Equine diseases of the head & neck 1
1/46
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
47 Terms
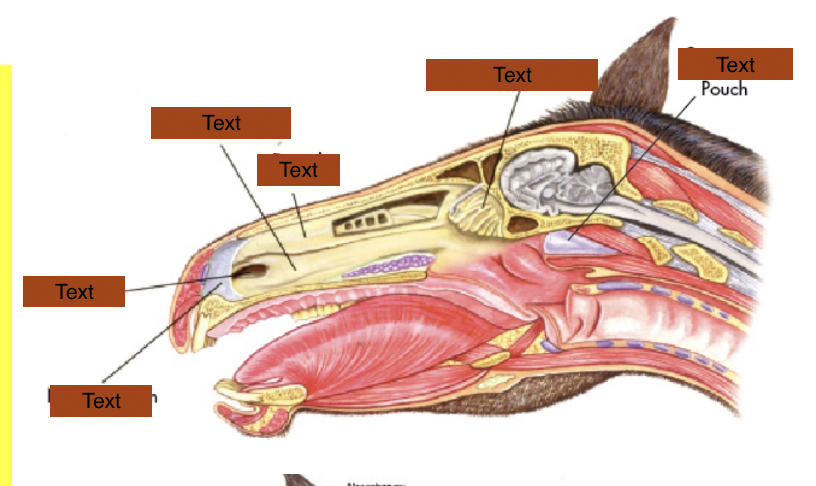
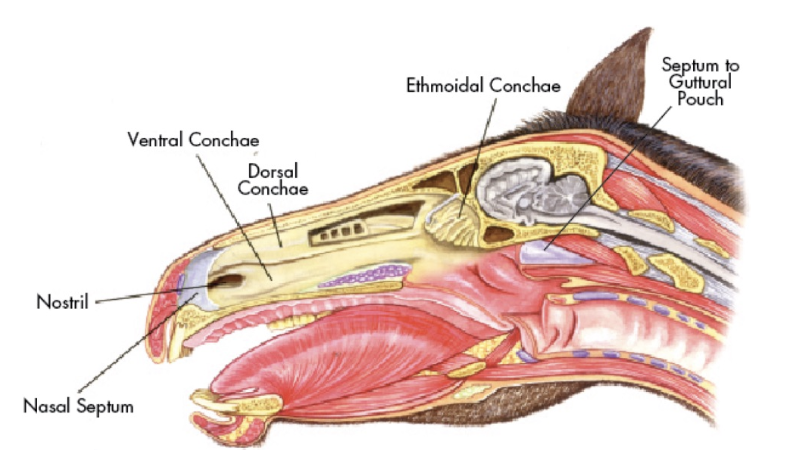
Label the normal anatomy
What are the functions of the upper airway?
1. Conduct airflow to & from lung
2. Filtering —> mucus
3. Protect lower airway from aspiration
4. Olfaction
5. Phonation
6. Swallowing
7. Thermoregulation
What type of breather is a horse?
Obligate nasal breather —> normal upper airway critical
cannot switch to mouth breathing
Describe normal resp anatomy & physiology of the horse
Resp muscles (diaphragm) provides force for ventilation
inhalation = -ve pressures → air moves into lungs
exhalation = +ve pressures → drives air out
What is the RR, tidal volume and minute ventilation of a horse at rest?
15 breaths per minute
Tidal volume = 5L
Minute ventilation = 75L
What can be considered a 'design fault' in the horses resp system?
Horses have big lungs
Small larynx and pharynx and any compromise will severely affect respiration
Minimal tolerance to any disruption in airflow
List the general pathogenesis of abnormal URT function?
Anything narrows lumen
Increases airflow resistance
Resistance inversely proportional to radius, so compromise of airway → large change in resistance
Increases -ve pressure on insp
Unsupported structures collapse
URT obstruction
Noise and reduced oxygen delivery
Why is URT disease important?
Common problem in horses
Can be life threatening
Limit lung capacity causing
Poor performance
Resp noise
What are the possible presenting signs of URT disease?
Resp noise / distress
Dysphagia
Coughing
Exercise Intolerance
Nasal discharge
Blood
Purulent material
Ingesta
Facial deformity
Neuro signs
What is the general history taken to determine URT dx?
Signalment & use
Duration of ownership / pre-purchase exam
General health / duration of problem
Management / recent changes
Dental prophylaxis / vacc status
Any other affected horses on yard
Eating & drinking normally?
What specific history would be taken to determine URT dx?
Nasal discharge
Resp noise @ rest or while exercising
Exercise intolerance
Cough
Prev. medical tx / surgery
What can unilateral vs bilateral nasal discharge tell you?
