Burns
1/61
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
62 Terms
functions of skin
protection
thermoregulation
fluid + electrolyte balance
metabolism
neurosensory
psychosocial, interactive → HIGHLY CONNECTED TO HOW YOU FEEL
_____ make up majority of burn pts in all age categories (except 80+)
men
nearly ___% of all burn injuries occur in children under age 15
25%
74% of burn injuries occur where?
at home
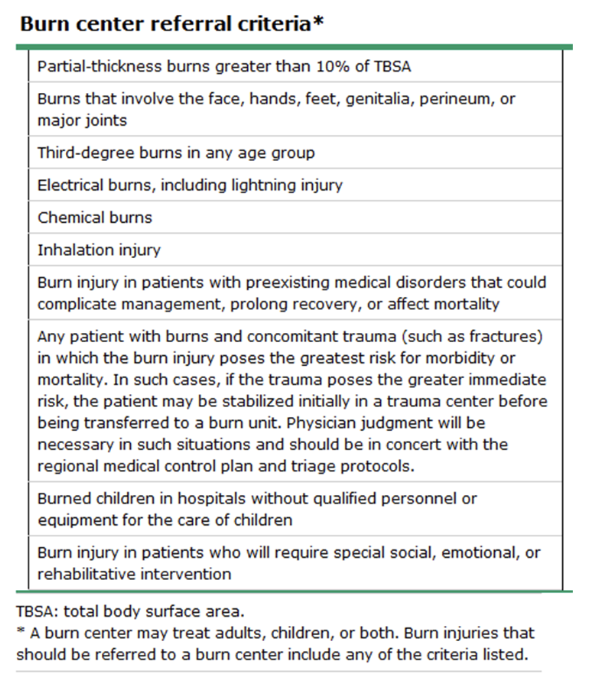
burn center referral criteria
most burns are what type of injuries?
thermal
thermal injuries
who is at greatest risk?
skin comes in contact w/ something hot enough to cause cell injury
flames, scalding liquids, steam, direct contact w/ heat source
children and elderly at greatest risk → b/c they are reliant on other ppl; skin gets thinner as you get older; babies also have thinner skin
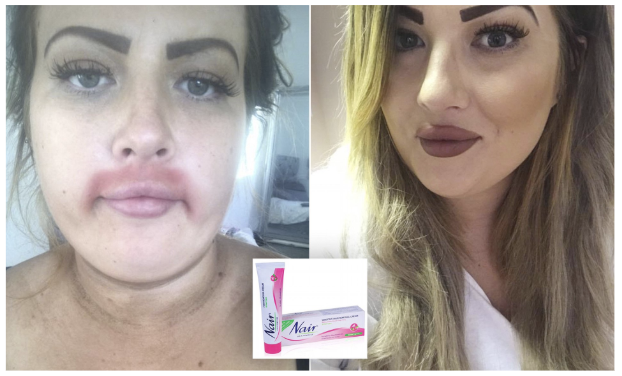
chemical injuries
what kind of effects?
severity related to ?
caused by what 3 agents?
contact, inhalation of fumes, ingestion, or injection
local and SYSTEMIC effects
severity related to type, volume, duration of contact, and concentration of agent
tissue damage continues UNTIL CHEMICAL completely REMOVED or neutralized
caused by 3 agents:
alkalis (oven cleaners, fertilizers, wet cement, lye—in different soaps) → MORE SEVERE THAN ACIDS b/c they denature proteins in your skin
acids (bathroom cleaners, rust removers, pool chemicals) → injury more limited b/c do NOT denature proteins in skin
organic compounds (gasoline, kerosene, ethanol) → CNS effects b/c they dissolve the lipid barrier in cells → can enter bloodstream quicker → to brain
are chemical injuries caused by alkali or acidic compound typically more severe?
alkali (oven cleaners, fertilizers, wet cement, lye—in different soaps) → MORE SEVERE b/c they denature proteins in your skin
what is special about chemical burns caused by organic compounds?
CNS effects b/c they dissolve the lipid barrier in cells → can enter bloodstream quicker → to brain
gasoline, kerosene, ethanol
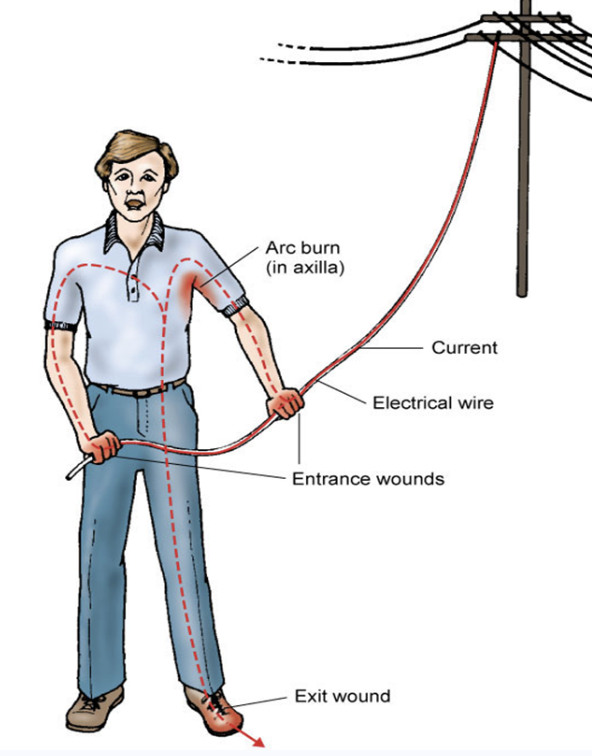
electrical injuries
___ injuries have HIGHER risk of cardiopulmonary arrest by VFib compared to DC injuries
what impacts severity?
almost all electrical injuries cause ?
caused by contact w/ electrical sources
AC (alternating current) injuries have HIGHER risk of cardiopulmonary arrest by VFib compared to DC injuries
AC can cause tetany → keeps circulating through
things that impact severity: type and pathway of current, duration of contact, environmental conditions, body tissue resistance
electroporation → your body cells are an excellent conduit for electricity to travel through your body → entry and exit wound!
wound can appear superficial!!!
electroporation
inc in conductivity and permeability of cell membranes
inhalation injuries
__ mortality rate
classifications?
dx based on what 3 things?
caused by inhalation of smoke, chemical toxins, and products of incomplete combustion
INC MORTALITY RATE (very high b/c airway is getting burned → impacts your ability to oxygenate your body)
classifications:
systemic injury caused by exposure to toxic gas
supraglottic injury
subglottic injury
dx based on hx, clinical signs, and bronchoscopy findings
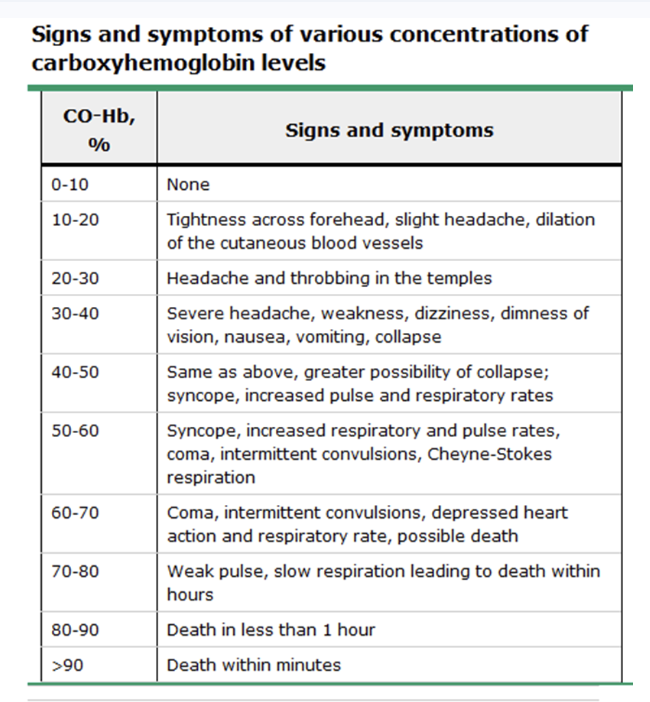
carbon monoxide poisoning
what type of injury is this?
PaO2 and SaO2 ?
tx?
inhalation injury
released when organic compounds (wood, coal) are burned or in heavy smoking
CO has 200x higher affinity for Hgb than O2 → forms carboxyhemoglobin → leads to tissue hypoxia
normal carboxyHgb level in practice = 2% or less
PaO2 and SaO2 suspiciously high/normal (b/c these tests simply test if something is bound to Hgb, not necessarily O2
tx: 100% O2 (to try to push CO off Hgb)
more common in ppl who smoke → they have baseline carboxyHgb level of 9-11%
cyanide poisoning
caused by ?
impairs ?, leads to ?
suspect w/ what 3 S&S?
antidote = ?
inhalation injury
caused by combustion of household synthetics (upholstery, carpet, plastic, vinyl)
impairs cellular respiration, leads to anaerobic metabolism → inc in serum lactate
suspect w/ unexplained hypotension, hypoxemia, and lactic acidosis
sx similar to CO poisoning (HA, dizzy, N)
antidote = hydroxocobalamin (CyanoKit)→ **causes RED discoloration of urine and body fluids
form of vit B12

