I - Inflammatory Skin Conditions
1/98
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
99 Terms
What is Seborrheic Dermatitis?
Subacute/Chronic inflammatory disorder
epidermal skin layer → increased proliferation
Where is seborrheic dermatitis commonly seen?
In areas of greatest sebaceous gland activity → scalp, face, chest
Presents commonly as a chronic, red, scaly, and itchy rash
What are the clinical features of infantile seborrheic dermatitis?
Occurs in first 3 months of life
Greasy scales/crust on bright red base
Common sites: scalp (cradle cap), behind ears, neck, skin folds
Self-limited → clears by 8–12 months
Rarely recurs before puberty
What are the clinical features of adult seborrheic dermatitis?
Occurs around fourth and seventh decade of life
Scalp → greasy scaling patches/plaques, thick crusting
Face → flaky/yellow scales on red, itchy skin
Ears → scaling, fissures, swelling possible
Also affects chest (V-area), back, skin folds
Seasonal pattern → better in warm weather, worse in cold
What are the treatment goals of seborrheic dermatitis?
Reduce inflammation and epidermal turnover rate of scalp/affected skin
Minimize or eliminate erythema/scaling
Minimize itch
What are the primary treatments for seborrheic dermatitis?
They work to control the disease rather than curing
Medicated shampoos
Topical corticosteroid
Examples of medicated shampoos used to treat seborrheic dermatitis?
Pyrithione zinc → OTC
Selenium sulfide → OTC
rinse thoroughly → prevents hair discoloration (esp. light/blonde hair)
Ketoconazole → Rx
How can OTC Pyrithione zinc and Selenium sulfide be used for seborrheic dermatitis?
Work shampoo into the scalp, leave lather on the hair and affected areas for 3-5mins
Daily for 1-2 weeks → then 2-3 times a week for 4 weeks → OTC products
Once controlled, apply weekly to prevent relapse
Can follow up with cosmetic shampoo/conditioner to control odor
How can Rx Ketoconazole be used for seborrheic dermatitis?
Work shampoo into the scalp, leave lather on the hair and affected areas for 3-5mins
2 times a week for 4 weeks
Once controlled, apply weekly to prevent relapse
Can follow up with cosmetic shampoo/conditioner to control odor
How can topical corticosteroids be used to treat seborrheic dermatitis?
Used for increased inflammation
Hydrocortisone ointment can be used 2x daily
Limit use up to 7 days, then consult PCP
What are salicylic acid and sulfur used for in seborrheic dermatitis?
Keratolytic agents → help loosen and remove keratin scales
Slow onset of action → weeks to months
Limited effectiveness compared to first-line treatments
Help reduce scaling by decreasing skin pH
How is cradle cap/seborrheic dermatitis managed?
Self-limiting condition
First-line → massage scalp with baby oil to loosen scales
Use non-medicated shampoo to remove flakes → gentle baby shampoo
If no improvement → refer to pediatrician
What is Diaper Dermatitis?
Diaper Rash
A skin rash that occurs in the diaper area
Causes → occlusion, moisture, contact with urine/feces, shift in skin pH friction
Appears as bright red shiny, wet looking patches/lesions on skin
Onset is very fast, but healing is slow
What can influence diaper rash?
Infants urinate up to ~20x/day → then decreases to ~8×/day by 8 months
Breast-fed infants have lower risk
Breast-fed stool = less alkaline, less irritating
Transition to solid foods can trigger diaper rash
What possible complications can result from diaper dermatitis?
Secondary infections → bacterial or fungal
Genital damage
Skin ulceration
What causes fungal diaper dermatitis and what does it look like?
Usually Candida albicans
Yeast infection often shows satellite lesions → clusters
Papules/pustules at margins of diaper dermatitis or in the skin folds
Non-pharmacologic counseling diaper rash?
Keep the patient dry
Change diaper at least 6x a day
Clean area with plain water / bland soft cloth or wipe
Make sure skin is dry before re-diapering → air dry
Disposable diaper decrease rates of severe diaper dermatitis
What are protectants used for in diaper rash treatment?
Non-prescription options (FDA-approved ingredients)
Act as a physical barrier → block irritants, reduce/absorb moisture
Most commonly used → zinc oxide

What are the top pharmacist recommended products for diaper rash?
