HHD- UNIT 3 AOS 2: Promoting health and wellbeing
1/94
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
95 Terms
Public health
Refers to the ways in which governments monitor, regulate and promote health status and prevent disease in the population.
is concerned with the organisation and collective effort to improve the health status of the entire population
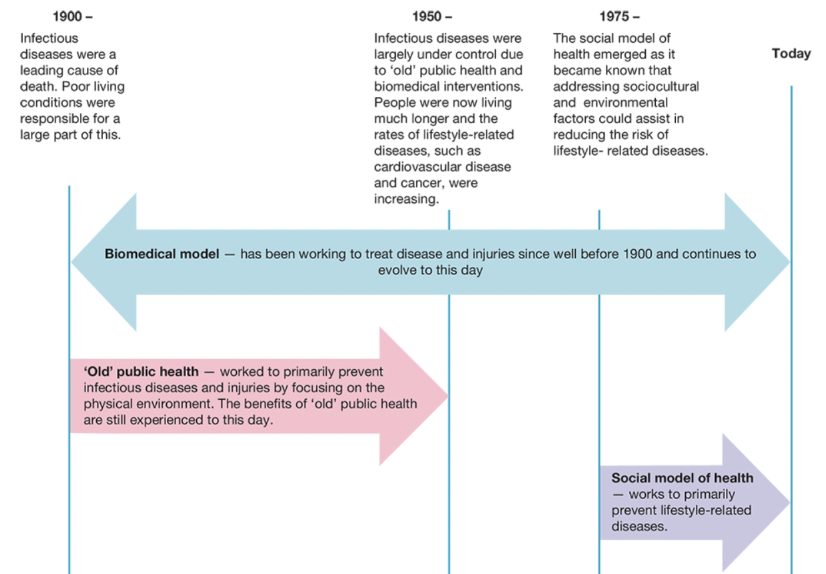
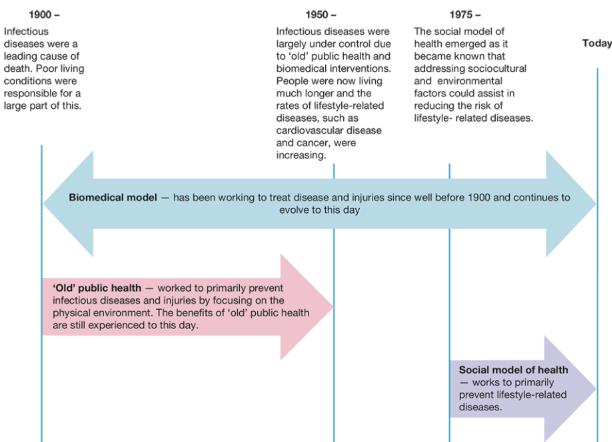
Changes in health from 1900 - Now
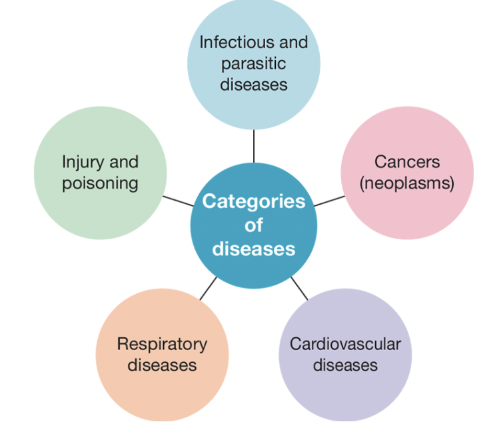
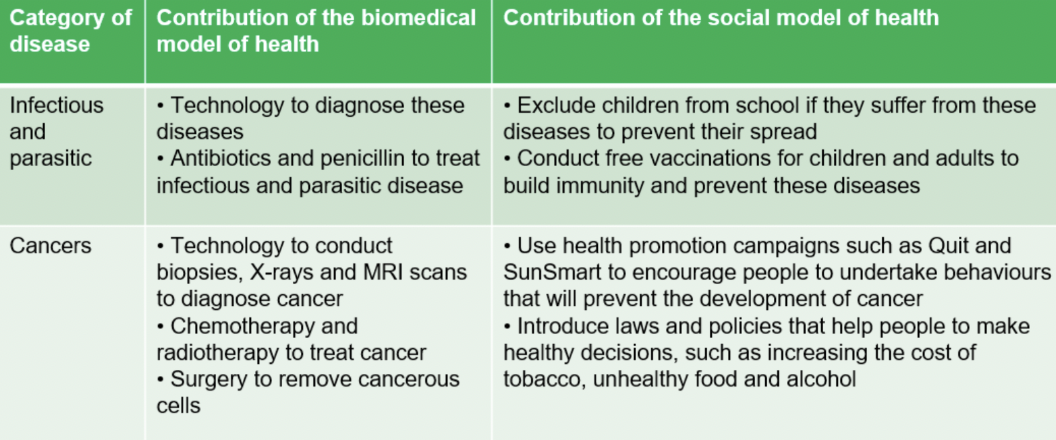
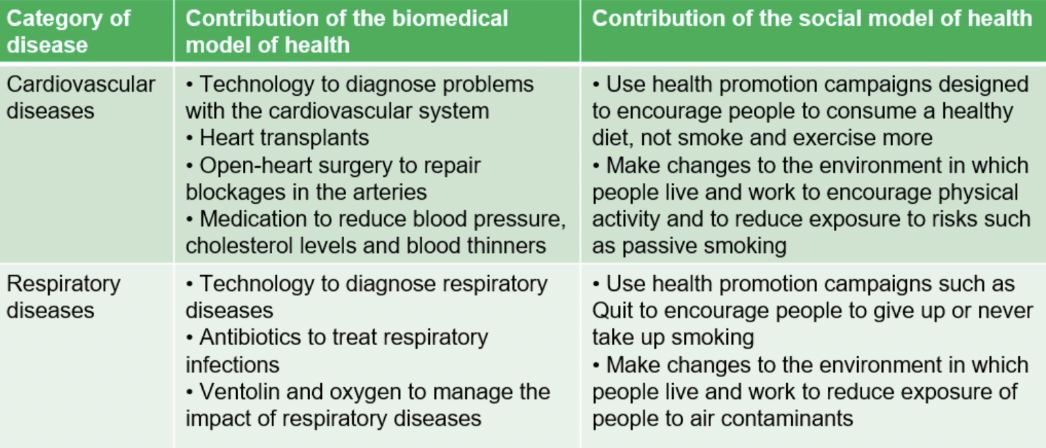
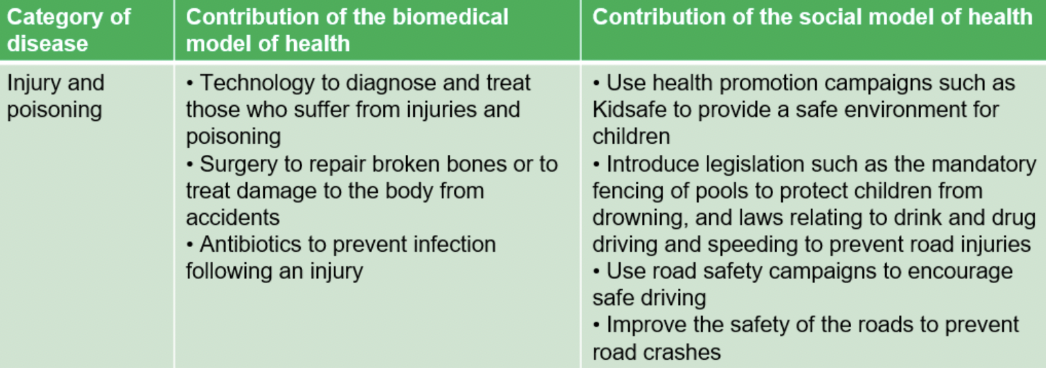
Categories of diseases
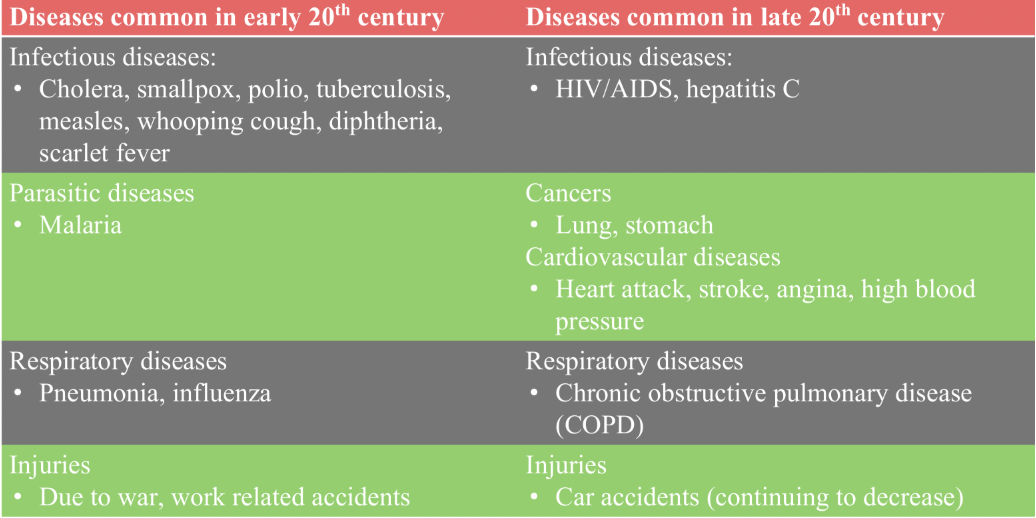
Common diseases in early 20th century vs late 20th century
OLD PUBLIC HEALTH
Bacteria was found to be the main cause of disease and death in the early 20th century
Living conditions were poor, clean water and sanitation was minimal, waste littered the streets (rats and mice carried disease), overcrowding in homes, food quality and storage was poor, working conditions were dangerous.
