4.2: filtration & absorption
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
20 Terms
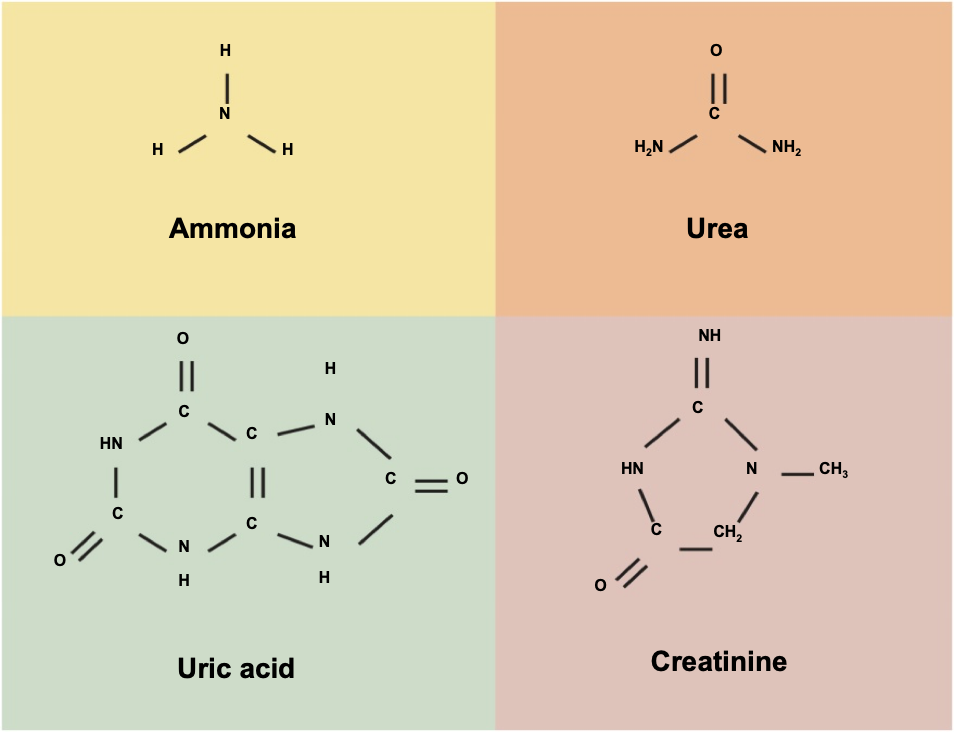
excretion of wastes
excretion separation & elimination of waste products
-nitrogenous wastes
stages of urine production
glomerular filtration
majority of PLASMA pushed out of capillaries
tubular reabsorption
necessary components returned to BLOOD
tubular secretion
other substances selectively added
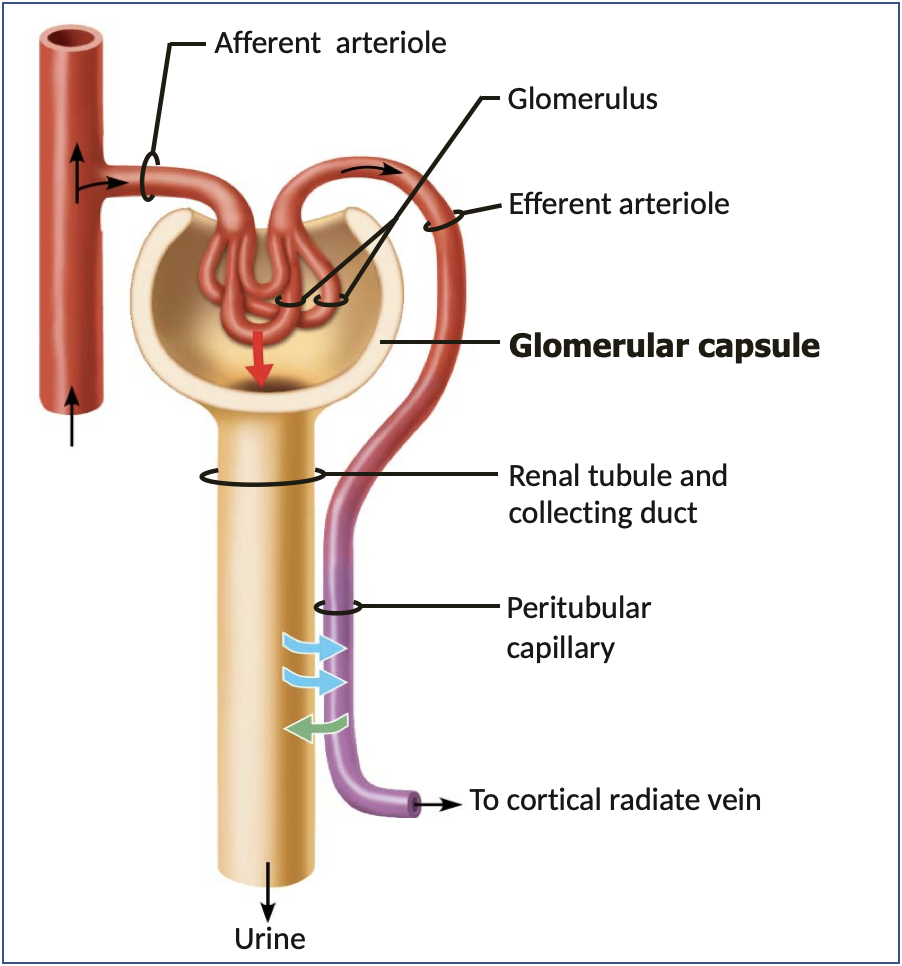
glomerular filtration
-water & solutes
-via
-water & solutes move from PLASMA into NEPHRON
-via hydrostatic pressure
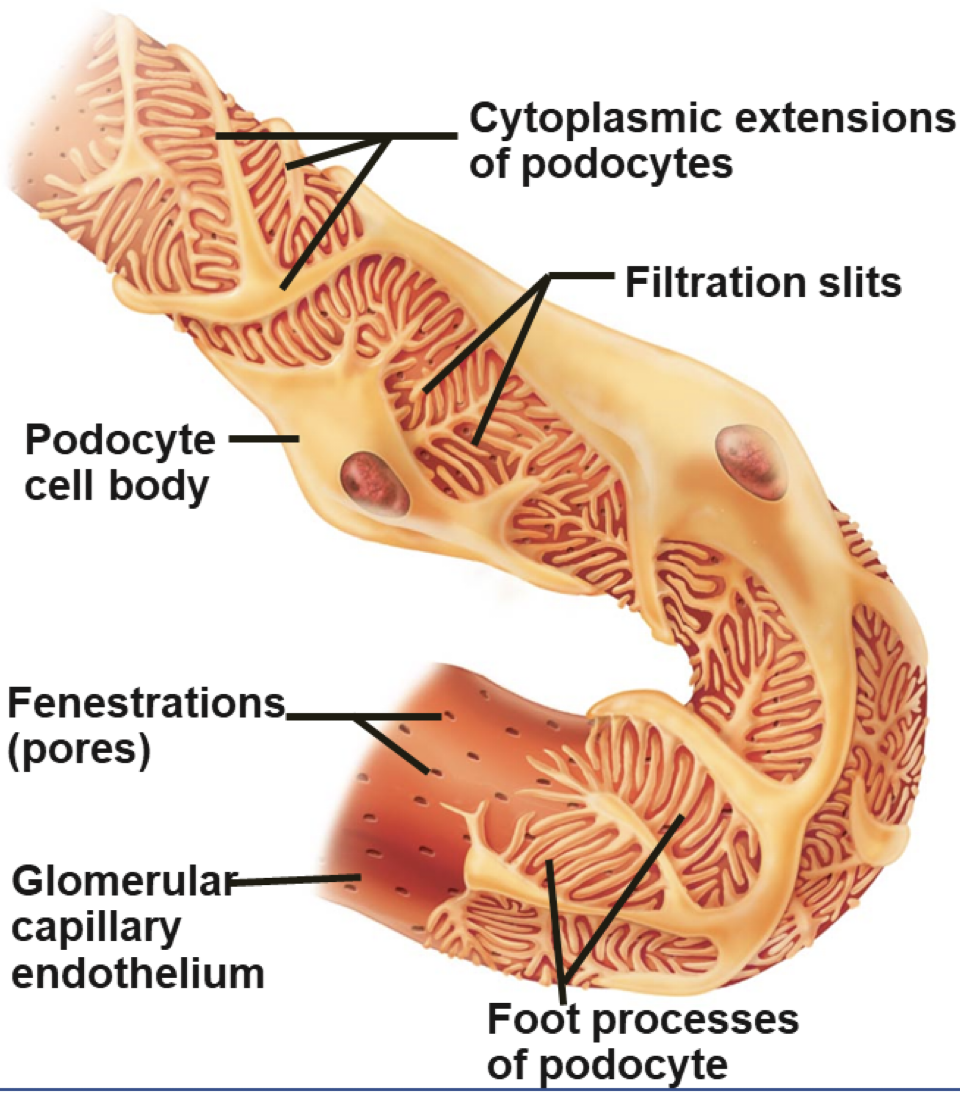
filtration membrane (pt 1)
capillary wall
basement membrane
capillary wall
fenestrated capillaries hold back blood cells & large proteins