Desitin Diaper Rash Cream → zinc oxide 40%, cod liver oil, white petrolatum, lanolin, talc
A+D Original Ointment → white petrolatum, lanolin
Boudreaux’s Butt Paste → zinc oxide 16%, mineral oil, white petrolatum
What are the key components of a triple butt paste for diaper rash?
Main component → Protectants/Emollients → A+D, white petrolatum (Vaseline), zinc oxide (Desitin®)
Antifungals → clotrimazole (OTC), nystatin (Rx)
Antacid → Maalox liquid, loose stools → decreases pH
Antibacterial → bacitracin ointment, questionable efficacy
Anti-inflammatory → hydrocortisone, short term use
How do you treat a candida/fungal diaper rash?
Treated with barrier creams + antifungal
Antifungals → clotrimazole (OTC), nystatin (Rx)
What are bacterial causes of diaper rash and how are they treated?
Perianal streptococcus → bright red rash around anus → requires oral antibiotics
Staph infection → crusted or oozing lesions → bacitracin or mupirocin (Rx), often still needs oral antibiotics
If unclear or not improving → refer to pediatrician
What are the key take-home points for managing diaper dermatitis?
Keep area clean and dry
Re-apply topical treatment after every diaper change
Combination “mixes” may include multiple barrier creams (protectants/emollients)
Know what’s in the mix →Antifungal, Topical corticosteroid, Antacid liquid
What is the typical treatment duration and follow-up plan for diaper rash?
Usually treated short-term (a few days) with OTC products
If no improvement after 7 days → refer to medical provider
If improving by 7 days → continue treatment for ~3 more days
What are the contraindications for self treatment of diaper rash?
Pesions present for > 7 days
Secondary infections → bacterial, fungal, viral
Presence of rash outside diaper region
Presence of broken skin → ulcers, blisters, peeling skin
Oozing, blood, vesicles, or pus at lesion sites
What prevents diaper rash?
Frequent diaper changes
Keeping area dry
Using protectants regularly → especially after bowel movement to prevent rash
What are the two types of contact dermatits?
Irritant contact dermatitis → 80-90% of all cases
Allergic contact dermatitis → 10-20% of all cases
Overall, contact dermatitis occurs in 1-10% of the population
Irritant contact dermatitis?
Caused by exposure to strong irritants → occupational acids, alkalis, fluorides
Primary irritants → cause direct skin damage
Presents with immediate severe irritation and blistering after exposure
Allergic contact dermatitis?
Caused by allergens
Ex; Plants: Toxicodendron, Metals: nickel, cobalt, chromium, Rubber and adhesives, Cosmetics, Topical anesthetics, Topical antibiotics, Topical diphenhydramine
Irritant vs Allergic contact dermatitis delay to reaction?
Irritant → minutes to hours
Allergen → days, much slower
Irritant vs Allergic contact dermatitis causative substances?
Irritant → H2O, urine, flour, detergents, hand sanitizers, soap, alkalis, acids, solvents, salts, surfactants, oxidizers
Allergen → Low molecular weight & lipid-soluble substances, fragrances, nickel, latex, benzocaine, neomycin, leather
What is the first and second line treatments in contact dermatitis?
1st → Corticosteroids
2nd → Fragrances free moistures / emollients
What are the possible mechanisms involved in the treatment of contact dermatitis?
Anti-inflammatory effects
Immunosuppressive effects
Antiproliferative effects
Vasoconstrictive effects
How corticosteroids ranked in potency?
From class 1 to class 7
Class 1 → most potent
Class 7 → least potent
Low potency corticosteroids?
Class 6/7
Safe for infants, children, longer duration, or intertriginous areas
Medium potency corticosteroids?
Class 4/5
Safe for short durations in infants and children → face, axillae, genitals ok in adults
High potency corticosteroids?
Class 2/3
May be used with close supervision in children for short (<2 weeks) duration
Ultra high potency corticosteroids?
