Respiratory System Study Guide
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
Define respiration and describe the types.
How organisms make energy
External Respiration: Also known as breathing, the transportation of gases move through the capillaries, lungs, and air.
Internal respiration: This occurs deeper in your body, the gases move to your blood and supply your body's cells.
Cellular respiration: Occurs in the cell, specifically in the mitochondria. It will create carbon dioxide by using oxygen for its main energy source. The carbon dioxide emitted by the cells will travel to the lungs.
What are the other functions of the respiratory system?
Removes particles from air
Helps control air temperature and water content
Produces vocal sounds
Participates in the sense of smell
Contributes to regulation of blood pH
Produces a hormone that regulates blood pressure (angiotensin II)
Platelet production (along with bone marrow)
Creates pressure gradient for venous and lymph flow
Filtering blood clots
Assists in expelling abdominal contents.
Describe the two divisions of the respiratory system. What is the other way we can divide the respiratory system?
Conducting zone: Passages that serve only for air flow (nostrils through major bronchioles)
Respiratory zone: Consists of alveoli and other gas exchange regions
Describe the organs of the conducting zone.
Nose: Warms, cleans, and humidifies inhaled air. Helps detect odors and resonate voice.
Nasal cavity: Open space behind the nose, includes the nasal chonchae (superior, middle and inferior), air passes over mucous membranes to heat up air because of blood. Air will evaporate and moisten. Mucous will trap dust, viruses, and small particles; cillia will also move the particles towards your lungs.
Pharynx: Muscular passage in the throat at which the respiratory and digestive tracts cross
Oropharynx: Space between posterior margin of the soft palate and the epiglottis
Laryngopharynx: Lies mostly posterior to the larynx, the esophagus begins at that point
Nasopharynx: Passes only air and is lined by pseudostratified columnar epithelium.
Larynx: Keeps food and drinks out of the airway, also known as the “voice box”
Epiglottis: During swallowing the extrinsic muscles of the larynx pull the larynx upward toward the epiglottis, it closes the airway and directs food and drinks into the esophagus
Vocal cords
Trachea: “Windpipe,” has rings to reinforce the trachea and keep it from collapsing when you inhale and create partial vacuum in the airway.
Bronchioles: Narrowest airway that lead to terminal bronchiole
Describe the organs of the respiratory zone.
Alveoli: Made up of simple squamous tissue to easily pass gas, O2 diffuses from the alveoli into blood, carbon dioxide comes from the blood into alveoli
Alveoli ducts: Connects to respiratory bronchioles and alveolar sacs
Alveoli sacs: Clusters of alveoli
List the path of airflow through the respiratory system. Distinguish between the two divisions.
In the conducting zone air passes into your nose entering your nasal cavity, it then travels to the pharynx and down to your trachea. It enters the main, lobar, then segmental bronchus into the bronchioles, where it ends at the terminal bronchioles
In the respiratory zone it enters the respiratory bronchiole into the alveolar ducts and finally the alveolus.
The bronchioles are housed in the lungs
Surrounded by pleura
What is the role of the pleurae?
Reduces friction: Allows lungs to expand and contract with minimal friction
Creation of pressure gradient
Compartmentalization: Prevents infections from one organ from spreading to others
Define Boyle’s Law.
The pressure of a given quantity of gas is inversely proprotional to its volume
Lung pressure changes based on atmospheric pressure
Define Charles’s Law.
Your bodys mechanism of warming up air, meaning that gas entering your body will expand based on your bodys and external temperature.
Describe expiration and inhalation. Explain how they work. Include which muscles are being used and how atmospheric pressure contributes.
Diaphragm is changing the volume of your lungs to oppose the atmospheric pressure
Expiration:
After inhalation the diaphragm will return to its original spot causing the alveoli to increase in pressure greater than the atmospheric pressure; the air will then leave the respiratory passages down the concentration gradient.
Inspiration:
Atmospheric pressure creates a pressure gradient that is lower than the external air so that it is able to enter your body. The push of outside air helps your body retain gases.
