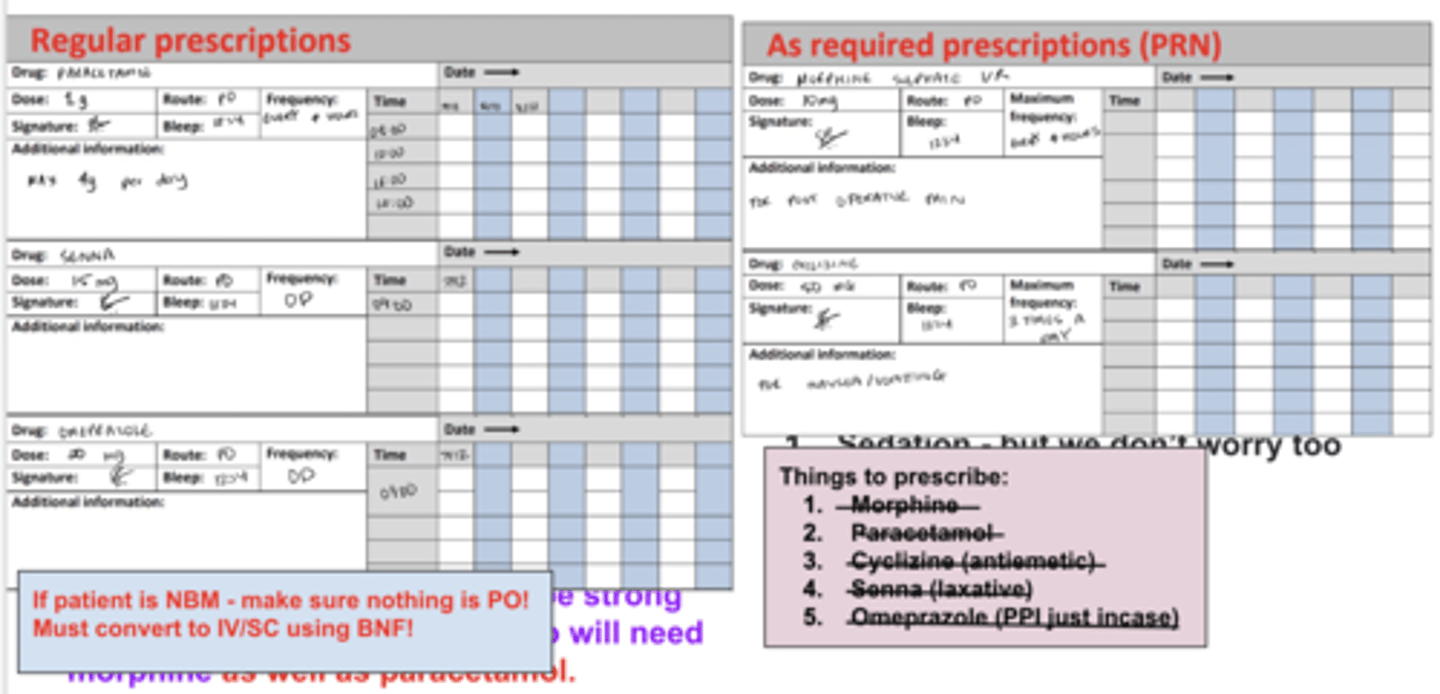
POST-OP what do you need to prescribe?
(WRITE OUT GRAMS AND MILLIGRAMS UNLIKE IN PIC)
FLUIDS - maintenance
THROMBOPROPHYLAXIS
ENOXAPARIN 40MG SUBCUT OD
REGULAR
Senna
15mg, PO ON
Omeprazole
20mg, PO OD
Paracetamol
1 gram, PO, QDS, max 4g a day
PRN - always put reason why
Morphine
10mg, PO, max dose every 4 hours
Cyclizine
50mg, PO, max 3 times a day
FT SOP MC
POST-OP what to do if reduced urine output?
500ml fluid challenge Hartmanns
BUT
if urine suddenly goes to 0,
check the catheter to ensure it hasn’t fallen out and that it’s patent with a ‘bladder washout’ (injecting then aspirating 50ml of sterile fluid)