Physiology & Pathophysiology of the Immune System (BIOMED- EXAM1 )
1/78
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
79 Terms
Describe the causative factor “intrinsic immune defects” of primary immunodeficiency ?
Inherited (congenital) genetic defects that compromise the normal development or function of the immune system. Such as:
Pattern Recognition Receptors (PRRs),
Toll-like receptor (TLR) deficiency
Nucleotide-binding oligomerization domain (NOD) deficiency
What are Pattern Recognition Receptors (PRRs)?
Congenital defects affecting immune recognition
What is Toll-like Receptor (TLR) deficiency
TLR-5 can't recognize flagella
What is Nucleotide-binding oligomerization domain (NOD) deficiency
GI mucosal defects and predisposition to Crohn's disease
Describe the causative factor “B deficiencies” of primary immunodeficiency ?
Due to low or absent antibody levels
Starts in first 6-12 months of life
Poor response to vaccination
Selective IgA deficiency (most common
X-linked hypogammaglobulinemia (Bruton’s agammaglobulinemia)
Hyper-IgM Syndrome
Common variable immunodeficiency (CVID)
Selective IgA deficiency
Recurrent lung, sinuses, GI infections, most common (B-cell deficiency)
X-linked hypogammaglobulinemia
Absence of B cells, deficiency in all immunoglobulins (B- cell deficiency)
Hyper IgM syndrome
Cannot change class of antibodies, excess of IgM but lack others. X-linked (B- cell deficency)
Common variable immunodeficiency
IgG deficiency later in life (B-cell deficiency)
Describe the causative factor “T deficiencies” of primary immunodeficiency ?
Most severe
Are central to many immune responses
Starts in first 6-12 months of life
Susceptible to a broad range of infections
Wiskott-Aldrich
Ataxia-Telangiectasia
Thymic aplasia (DiGeorge syndrome)
Chronic mucocutaneous candidiasis
Wiskott-Aldrich syndrome
X-linked mutation to WAS gene, pyogenic infections (T-cell deficiency)
Ataxia-telangiectasia
Defective ATM gene, low IgA (T-cell deficiency)
Thymic aplasia (DiGeorge)
Chromosome 22 deletion, thymus and parathyroid glands fail to develop, absence of T cells (T-cell deficiency)
Chronic mucocutaneous candidiasis
IL-17 receptor deficiency, deficient T cell response to candida (T-cell deficiency)
Severe Combined Immunodeficiency Syndrome (SCID)
X linked, lack of B and T cells, low immunoglobulin levels, bubble boy
Describe the causative factor “Leukocyte adhesion deficiencies” of primary immunodeficiency ?
Autosomal recessive inheritance
Defective adhesion protein LFA 1
Manifests as severe pyogenic infections early in life; extremely high leukocyte count
Chronic Granulomatous Disease (CGD)
Chédiak-Higashi Syndrome
Cyclic Neutropenia
Chronic Granulomatous Disease
X linked, can trap organism but cannot kill it, leads to granules
Chediak-Higashi syndrome
Autosomal recessive, LYST gene mutation, lysosomes cannot lyse stuff
Cyclic neutropenia
Autosomal dominant, ELANE gene mutation, low neutrophils every 21 days
Describe the causative factor “complement deficiencies” of primary immunodeficiency ?
A lack of specific complement proteins (such as C3), which hinders the complement cascade needed to clear infections.
C3 Deficiency
C5, 6, 7, 8, 9
C1 esterase inhibitor deficiency
Autoimmune disease
C3 Deficiency
Increased susceptibility to encapsulated organisms
C5, 6, 7, 8, 9 deficiency
No MAC, susceptible to Neisseria
C1 esterase inhibitor deficiency
Hereditary angioedema
Describe Immune tolerance
Lack of response to antigen, avoiding attacking self
What are factors that determine tolerance
Immune system maturity
Antigen structure
Cross reactivity
Inflammatory signals
Immune system maturity
Immature systems learn to tolerate better (tolerance)
Antigen structure
Simple or self-like structures can be better tolerated
Cross-reactivity
Tolerance is maintained or autoimmunity occurs
Inflammatory signals
No signals lead to more tolerance; inflammatory signals lead to less tolerance
Describe central tolerance (thymic)
Tolerance to self-antigens that is acquired within the thymus. It involves "positive selection" (keeping T cells that recognize MHC receptors) and "negative selection" (eliminating T cells that react strongly to self-antigens).