supraglottic inhalation injury
usually caused by what type of injury?
S&S?
usually caused by thermal injury
heat absorption and damage occur mostly in pharynx and larynx
may cause airway obstruction
hoarseness, dry cough, labored breathing, difficulty swallowing, stridor (signs associated w/ upper airway obstruction)
subglottic inhalation injury
usually caused by what type of injury?
extensive damage to ?
hallmark sign?
usually a chemical injury that produces impaired ciliary activity, erythema, hypersecretion, edema, ulceration of mucosa, inc blood flow, bronchospasm
extensive damage to alveoli and impaired pulm. function
hallmark sign = carbonaceous sputum = sputum looks sooty (dark, specks of ash)
can develop ARF and ARDS
clinical indicators of inhalation injuries
hx of exposure in confined or enclosed spaces
facial burns
singed nasal hairs
carbonaceous suptum
hypoxemia
abnormal breath sounds
signs of resp distress
elevated carboxyHgb levels
abnormal ABG values
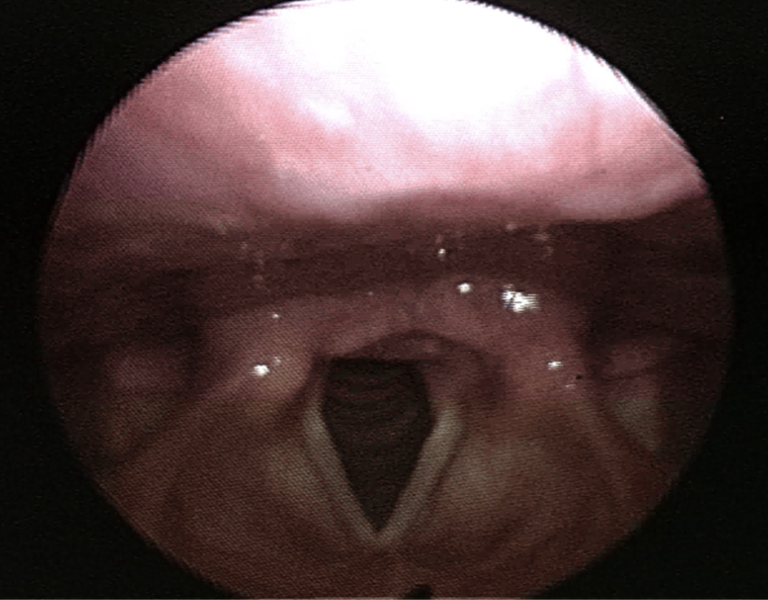
bronchoscopy of normal larynx
pretty nice and pink, can visualize vocal cords
nice little triangle