The phrenic nerves will activate your diaphragms skeletal muscles to contract, moving the outer pleura downward as the diaphragm moves. Essentially your lungs and chest wall pulls your inner and outer pleura in the opposite direction, one will pull in and the other out.
Define minute respiratory volume
How much air you breath within one minute
Define alveolar ventilation rate
How much oxygen is supplied and able to travel to your tissues. How much gas your alveoli is holding in each breath
Define tidal volume
How much air you breath in and out during one cycle of normal breathing/eupnea. The normal amount is around 500mL
Define inspiratory reserve volume
The amount of air in your lungs after inhaling at your maximum capacity. The normal amount being about 3,000mL
Define expiratory reserve volume
Measures the amount of air your breath out when forcing all the air out of your lungs. The normal range is about 1,100mL
Define residual volume
How much air is left when you try to force all the air out of your lungs. The normal amount being 1,200mL.
Define vital capacity
Maximum volume of air a person can exhale after taking the deepest breath possible
Inspiratory reserve volume + Tidal volume + Expiratory reserve volume
3,000mL + 500mL +1,100mL
Normal value: 4,700mL
Define inspiratory capacity
Breathing in air with as much force as you can then breathing out normally
Inspiratory capacity= Inspiratory reserve volume + Tidal volume
3,000 mL + 500mL
Normal value: 3,500
Define functional residual capacity
The amount of air left in the lungs after breathing normally
Functional residual capacity= Expiratory reserve volume + Residual volume
1,100mL + 1,200mL
Normal value: 2,500mL
Define total lung capacity
How much your lungs can hold when inhaling
Total Lung Capacity = Inspiratory reserve volume + Tidal volume + Expiratory reserve volume + Residual Volume
3,000mL + 500mL + 1,100mL + 1,200mL
Total lung capacity = Vital Capacity + Residual Volume
Normal value: 6,000mL
Describe the roles of the three respiratory centers in the brain.
Ventral Respiratory group: Works the hardest to coordinate forced breathing or respiratory patterns. It is located in the medulla and connected with neurons:
Inspiratory neurons (I): Helps with breathing in, when the I neurons stimulate the integrating centers of the spinal cord in 2 second intervals, which then sends signals phrenic nerve that controls the diaphragm. Your diaphragm will contract when your intercostal nerves are stimulated, causing you to inhale. When I neurons are working the E neurons are resting.
Expiratory neurons (E): Helps with breathing out, they are stimulated when the I neurons are tired from working or something prevents them from performing. When E neurons are stimulated they let the I neurons rest, without the I neurons working your external intercostal muscles relax or other part of the inspiratory muscle group. The E neuron pulls back the thoracic cage to release air.
Both neurons work together to create around 12 breaths within a minute
Dorsal Respiratory Group: Is also located in the medulla oblongata and helps regulate and allow for the basic respiratory rhythm to perform better.
It takes in information from the pons, chemoreceptors, medulla oblongata, and part of your brain that regulates breathing based of emotional reactions. It sends this information to the ventral respiratory group so that they can change your breathing pattern.
Pontine Respiratory Group: Located in the pons; it recieves information from the hypothalamus, limbic system, and cerebral cortex to notify the dorsal and ventral respiratory group.
It is able to control the duration of breathing, either making it slower or faster. As well as depth, either making it deep or weak.
It is able to regulate and accustom itself to different physical activity or emotions.
Describe the other inputs into control of respiration.
Chemoreceptors: They act when pH levels in your cerebrospinal fluid (central chemoreceptors) or blood (peripheral chemoreceptors) changes
They communicate with the brain through the vagus nerve to send information to the medulla oblongata.
Stretch receptors: Bronchioles contain stretch receptors in their smooth muscle. They communicate using the vagus nerve to notify the dorsal respiratory group
Irritant receptors: In the airways that detect smoke, dust, pollen, chemicals, cold air, mucous. They also communicate with the dorsal respiratory group via the vagus nerve.