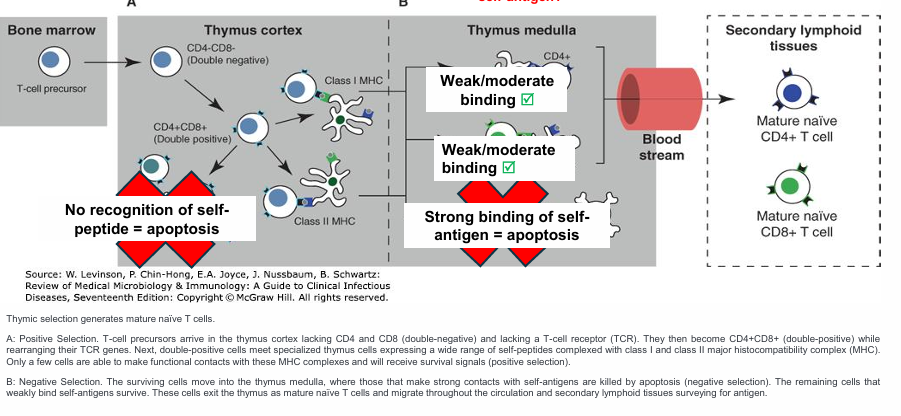
What is positive selection in reference to T cell tolerance
selects for T cells with a T cell receptor and CD4/CD8 receptor (double positive) that recognize MHC I/MHC II
“Rule of eight”
What is the Rule of eight
Class II MHC binds to CD4-positive T cells → (2 x 4 = 8)
Class I MHC binds to CD8-positive T cells → (1 x 8 = 8)
What is negative selection in reference to T cell tolerance
eliminates T cells that react strongly to self antigens encountered in the thymus
Describe Peripheral Tolerance (Post-thymic)
Tolerance acquired outside the thymus. It acts as a necessary backup mechanism to control self-reactive T cells that encounter self-antigens which were not present in the thymus.
Anergic
T regulatory (Tregs)
Define Anergic
Unresponsive (Lack of T cell co-stimulation)
Define T regulatory cell (Tregs)
suppresses T cell activation or induce apoptosis
Describe B-cell tolerance
Tolerance developed through negative selection in the bone marrow
Fails tolerance test
Antibody receptor editing
unique to B cells only
Apoptosis
Anergy
Loss of self tolerance (LoT) leads to….
autoimmune diseases
What are the types of immune response to LoT
Antibody to receptors
Antibody to cell components
T-cell mediated
Genetic predisposition (LoT)
Involves human leukocyte antigens (HLA).
HLA-DR (LoT)
Associated with diabetes
HLA-B27 (LoT)
Associated with ankylosing spondylitis
Autoimmune diseases prevalence in women (LoT)
90% occur in women, estrogen main cause
Molecular mimicry (LoT)
Infectious agent induces immune response that cross-reacts with self-proteins.
Graves disease
Involves TSH receptor, autoimmune disease
Myasthenia gravis
Involves acetylcholine receptor, autoimmune disease
Insulin dependent diabetes
Involves islet cells, autoimmune disease
Rheumatic fever
Affects heart and joint tissue, autoimmune disease
Celiac disease
Enterocytes destroyed by cytotoxic T cells, autoimmune disease
Define Antibody receptor editing
gets rid of self-reacting cells by creating a slightly different antibody with a slightly different light chain with different recognition
Unique to B cells ONLY
Define Anergy
developmental arrest/unresponsive
Define Autograft
Transfer of an individual’s own tissue to another body site
Define Isograft (syngeneic graft)
Transfer of tissue between genetically identical individuals (identical twins)
Define Allograft
graft between genetically different members of the same species
Define Xenograft
transfer of tissue between different species
Define a "Host vs. graft" response in transplantation.
The recipient's immune system identifies the transplanted tissue as foreign and attacks it.
Hyper acute rejection
Acute rejection
Chronic rejection
Graft vs Host reaction (GVH)
In allogenic stem cell transplants, donor T cells attack the recipient’s tissues a organ dysfunction
Risk factors:
HLA mismatch
Unrelated donor
Older age of donor/recipient
Symptoms: often affects skin and GI tract
Severe body rash
Oral ulcers
Nausea, vomiting, diarrhea, hepatitis
Hyper acute rejection
Occurs minutes to hours after transplant, due to ABO incompatibility
Acute rejection
T cell mediated rejection occurring 2 weeks post-transplant due to HLA mismatch
Chronic rejection
Gradual loss of function occurring months to years, persistent acute rejection