basement membrane
holds back most large molecules
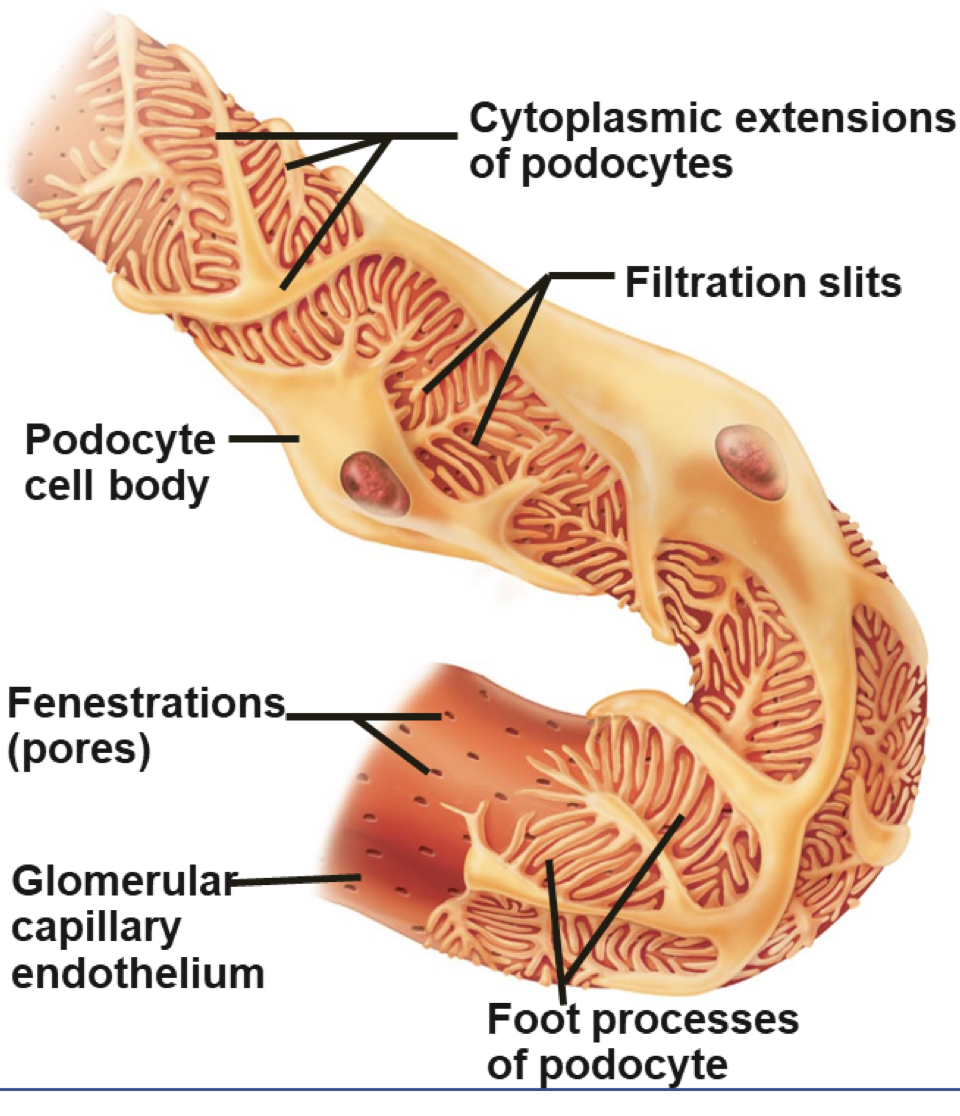
filtration membrane (pt 2)
filtration slits
-spaces between
-most ___ molecules
-unless
filtration slits
spaces between cells of visceral layer
most small molecules can pass through (like water, electrolytes, glucose, wastes)
unless bound to plasma proteins (like calcium, iron, thyroid hormone)
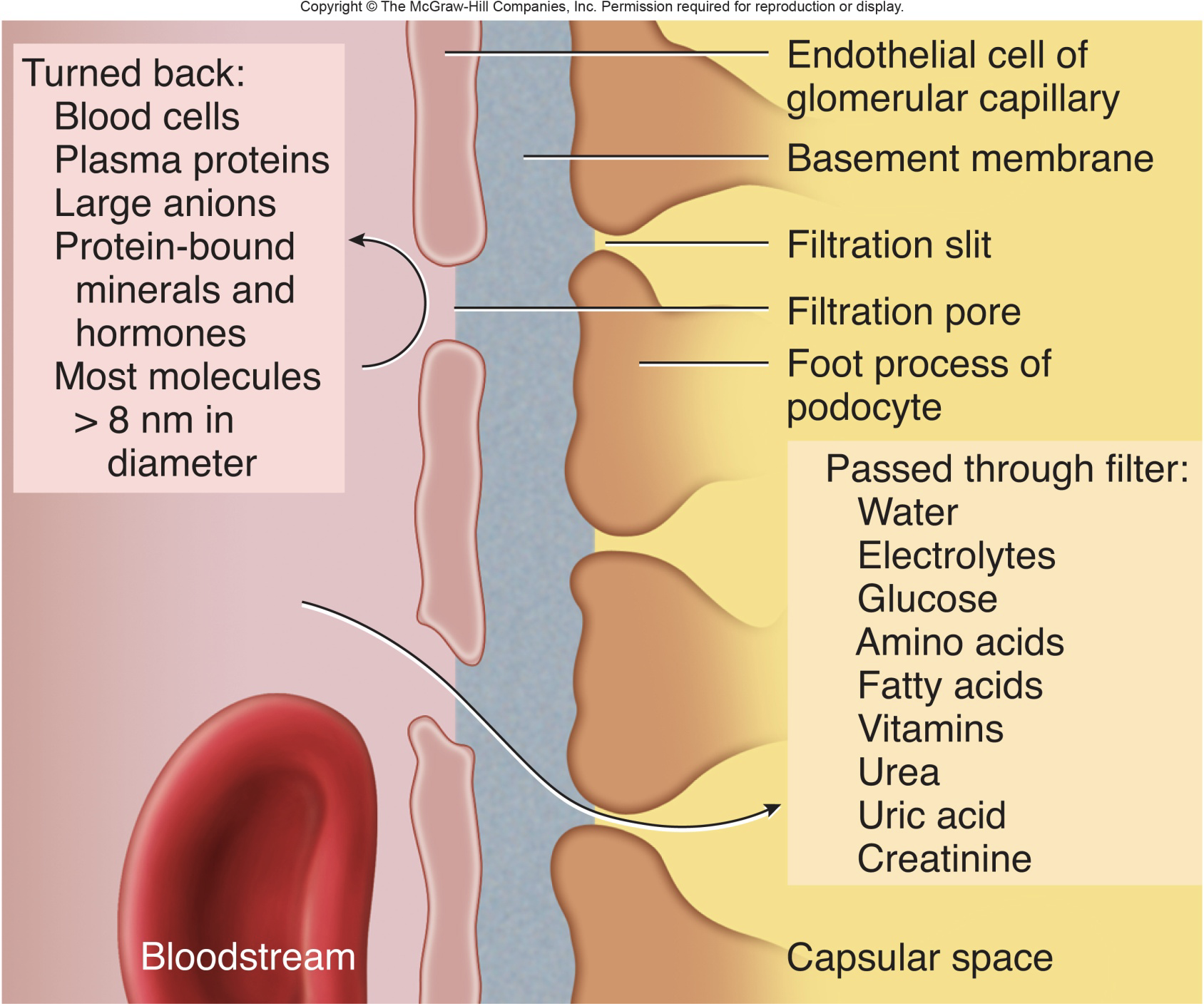
anything on left side would stay in circulatory system and not into urinary system
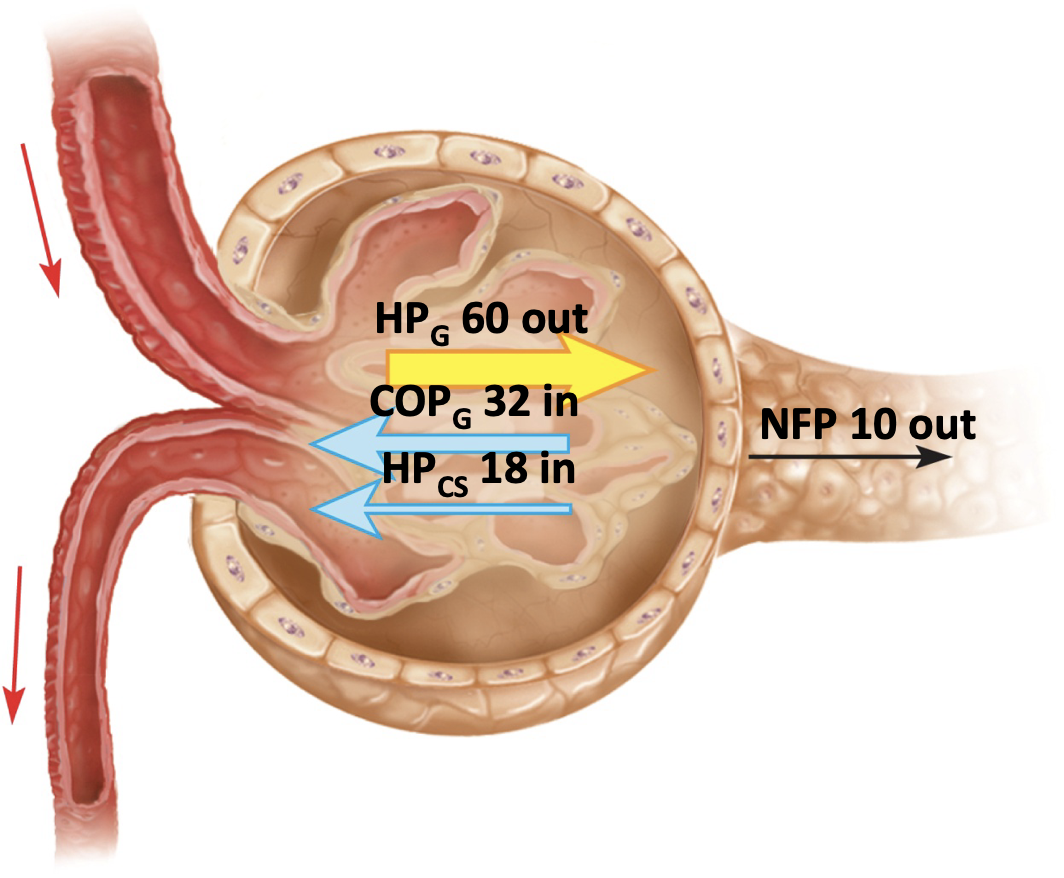
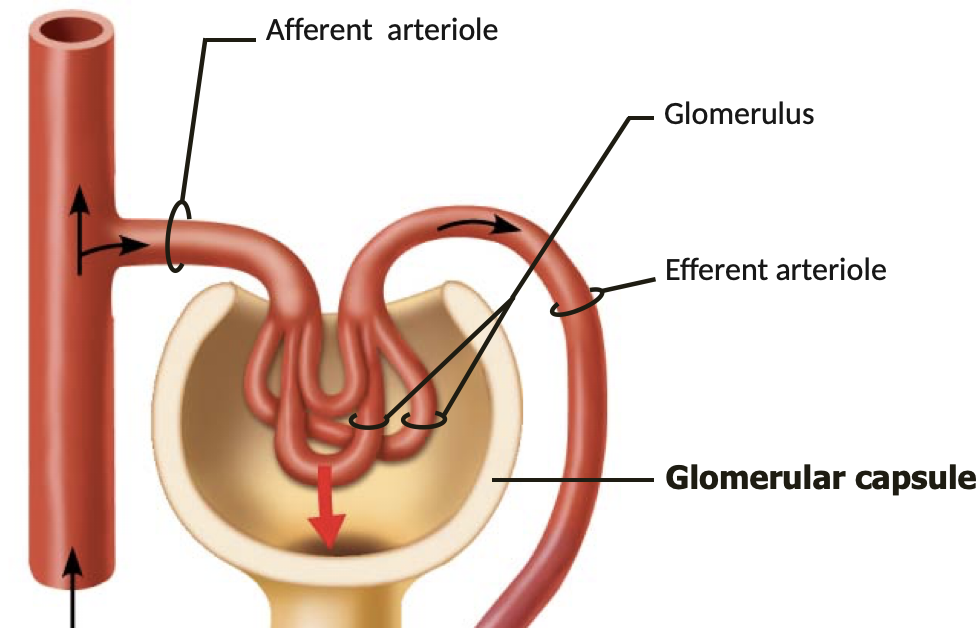
glomerular filtration pressure
-glomerular
→ driven
-outwards
-kidneys
-glomerular blood pressure is very high
→ driven by small diameter of EFFERENT arteriole