Where it is coming from
Unilateral —> at or rostral to nasal septum
Sinus / nasal passages
Bilateral —> behind nasal septum
guttural pouch, larynx, pharynx, lower resp tract
What do you need to assess in nasal discharge?
Unilateral or bilateral
Duration
Nature of discharge (serous/ blood/ purulent/ food material)
Evidence of trauma
What do you need to assess when resp noise is present?
Severity of obstruction
When? —> @ rest / exercise
Insp. / exp. / both
movement of chest & abdomen
Sounds? —> Whistle/ Roar / Gurgle/ Snoring
Continuous / Intermittent
noise only at full gallop?
noise only at flexion? (neck brought in) —> changes shape & diameter of airways
Poor performance?:
Does the horse stop/slow down when noise occurs
Are they recovering normally?
What should you examine at rest in a respiratory case?
Look, listen, palpate
General physical exam
All body systems
Concurrent dx
RR & character
Nostril flare
Auscultation of thorax & trachea
Rebreathing (plastic bag over nasal passages to get them breathing a bit more deeply so can assess abnormal sounds —> abnormal sounds exacerbated)
Assess for other causes of poor performance —> lameness, cardiac disease
What on the head is assessed?
Symmetry
Nasal / ocular discharge
Airflow from both nostrils
Percussion of sinuses
tap over sinuses —> should be air filled i.e. hollow
if fluid-filled or has mass = dull-sounding
Palpation of larynx
Previous surgical scars
What should you assess when examining a resp case at exercise?
If abnormal noise is heard:
When it occurs (throughout or when pushed / tired)
Quality / Pitch (whistle/roar/gurgle/snoring)
Stride phase (Locomotor respiratory coupling)
Which sounds are normal and heard at exercise?
Snorting
“High blowing”
Sheath noise
“Thick wind”
What methods can be used for diagnostic imaging of the head?
ENDOSCOPY
RADIOGRAPHY
SINOSCOPY
CT
Ultrasonography
MRI
Scintigraphy
Sound analysis (spectral analysis)
What are the features of resting endoscopy?
Widely available, affordable
Minimally invasive (no surgical incision)
Can pair w/ tx (laser removal / fenestration of tissues)
When is resting endoscopy indicated?
Nasal discharge / malodour
Resp noise
Dysphagia (difficulty eating)
What can you see in this image?

Epiglottis = leaf shaped structure
Arytenoid cartilages behind
Haemorrhage from guttural pouch can be seen on right side of image
What does this image show?

Epligottic entrapment
What does this image show?

Dorsally displaced soft palate
What does this image show?
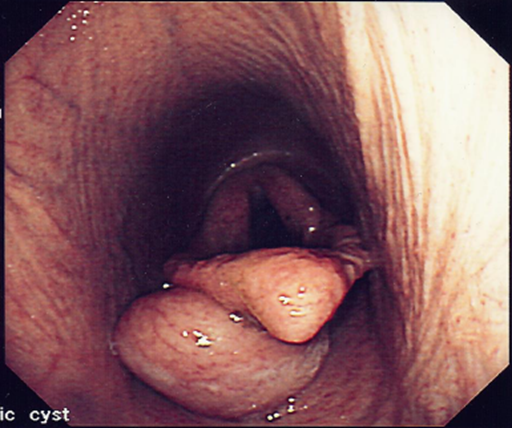
Subepiglottic cyst
What does this image show (URT dx)?
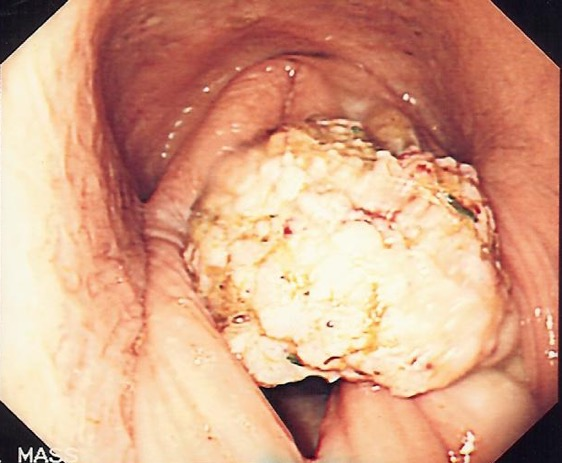
Neoplasia
What are the features of exercising endoscopy?
Important in assessing poor performance at exercise
More accurate assessment of dynamic airway function at exercise
many URT obstructions occur only at exercise
How do you use dynamic respiratory endoscopy?
Used to have to do on treadmill in a hospital
Now can do it with attachment to bridle and wireless imager and real time exam whilst horse is actually exericising
What are the advantages and disadvantages of radiography of the head?
+ve
Gold standard diagnostic test
Images can be obtained with portable machines
Easy to perform many of the standard views
-ve
Complex anatomy
2 dimensional images
What standard and additional radiographic views are used for assessment of the head?