Focus on improving the physical environment became known as the 'old' public health
The government invested in water and sewage systems, better sanitation, improved nutrition, improved housing conditions and better work conditions (among other things!)
Initiatives associated with 'old' public health

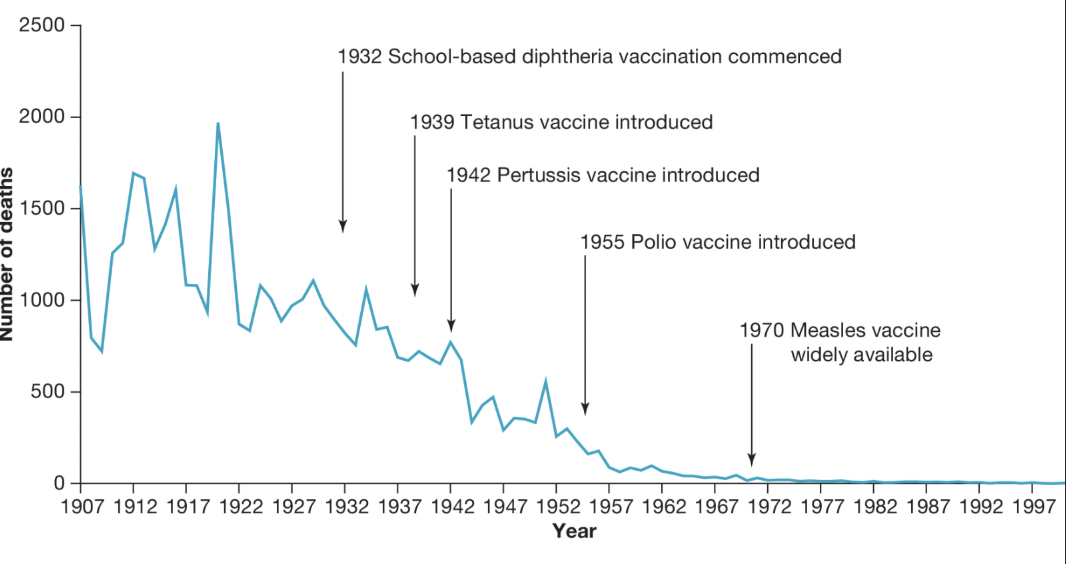
IMPROVEMENTS IN HEALTH
Many of the initiatives associated with 'old' public health were introduced alongside advancements in medical technology - specifically in relation to the diagnosis, treatment and monitoring of disease.
This is often referred to as the 'biomedical' approach and will be discussed in more detail in the next lesson.
Important to note that the discovery of vaccines themselves is not an 'old' public health initiative (it's biomedical), rather ensuring that as many people as possible received these vaccines through mass public vaccinations in schools/community settings is the 'old' public health initiative.
THE SHIFT TO HEALTH PROMOTION
The process of enabling people to increase control over and improve their health
By the 50's-60's, people were living longer and infectious diseases were now controlled and rapidly decreasing.
Lifestyles diseases such as CVD and cancer were quickly becoming the major cause of death, and a new approach to public health was needed.
This was when the 'new' public health (also called the social model of health), was introduced.
Health promotion campaigns, designed to focus on changing the behaviour of the individual in order to reduce ill health - were implemented.
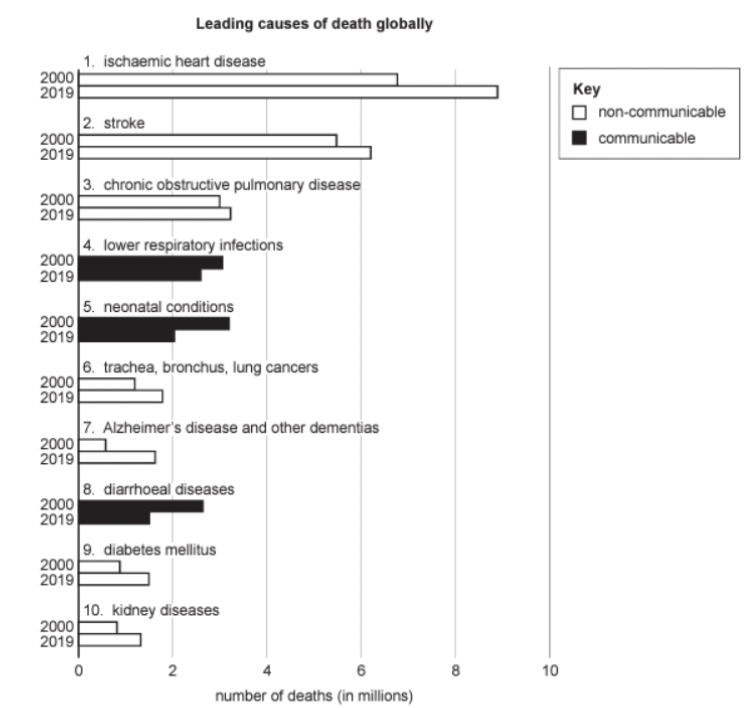
Leading causes of death globally
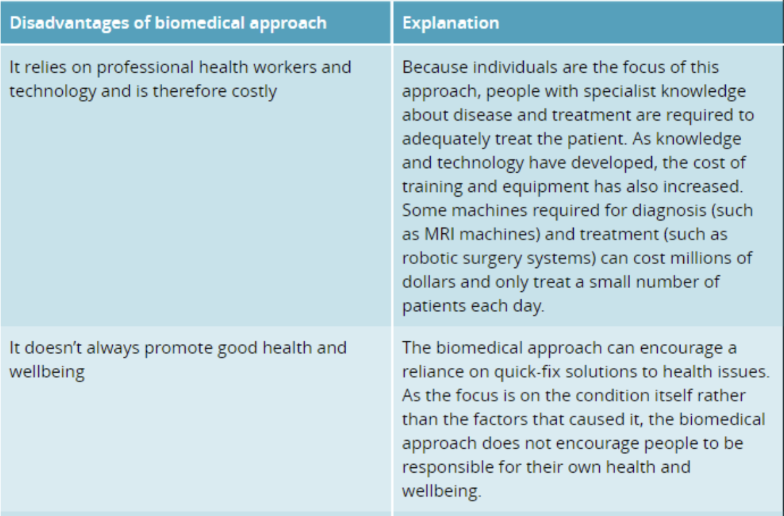
BIOMEDICAL APPROACH TO HEALTH
Focuses on the physical or biological aspects of disease and illness.
Focus is on the individual and the disease (not the cause) and returning the individual to their pre-illness state (contrast to the population-based focus of public health).
It accounts for a large proportion of the health budget (over 95%).