-outwards pressure always exceed inwards pressure → only filtration (FILTRATION = IN OR OUT OF TUBULE)
-kidneys very sensitive to hypertension
glomerular filtration rate (GFR)
-males: 125 mL/min or 180 L/day
-females: 105 mL/min or 150 L/day
-1-2L urine excreted daily
→ 99% of filtrate is reabsorbed
-amount of filtrate formed each minute by both kidneys
-GFR = NFP x Kf
→ NFP = net filtration pressure
the following makes up the filtration coefficient (Kf):
→ filtration membrane surface area
→ filtration membrane permeability
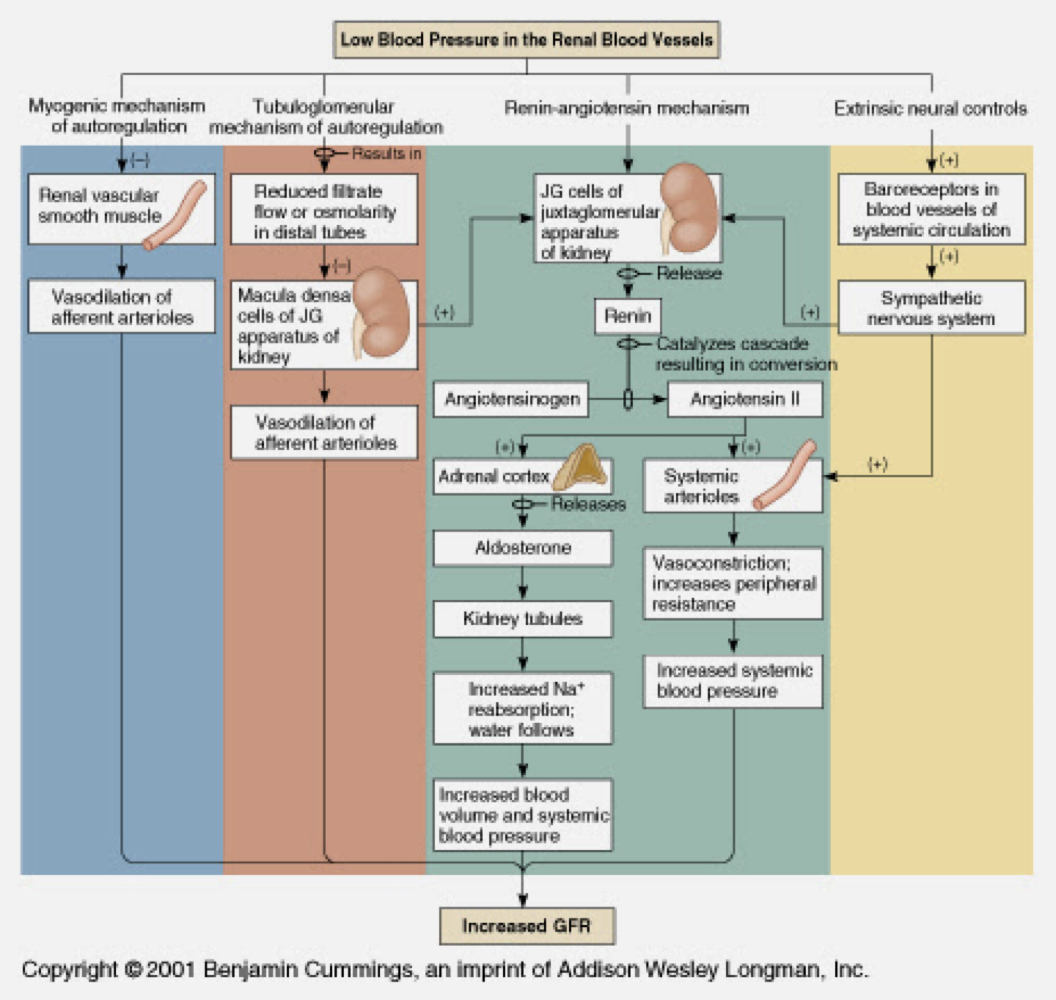
regulation of GFR
-GFR maintained by
-GFR maintained by adjusting glomerular blood pressure
-intrinsic controls: renal autoregulation
-extrinsic controls: nervous or hormonal regulation
intrinsic controls
-kidneys