What is latero lateral view used for?
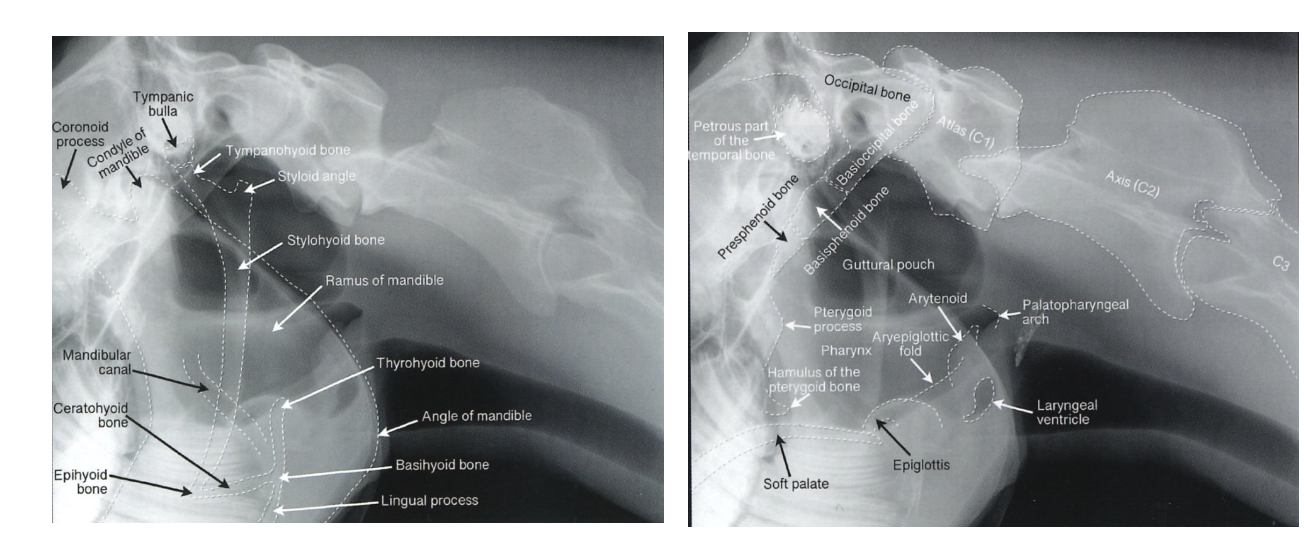
Good for assessing the paranasal sinuses, guttural pouches & pharynx
but cheek teeth superimposed on each other
