Oncologic or Degenerative Neurologic Disorders
1/17
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
18 Terms
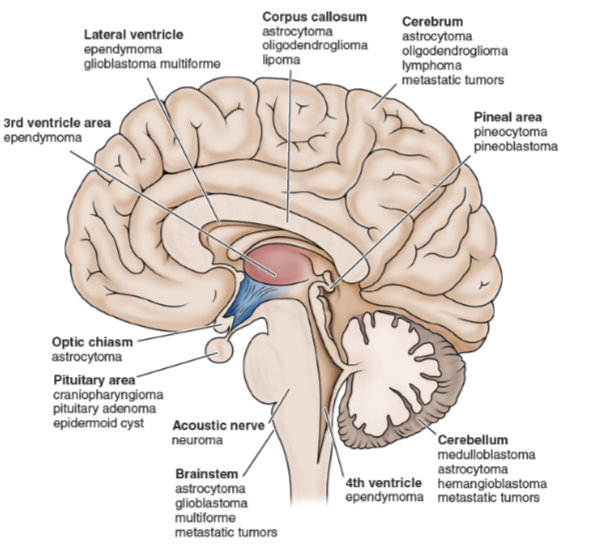
Brain tumors
Benign or malignant
Classification is based on location and histologic characteristics
Types of primary tumors
Gliomas
Meningiomas
Acoustic neuromas
Pituitary adenomas
Angiomas: masses of abnormal blood vessels
Metastatic tumors
Manifestations of Brain tumors
Symptoms depend on the location and size of the lesion and the compression of associated structures
Manifestations
Localized or generalized neurologic symptoms
Symptoms of increased ICP → Cushings triad: Bradypnea/ irregular Cheyne-Stokes, Bradycardia, HTN (widened pulse pressure)
Headache
Vomiting
Visual disturbances
Seizures
Hormonal effects with pituitary adenoma
Loss of hearing, tinnitus, and vertigo with acoustic neuroma
What are the common brain tumor sites and what are the diagnostic evaluation of brain tumors?
Neurologic examination
CT scan
MRI
PET scan
EEG
Cytologic study of cerebrospinal fluid
Biopsy
Medical management of brain tumors
Specific treatment depends on the type, location, and accessibility of the tumor
Surgery
Goal is removal of tumor without increasing neurologic symptoms or to relieve symptoms by decompression
Craniotomy, transsphenoidal surgery, stereotactic procedures
Radiation therapy
Cornerstone of treatment for many brain tumors
Chemotherapy
Pharmacologic therapy
Spinal Cord Tumors
Classified according to their anatomic relation to the spinal cord
Intramedullary: within the cord
Extramedullary: intradural; within or under the spinal dura
Extramedullary-extradural: outside the dural membrane
Manifestations include pain, weakness, loss of motor function, loss of reflexes, loss of sensation
Treatment depends on the type of tumor and location
Surgical removal
Measures to relieve compression: dexamethasone combined with radiation
Antinausea: Zofran
Assessment of the Patient with Nervous System Metastases or Primary Brain Tumors
Baseline neurologic exam with focus:
Patient function, moving, and walking; adapting to weakness and paralysis and to loss of vision and speech; dealing with seizures
Pain, respiratory symptoms, bowel and bladder function, sleep, skin integrity, fluid balance, and temperature regulation
Nutritional status and dietary history
Family coping and family process
Nursing interventions for patient with Nervous System Metastases or Primary Brain Tumors
Encourage independence for as long as possible
Measures to improve cognitive function
Allow patient to participate in decision making
Allow patient to express fears and concerns
Presence of family, friends, spiritual advisor, and health care personnel may be supportive
Referral to counselor, social worker, home health care, support groups
Referral for hospice care
Improving nutrition
Oral hygiene before meals
Plan meals for times when patient is comfortable and well rested
Measures to make mealtimes as pleasant as possible
Offer preferred foods
Dietary supplements
Daily weight
Record dietary intake
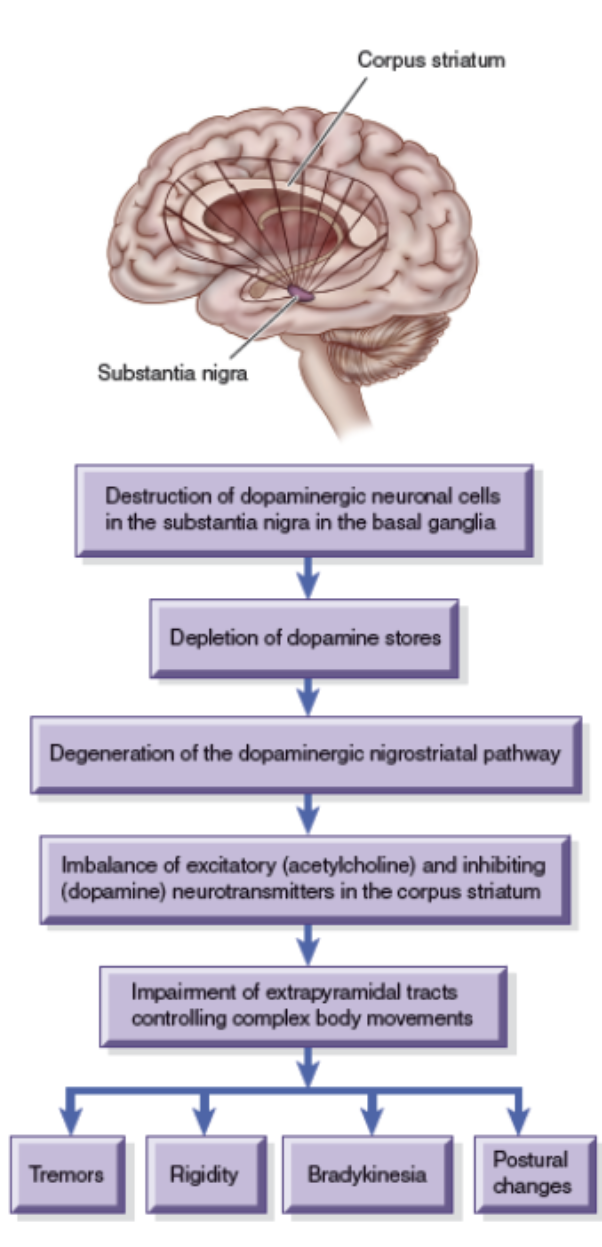
Parkinson’s Disease
Slow, progressive neurologic movement disorder associated with decreased levels of dopamine
Manifestations:
Cardinal: tremor, rigidity, bradykinesia/akinesia →pill rolling, postural instability
Autonomic: sweating, drooling, flushing, orthostatic hypotension, gastric and urinary retention
Dysphagia
Psychiatric changes: depression, anxiety, dementia, delirium, hallucinations
Assessment of the patient with Parkinson’s Disease
Focus on the degree of disability and functional changes that occur throughout the day, such as responses to medication
Almost every patient with a movement disorder has some functional alteration and may have some type of behavioral dysfunction