Class 1
No occlusion, maximum duration 2-4 weeks
Do not use in infants, children, on face, axillae, or groin
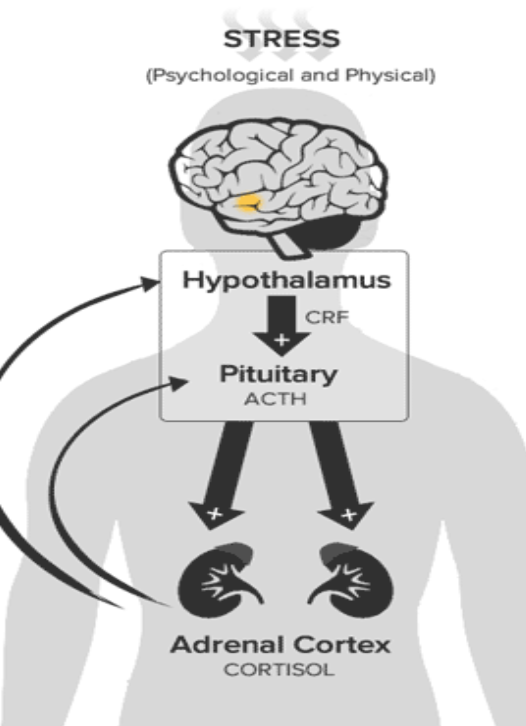
How do corticosteroids effect the HPA axis?
Exogenous steroids cause negative feedback on the HPA axis
Leads to decreased endogenous cortisol production over time
Typically seen with high/ultra-high potency topical steroids
Risk increases with use on >20% body surface area for >4 weeks
What factors should be considered when selecting a topical corticosteroid?
Potency
Vehicle type → ointment > gel > cream > lotion
Frequency of application
Area being treated (size and location)
How does the treatment area affect the choice of corticosteroid formulation?
Large areas → ointments may be impractical (too greasy/viscous)
Hairy/scalp areas → prefer foam, shampoo, or aerosol
Less suitable → ointments or creams for scalp/hair-bearing skin
How is topical corticosteroid potency chosen when treating dermatitis?
For dermatitis, potency depends on skin thickness and location
Thick skin (palms, soles, scalp) → high potency steroids
Moderate skin (arms, legs, abdomen) → medium potency steroids
Thin/sensitive skin (face, eyelids, anogenital area) → low potency steroids
What counseling points are important for topical corticosteroid use in dermatitis?
Use a small amount → a little goes a long way
Apply only to affected dermatitis areas
Wash hands before and after application
What are the side effects of topical corticosteroids?
Acneiform lesions
Striae → thinning of skin
Pigmentation changes
Folliculitis
Fungal infections, delayed wound healing
Possible perioral dermatitis if applied close to the mouth
The most potent the more quickly these symptoms can present !!!!
OTC Hydrocortisone?
Is the only OTC topical corticosteroid available
Available as → Hydrocortisone 0.5–1%
Can be effective for small-area contact dermatitis (may need stronger Rx steroid for larger areas)
Apply to affected area 3–4 times daily
When are systemic corticosteroids used in contact dermatitis?
Used when ≥20% body surface area is affected
Indicates more severe/widespread contact dermatitis
What systemic corticosteroid is used for contact dermatitis?
Prednisone → 0.5–1 mg/kg daily for ~10 days
Less 2–3 week courses usually do not require tapering
Dermatology often still uses tapers to reduce flares
What is poison ivy?
A type of allergic contact dermatitis
How do you treat poison ivy?
Topical hydrocortisone → 3-4x daily
Oral hydrocortisone → prednisone can be used as well
Oozing → astringents → domeboro, witch hazel, or calamine
Topical diphenhydramine?
NEVER THE ANSWER !!!!!
Non-pharmacologic options for allergen contact dermatitis?
Know the allergen and avoid it
Wear protective clothing when potentially being exposed to allergen
Non-pharm options urushiol oil specific?
Do not burn the plants → increases exposure
Immediately after exposure → remove clothes and wash separately with laundry detergent
Wash things that may have had oil transfer to them
Clip/trim nails to avoid transfer of urushiol
Wear gloves when washing contaminated objects
Barrier products for poison ivy?
Zanfel
Tecnu
Tecnu extreme
Exclusions for self treatment for allergen/irritant dermatitis?
Involvement of >20% BSA
Swelling of the body/extremities
Swollen eyes/eyelids shut
Discomfort in genitalia from itching, redness, swelling, or irritation
Involvement and/or itching or mucous membrane of mouth, eyes, nose, or anus
Signs of infection
What is the treatment for a contact dermatitis flare?
inflammation/pruritus → Corticosteroids
Oozing →Aluminum acetate, witch hazel, calamine, dressings
Itch relief/sleep→ 1st gen antihistamines
Atopic Dermatitis?