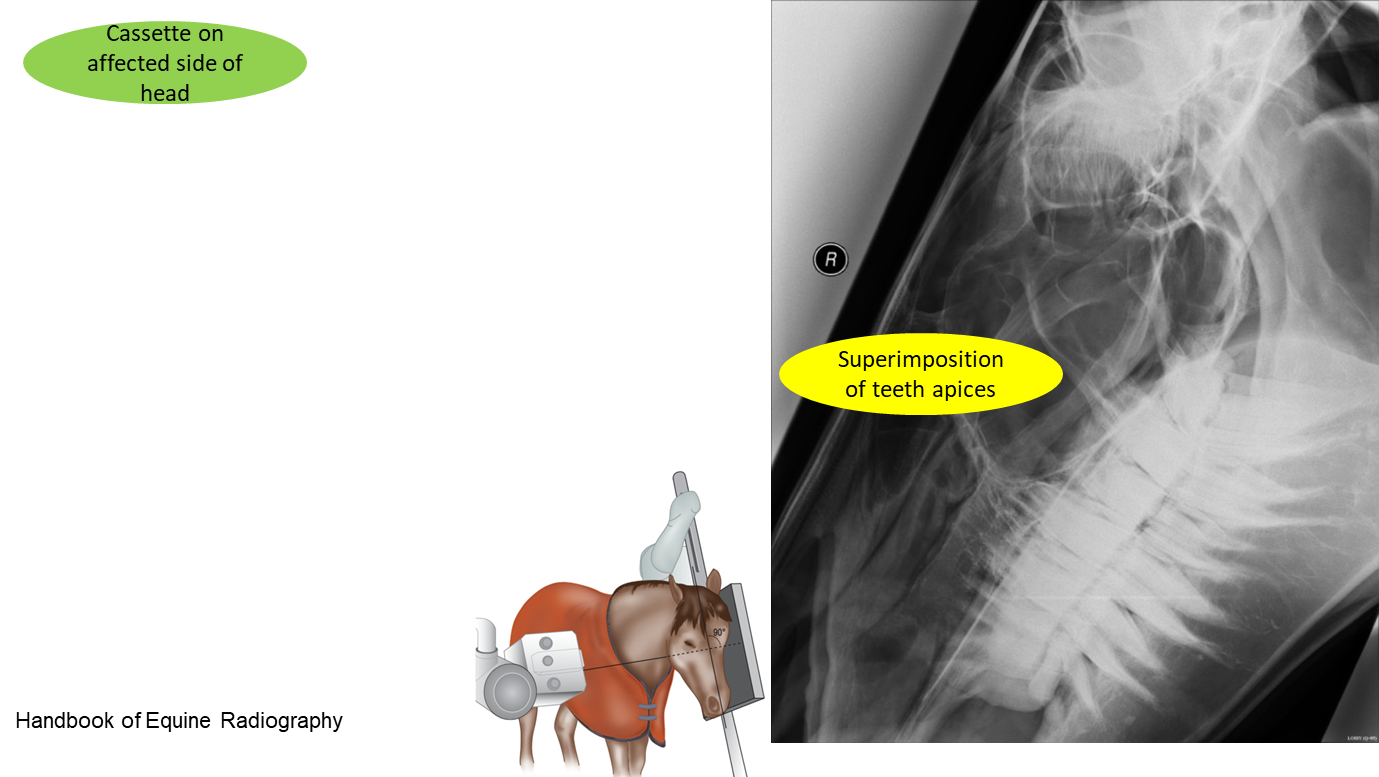
Latero-lateral view anatomy for reference
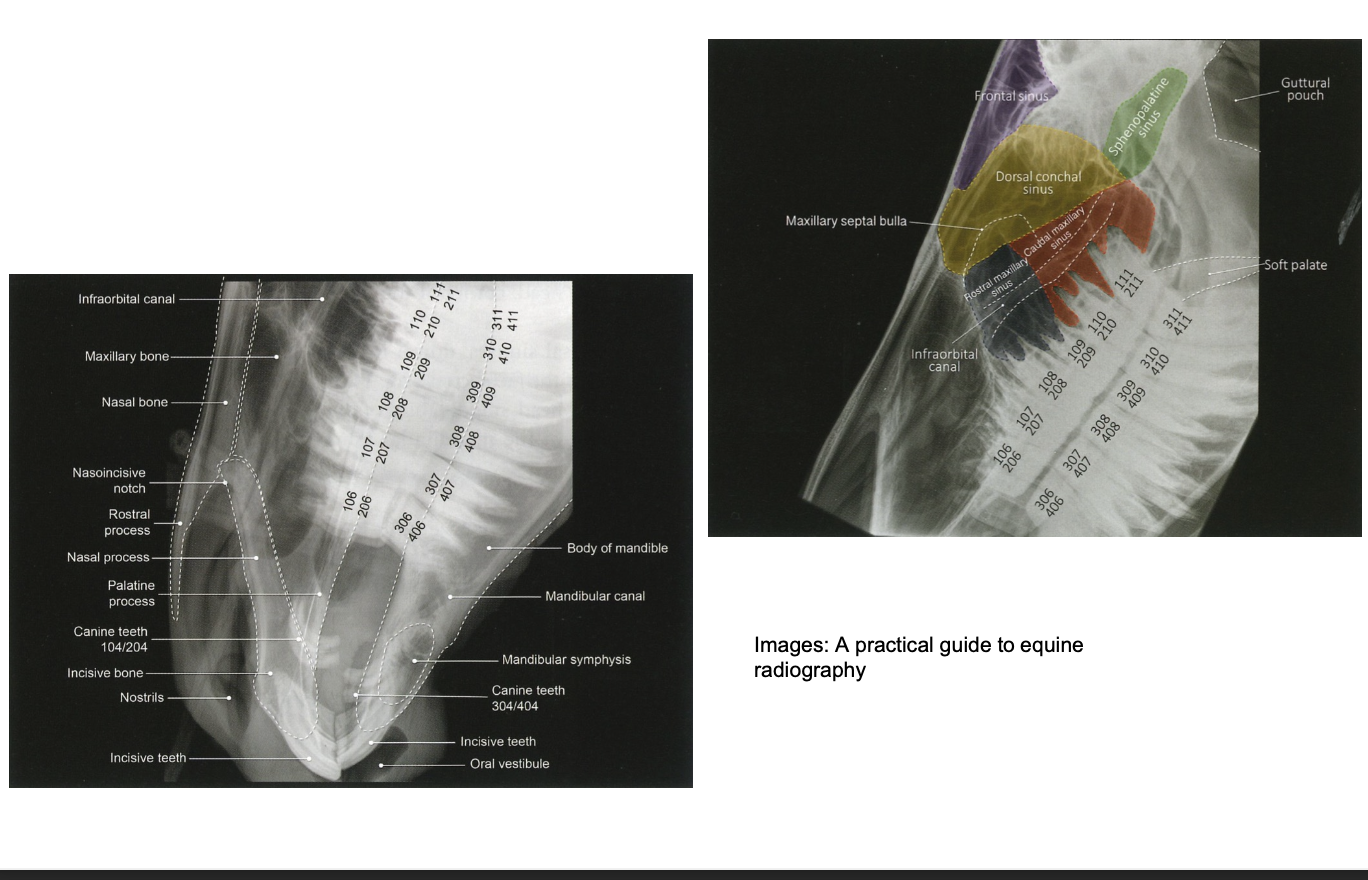
What is lateral oblique view used for? How is it taken?