Often referred to as the 'quick-fix' or 'bandaid' approach
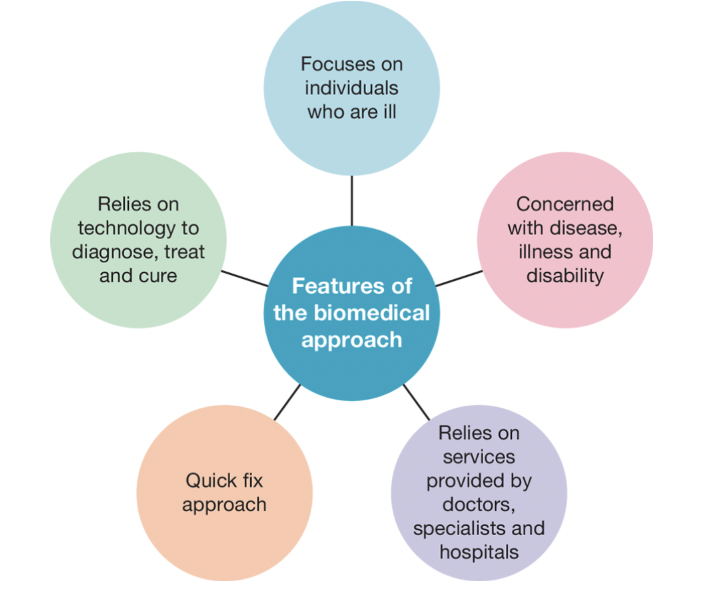
Features of the biomedical approach
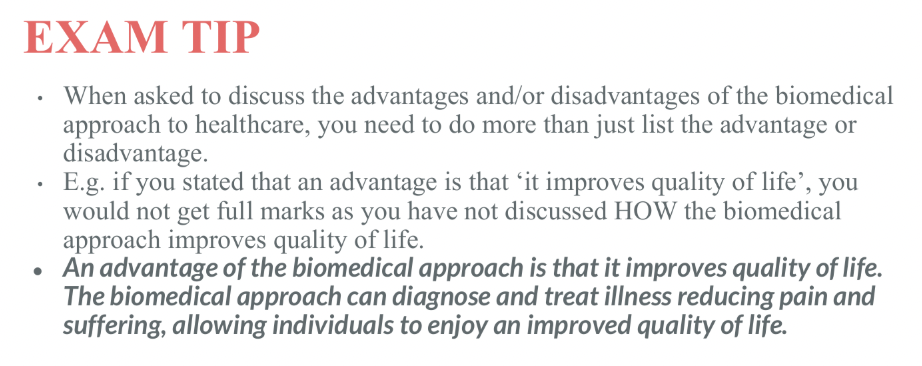
EXAM tip for + & - of biomedical approach
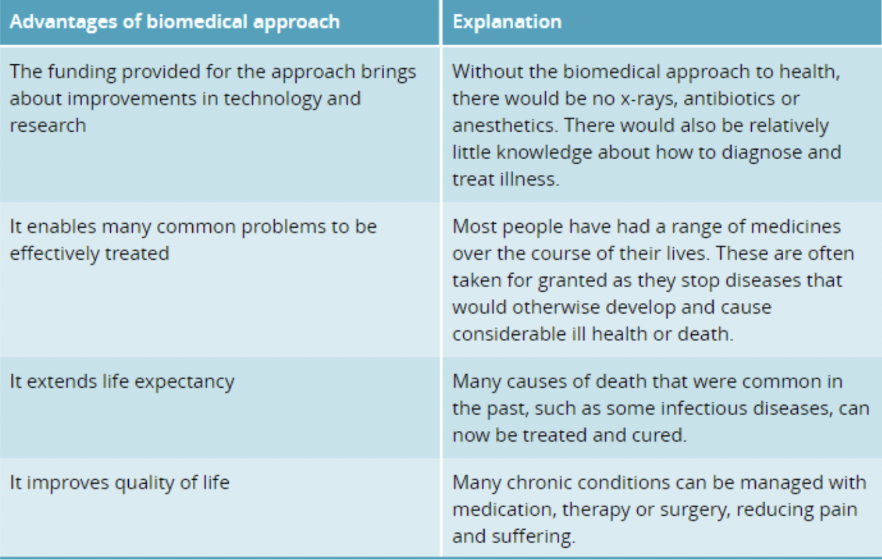
Pros of biomedical approach
Cons of biomedical approach
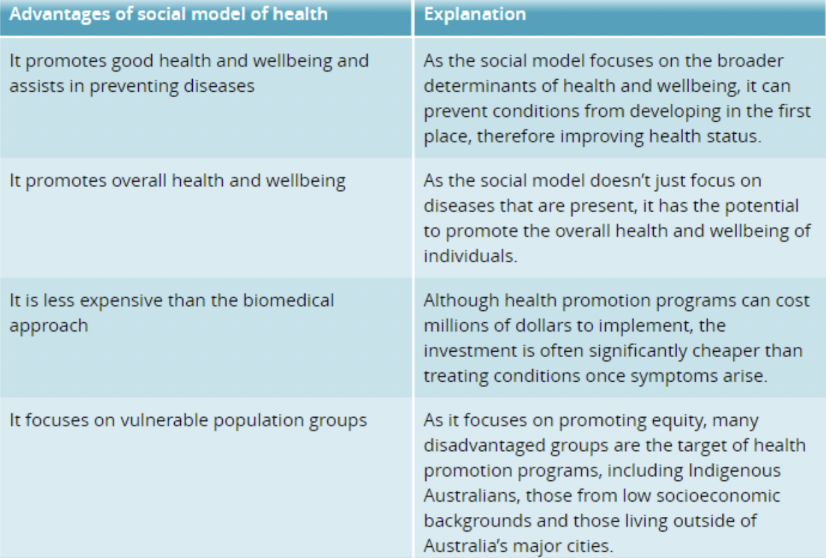
Social model of health
Once infectious diseases were controlled (thanks to old public health and the biomedical model), focus shifted to the lifestyle diseases and their contribution to mortality and morbidity (around 1970s)
- Although biomedical interventions could treat some cases, many ended in death.
Another approach was needed that encouraged people to lead healthier lives.
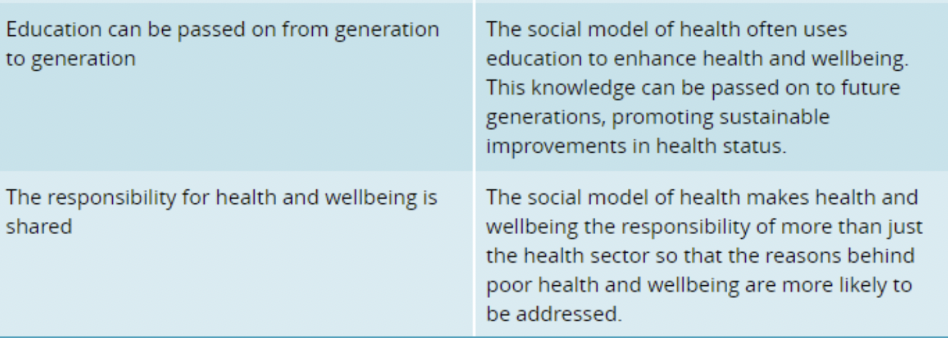
The social model of health (also referred to as 'new' public health) now focused on health promotion (the process of enabling people to increase control over, and improve their health through understanding the consequences of health behaviours)
Physical, sociocultural and political environments were recognized as having an impact on health, rather than just the individual and their choices
DEFINING FEATURES (prevention, community approach, disadvantaged groups)
The social model of health takes into account the significant role that Sociocultural factors (socioeconomic status, access to healthcare and social connectedness) plays in bringing about improved health status.
If we can address these factors (e.g. through education.policies, and health promotion activities), than many of these diseases can be prevented.