Eczema
Chronic inflammatory pruritic skin disease
Caused by → genetics, environment, skin barrier defects, immune system
What are the pattern and characteristics of atopic dermatitis?
Chronic, relapsing course
Often improves in childhood by puberty
Some develop atopic triad → asthma, allergic rhinitis, eczema
associated with increase IgE and other atopic conditions
How does immune dysfunction contribute to atopic dermatitis?
Imbalance of TH1 and TH2
TH2 overactivity → increase IL-5, IL-13 → more inflammation and IgE
TH1 normally helps → decrease IgE and inflammation
Why is keeping the skin barrier intact important in atopic dermatitis?
It helps to limit the access of infection, dust, allergens, etc.. that can trigger inflammation
What are the main goals of nonpharmacologic treatment for atopic dermatitis?
Avoid triggers
Reduce itching and scratching
Maintain skin hydration
Prevent infection
Restore skin barrier function
What are recommended nonpharmacologic treatments for atopic dermatitis?
Fragrance-free moisturizers / emollients used regularly
Mild cleansers
Ex; ceramides (CeraVe), white petrolatum, Eucerin, Vanicream, Cetaphil
Non-pharmacologic suggestions for atopic dermatitis?
Avoid excessive bathing
Apply moisturizers immediately after bathing
Use humidifier in dry seasons/low humidity environments
Avoid known irritants
Minimize scratching
Wet wraps
Bleach baths
What is the treatment for a atopic dermatitis flare?
Inflammation → Emollients then topical corticosteroids, → Eucrisa → topical calcineurin inhibitors
Pruritis/Controlling allergies → 1st or 2nd generation oral antihistamines
Eucrisa / Crisaborole ?
Used for atopic dermatitis
MOA → PDE-4 inhibitor → prevents cAMP breakdown → decreases pro-inflammatory cytokines and increases anti-inflammatory mediators
Dosing → topical used 2x daily
2% ointment
Side effects → itching, hypersensitivity reactions
Pimecrolimus/Elidel and Tacrolimus/Protopic?
Used for atopic dermatitis
Calcineurin inhibitors
MOA → inhibits calcineurin from initiating T cell activation → decreases itching/inflammation
What Pimecrolimus/Elidel and Tacrolimus/Protopic used as?
An alterative option to long-term use of corticosteroids → but much more $$$
No skin atrophy/striae and can be applied to face and children
What are the side effects/black box warning of calcineurin inhibitors?
Pimecrolimus/Elidel and Tacrolimus/Protopic can cause → burning, stinging, and immunosuppression
Long term use has been linked to basal cell and squamous cell carcinomas as well as lymphomas
What are alternative treatments for moderate–severe atopic dermatitis?
JAK inhibitors (oral/topical):
Cibinqo (abrocitinib) – oral
Rinvoq (upadacitinib) – oral
Opzelura (ruxolitinib) – topical
Interleukin antagonists (injectables):
Dupixent (dupilumab) – blocks IL-4 & IL-13
Adbry (tralokinumab) – blocks IL-13
Atopic vs Contact Dermatiitis?
Contact → Topical or oral corticosteroids, avoid allergen
Atopic → Maintain skin barrier, can progress to topical steroids, calcineurin inhibitors, eucrisa, complex immunologic agents
Psoriasis?
Increased proliferation of epidermis due to inappropriate migration of T cells/cytokines leading to plaque formation
Chronic inflammatory multi-system disease that waxes/wanes over time
Can be associated with other disease → Chron’s, Ulcerative colitis, MS, obesity, lymphoma
What are the characteristic lesions of plaque psoriasis?
Thick raised plaques (most common form, ~80–90% of cases)
Silvery-white scales
Well-demarcated deep red (erythematous) lesions
What are the therapeutic goals of psoriasis?
Chronic disease → control symptoms
Maximize adherence to therapies
Minimize drug toxicity
Improve cosmetic appearance of the skin
Preserve quality of life
Minimize joint symptoms when present
How is psoriasis classified by severity?