Assess the periapical regions of the cheek teeth for evidence of infection
30° angulation maxillary arcades

45° angulation for mandibular arcades
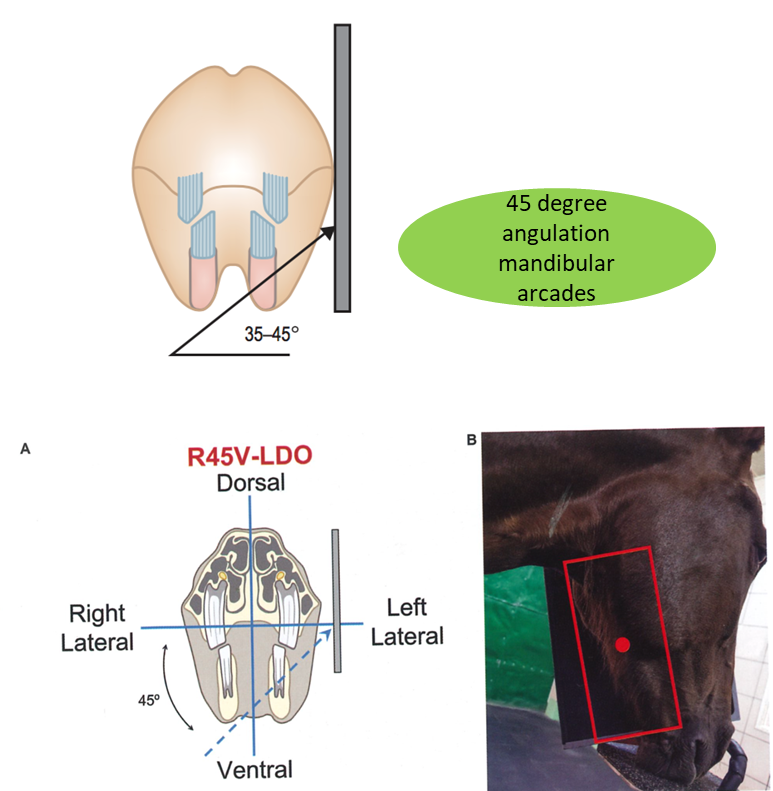
No superimposition of teeth apices (cf. to latero lateral)
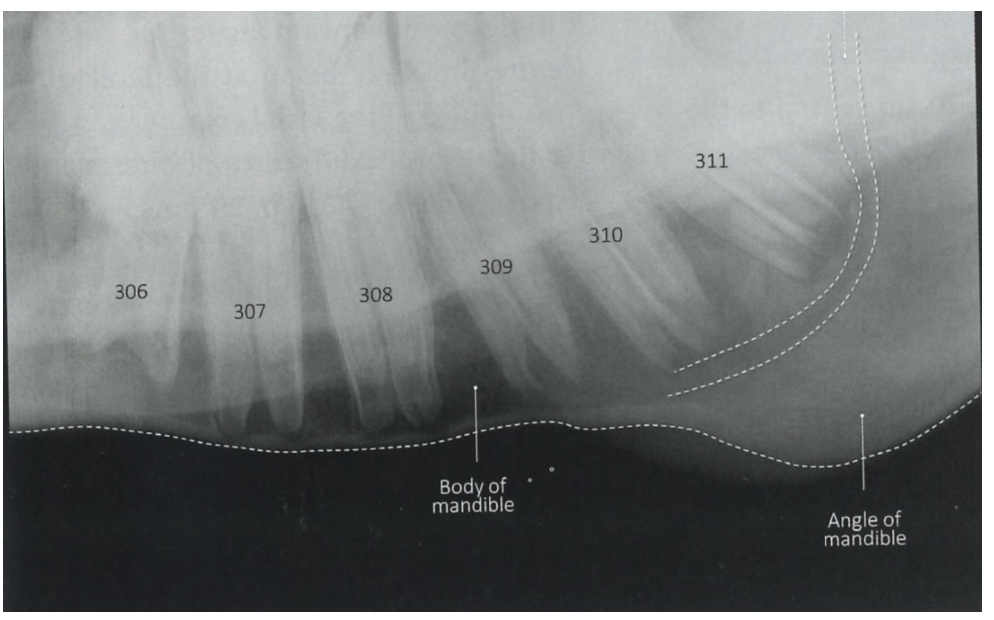
Normal anatomy in lateral oblique
Maxillar
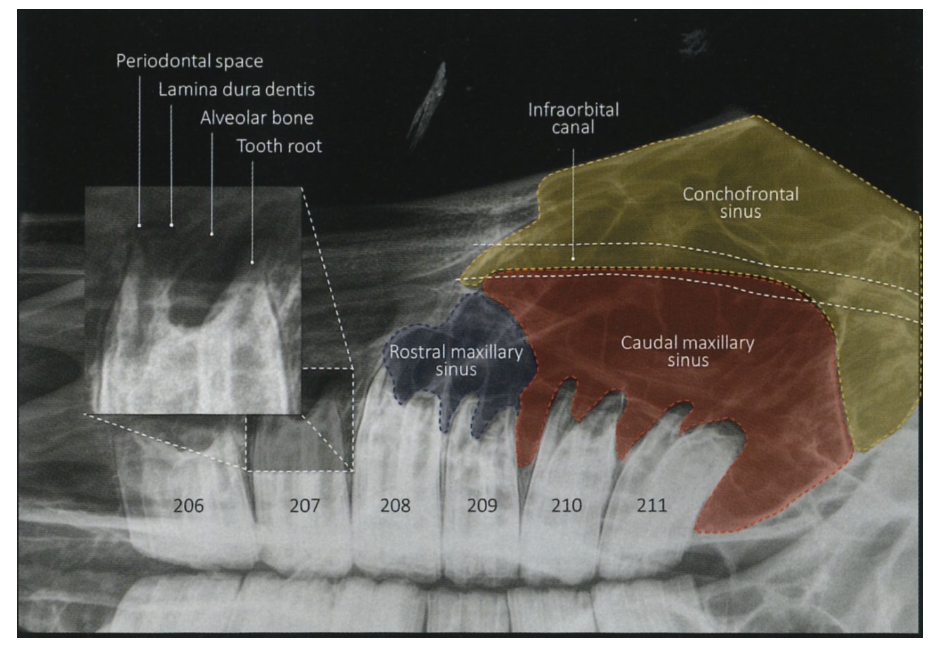
Mandibular
When is a dorsoventral view used?