→ activation
→ chemistry
-maintain
-kidneys regulate BP in response to internal stimuli:
→ activation of stretch receptors in afferent arteriole
→ chemistry of filtrate
-maintain dynamic equilibrium
extrinsic controls
-needed to
-neural control:
→ constricts
→ reduces
→ redirects
-needed to mediate larger changes in BP
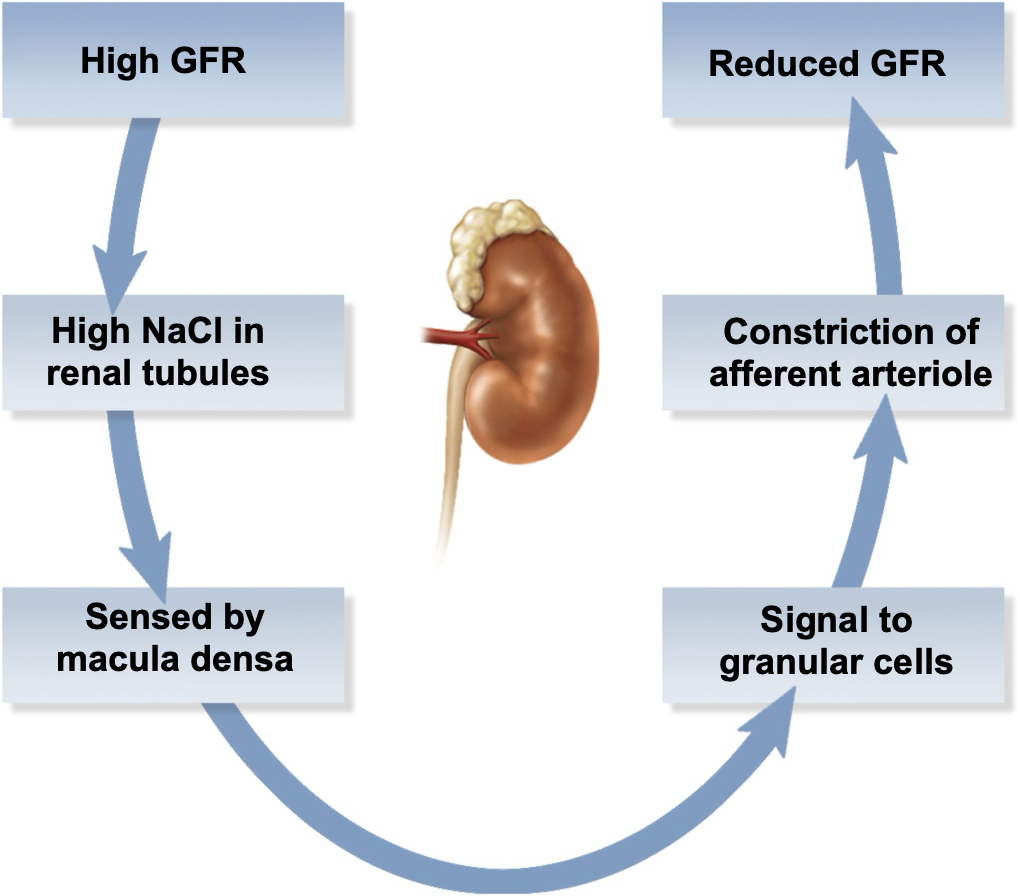
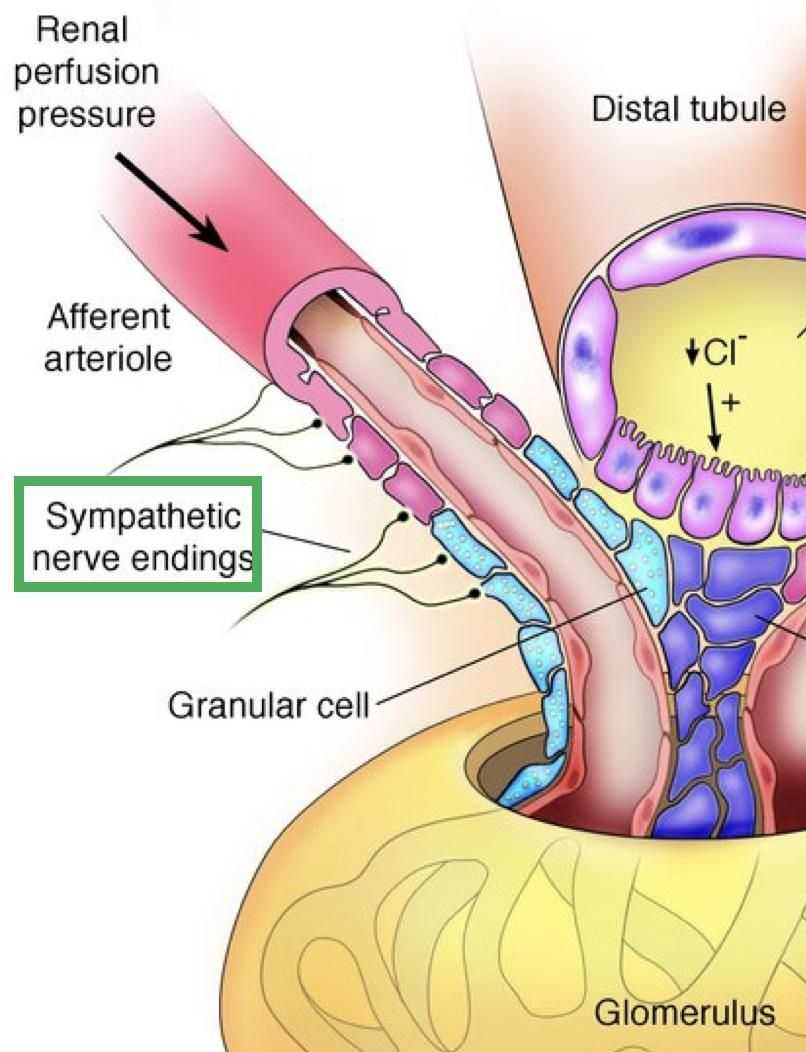
-neural control: sympathetic stimulation
→ constricts afferent arteriole
→ reduces GFR & urine output
→ redirects blood away from kidneys
extrinsic control: renin-angiotensin-aldosterone (RAA) mechanism
ie
-decrease
-granular
→ sympathetic
→ signal
→ decreased
-renin
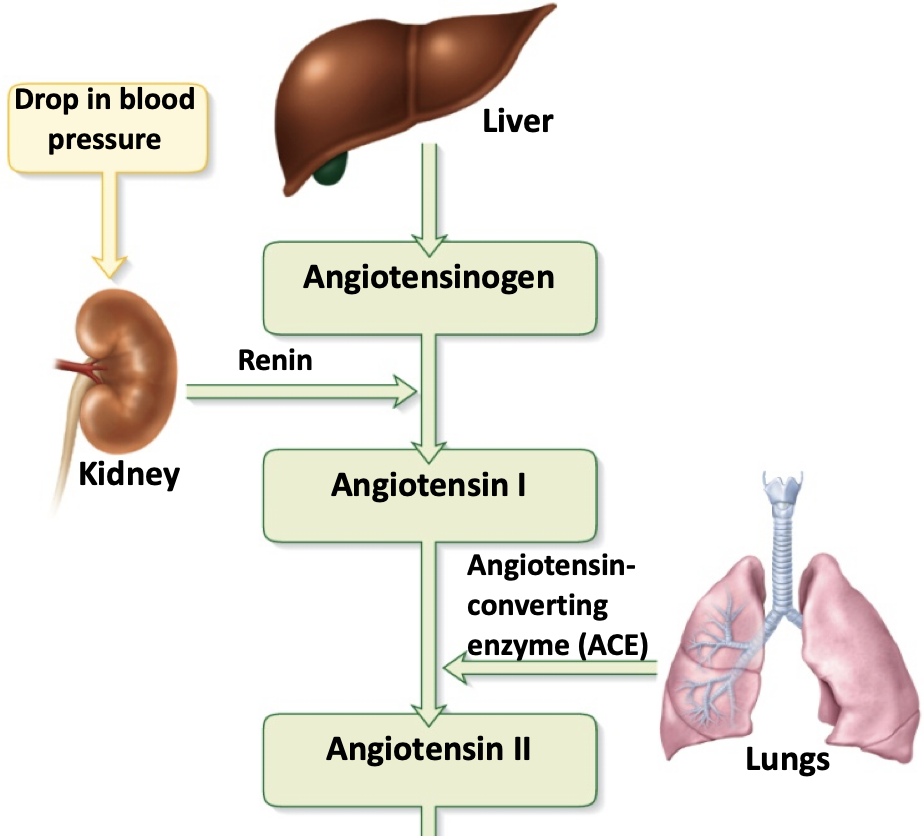
ie indirect renal mechanism