Based on quality of life scores and psoriasis area severity indices
PASI improvement of 75% → treatment is considered effective
Mild → <3% BSA
Moderate → 3–10% BSA
Severe → >10% BSA
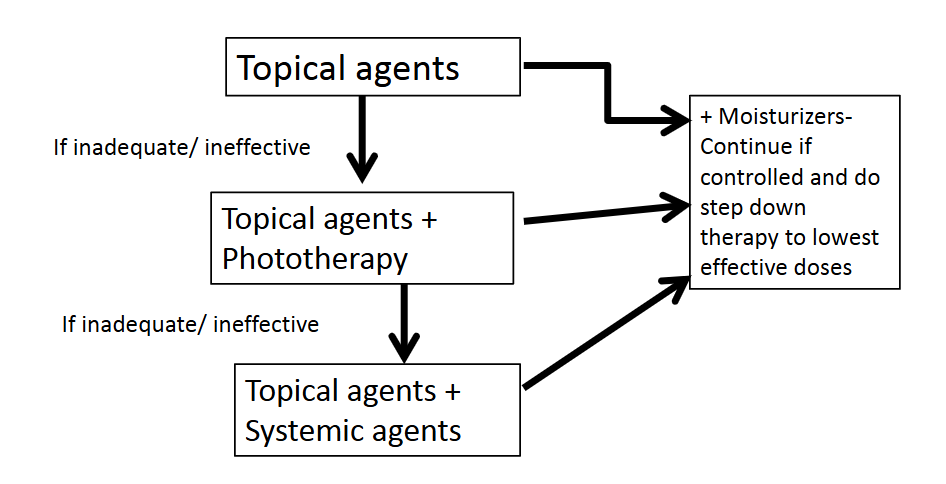
What is the treatment algorithm for mild to moderate psoriasis?
Start with topical agents and moisturizers
If inadequate → add phototherapy
If still inadequate → add systemic agents
If controlled → step down to lowest effective doses and continue maintenance
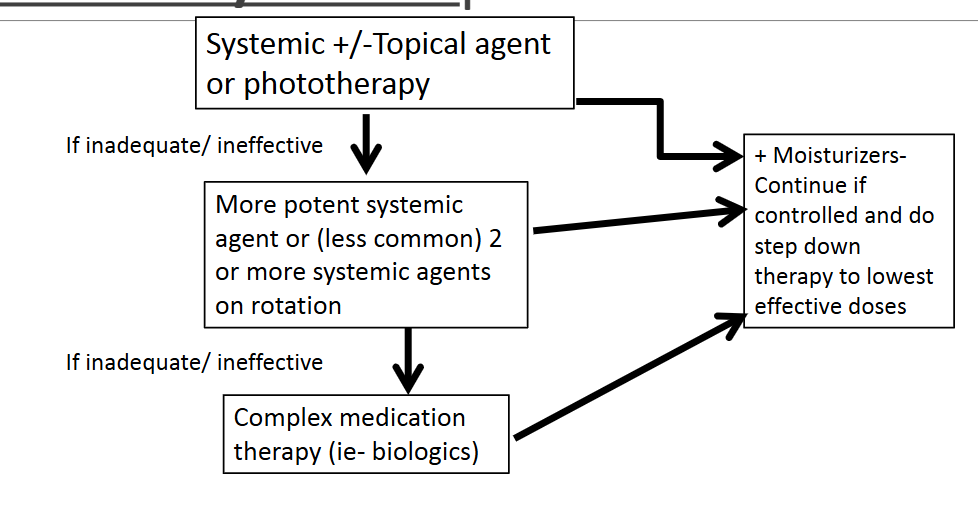
What is the treatment algorithm for moderate to severe psoriasis?
Start → systemic therapy and topical agents or phototherapy
If inadequate → switch to more potent systemic therapy or rotate ≥2 systemic agents
If still inadequate → biologic (complex therapy)
If controlled → step down to lowest effective dose + continue moisturizers
What are the general principles of topical therapy in psoriasis?
Vehicle matters (cream, ointment, etc.)
Can be used short-term or long-term
Can be combined with phototherapy or systemic therapy
Choose regimen based on patient adherence and ease of use
What are the goals and key points of topical corticosteroids in psoriasis treatment?
Goals → decrease erythema, scaling, and pruritus
Often use higher potency earlier than in other skin conditions
Guidelines recommend starting with potency level 2–5
Main role → reduce inflammation and plaque symptoms
What are key dosing considerations for topical corticosteroids in psoriasis?