Assessment of paranasal sinuses, nasal septum & teeth
Helps to determine if lesions unilateral/bilateral
Normal dorsoventral view anatomy
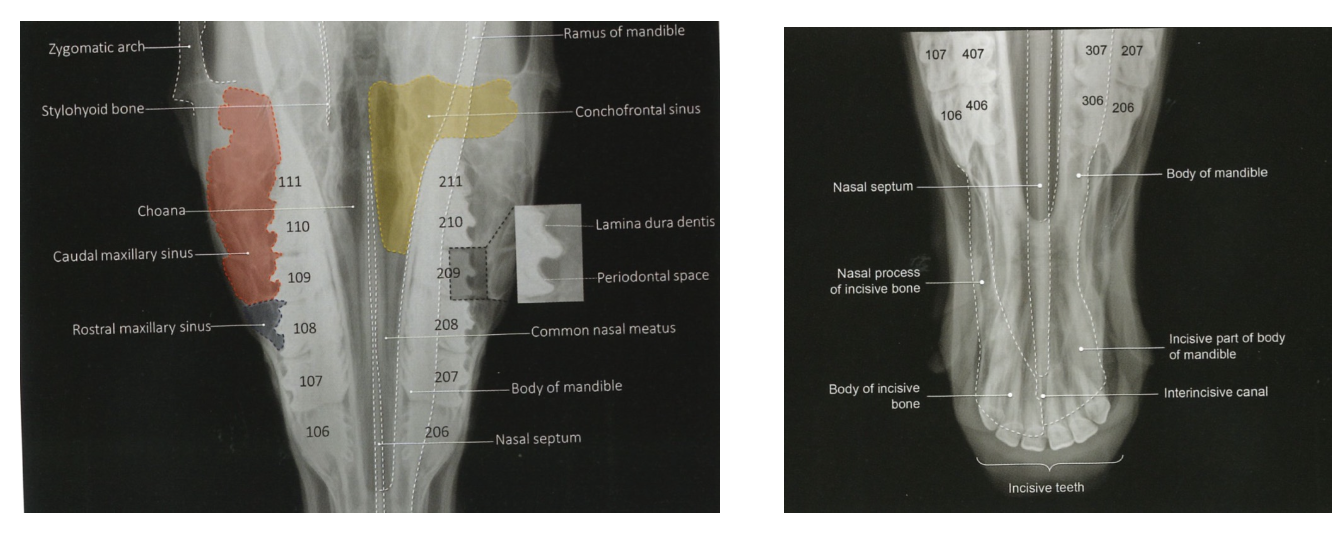
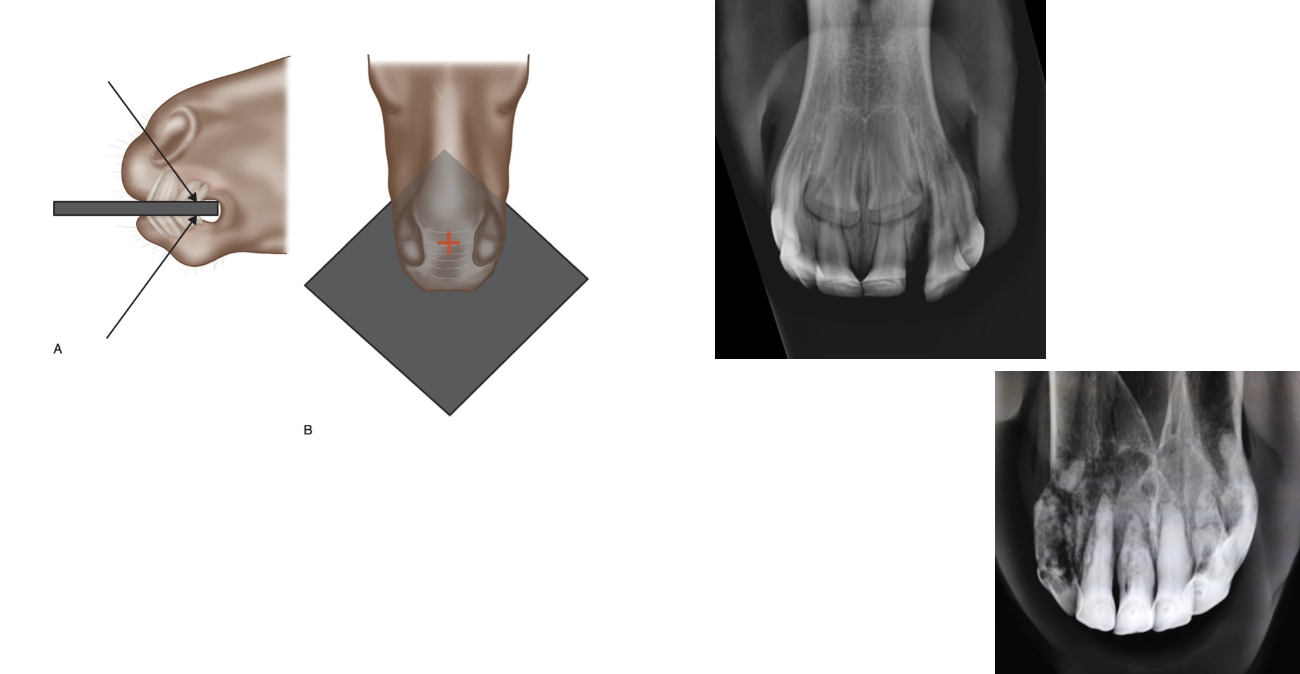
When is intra oral view indicated?
Assessment of incisor teeth & associate bone
Fractures of incisor teeth/associated bone, EORTH (EQ odonoclastic tooth resorption & hypercementosis)
What are the features of sinoscopy?
More invasive than route endoscopy
Standing sedation & LA used
Minimally invasive means of visualising paranasal sinuses
Enables surgical treatment to be undertaken and ongoing lavage of sinuses

What are the features of ultrasonography as an imaging technique of the head?
Widely available
Bony skull limits its use in assessment of some areas of head
When is ultrasonography used in the head?
