Lecture 6 - ADHD
1/40
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
41 Terms
ADHD
-historically classified as mental health disorder
-conceptualised as a neurodevelopmental condition/neurodiversity
-but is treatable with drugs unlike other neurodevelopmental conditions
-behaviours may not always cause clinical impact
characteristics of ADHD
-triumvirate of symptoms → hyperactivity, impulsivity, attentional problems
-diagnosed typically based on childhood presentations:
difficulty sustaining attention in tasks
fidgets or squirms
or both
DSM 5-TR (characteristics of ADHD)
-persistent pattern of inattention and/or hyperactivity-impulsivity interfering with functioning, with symptoms present before age 12 in two or more settings
-frontline treatment is lisdexamfetamine or methylphenidate
ICD-11 (characteristics of ADHD)
-persistent pattern of inattention and/or hyperactivity that has a direct negative impact on academic, occupational or social functioning
-needed both inattention and hyperactivity in ICD-10
inattention (symptom presentations)
-lack of attention in academic, occupational or social situations
-careless mistakes
-difficulty maintaining sustained attention
-failing to take in or respond to instructions
-shifting from one task to another without completing any of them
-being easily distracted by irrelevant stimuli or events
hyperactivity (symptom presentations)
-excessive fidgetiness
-not remaining seated
-excessive running or climbing when inappropriate
-talking excessively
-difficulty participating in sedentary activities
impulsivity (symptom presentations)
-impatience
-difficulty in delaying responses
-constantly interrupting others
-drive for immediate rewards over delayed rewards
-proneness to accidents
-indulging in dangerous activities
diagnosis and persistence
-5% children and 2-3% adults diagnosed
-male:female diagnosis of 3:1 -> referral bias and issues with criteria
-trend is narrowing in adults → men and women equally likely to think they had ADHD
-underdiagnosis costs UK £17B per year
-symptoms continue into adulthood
1902 (history of ADHD)
-G.F Still first formally recorded definition of ADHD
-identified children with core traits of modern ADHD
-described as a defect of moral control
prehistory (history of ADHD)
-may have been adaptive for migration hunter-gather societies
-genes associated with ADHD have high prevalence in some modern nomadic tribes
ancient greece (history of ADHD)
-hippocrates described children who had quickened responses to sensory experience, but less tenaciousness because the soul moves quickly to the next impression
-recommend they eat fish instead of meat → some recent evidence suggests omega 3 fish oils can help ADHD
1600s (history of ADHD)
-shakespeare character with malady of attention
-plays showing ADHD-like behaviours
1800s (history of ADHD)
-faust character described as having pattern motor activity, constantly coupled with impulsive actions, without any attention to parents’ warnings or adverse consequences
1920 (history of ADHD)
-encephalitis lethargica link between ADHD-like behaviours and neural changes
-symptoms comatose like sleepiness and headaches → post encephalitic behaviour was distractible, irritable and antisocial
-also presented parkinsonian symptoms → common factor of dopamine
1937 (history of ADHD)
-benzedrine first evidence of stimulant efficacy in the treatment of ADHD-like behaviours
-noticed children became calm and easier to work with
-first evidence of stimulant efficacy in neurodiversity
1960s (history of ADHD)
-introduction of minimal brain dysfunction
-shift between thinking of ADHD as acquired (brain damage/dysfunction) to developmental/behavioural
-first DSM criteria → hyperkinetic reaction of childhood in DSM 2
1980s (history of ADHD)
-refinement of criteria
-ADHD diagnostic label:
1980 → ADD with or without hyperactivity
1987 → ADHD label officially used
1994 → DSM 4 introduce ADHD subtypes, required before age of 7
2000s to present (history of ADHD)
-introduction of ADHD sub-types in DSM
-lowered symptoms needed for adult diagnosis
-move towards neurodiversity in research and societal understanding
current research focus
-understand shorter life expectancies
-how symptoms fluctuate over time
-genetic basis and shared basis with other conditions
-neural changes underpinning ADHD and how to target these
-improving treatment efficacy
-more effective diagnosis
educational attainment
-ADHD students 6.5x more likely to leave school with sub-GCSE qualifications
-higher risk in girls (8.46x)
-significantly increased likelihood of exclusion
occupational outcomes
-mean age 41 with childhood ADHD diagnosis
-lower employment rates
-lower occupational status and lower average salaries compared to controls
peer relations
-ADHD significantly more likely to be ‘rejected’ by peers
-social challenges may begin as early as 7-10
-UG students watched video of woman showing symptoms of ADHD, depression or no psychopathology → rejection significantly higher for those with ADHD or depression