bronchoscopy — inhalation injury — edema
very difficult intubation
8-12hrs post burn injury
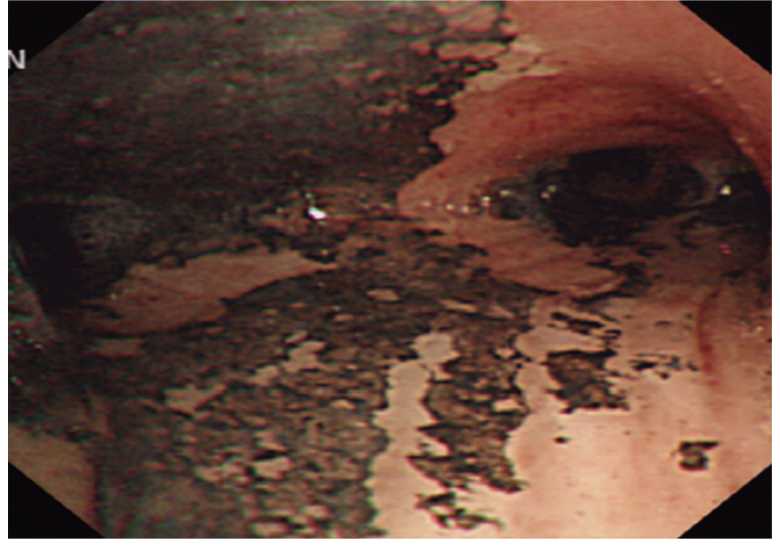
bronchoscopy — inhalation injury
edema has resolved, but now lots of scarring
burn severity is determined by
type
characteristics
concomitant injuries
pt age
preexisting health status
extent and depth of burn injury is affected by
duration of contact
temp
amt of tissue exposed
ability of agent and tissue to dissipate thermal injury
superficial burn
involves ?
what does it look like?
on dark skin?
healing time?
aka 1st degree
involves ONLY EIPDERMAL LAYER
area pink to red; slightly edematous, usually NO BLISTERING
on dark skin: appears reddish-brown
healing time: 3-5 days

