Lecture 13: Stroke and TBI
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
Ischemic vs hemorrhagic stroke
Ischemic: No pain, No impaired consciousness (blood obstruction; 80-85% of strokes)
Hemorrhagic: headache + neurologic deficits gradually worsens as the hemorrhage expands
Anterior Cerebral Artery Syndrome signs + symptoms
- Contralateral motor and sensory loss LE > UE
- Motor and behavioral impairments
- Urinary incontinence
- Imitation, bimanual tasks, apraxia
Middle Cerebral Artery Syndrome signs and symptoms
- Contralateral motor and sensory UE > LE
- Contralateral homonymous hemianopia
- L sided: aphasia
- R sided: perceptual deficits (neglect, spatial relations, agnosia, apraxia)
Posterior Cerebral Artery Syndrome signs and symptoms
- Contralateral homonymous hemianopia
- Memory impairments
- Visual agnosia
- Prosopagnosia
- Post-stroke pain
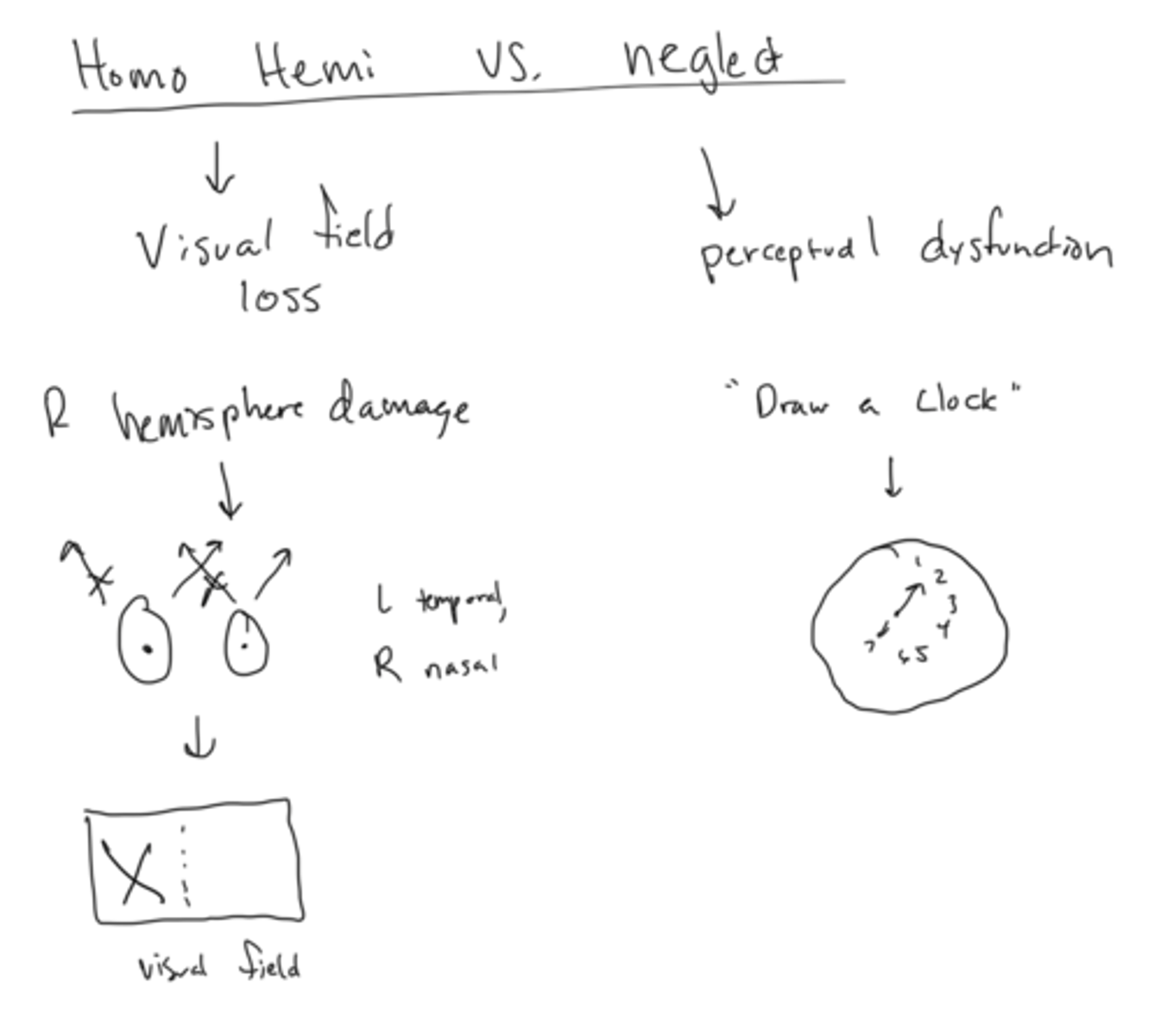
Homonymous Hemianopia vs Unilateral Neglect
Homonymous Hemianopia- visual field loss causing inability to see contralateral half of vision
Unilateral neglect- perceptual dysfunction causing inattention to contralateral side
What is spatial perceptual dysfunction
Incorrect perception of self, illness, or self in space
Agnosia vs Apraxia
Agnosia: inability to recognize an object by sight, touch, or hearing
Apraxia: inability to perform specific purposeful actions
Ideational apraxia
inability to formulate an initial motor plan and sequence tasks where the proprioceptive input necessary for movement is impaired
"Inability to figure out what a pen does vs what a toothbrush does"
Ideomotor apraxia