-decrease in systemic BP detected by baroreceptors, juxtagomerular apparatus
-granular cells release renin in response to:
→ sympathetic input
→ signal from macula densa (densely packed cells in kidney for sensory reception)
→ decreased stretch
-renin initiates production of angiotensin II
renin-angiotensin-aldosterone (RAA) mechanism
-vasoconstriction
→ raises
→ lowers
-stimulates
-acts
-overall
antiotensin II
-vasoconstriction of efferent arteriole
→ raises glomerular blood pressure → maintains GFR
→ lowers BP in peritubular capillaries/ vasa recta → enhances absorption (bc of decrease in hydrostatic BP and decreased resistance against vessel fluid movement)
-stimulates secretion of aldosterone and antidiuretic hormone → promote salt and water retension
-acts on hypothalamus to stimulate thirst
-overall effect is to increase systemic BP
tubular reabsorption
-primarily
-necessary
→ almost
→ H2O
-produces
-primarily takes place in PCT
-necessary water & solutes return to blood
→ almost all organic materials
→ H2O & some ions reabsorbed selectively
-produces hypertonic tubular fluid
reabsorption of sodium
-actively
→ symports:
-drives
-alters
-actively transported through TUBULE walls
→ symports: simulatneously binds Na+ and other solute
→ Na+ — H+ antiports
→ Na+ — K+ pumps
-drives reabsorption of everything else
-cotransportation
-alters osmotic & electrical gradients
reabsorption of water
-driven
-aquaporins:
→ always
→ inserted
-solvent drag:
-driven by osmotic gradient
-aquaporins: channels through tubule cells