Occlusion (plastic wrap / wet wraps) increases potency
Apply BID to TID
Ointments are more potent than creams
Vehicle choice depends on plaque location and skin area
Type of hydrocortisone cream for lesions on hands/feet?
High potency
Vehicle → Ointments, emollients, gels
Ex; Betamethasone, clobetasol, triamcinolone
Type of hydrocortisone cream for lesions on trunks/extremities?
Potency → Med-High
Vehicle → Ointments, creams, emollients
Ex; Fluocinonide cream, triamcinolone
Type of hydrocortisone cream for lesions on scalp?
Potency → Med-High
Vehicle → Solutions, oil, sprays, foams
Ex; Clobetasol solution/foam, Derma Smoothe-FS
Type of hydrocortisone cream for lesions on Face or Axillae?
Potency → Low-Med
Vehicle → Creams, lotions
Ex; Desonide, Hydrocortisone
Type of hydrocortisone cream for lesions on ear canals?
Potency → Low
Vehicle → Lotions, creams, solution, oils
Ex; Desonide lotion, fluocinolone oil
Counseling for topical steroids?
A lil bit goes a long way
Only apply to affected area
Wash hands before/after use
Use higher potency steroids no longer than 2-3 weeks for flares unless under supervision of provider
Higher potency → side effects can pop up earlier
What are vitamin D analogs and how are they used in psoriasis treatment?
First-line topical therapy → often combined with topical corticosteroids or used to provide steroid-sparing effect
Ex; Calcipotriene
MOA: regulates skin cell growth and differentiation
Dosing: thin layer applied BID
Possible adverse effects of Vitamin D analogs?
Burning, itching, skin irritation
Erythema, dry skin
Exacerbation of psoriasis
Hypercalcemia → rare
Other steroid sparing topical therapies for psoriasis?
Tazarotene (Tazorac): topical retinoid → increases cell turnover → used common in acne
Calcineurin inhibitors → used for maintenance after 2–4 weeks of steroids or in sensitive areas (face, groin, armpits, nails)
Typically limited use: ~8–12 weeks for calcineurin inhibitors

Phototherapy in psoriasis ?
UVA radiation
Causes DNA damage → decreases skin cell proliferation
Can be delivered via light boxes or controlled sun exposure
Typical regimen: ~15 minutes, no sunscreen, ~3 times per week (summer)
Possible adverse effects of phototherapy?
Increased risk of skin cancer
Cataracts
Nausea
Skin burning

What is coal tar and how is it used in psoriasis treatment?
3rd/4th line therapy
MOA → inhibits skin cell reproduction
Forms → shampoos, bath preparations
Often used with phototherapy
Adverse effects → unpleasant odor, staining, messy to use
When is systemic therapy first-line in psoriasis?
When psoriatic arthritis → joint involvement is present
Widespread skin involvement/lesions
Moderate to severe disease (>3% BSA)
Examples of systemic therapies for psoriasis?
Methotrexate
Cyclosporine
Acitretin
Methotrexate?
MOA → Folate antagonist leading to decreased cell replication
Dosing → 10-25mg once weekly
Titrate upwards based on response by 2.5mg/week
Max dose → 30mg/week
Methotrexate adverse effects?
GI toxicity → anorexia, nausea
Liver toxicity → fibrosis/cirrhosis
Neutropenia, thrombocytopenia, anemia
MANY DDIs
Cyclosporine?
MOA → Immunosuppressant via reversible inhibition of lymphocytes
Works very fast
Cyclosporine dosing?
PEDs → 3-5mg/kg daily
Adults → 150mg-300mg BID
Cyclosporine requirements?
Bloodwork and monitoring requirements → CBC, BMP, Trigs, Uric acid, BP
MANY DDIs
Acitretin?
Aka Soriatane
MOA → unknown, thought to decrease cell life proliferation/differentiation
Avoid alcohol
Known teratogen → pregnancy may be considered 3 years after last does
Acitretin adverse effects?
Hyperlipidemia
Liver toxicity
Bone/muscle pain
Pseudotumor cerebri → increase in intracranial pressure without tumor → headache, vision changes, papilledema
Eye irritation
Contraindicated in pregnancy (teratogenic)