the inability to carry out a simple motor activity in response to a verbal command, even though this same activity is readily performed spontaneously
"Inability to pick up and object off the floor if asked, but does it on own"
What is the difference between ideation apraxia and form discrimination
Ideation apraxia is inability to use pen correctly
Form discrimination is inability to tell the difference between a pen and a straw (does not have to do with what their function is)
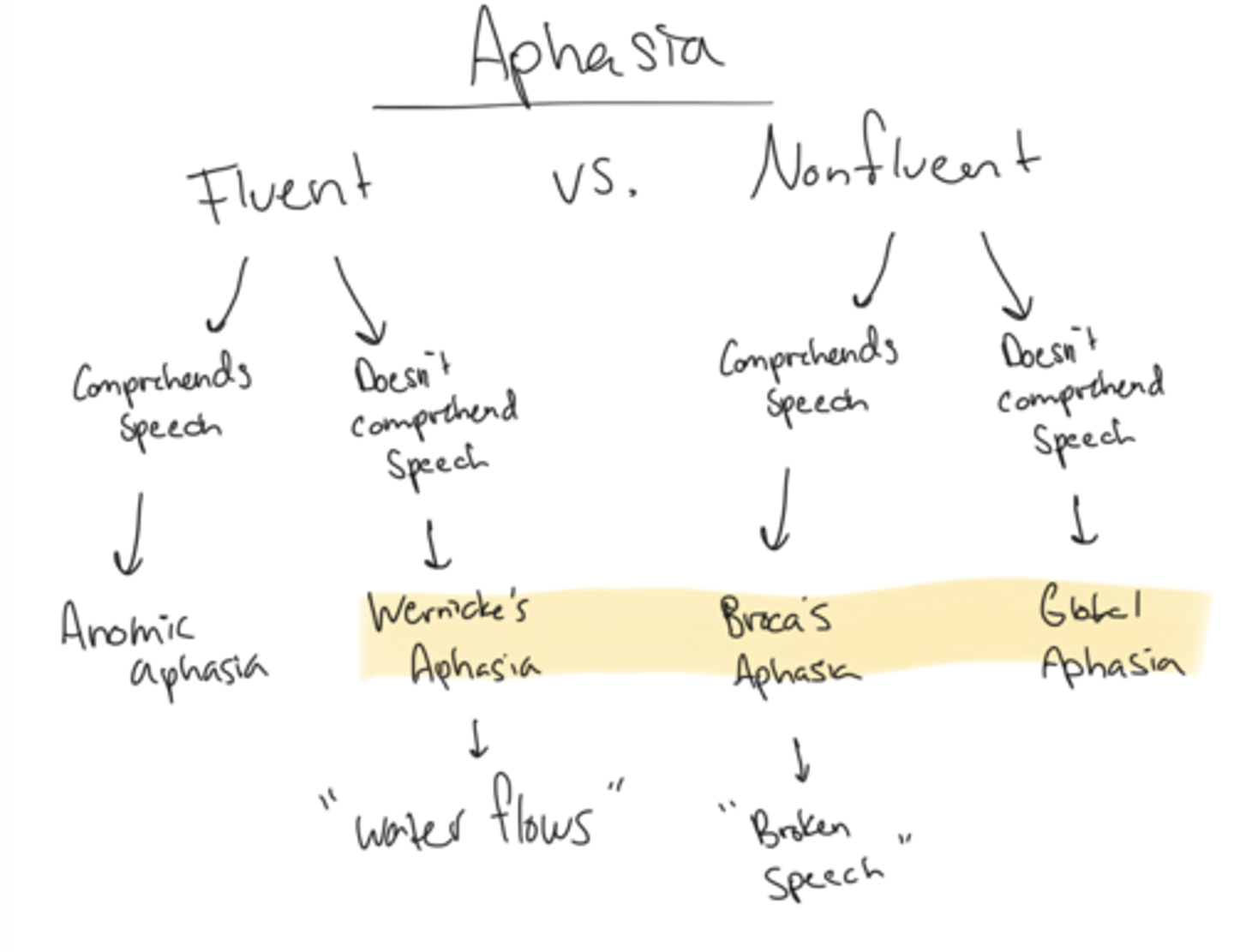
Wernicke's Aphasia
Fluent, does not comprehend speech
"Water flows"
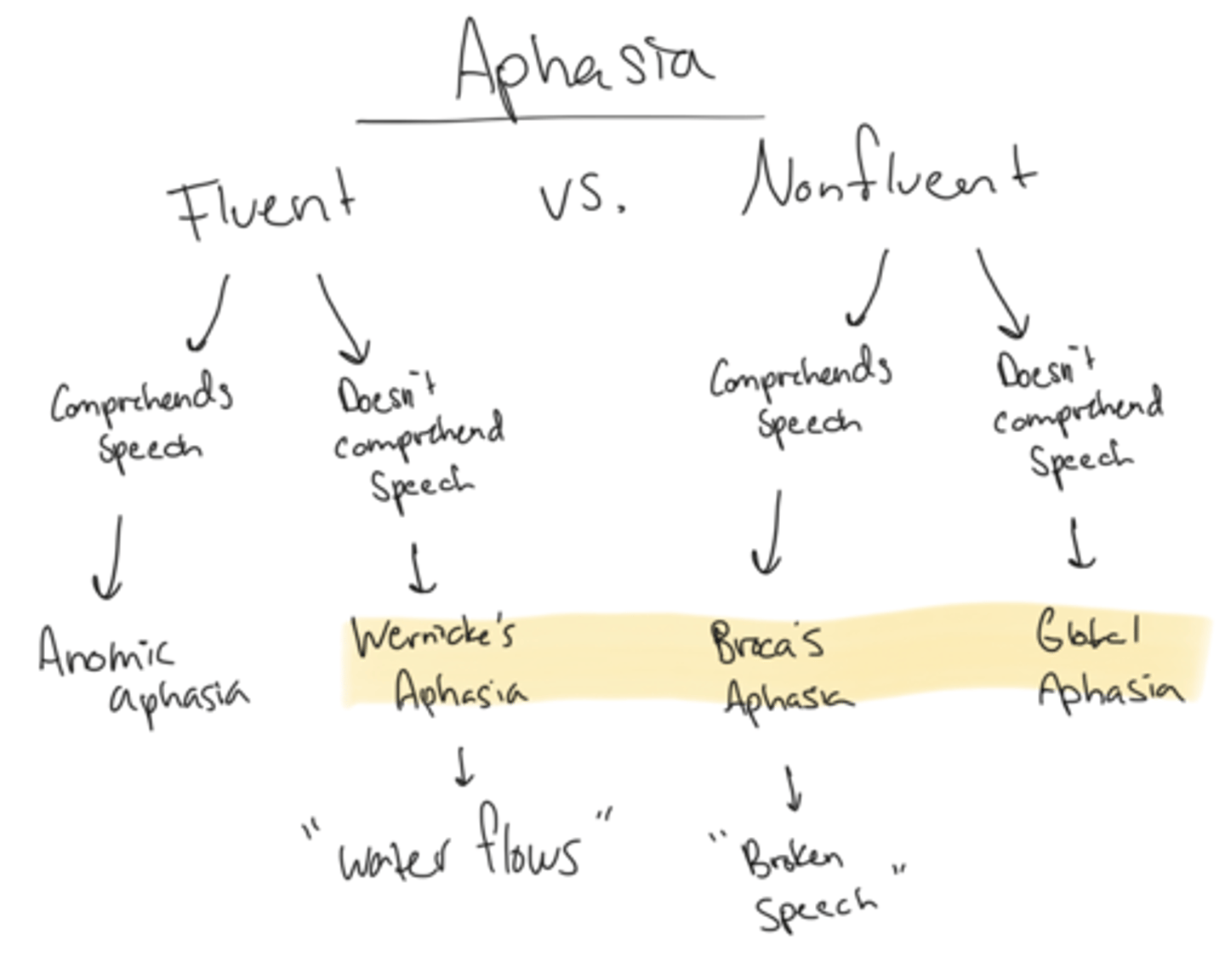
Broca's Aphasia
Nonfluent, comprehends speech
"Broca Broken Speech"
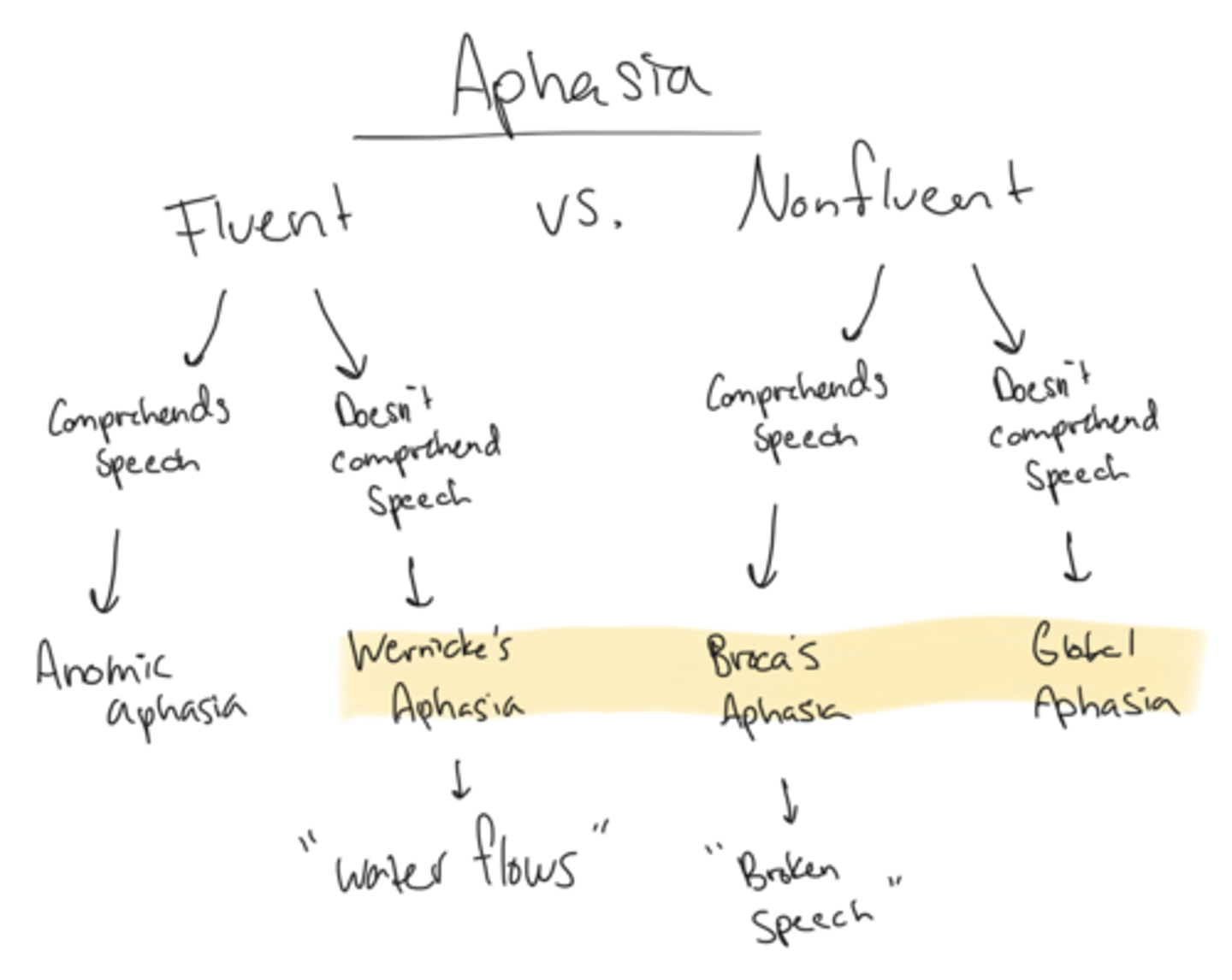
Global Aphasia
Nonfluent + does not comprehend speech
Where is lesion Wernicke's Aphasia
L Lateral temporal lobe
Where is lesion Broca's Aphasia
L frontal lobe
Right vs Left CVA symptoms
Right: "like babies"
- L weakness
- L neglect, perceptual issues
- Poor judgement, impulsive
- Short attention span, short term memory loss
- Weak facial muscles
- Cognitive problems
Left: "like old people"
- R weakness
- Aphasia
- Cautious, disorganized, slow
- Difficulty conceptualizing
- Dec memory
UE flexion synergy
- Scapular retraction/elevation
- shoulder abduction, external rotation
- elbow flexion
- forearm supination
- wrist and finger flexion*
LE extension synergy
- Hip extension, adduction, IR
- knee extension
- PF/INV
- Toe ext
Brunnstrom's Stages of Recovery
1-flaccid
2-spasticity begins to develop
3-voluntary movements begin within basic limb synergies. spasticity reaches its peak.