→ always present in PCT → obligatory water reabsorption
→ inserted in collecting ducts only if ADH is present → facultative water reabsorption
-solvent drag: water carries along dissolved solutes
reabsorption of other solutes
-glucose, amino acids, vitamins, other ions
-nitrogenous wastes
-glucose, amino acids, vitamins, other ions
→ some co-transported with Na+
→ some carried with water
→ lipid-soluble solutes follow concentration gradient across tubule wall
-nitrogenous wastes
→ almost all uric acid
→ secreted back later
→ ~50% urea
→ but more diluted in blood than in urine
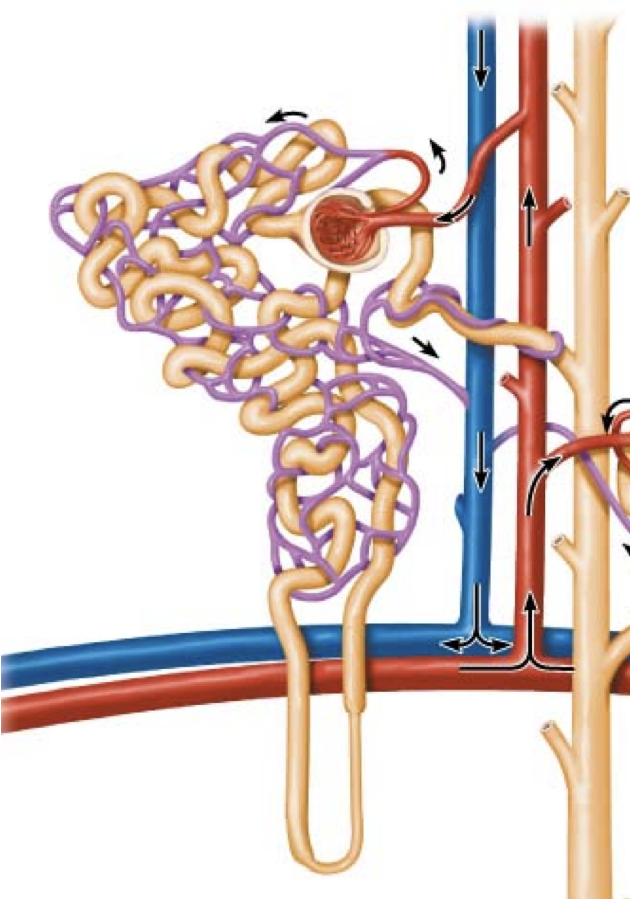
uptake by peritubular capillaries
capillary absorption driven by:
-accumulation of
-narrow
-plasma
-accumulation of reabsorbed fluid → high interstitial hydrostatic pressure (HPif)