More of a community approach, as opposed to individual focus of biomedical approach
Aims to improve the health status of disadvantaged groups
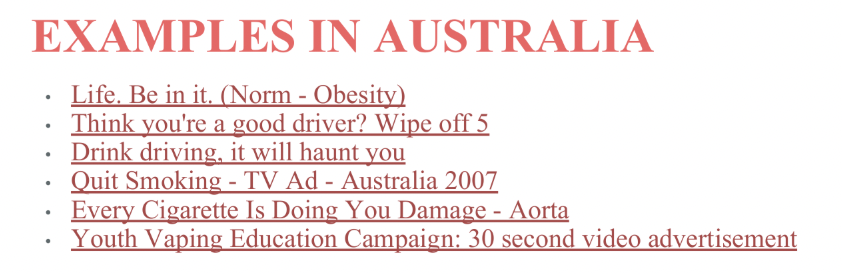
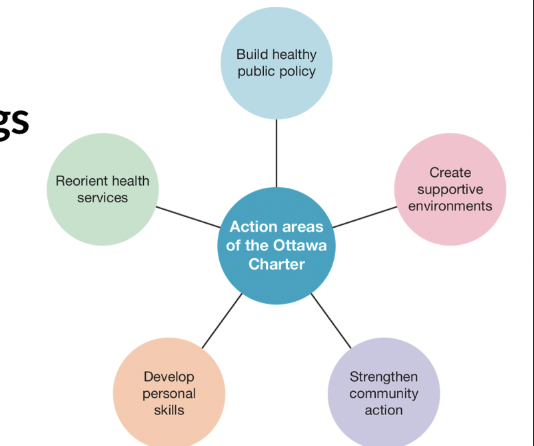
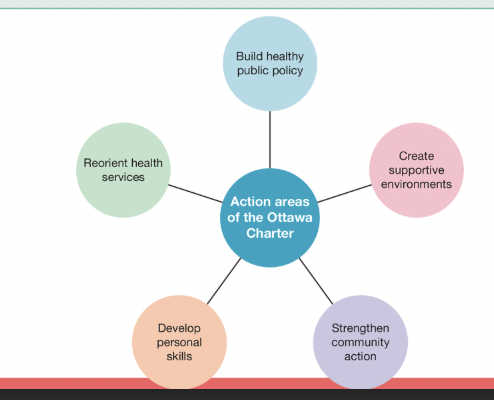
OTTAWA CHARTER FOR HEALTH PROMOTION
Developed at the World Health Organisation's first International Conference on Health Promotion held in 1986 in Ottawa, Canada
This framework aims to assist government and non-government organisations in implementing the social model of health.
This is where the health promotion definition was created
- The process of enabling people to increase control over, and improve their health through understanding the consequences of health behaviours
Health promotion
Guidelines to how key organisations and stakeholders promote all the health promotion ideas,
Action areas of Ottawa Charter
Build healthy public policy
Relates directly to the decisions made by government and organisations regarding laws and policies that make it more difficult for people to undertake unhealthy behaviours and seek to make healthier choices the easier choices.
eg:
Banning smoking in public places, which makes the environment healthy for everyone
Compulsory wearing of seatbelts, which aims to directly influence behaviour
Increasing the tax on tobacco and alcoholic drinks, which aims to discourage unhealthy behaviour by making them more expensive
Create supportive environments
Recognises the impact that the broader determinants have on health and wellbeing and health status
Aims to promote a healthy physical and sociocultural environment for all members of the community
A supportive environment is one that promotes health and wellbeing by being safe, stimulating, satisfying and enjoyable
Strengthen community action
Focuses on building links between individuals and the community, and centres around the community working together to achieve a common goal
Giving the community a sense of ownership of a health and wellbeing strategy and working together increases the likelihood that it will be effective
Develop personal skills
Education is the main aspect of this action area. Education refers to gaining health-related knowledge and skills that allow people to make informed decisions that may indirectly affect health and wellbeing (such as talking to people to resolve conflict rather than using violence or teaching people the skills they need to cook a healthy meal).
Education can occur in many places, including school and work settings, families, and government and non-government organisations
Reorient health services
Refers to changing the health system so that it promotes health and wellbeing rather than just focusing on diagnosing and treating illness, as is the case with the biomedical model
Addressing all factors that influence health and wellbeing, not just diseases. This requires a shift towards health promotion, which includes doctors taking on the role of educator.
OTTAWA CHARTER FOR HEALTH PROMOTION
Developed at the World Health Organisation's first International Conference on Health Promotion held in 1986 in Ottawa, Canada
This framework aims to assist government and non-government organisations in implementing the social model of health.
This is where the health promotion definition was created: The process of enabling people to increase control over, and improve their health through understanding the consequences of health behaviours.
Action Areas of the Ottawa Charter: Ben Cousins Smoked Drugs Regularly
ACTION AREA 1: BUILD HEALTHY PUBLIC POLICY
Relates directly to decisions made by government and organisations regarding laws and policies that make it more difficult for people to undertake unhealthy behaviours
Seek to make healthier choices the easier choices.
Examples include:
Removing GST on unprocessed foods that are healthier
Increasing tax on cigarettes and alcohol (discourage by making more expensive)
Compulsory wearing of a seatbelt (directly influencing behaviour)
Banning smoking in public places (makes the environment healthy for everyone)
Children in childcare have to be immunised
Mandatory pool fences
ACTION AREA 2: CREATE SUPPORTIVE ENVIRONMENTS
Recognises the impact that the broader factors have on health and wellbeing and health status and aims to promote a healthy physical and sociocultural environment for all
members of the community.
A supportive environment is one that promotes H&W by being safe, stimulating, satisfying and enjoyable.
Examples include:
Providing a safe working environment
Having shaded areas in schools/playgrounds/outdoor areas (reduce UV exposure)
Resources such as Quitline (support service for smokers wanting to quit)
Bike paths that have adequate lighting
Investing in sustainable energy production
ACTION AREA 3: STRENGTHEN COMMUNITY ACTION
Focuses on building links between individuals and the community, and centres around the community working together to achieve a common goal.
Gives the community a sense of ownership over a strategy.
People working together increases the likelihood that it will be effective.
Examples include:
Community immunisation program that involves media, doctors, schools and parents working together to achieve higher immunisation rates for children
Central Australian Aboriginal Congress - health service run by Aboriginal people for Aboriginal people in Alice Springs. Focus is on providing health care, education and advocacy. Rates of participation are high because people feel connected.
ACTION AREA 4: DEVELOP PERSONAL SKILLS
Focus on educating people to be more knowledgeable about their health, able to make informed decisions that affect their H&W.
If people have the skills to improve their H&W, they are more likely to do so.
Can occur in schools, work settings, family and government and non government organisations
Examples include:
A community health centre running cooking classes to learn how to cook healthy meals
Quit campaign educating people about the harmful effects of smoking
Talking to people to resolve conflict rather than using violence
Learning how to check your body for skin cancer
Educating parents about the importance of putting screen on their children when out in the sun.
ACTION AREA 5: REORIENT HEALTH SERVICES
Focus on promoting health and wellbeing (social) rather than focusing on diagnosing and treating illness (biomedical).
Flips what we use the healthcare system for and addresses ALL factors that influence H&W, not just diseases.
Doctors take on the role of educator
Examples include:
Having doctors discuss healthy eating, rather than just medication and surgery to reduce impact of CVD
Medical professionals recommend physical activity to prevent conditions such as type 2 diabetes.
Ambulance workers providing road safety sessions for high school students
Dietitian conducting cooking classes with an emphasis on achieving adequate nutrition
Pros of the social model of health
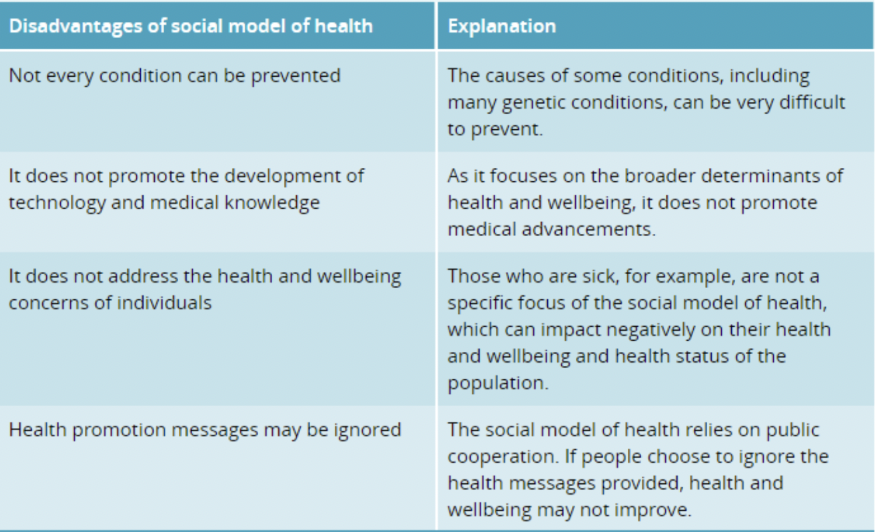
Cons of the social model of health
Relationship between models
Specific issues are targeted by health promotion in Australia for a number of reasons, including:
They contribute significantly to the burden of disease in Australia
They incur substantial economic costs through health care, absenteeism, loss of productivity and social security payments.