4-limb movements outside limb synergies
5-spasticity present but decreases
6-disappearance of spasticity. coordinated joint movements
7-normal mm function restored
Positioning strategies: Supine
UE:
- scap pro
- shld flex + abd
- elbow ext
- wrist neutral
- fingers ext, thumb abd
- UE supported on pillow
LE:
- hip flexed
- Knee supported to stop hyperext
- Splint to keep foot neutral (nothing on sole of foot)
Positioning strategies: S/L on affected side
UE
- Scap pro
- Shld flex + abd + slight ER
- Elbow ext
- Forearm sup
- Wrist neutral
- Fingers ext, thumb abd
LE
- Hip ext
- Knee flex with pillow support
Positioning strategies: S/L on unaffected side
Pillow under ribs to elongate hemi side
UE:
- Scap pro
- Shld flex
- Elbow ext
- Wrist neutral
- Fingers ext, thumb abd
- UE supported on pillow
Positioning strategies: Seated
Trunk extended
UE:
- Scap pro
- Shld flex, arm on trough or lapboard
- Elbow resting
- Wrist neutral
- Fingers ext, thumb abd
LE:
- Hip flex to 90
Pusher Syndrome
significant lateral deviation toward the hemiplegic side. More common in patients with a right CVA.
Pusher Syndrome Treatment
Actively correct (PT sit on stronger side, ask pt to lean into you)
Mirror therapy beneficial
How to remember PNF UE patterns
"Eat before War"
PNF UE D1 flex + ext
"Eating"
Flex:
- Shld flex, add, ER
- Forearm sup
- Wrist radial flex
Ext:
- Shld ext, abd, IR
- Forearm pro
- Wrist ulnar ext
PNF UE D2 flex + ext
"Sword pull"
Flex:
- Shld flex, abd, ER
- Forearm sup
- Wrist radial ext
Ext
- Shld ext, add, IR
- Forearm pro
- Wrist ulnar flex
PNF Chop
Strong arm performs D2 ext, which makes weak arm perform D1 ext
PNF Lift
Strong arm performs D1 flex, which makes weak arm perform D2 flex
LE D1 flex + ext
Flex
- Hip flex, add, ER
- Knee flex or ext
- Ankle DF, inv
- Toe ext
Ext
- Hip ext, abd, IR
- Knee flex or ext
- Ankle PF, ev
- Toe flex
LE D2 flex + ext
"Fire hydrant"
Flex
- Hip flex, abd, IR
- Knee flex or ext
- Ankle DF, EV
- Toe flex
Ext
- Hip ext, add, ER
- Hip flex or ext
- Ankle PF, inv
- Toe flex
Glasgow Coma Scale
Eyes opening
4 spontaneous
3 sound
2 pain
1 never
Verbal
5 oriented
4 confused
3 inappropriate
2 sounds
1 nothing
Motor
6 obeys commands
5 localizes pain
4 flexion withdrawal
3 abnormal flex
2 extension
1 no response
Glasgow Coma Scale scoring
Mild: 13-15
Moderate: 9-12
Severe: <8
Decorticate vs Decerebrate
Decorticate: UE flex, LE ext
Decerebrate: UE ext, LE ext
Ranchos Los Amigos Cognitive Functioning Scale
Level 1- no response
Level 2- General response
Level 3- Local response
Level 4- Confused agitated
Level 5- Confused inappropriate
Level 6- Confused appropriate
Level 7- automatic appropriate
Level 8- purposeful appropriate
RLA Cognitive Function Scale and their needed assistance
Lvl 1-3 Total assist
Lvl 4-5 Max assist
Lvl 6 Mod assist
Lvl 7 Minutes assist
Lvl 8 Supervision assist
A physical therapist is working with a 53-year-old male retired physician. The patient had a stroke that affected his anterior cerebral artery. Which of the following presentations is the patient MOST likely going to display?