partial thickness burns
involves ?
what does it look like?
further broken down into?
2nd degree burns
involves ENTIRE epidermal layer AND varying depths of DERMAL LAYER
BLISTERS!!
further broken down into superficial partial thickness burns and deep partial thickness burns
superficial partial thickness burns
looks like?
cap refill?
blisters?
heal time?
pain?
type of 2nd degree — not as far into dermis
hair follicles, sebaceous and sweat glands typ intact
bright red, edematous
near normal cap refill
blisters appear w/in MINUTES (ALWAYS)
heal time: 7-10 days
MORE PAINFUL (b/c all of your nerve endings are still intact)
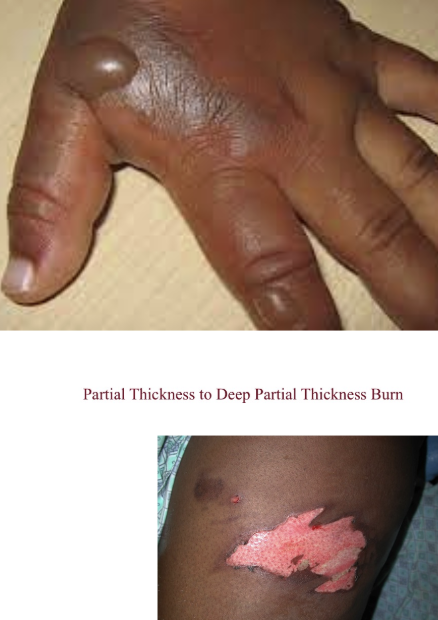
deep partial thickness burns
looks like?
cap refill?
blisters?
heal time?
pain?
type of 2nd degree
damaged nerve cells
white and waxy; surface can be wet or dry
dec cap refill
may see blisters
heal time: 2-4 wks
typ less painful
full thickness burns
what layers of skin are damaged?
cap refill?
what’s it look/feel like?
pain?
heal time?
aka 3rd degree
destruction of ENTIRE epidermis AND dermis
little to no cap refill
thrombosed blood vessels (essentially cauterized) may be visible
surface firm, dry, leathery
NO pain or sensation
does not heal on its own — will require skin grafting