Quality of speech, loss of facial expression, swallowing deficits (drooling, poor head control, coughing), tremors, slowness of movement, weakness, forward posture, rigidity, evidence of mental slowness, and confusion
Fall risk assessment
Medical management of Parkinson’s Disease
Treatment directed toward controlling symptoms and maintaining functional independence
Pharmacologic treatment
Levadopa/Cardopa- Sinemet (is combination of both)
Table 65-1
Surgical procedures
Stereotactic Procedures; thalamotomy, pallidotomy
Neural transplantation
Ongoing research
Nursing interventions for Parkinson’s Disease
Improving mobility
Progressive daily program of exercise (stretching, ROM, postural)
Consultation with physical therapy
Walking techniques for safety and balance
Frequent rest periods
Proper shoes and use of assistive devices
Enhancing self-care activities
Encourage, educate, and support independence
Environmental modifications
Use of assistive and adaptive devices
Consultation with occupational therapy
Supporting coping abilities
Set achievable, realistic goals
Encourage socialization, recreation, and independence
Planned programs of activity
Support groups and referral to supportive services: counselors, social workers, home care
Huntington Disease
A chronic progressive hereditary disease that results in choreiform movement and dementia → repetitive, unstable movement
Transmitted as an autosomal dominant trait
Pathology involves premature death of cells in the striatum of the basal ganglia (control of movement) and the cortex (thinking, memory, perception, judgment)
Refer to Chart 65-4
Amyotrophic Lateral Sclerosis (ALS)
“Lou Gehrig disease”
Loss of motor neurons in the anterior horn of the spinal cord and loss of motor nuclei of the lower brainstem → Upper & lower motor neurons: all over
Manifestations
Progressive weakness and atrophy of muscle cramps, twitching, and lack of coordination
Spasticity, deep tendon reflex brisk, and overactive
Difficulty speaking, swallowing, breathing
Muscular Dystrophies
Incurable disorders characterized by progressive weakening and wasting of skeletal and voluntary muscles
Most are inherited disorders
Duchenne muscular dystrophy is the most common and inherited as a sex-linked trait
Common characteristics:
Varying degrees of muscle wasting and weakness
Abnormal elevation in serum levels of muscle enzymes
Degenerative Disc Disease
Low back pain is a significant public health disorder and has significant economic and social costs
Most back problems are related to disc disease
Degenerative changes occur with aging or are the result of previous trauma
Radiculopathy produces pain
Continued pressure may produce degenerative changes in the nerves with resultant changes in sensation and motor responses
Treatment is usually conservative: rest and medications
Surgery may be required
Post-Polio Syndrome
Occurs at least 15 years after polio exposure
Symptoms include new musculoskeletal weakness, fatigue, and musculoskeletal pain
Cause is unknown; researchers suspect that with aging or muscle overuse, the neurons not destroyed by the poliovirus continue generating axon sprouts
No specific medical or surgical treatment available
Assessment of the Patient Undergoing a Cervical Discectomy
Determining the onset, location, and radiation of pain
Assessing for paresthesia, limited movement, and diminished function of the neck, shoulders, and upper extremities
Determine whether the symptoms are bilateral
Cervical spine palpated to assess muscle tone and tenderness
Range of motion in neck and shoulders is evaluated
Health issues
Mood and stress levels
Patient education
Nursing Interventions for the Patient Undergoing a Cervical Discectomy
Relieving pain
Improving mobility
Monitoring and managing potential complications
Promoting home, community-based, and transitional care