physical health and accidents
-at increased risk of accidents and injuries
-risk and type of injuries changes over the lifespan
-ADHD medication decreases the risk of accidents and injuries in all ages
-1.6x more likely to require medical treatment for accidents in 12 month period
mental health
-anxiety and depression very common
-substance use disorders much more common in adults with childhood ADHD
-but untreated ADHD is the risk and treatment is protective
issues with outcome studies
small samples or prescription based identification
methodological issues → lab or classroom settings and rejection may be a response to stigma rather than behaviours
problems with controls → comorbidity effects, SES, parental factors, different symptom clusters displayed by participants
problems with the constructs → little evidence of general intelligence deficits in ADHD, may reflect ability to complete standardised tests
frontal issues
-executive control
-evidence from:
neuropsychological tests
structural imaging
functional imaging
dopamine issues
-reward processing
-mechanisms of drugs
-differences in reward processing
-some relevant genetic evidence → 76% twin studies
-gene-environment interactions
mDAT1 gene + exposure to prenatal smoking
iowa gambling task (frontal cortex)
-neuropsychological test of cognitive impulsivity
-4 decks of cards with advantageous decks and disadvantageous decks
-ADHD groups typically seduced by big immediate gains despite long-term loss
represents delay aversion
-associated with strong preference for smaller soon rather than larger late rewards
-characteristics of behavioural disinhibition and linked to dopamine dysfunction
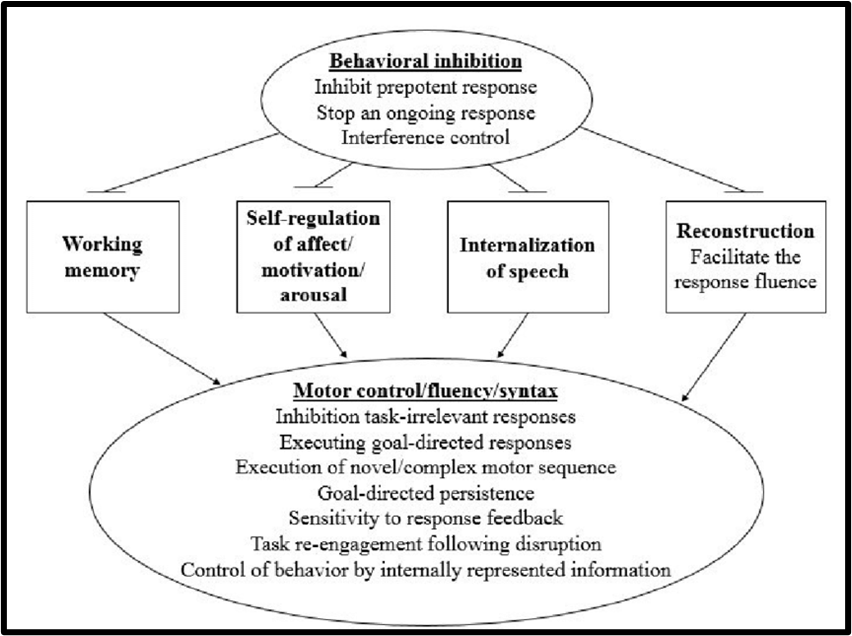
behavioural inhibition model
-failure to inhibit behaviour:
attention problems → distractibility
kinetic symptoms → movement
-neural basis is frontal cortex
frontal cortex insult
-Phineas Gage
-neurocognitive disorders, schizophrenia, lesion studies in animals
structural evidence (ADHD and frontal cortex)
-consistent reductions in frontal lobe compared to age matched controls → associated with control and EFs
-effect size is small changes in cortical thickness rather than large changes
-but evidence may be a delay rather than chronic underdevelopment
-correlational
function evidence (ADHD and frontal cortex)
-broad evidence of frontal hypoactivity during cognitive tasks of attention
-reviews show areas where ADHD patients have greater level of activation
-limited research on adults → delayed maturation
-may represent task performance deficits rather than real world deficits
-continuous performance task measures sustained attention
overview of ADHD and frontal cortex
-deficits in neuropsychological tests of frontal functions
-insult to frontal regions
-frontal regions are underdeveloped relative to age-matched controls
-frontal regions show hypoactivation during cognitive tasks of attention
ADHD and dopamine
-associated with increased dopamine clearance → dopamine vacuuming where it isn’t around long enough to have an effect
-drugs used to treat ADHD increase dopamine levels in murine forebrain
-microdialysis → invasive technique that enables sampling of neurotransmitters, allows us to monitor drug-induced changes
effects of stimulants on dopamine levels
-both d-amphetamine and methylphenidate significantly increase DA levels in PFC or other regions with dopaminergic neurons:
d-amphetamine more potent
methylphenidate longer lasting
stimulant mechanisms (ADHD and dopamine)
-both drugs interfere with dopamine transport
amphetamine → enters pre-synaptic neuron and reverses transporters DA out of cells
methylphenidate → antagonises transports, blocks reuptake
DAT and dopamine vacuum (ADHD and dopamine)
-drug-naive ADHD children have more transporters
-so dopamine is cleared too quickly, creating a low dopamine state
-PET evidence that methylphenidate occupies DAT, decrease dopamine transporter binding preventing reuptake too quickly → suggests therapeutic benefits are achieved through impeding DA reuptake
reward and reinforcement (ADHD and dopamine)
-robust evidence that dopamine is released during reward and that this is disrupted in ADHD
-may be due to tonic vs phasic activity → researchers could be recording phasic rather than tonic activity
tonic activity (ADHD and dopamine)
-cells constantly fire at low rate
-dopamine signal maintains things in a state where ready to respond to reward
-motivation and on-task concentration
phasic activity (ADHD and dopamine)
-sharp burst of activity in dopaminergic neurons in response to reward
tonic vs phasic dopamine
-dopamine activity in the striatum key to efficient reward processing
-PET scan for DA receptors in striatum during reward in ADHD vs non-ADHD
-higher binding means reduced DA activity
found higher binding at rest → lower tonic DA activity
lower binding during rewards → enhanced phasic DA