Define eupnea
Normal, unlabored breathing that occurs when a person is at rest
Define apnea
Temporary cessation of breathing
Define hypernea
Increased breathing in response to exercise, pain, or other conditions
Define hypoventilation and hyperventilation
Hypoventilation—Low pulmonary ventilation
Hyperventilation—High pulmonary ventilation
Explain Dalton’s Law.
An array of gases such as: nitrogen, oxygen and carbon dioxide in the air; less contributed gases such as: argon, neon, helium, methane, and ozone, as well as water vapor all contribute to create the total amount of atmospheric pressure.
Explain Henry’s Law.
At the air-water interface, for a given temperature, the amount of gas that dissolves in the water is determined by its solubility in water and its partial pressure in the air
Why do oxygen and carbon dioxide dissociate in the lungs at the same rate, even though the partial pressure gradient of oxygen is much steeper?
Carbon dioxide is greatly more soluble than oxygen, this big difference allows it to diffuse into the lungs before oxygen without having to use a higher pressure gradient.
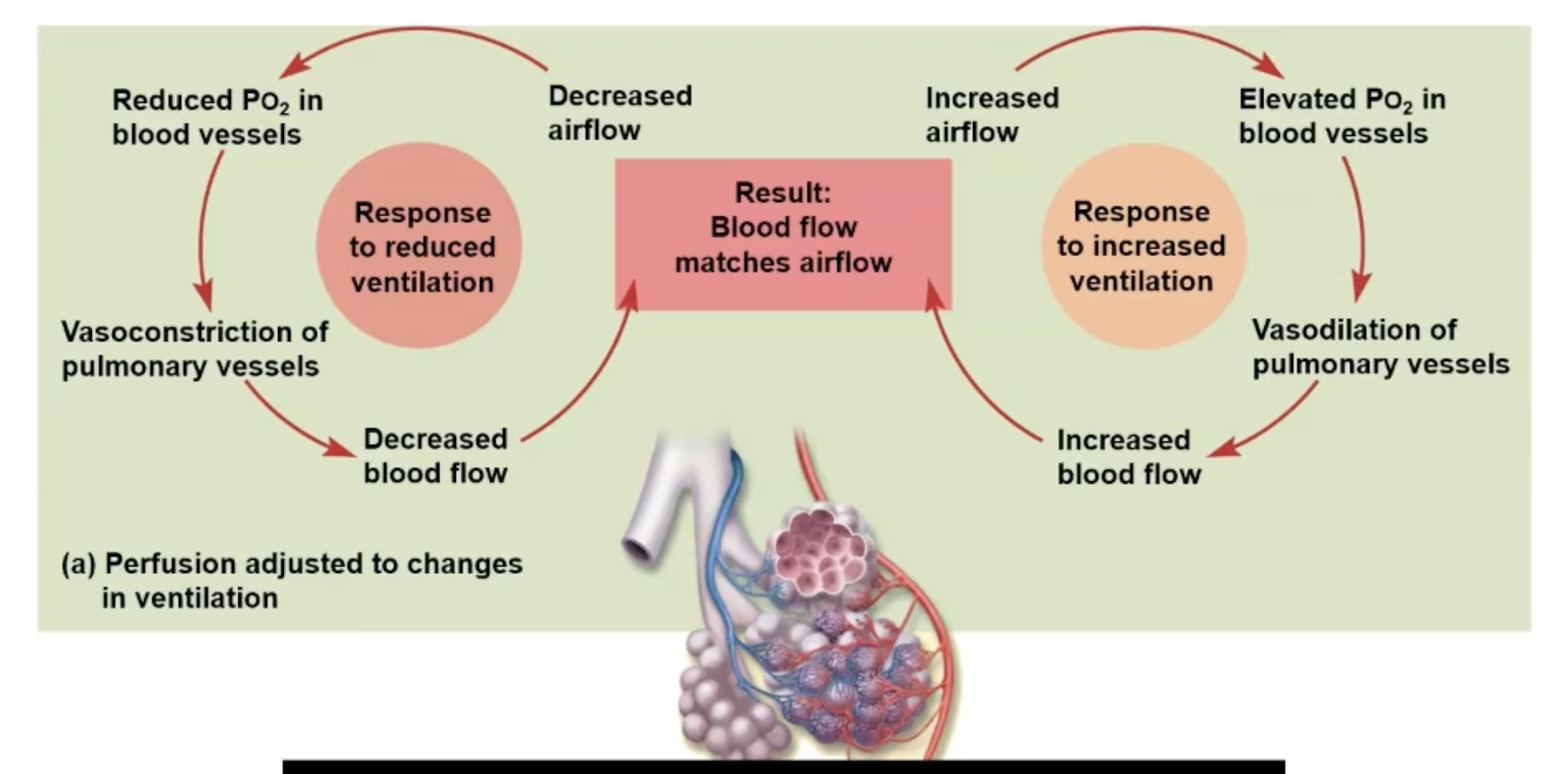
Explain ventilation-perfusion coupling.