Direct pathway
HLA mismatch where host cytotoxic T cells recognize graft cells as foreign, causing acute rejection
Indirect pathway
Chronic rejection where donor proteins are presented by host APC
Major histocompatibility complex (HMC)
Set of genes that encode major antigens (human leukocyte antigens-HLA) and is important in organ transplantation. MOST crucial for matching donors and recipients for transplants, chromosome 6
Minor histocompatibility complex (MHC)
Encoded by genes at sites other than the HLA locus. Typically induces a weak immune response→ slow rejection of a transplant. Difficult to predict rejection based on minor antigens
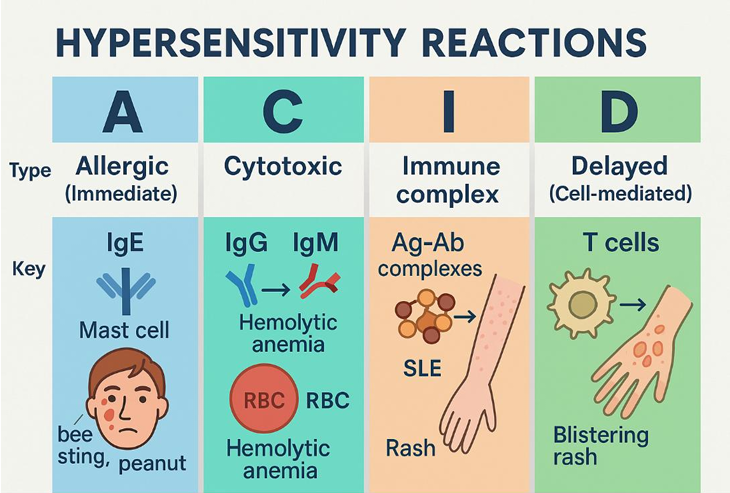
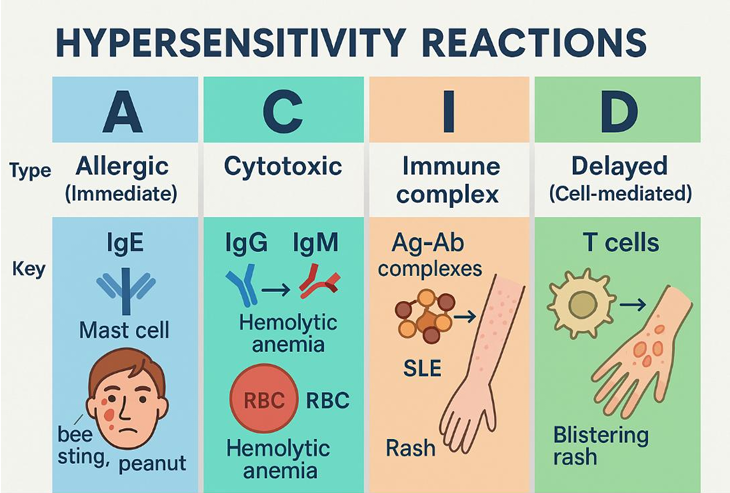
Describe Type I hypersensitivity and the clinical manifestations
immediate hypersensitivity
IgE mediated, response to allergen, mild to life threatening, mast cell degranulation.
Atopy
Atopic triad
Clinical manifestations
Systemic anaphylaxis
Rash
Urticaria (hives)
Rhinitis
Conjunctivitis
Wheezing (asthma)
Edema
Atopic Triad
Asthma, eczema, allergies
Define Atopy
genetic tendency to develop allergic diseases
Describe Type II hypersensitivity and the clinical manifestations
Cytotoxic hypersensitivity
Occurs when antibody directed at antigens of the cell membrane activates complement →cell death
IgG or IgM mediated
Antigen bound to cell membranes
Clinical manifestations:
Hemolytic anemia
ABO transfusion reactions
Rh hemolytic disease
Infections (Mycoplasma pneumoniae
Hemolytic transfusion reaction
Type 2 Hypersensitive reaction
Hemolytic disease of the newborn
Rh negative mother has Rh positive fetus, mother can become sensitized and attack second Rh positive fetus. Type II reaction
Cold agglutinin disease
IgM binds in cold, causes complement to bind. Type II reaction
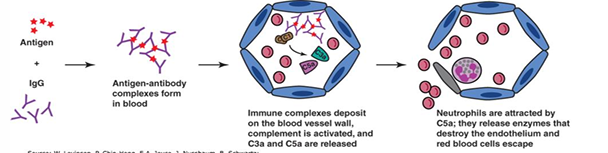
Describe Type III hypersensitivity and the clinical manifestations
Immune complex hypersensitivity
Occurs when antigen-antibody complexes induce an inflammatory response in tissues
Antigens are freely circulating
Antigens-Antibodies form large complexes
Clinical manifestations
Arthus reaction
Serum sickness
Immune complex deposition disorders (lupus
Arthus reaction
localized inflammation caused by immune complex deposition in vessel walls, alveoli. Type III hypersensitivity

serum sickness
systemic inflammatory response to the presence of immune complexes deposited in many areas of the body due to injection of foreign serum. Type III hypersensitivity
Lupus
Autoantibodies, complexes deposit everywhere. Type III hypersensitivity
Describe Type IV hypersensitivity and the clinical manifestations
Delayed hypersensitivity
Caused by T lymphocytes, not antibody
Delayed response
Occurs hours to days after contact with antigen and lasts for days
Clinical manifestations:
Poison ivy
Tuberculin skin test (PPD)
Contact hypersensitivity
Nickel, soaps, cosmetics, neomycin
Erythema multiforme
Stevens-Johnson Syndrome
Toxic Epidermal Necrolysis
contact dermatitis
T cells recognize antigen. Type IV hypersensitivity
Tuberculin skin test
Macrophages show up due to memory T cell response. Type IV hypersensitivity
Severe reactions in Type IV
Caused by cytotoxic T cells attacking skin - EM, SJS, TEN.