They are associated with considerable social impacts, such as avoidable deaths and inequalities between population groups.
They all have a modifiable component and, if addressed, significant components can be made.
Action areas of the Ottawn Charter
Quit
A program run y the Cancer Council Victoria, which is funded by the Victorian government and VicHealth, and is an example of strengthening community action.
Aims to decrease the use of both traditional cigarettes and e-cigarettes
Quit develops personal skills by providing information regarding tobacco smoking and vaping through public education using mass media advertising campaigns, public relations and downloadable information on the Quit website
Quitline is a telephone service that:
Creates supportive environments by providing support through the quitting process
Develops personal skills by providing advice and practical strategies for quitting.
Quit Victoria's Aboriginal Quitline strengthens community action by using Aboriginal and Torres Strait Islander Quit specialists with additional training to assist people with smoking or vaping cessation in a culturally appropriate way.
Quit undertakes research and provides advice to the state government to build health public policy.
Quit provides a free online learning training program for health professionals that assists in reorienting health services.
Impact of Quit Victoria on health and wellbeing
Reduced rates of smoking/vaping, resulting in higher levels of fitness in the population, promoting physical health and wellbeing.
Lower levels of diseases, which can reduce the levels of stress and anxiety in the community, because fewer people will develop life-threatening diseases, promoting mental health and wellbeing.
Impact of Quit Victoria on health status
A decrease in the prevalence of smoking related conditions such as cancer, cardiovascular disease and respiratory diseases
A reduction in premature death from smoking-related diseases and therefore increased life expectancy.
LiveLighter
LiveLighter works to help people to eat well, be physically active and avoid excess weight gain.
The program develops personal skills by providing fact sheets and a range of health recipes to download for free from its website
LiveLighter works to create supportive environments that make the healthy option the easy option by advocating for less promotion of junk food, better access to healthy food for all, improved junk food labelling and infrastructure, and policies to empower people to be more active.
The program strengthens community action by working with retailers, universities, community organisations and all levels of government to make it all happen.
LiveLighter reorients health services by providing professional development opportunities for health professionals (incl. GPs), that include topics such as *weight management training for health professionals' and 'talking to patients about health and weight".
LiveLighter develops healthy public policies that workplaces can use to promote healthy eating and physical activity. Policy templates are available to download for free from their website.
Impact of LiveLighter on health and wellbeing
Reducing rates of obesity can mean that people have more energy, promoting physical health and wellbeing.
Overweight and obesity can cause people to feel self-conscious, so reducing these conditions can contribute to higher levels of self-esteem among the population, promoting mental health and wellbeing.
Impact of LiveLighter on health status
Reducing rates of obesity can contribute to lower incidence of related conditions such as arthritis, depression and Type 2 diabetes
Reducing levels of obesity in the community can mean that fewer people die prematurely from heart attack and stroke, decreasing mortality rates.
Health services
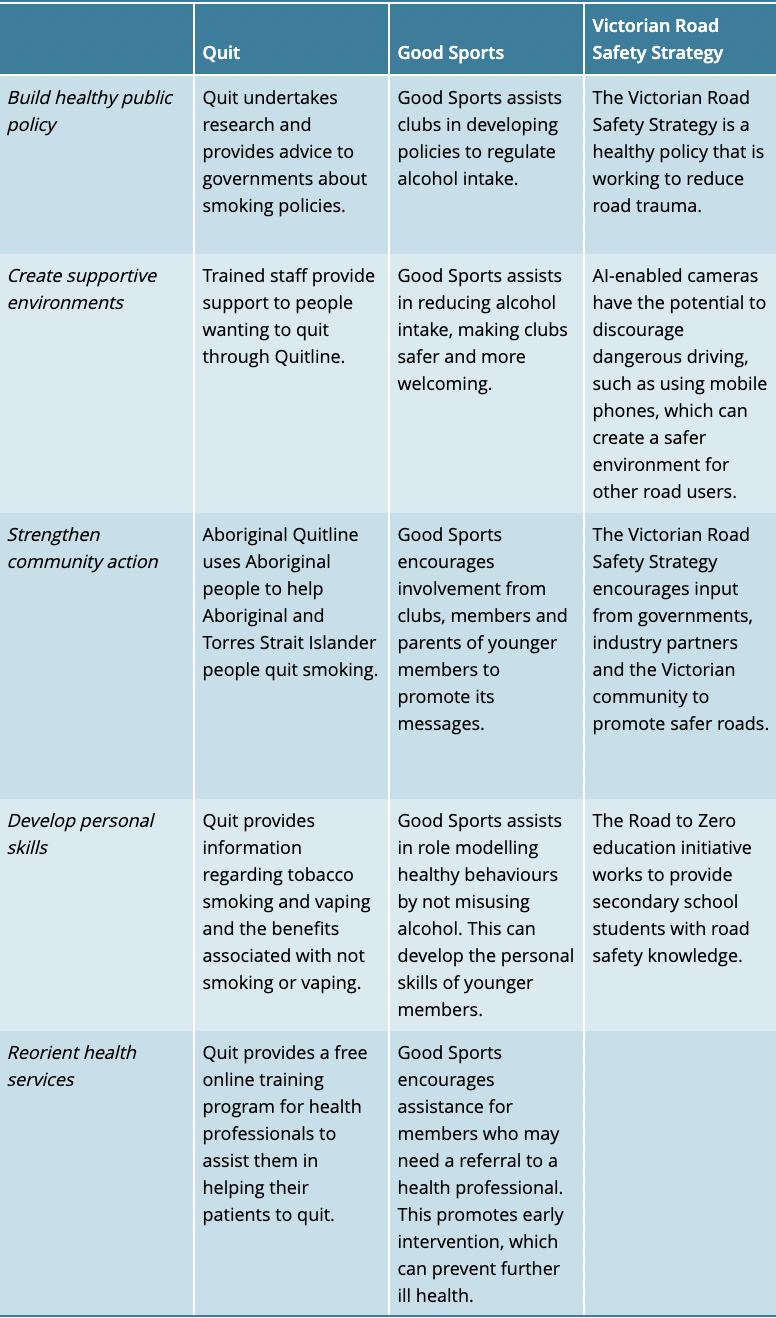
Overview of Victorian Road Safety
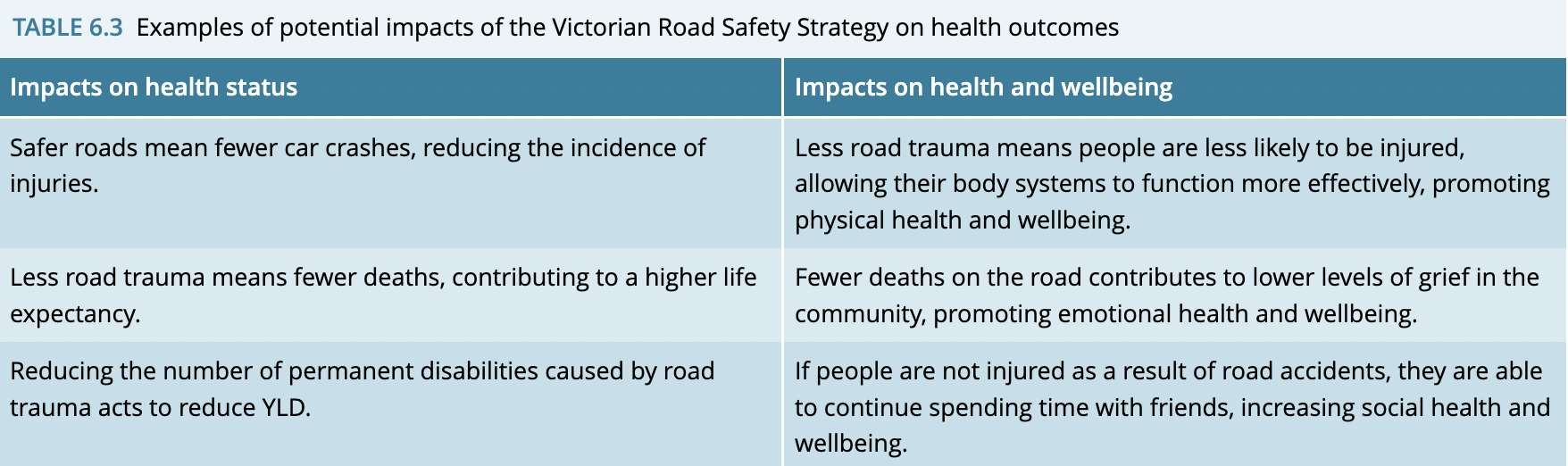
The Victorian Road Safety Strategy: a healthy policy that is working to reduce road trauma.