A. Contralateral hemiparesis of LE, urinary incontinence, apraxia, and contralateral hemisensory loss of LE
B. Contralateral hemiparesis of UE and face, contralateral hemiparesis of UE, global aphasia, and ataxia
C. Contralateral homonymous hemianopia, prosopagnosia, visual agnosia, and memory defect
D. Ipsilateral paralysis of conjugate gaze, nystagmus, diplopia on lateral gaze, and paresis of face, UE, and LE.
A
A PT commands a patient to pick a pen amongst straws, but he is unable to complete the task due to inability to find pen. Which of the following is the MOST APPROPRIATE diagnosis to document this deficit?
A. Form discrimination
B. Figure-ground discrimination
C. Position in space impairment
D. Ideational apraxia
A
A patient with a recent episode of right-sided cerebral infarct presents with perceptual deficits and poor awareness of their impairments. Which of the following strategies is LEAST likely to be recommended while treating this patient?
A. Using more verbal cues/commands while treating the patient
B. When in supine position, L scapula should be protracted and
shoulder slightly abducted
C. Using visual cues while treating the patient
D. When in L side lying position, left hip should be extended and
knee flexed and supported by pillows
C
A PT is evaluating an 86 years old female who sustained a right CVA due to an MCA infarction 3 weeks ago. Patient has the classical signs and symptoms of MCA CVA. During the initial evaluation, the PT performs reflex testing on the patient. Which of the following should the PT expect on assessment?
A. Right side hyperreflexia and - Babinski
B. Right side hyporeflexia and + Babinski
C. Left side hyperreflexia and + Babinski
D. Left side hyporeflexia and - Babinski
C
A 82-year-old patient suffered a right sided CVA about a week ago. The therapist is educating him on various positioning strategies. Which of the following is the MOST appropriate while lying on the left side?
A. Head/neck: neutral, left Scapular protracted; L arm in slight abduction and external rotation; elbow extended, forearm supinated, wrist neutral, fingers extended, and thumb abducted.
B. Head/neck: neutral, left Scapular retracted; L arm in slight abduction and internal rotation; elbow extended, forearm pronated, wrist neutral, fingers extended, and thumb adducted
C. Head/neck: neutral, right Scapular retracted; L arm in slight abduction and internal rotation; elbow extended, forearm pronated, wrist neutral, fingers extended, and thumb adducted
D. Head/neck: neutral, left Scapular protracted; L arm in slight adduction and external rotation; elbow flexed, forearm supinated, wrist extended, fingers flexed, and thumb abducted.
A
A patient diagnosed with Parkinson's Disease exhibits a forwardstooped posture. As part of the patient’s care plan the PT selects a number of active exercises that promote improved posture. Which PNF pattern would be the MOST appropriate to achieve the PT’s objective?
A. D1 Extension
B. D1 Flexion
C. D2 Extension
D. D2 Flexion
D
A patient suffered a traumatic brain injury from a fall out of bed resulting in a subdural hematoma. When intervening the patient, the clinician finds the patient opens their eyes to speech, and they make conversation but use inappropriate words. Upon examination, the patient withdrawals from touch and rolls their eyes. What level of severity would the patient MOST LIKELY be classified as?
A. Mild
B. Moderate
C. Severe
D. Very Severe
B
A PT is treating a patient with traumatic brain injury. The patient is classified as confused and agitated per the RLA classification. The patient also has memory impairments and is unable to recall the day/location or the activities performed in the previous sessions. Which of the following is the LEAST appropriate recommendation for the physical therapist?
A. Establish a daily routine for the patient
B. PT should orient the patient place and time frequently
C. Challenge the patient to provide the location/date and PT should
not give that information
D. Use chart/white board in the patient’s room to document
progress for the patient
C