-narrow efferent arterioles → low capillary hydrostatic pressure (HPc)
-plasma proteins retained during glomerular filtration: high colloid osmotic pressure (COPc)
(high HPif) + (high COPc) - (low HPc) = absorption
transport maximum (Tm)
-maximum amount of solute renal tubules can reabsorb (mg/ min)
-reached when transporters are saturated
→ sets maximum rate of reabsorption
-impacts reabsorption/ secretion of most solutes
→ each has its own Tm
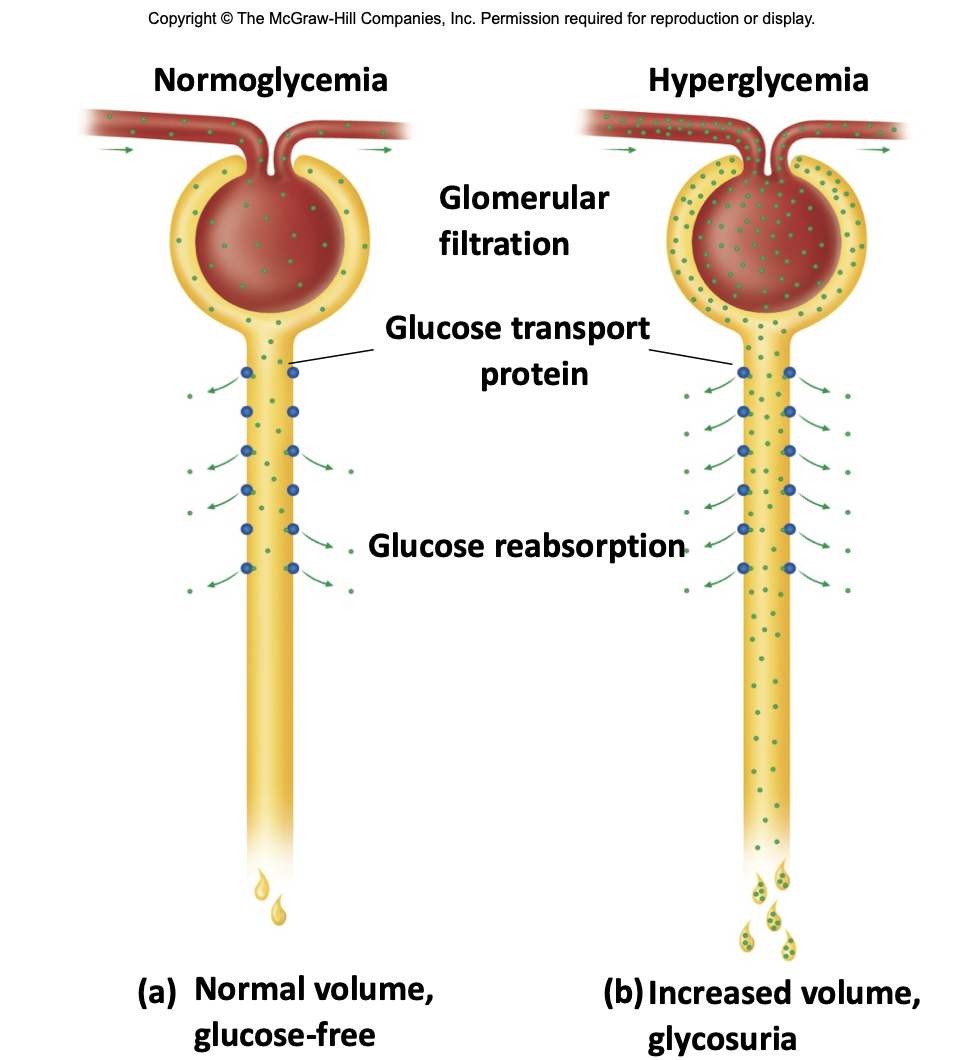
glucosuria
-glucose in urine
-normally passes through renal tubule at 125mg/min
→ glucose Tm: 320mg/min
-high blood glucose increases glucose filtration (into tubule): may exeed Tm
-reduced H2O reabsorption
→ higher urine output
-associated with diabetes mellitus