The Road to Zero education initiative works to provide secondary school students with road safety knowledge.
Aims to halve the number of deaths and significantly reduce serious injury on our roads over the next 10 years.
Eliminate all road deaths within three decades.
Vision for zero road deaths by 2025.
Al-enabled cameras have the potential to discourage dangerous driving, such as using mobile phones, which can create a safer environment for other road users.
The Victorian Road Safety Strategy encourages input from governments, industry partners and the Victorian community to promote safer roads.
How Victorian road safety address each action area of the OCHP
Build healthy public policy: Via the road rule implemented by Victoria police that requires motorists to leave at least 1 metre safe passing distance to keep cyclists safe.
Create positive environments: Investing over $41 million to support the employment of over 3,000 crossing supervisors who support children in a safe journey to and from school which helps to create supportive environments as more children are encouraged to walk and ride to school.
Strengthen community action: An action plan will be delivered by a group of road safety partners such as the department of transport, Victoria police and the transport accident commission.
Develop personal skills: As part of the action plan there will be an enhancement to the current RoadSmart program to teach young people a targeted road safety program aimed to identify risks on the road and teach the importance of vehicle safety and will support disadvantaged learner drivers to gain access to driving lessons.
Reorient health services: Under the strategy there is an investment in the road to zero education complex at the Melbourne museum which educates young drivers on the risks to help prevent road trauma.
How Victorian road safety improves health outcomes
Aboriginal and Torres Strait Islanders’ often experience poorer health outcomes than other Australians, including:
Life expectancy about 8.5 years less than other Australians
Higher mortality rates in each age group
Twice as likely to have a severe profound disability
Twice the rate of low birthweight babies and infant mortality than the rest of the population
Half as likely to rate health status as excellent or very good
Burden of disease rates 2.3 times higher than the non-Indigenous population
As a result of these variations, numerous programs have been implanted to promote Aboriginal and Torres Strait Islander Peoples' health.
HAPE principles of social justice
A focus on social justice ensures the underlying causes of disadvantage are addressed.
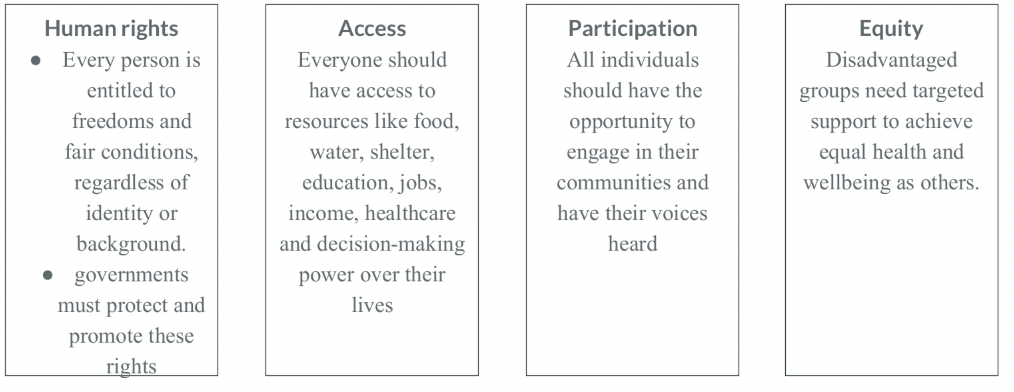
Social justice
Relates to fairness within society and is based on the principles of human rights, access, participation and equity.
Social Justice Principles
Closing the gap
Established to achieve health and life expectancy equality between Aboriginal and Torres Strait Islander Peoples and non-Indigenous Australians by 2030.
This commitment is known as 'Closing the Gap' and represents a healthy public policy.
Updated in 2020 to include Aboriginal and Torres Strait Islander groups in planning and implementation, which is an example of strengthening community action.
The focus was expanded to equality in all aspects of life, with a revised target year of 2031.
16 targets of closing the gap are to improve;
health
education
employment
housing (while reducing incarceration)
violence
suicide
Key targets include, by 2031:
Close the life expectancy gap
91% of babies born at a healthy weight
67% of youth (15-24) in employment, education, or training
88% living in appropriate housing
Significant reductions in violence, abuse, and suicide towards zero
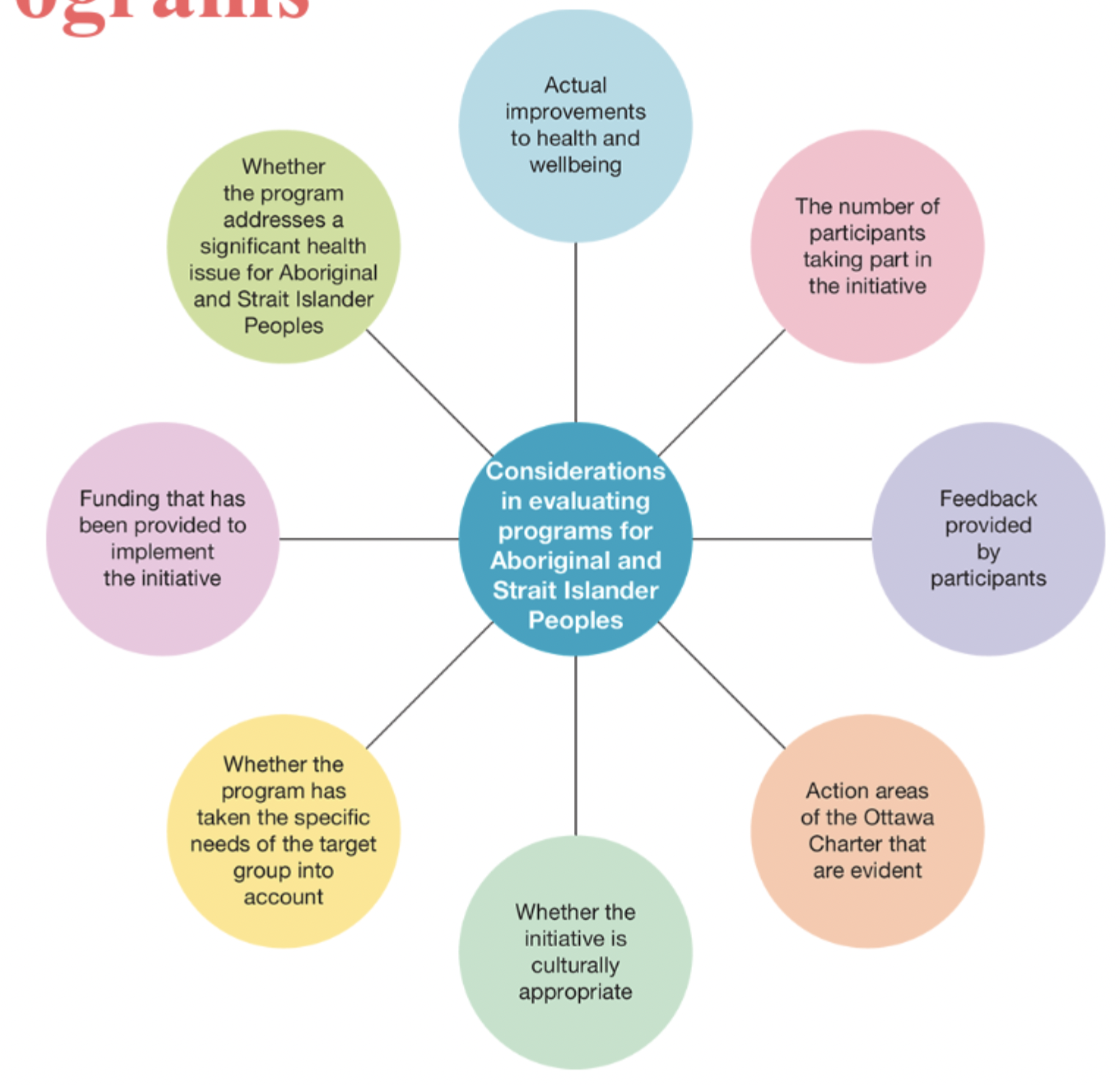
Evaluating Aboriginal and Torres Strait Islander Initiatives
Ensures effectiveness in improving Aboriginal and Torres Strait Islander health outcomes.