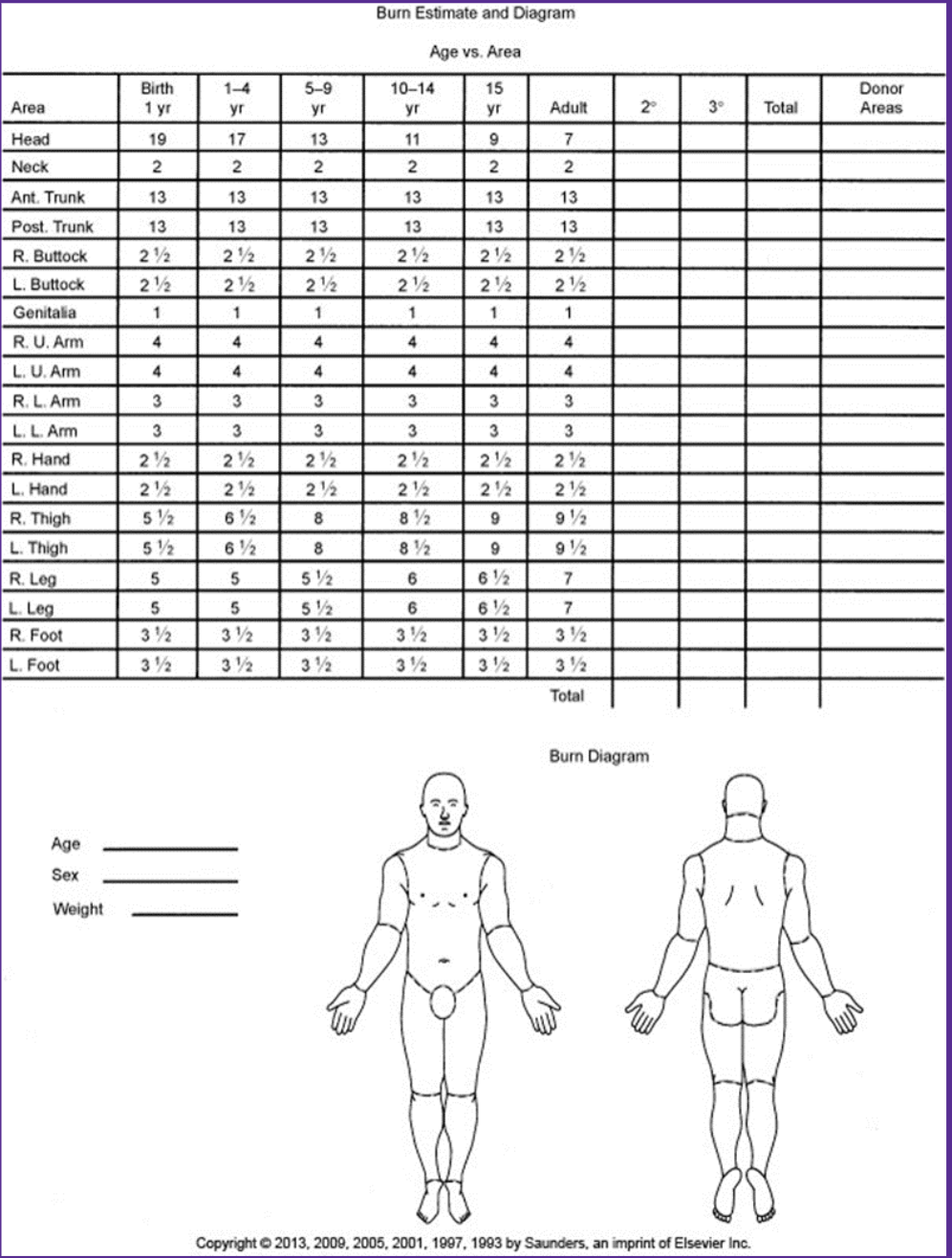
total body surface area (TBSA)
rule of nines
only used for partial and full thickness burns
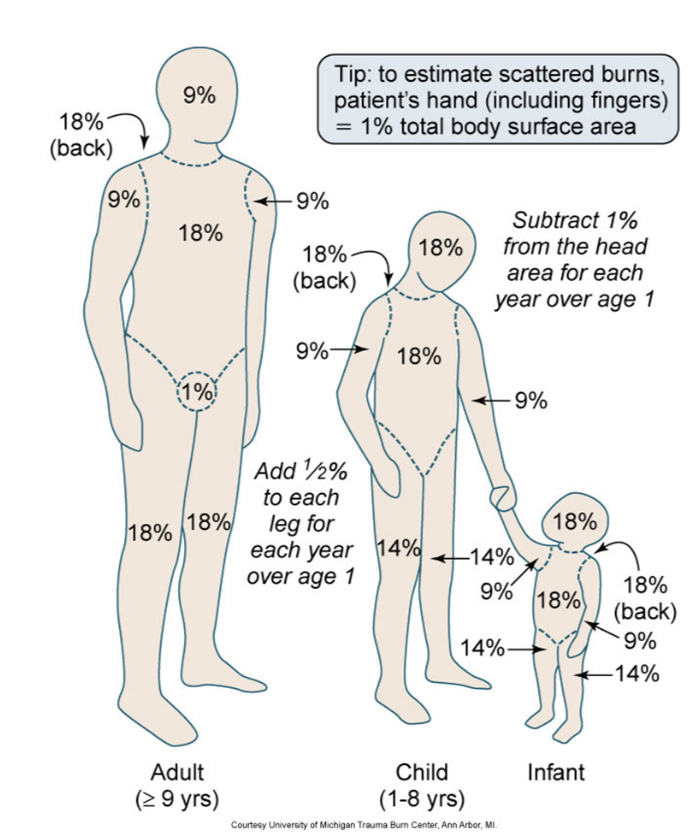
what is used to calculate extend of burn injuries in burn centers (more detailed)
Lund and Browder chart
physiologic response of getting burned
significant changes in almost every body system — local AND systemic!!
intravascular coagulation from thermal damage
inflamm mediators released from damaged cells
inc cap permeability (leak) → edema and intravascular fluid depletion (RELATIVE hypovolemia)
burn shock — combination of distributive and hypovolemic shock
phases of burn care
resuscitative phase
acute phase
rehabilitative phase
phase 1 of burn care: resuscitative phase
when?
tx priorities?
begins at time of injury - 48hrs until fluid and protein shifts stabilized
ABCs and prevention of burn shock
correct someone’s fluid balances and correcting relative hypovolemia
phase 2 of burn care: acute phase
when?
tx priorities?
48-72hrs until wound closure occurs
burn center — weeks, months
focus on: wound healing, prevention of infections, lots of psychological support
phase 3 of burn care: rehabilitative phase
when?
tx priorities?
could be lifelong
improve function and ROM
minimize scarring
restore ADLs
resuscitative phase tx
pre-hospital
hospital / burn center
pre-hospital:
remove pt from scene
stop burning process
triage injuries
avoid heat loss
secondary survey
hospital / burn center:
primary survey
IV narcotics
prevent burn shock
ABCs — monitor ventilation w/ circumferential full-thickness burns to thorax
DVT / PE prophylaxis
nutrition w/in 24 hrs (need ntrn to heal)
procedure to treat full-thickness circumferential burns
escharotomy
full-thickness burns will act like a tourniquet → super tight → your diaphragm and lungs cannot expant and contract
prophylactically or to release pressure and facilitate circulation
incision through eschar to expose subQ layer → incision will widen substantially b/c of all the pressure that’s being released