Ophthalmic
Soft tissue swellings external to the skull
Assessment of skull bones / temporomandib joint
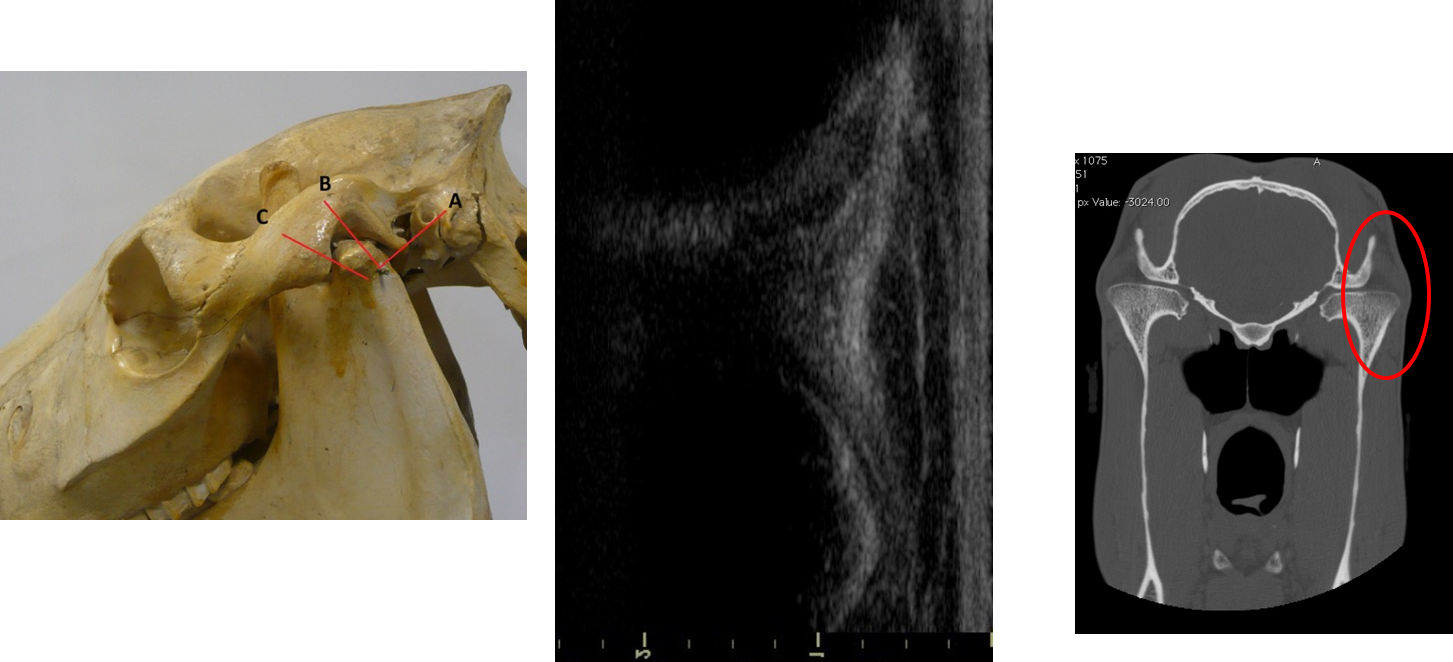
Larynx
What are the major advantages of CT?
Gold standard diagnostic test
Affordable & cost effective
Cross sectional images
Superior resolution
Tissue density measurement
What is CT indicated for?
Dental disease
Masses within the paranasal sinuses / nasal passages
Trauma
What are the different systems used for CT systems?
Multiple systems
GA
Standing sedation
What are the advantages of standing CT?
Avoid risks of GA
Stabilise patient prior to surgery
Pre surgical planning
What are the features of MRI as a diagnostic imaging tool for the head?
Rarely performed in head and neck
Limited to only a few facilities
Requires GA
Very costly & time consuming (~90mins)
When is an MRI indicated?
Quite uncommonly
Brain lesions
Neoplasia
When is scintigraphy indicated for Dx imaging of the head?
Differentiation between primary / secondary sinusitis
Identification of correct tooth
Suspected temporomandib joint dx
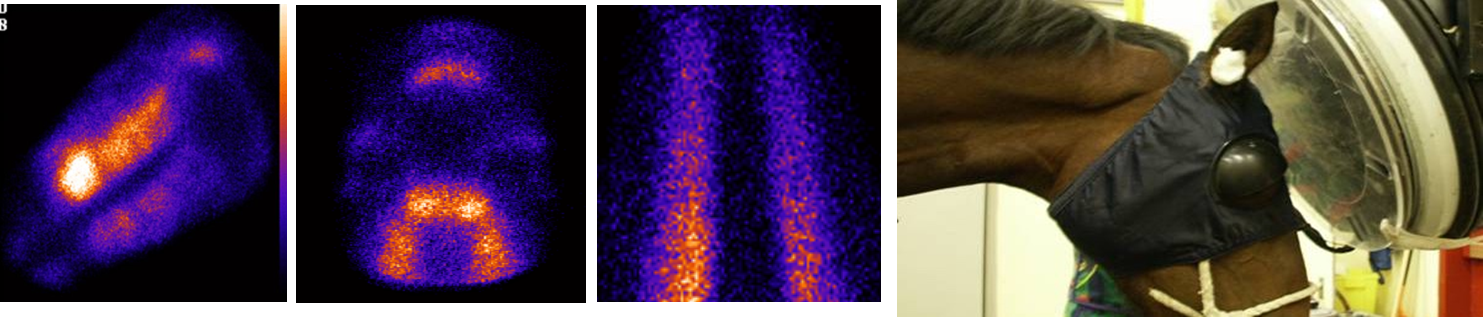
(Superseded by CT, rarely used now)