Helps direct limited funding toward the most successful programs.
Evaluation includes identifying effective features and potential limitations of programs.
(It is important that you can explain how a feature makes the program more or less effective and ensure a link is made to health outcomes if specified in the question).
Considerations in evaluating programs for Aboriginal and Strait Islander Peoples
Promoting Healthy Eating in Australia
A healthy diet lowers the risk of obesity, cardiovascular disease, some cancers and type 2 diabetes
Poor nutrition is a major contributor to Australia's disease burden, with cases expected to rise without behaviour changes (health promotion!)
Significant social and emotional impacts, affecting individuals and the broader community.
The federal government plays a key role in promoting healthy eating to reduce these health issues.
The Australian Dietary Guidelines
Developed by the National Health and Medical Research Council (NHMRC), with updates due in 2026.
Aims to combat rising diet-related diseases by promoting healthier food choices.
Target audience: Health professionals, educators, industry bodies, and the general healthy population.
Available for free on the government's 'Eat for Health' website in multiple formats for accessibility.
The Australian Dietary Guidelines provides advice relating to the types and amounts of foods, food groups and dietary patterns that will help Australians to:
Develop healthy dietary patterns that will promote health and wellbeing in the community
Reduce the risk of developing a range of diet-related conditions such as hypertension (high blood pressure) and impaired glucose regulation
Reduce the risk of developing chronic conditions such as type 2 diabetes, cardiovascular disease and some cancers
Considerations included for different groups:
Life stages (children, elderly, pregnant/lactating women)
Dietary preferences (vegetarian/vegan)
Cultural backgrounds (Indigenous Australians, Australians of Asian origin)
Location and socioeconomic factors (rural areas, lower-income groups)
There are 5 written guidelines with extra advice provided in relation to each one.
Guideline 1
To achieve and maintain a healthy body weight, be physically active and choose amounts of nutritious foods and drinks to meet your energy needs.
Children and adolescents should eat sufficient nutritious foods to grow and develop normally.
They should be physically active every day and their growth should be checked regularly.
Older people should eat nutritious foods and keep physically active to help maintain muscle strength and a healthy weight.
Guideline 2
Enjoy a wide variety of nutritious foods from the following five food groups every day and drink plenty of water
1. Plenty of vegetables, including different types and colours, and legumes/beans
2. Fruit
3. Grain (cereal foods), mostly wholegrain and/or high cereal fibre varieties, such as breads, cereals, rice, pasta, noodles, polenta, couscous, oats, quinoa and barley.
4. Lean meats and poultry, fish, eggs, tofu, nuts and seeds and legumes/beans.
5. Milk, yoghurt, cheese and/or their alternatives, mostly reduced fat (reduced fat milk are not suitable for children under the age of 2 years).
Drink plenty of water
Guideline 3
Limit intake of foods containing saturated fat, added salt, added sugars and alcohol.
Limit intake of saturated fats
Replace saturated fats with polyunsaturated and monounsaturated fats (oil, nut pastes, avocado)
Low fat diets are not suitable for children under the age of 2.
Read labels to choose options with lower amounts of sodium.
Do not add salt while cooking or eating
Limit confectionary, sugar-sweetened drinks, cordials, fruit drinks, vitamin waters, sports drinks
Limit intake of alcohol.
Guideline 4
Encourage, support and promote breastfeeding
Mothers are encouraged to exclusively breastfeed their children for the first 6 months after birth.
Children should be breastfed for 2 years.
Reduces the risk of infection.
Protective factor against obesity and hypertension.
Guideline 5
Care for your food; prepare and store it safely
Foodborne illnesses can have serious consequences
Care needs to be taken in purchasing, transport, storage, preparation, cooking, serving and cleaning.
Guidelines booklet
Contains the average number of serves required for different people
The booklet also contains serving sizes for the five main food groups, healthier fats and discretionary foods.
Discretionary foods: foods that are often high in saturated fat, added salt, added sugar and/or alcohol)
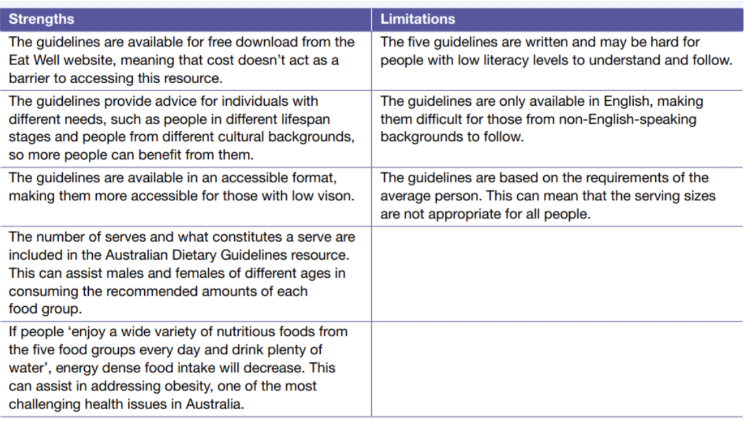
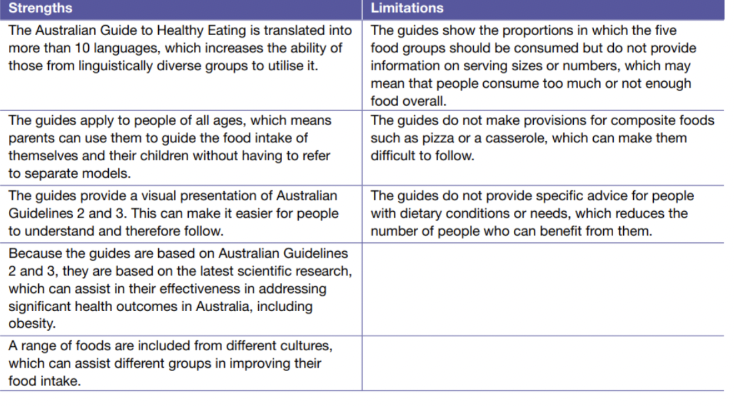
Pros and cons of The Australian Dietary Guidelines
The Australian Guide to Healthy Eating (AGHE)
Intended to be used by consumers (regular people) to assist them in planning, selecting and eating adequate portions of foods from the five food groups.
A visual tool that reflects the recommended dietary advice detailed in Australian Dietary Guidelines 2 and 3.
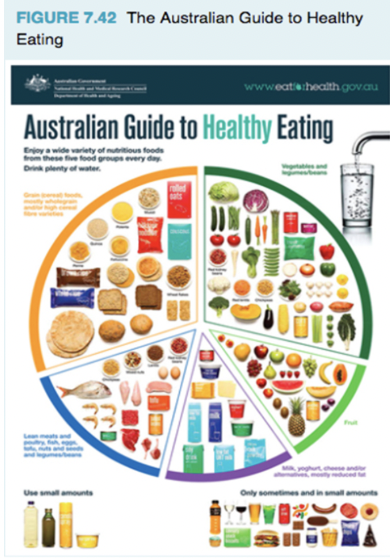
The Guide shows a circle divided into five wedges, each representing one of five food groups (Guideline 2).
The size of each wedge reflects the proportion of each food group that should be consumed daily.
The Five Food Groups
Grain
Vegetables/legumes/beans
Meat and meat alternatives
Fruit
Milk and other dairy products or alternatives
Grain
Foods are high in carbohydrates (provides fuel for energy) and fibre (assists in weight management and maintenance of digestive health)
Biggest wedge in the AGHE, should account for approx. 30-35% of daily food intake
Contains breads, cereal, rice and pasta
Vegetables/legumes/beans
Contains fresh, frozen and tinned vegetables, lentils, chickpeas, kidney beans etc.