fluid resuscitation — ONE OF THE BIGGEST PARTS OF RESUSCITATIVE PHASE
b/c pt has relative hypovolemia
myocardial depression leads to massive fluid shifts and low CO
central line or 2 large-bore IVs or IO
oral hydration for smaller burns
IV hydration for burns >20% TBSA
Parkland formula!!
LR
Parkland formula
first ____ hrs give 50% of total fluid
administer remaining 50% over _____ hrs
IV hydration for burns >20% TBSA
(4mL) x kg x (% TBSA)
first 8 hrs give 50% of total fluid
administer remaining 50% over 16 hrs
Patient weighs 75kg and has 55% TBSA
How many mL in first 8 hours?
How many in 16 hours?
How would you set pump for first 8 hours?
4×75kg*55% = 16,500mL total
8250mL in first 8 hrs
8250mL in next 16 hrs
pump rate for first 8 hrs: 1031 mL/hr
why does it matter if a pt has inhalation injuries when considering the amt of fluids to give them?
if pt already has an inhalation injury, then their pulm circulation is already damaged and impaired → if you’re giving them a ton of fluids on top of that, then you have to be very careful to not send them into flash pulm edema b/c they’re already having pulm issues
how do yk that fluid resuscitation was successful?
adequate urine output (30 mL/hr or 0.5mL/kg/hr for adults)
BP / MAP (want MAP to be 65)
HR (<120bpm)
acute phase tx specific
pt should be stabilized w/in 48-72 hrs, good urine output and VS
goals: promote wound healing, prevent complications, and improve function of body systems
wound care VERY important
ensure up-to-date on tdap vaccine
prevent hypothermia — burn units are super hot
cleaning and debriding wounds to prevent infection
VERY PAINFUL — give IV narcotics
surgical intervention needed?
dressing change protocol
topical ointments / dressings — silver sulfadiazine, mafenide acetate, bacitracin, Xeroform gauze
ntrn promotes healing!! — high proteins, high calories, high fat
what diet should pts on the burn unit (acute phase) be on?
high protein, high calories, high fat — ntrn promotes healing!!
rehabilitation phase specific tx
wound and scar management
preventing wound complications
pain — very high risk of developing substance use disorders
psychosocial support
disfigurement, chronic pain, social support, safety concerns, pre-existing psychiatric disorders, high risk behaviors (substance/alcohol use), PTSD