Ventilation: Amount of gas reaching alveoli
Perfusion: Blood flow in pulmonary capillaries
Changes to match ventilation
Po2 (partial pressure of O2) controls perfusion by changing arteriolar diameter
Pco2 controls ventilation by changing bronchiolar diameter
Increased Airflow:
Increase O2 in the blood vessels causing vasodilation of pulmonary vessels, increasing blood flow to match the airflow
Decreased Airflow:
Reduced O2 in the blood constricts the pulmonary vessels, decreasing blood flow to match the airflow.
Describe oxygen transport.
Hemoglobin plays an important role in oxygen transport, it is made up of four protein chains and a heme group. A heme group can attach to a ferrous ion so that it can carry more oxygen. More than one oxygen adhering onto a hemoglobin turns into a oxyhemoglobin, when hemoglobin lacks oxygen it is called deoxyhemoglobin.
When there is an abundant amount of oxygen the partial pressure of oxygen also increases
The partial pressure of oxygen will no longer increase if hemoglobin is carrying too much oxygen on it.
Describe carbon dioxide transport.
Transportation of gases between the tissues and alveoli.
1) Most CO2 that can respond to water which turn into carbonic acid, turning into bicarbonate and hydrogen ions
2) Carbamino compounds are created when plasma proteins and hemoglobin adhere to each other. Hemoglobin will be used to take oxygen and carbon dioxide to a targeted area at the same time.
3) Left over carbon dioxide is then brought into the blood
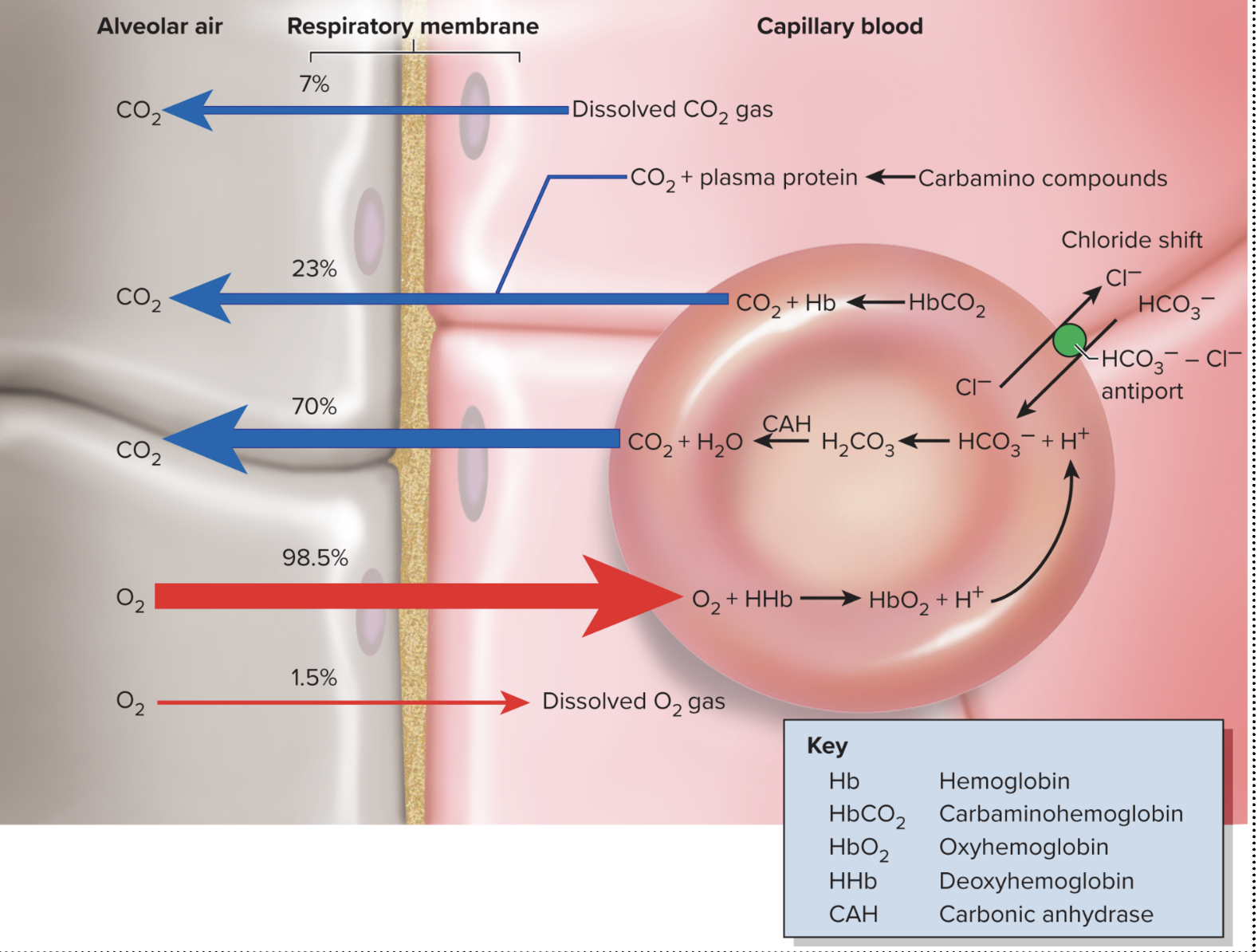
Explain alveolar gas exchange.
Taking out CO2 into the alveoli and transporting oxygen to the blood.
1) Most of the oxygen entering the lungs will bind to hemoglobin in the capillaries. The carbon dioxide will be released into the lungs and detach itself from the hemoglobin.
2) The bicarbonate ion will bind to a hydrogen ion to create carbonic acid. The carbon dioxide separates itself from the carbonic acid due to the concentration gradient to make water.
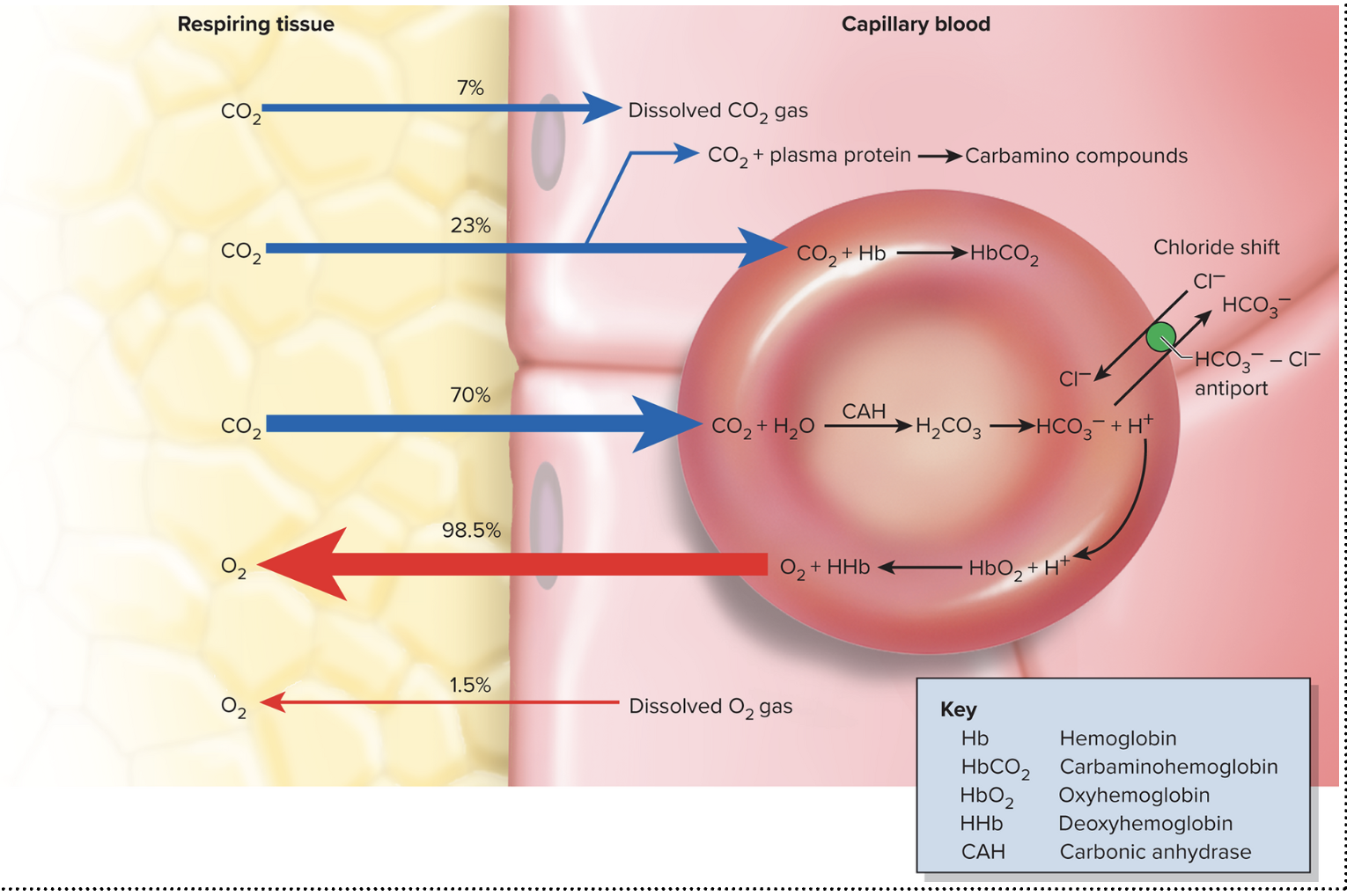
Explain systemic gas exchange. How does it differ from alveolar gas exchange?
Systemic capillaries take out oxygen and take in carbon dioxide
1) Carbon Dioxide Loading: A small percent (7%) of carbon dioxide dissolved in your blood will travels towards the capillary blood. Carbon dioxide can also travel with hemoglobin to transport O2 and CO2 at the same time, carbaminohemoglobin (23%). Bicarbonate ions are what is mostly transported (70%), it is made when water and CO2 are bound to create carbonic acid. To get rid of the acid a chloride shift releases one hydrogen ion to become a bicarbonate ion, adding another hydrogen ion into your blood increasing pH in your blood.
2) Oxygen Unloading: Oxygen breakdown the bonds of hemoglobin so these fragments move towards the tissues. More oxygen is released when there is an increase in carbon dioxide levels in the blood, can be caused by exercising. Oxygen will also be released if the blood becomes too acidic or temperature in your body increases.
Explain the Bohr effect.
How pH affects the unloading of oxygen. When pH in the blood is low hydrogen ions will reduce oxygen and hemoglobin from adhering, causing an increase in oxygen release.
What determines oxygen to dissociate from hemoglobin
Will tell hemoglobin and oxygen to break apart when CO2 levels are too high
Explain the Haldane effect.
Oxygen bound to hemoglobin creates oxyhemoglobin, if there is a decrease in this it stimulates the blood to stimulate more carbon dioxide to leave the blood.