Also rich in carbohydrates, fibre, protein (build, repair, maintain muscle cells) and antioxidants (fight free radicals - decreases damage to cells, reduced risk of cancer).
Second biggest wedge, should account for approx. 30% of daily food intake.
Meat and meat alternatives
Provide much of the protein needed for maintenance of cells and tissues and can be used as an energy source.
Account for approx. 15% of daily food intake.
Fruit
Contains many vitamins and minerals that contribute to overall optimal health and wellbeing.
Contains lots of carbohydrates, can contribute to weight gain if not used for energy.
Account for approx. 10-12% of daily food intake.
Milk and other dairy products or alternatives
Rich in calcium and required for optimal bone health.
- Account for approx. 10-12% of daily food intake.
Australian Guide to Healthy Eating Recommendations
Recommends people consume plenty of water, represented by an image of glass being filled from a tap.
The healthier fats (margarine, canola spray) are shown in the bottom left corner, stating they should be used in small amounts as part of a healthy diet.
Discretionary foods shown in the bottom right corner, indicating they should not be a regular part of the daily diet (Guideline 3)
Provides basic nutrition advice, does not include serving sizes, composite foods. This makes it more difficult to follow.
Aboriginal and Torres Strait Islander Guide to Healthy Eating
Adapted from the Australian Guide to Healthy Eating
Similarities between AGTHE and Aboriginal and Torres Strait Islander Guide to Healthy Eating
Shows the five food groups in the proportions in which they should be consumed
Promotes water consumption
Suggests to limit discretionary foods
Recommended to include small amounts of healthier fats
Differences between AGTHE and Aboriginal and Torres Strait Islander Guide to Healthy Eating
Includes references to traditional foods such as kangaroo, goanna and crab meat, bush fruits and vegetables and damper.
ATSIAGHE states 'eat different types of food from the five food groups every day, whereas the AGHE uses wording from Guideline 3 'enjoy a wide variety of nutritious foods from the five food groups every day'
Pros and cons of food selection models
Challenges in Bringing About Dietary Change
Australians have moved from nutrient-dense whole foods to energy-dense processed foods, thus increasing rates of obesity and diet-related diseases.
Health promotion efforts exist, but long-term nutritional change remains complex due to a range of factors we will explore today.
Factors
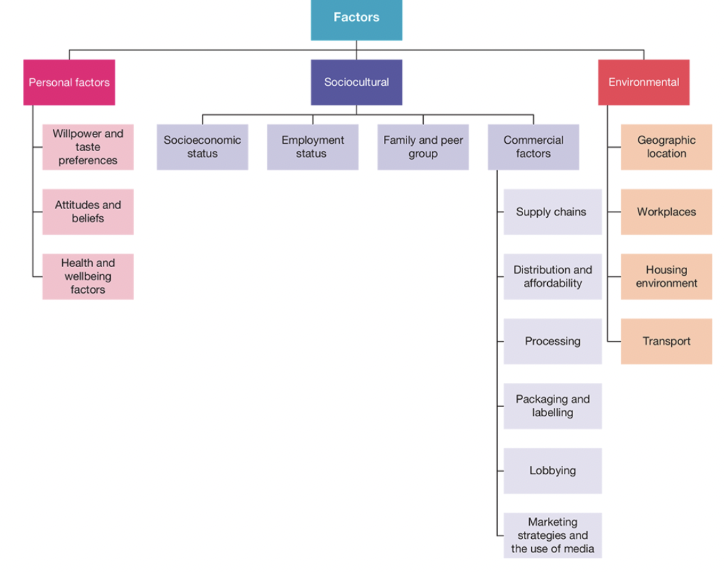
Personal Factors
Relate to characteristics of individuals that influence food intake.
Personal factors include:
Willpower and Taste Preferences
Attitude and Beliefs
Health and Wellbeing Factors
Willpower and Taste Preferences
Making lasting changes to food intake requires considerable willpower.
People often prefer certain foods due to taste preferences and past experiences.
Foods high in fat, salt and sugar stimulate taste buds and release dopamine, creating cravings.
Taste preferences are established over time and can be difficult to change.
Attitude and Beliefs
People may have perceptions that healthy. foods are bland or tasteless.
May ignore the negative effects of unhealthy foods.
Some people may have strong philosophical beliefs (e.g. vegetarian, organic preferences) that shape food intake.
Some restrict certain foods, leading to underconsumption.
Health and Wellbeing Factors
7% of Australians reported food allergies.
Many others have intolerances, particularly to cow's milk and gluten.
Cutting these foods can reduce adherence to health guidelines without knowledge of substitutes.
Certain foods trigger dopamine release, enhancing mood and emotional distress can lead to using food as a coping mechanism.
Sociocultural Factors
Influence of society and culture on food intake.
SES - Education:
Lack of nutritional knowledge and cooking skills leads to unhealthy meals Difficulty in reading food labels and understanding portion size can lead to unhealthy food selection and overeating
SES - Income
Directly affects food affordability and choices
Lower income limits access to healthy foods
SES - Occupation
Certain jobs (truck drivers, trades, night shift etc.) rely on convenient (often unhealthy) food options.
Employment status influences meal planning based on time and convenience.
Employed individuals may opt for convenience food due to time constraints.
Employment status
Families with both parents working spend less time preparing meals.
Convenience foods are often consumed due lack of time for fresh meal preparation.
Family Influence
Early food experiences are shaped by family, cultural and religious backgrounds
Childhood establishes personal food preferences, making
change difficult.
Peer influence
Children and young people may choose foods based on friends' preferences, limiting ability to choose healthier options.
Commercial Factors
Relate to the impact that the private sector has on health and wellbeing.
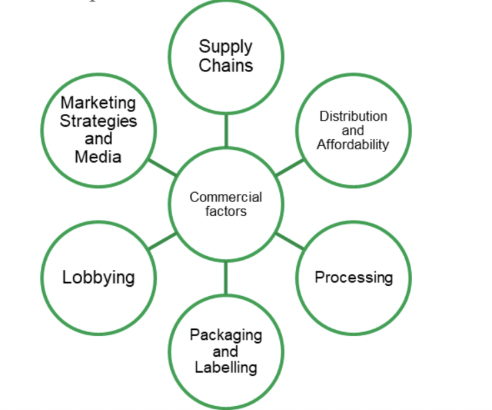
Supply Chains
Relate to the process that all foods go through, from where they are produced and consumed.
Supply chains influence food distribution, pricing, processing and packaging
Current example: avian influenza (bird flu) has led to large mortality rates of hens in egg farms, thus disrupting the supply chain as the amount of eggs being produced has massively decreased.
Distribution and Affordability
Food prices are set by the supermarket, restaurant or retailer and are affected by:
Wholesale cost (cost when bought from factory/farm before it gets to the supermarket).
Transport (e.g. more expensive if shipped or flown from overseas).
Storage (may require refrigeration/freezing)
Staffing
Cost of food is typically higher in rural areas (more difficult/time consuming to get food to these areas), affecting the availability and quality of nutritious food.
Processing
Food processing; involves transforming raw ingredients into consumable products.
This can range from simple methods like washing and cutting the food, o complex techniques like canning and freezing.
Processing can increase food safety and extend shelf life, however it often decreases the nutritional value of food.
Highly processed foods (which we know are extremely convenient and available everywhere), typically contain added sugars, fats, salt and preservatives, thus negatively influencing dietary patterns and health outcomes.
Packaging and Labelling
Packaging protects food and extends shelf life.
Can provide important information through labelling, such as nutritional content, ingredients and expiration dates.
Helps people make informed food choices.
Packaging can also mislead consumers through deception, which makes nutritional change difficult.
Lobbying
Is an attempt by individuals or private interest groups. to influence the decisions of government Think alcohol companies, soft drink companies etc.
Lobbying by food industry groups can significantly influence food policies and regulations which then impact the food environment.
This can directly affect what products are available, how they are produced and how they are marketed.
E.g. Pepsi Co, Coca Cola Australia and Asahi Lifestyle Beverages (includes brands such as Schweppes, Mountain Dew, Solo etc.) have actively opposed implementing a sugar tax in Australia).
Marketing Strategies and Media
Includes things such as:
Advertising
Celebrity endorsements
Social media campaigns
Can create demand for specific products, often focusing on energy-dense foods
Marketing strategies frequently target children and young adults, shaping their food preferences early on.