deep partial thickness burns
skin is a bit wet
red
aren’t all the way down to third layer

deep partial thickness
blisters
white, waxy skin underneath — burned through wet layers

superficial / 1st degree burn

blister!! → second degree
superficial partial thickness burn

full thickness / 3rd degree burn

4th degree burn → fingers are gonna be amputated

2nd degree — superficial partial thickness burn

2nd degree — superficial partial thickness
intact blisters

some 2nd and 3rd degree
A pt was rescued from a house fire and is suspected of having an inhalation injury. Which clinical finding is the most immediate priority for the nurse to report to the healthcare provider?
Agitation and bright red skin
The nurse is applying silver sulfadiazine to a pt’s burn wounds. Which lab value should the nurse monitor specifically for a common side effect of this med?
WBC count
a pt w/ an electrical burn from a high-voltage wire is admitted to the ICU. The nurse observes that the pt’s urine is dark and reddish-brown. Which nursing intervention is the priority?
inc IV fluids to maintain a urine output of 75-100 mL/hr
A pt is admitted to the ED w/ deep partial-thickness burns to the entire left arm, the anterior chest, and the anterior left leg. Using the Rule of Nines, the nurse should calculate the Total Body Surface Area (TBSA) burned as
27%
left arm (9%) + anterior CHEST (9%) + anterior left leg (9%)
during the emergent (resuscitative) phase of a major burn injury, which electrolyte imbalance is the nurse most likely to observe due to cellular destruction?
hyperkalemia — when cells are burned and rupture, they release their intracellular contents (K+) into the bloodstream
which nutritional intervention is most appropriate for a pt in the acute phase of recovery from a 50% TBSA burn?
high calorie, high-protein diet w/ early enteral feedings
A nurse is caring for a firefighter w/ full-thickness circumferential burns to the right arm. The nurse notes that the right hand is cool to the touch, and the radial pulse is no longer palpable w/ a doppler. Which procedure should the nurse anticipate first?
escharotomy
An adult weighing 70kg has sustained 40% TBSA burns. Using the Parkland Formula, the nurse calculates the total fluid resuscitation required for the first 24hrs. At what rate (mL/hr) should the nurse set the infusion pump for the first 8 hrs?
700 mL/hr