Perioperative Crystalloid and Colloid Therapy
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
T/F: Crystalloid and Colloid fluids are drugs
True
T.B.W = __% of body weight
60%
Which has more T.B.W neonates or older patients?
Neonates
T.B.W needs to established based off of ___ weight, why is this important?
Lean
Fat can disrupt this calculation, making the T.B.W seem higher than it is
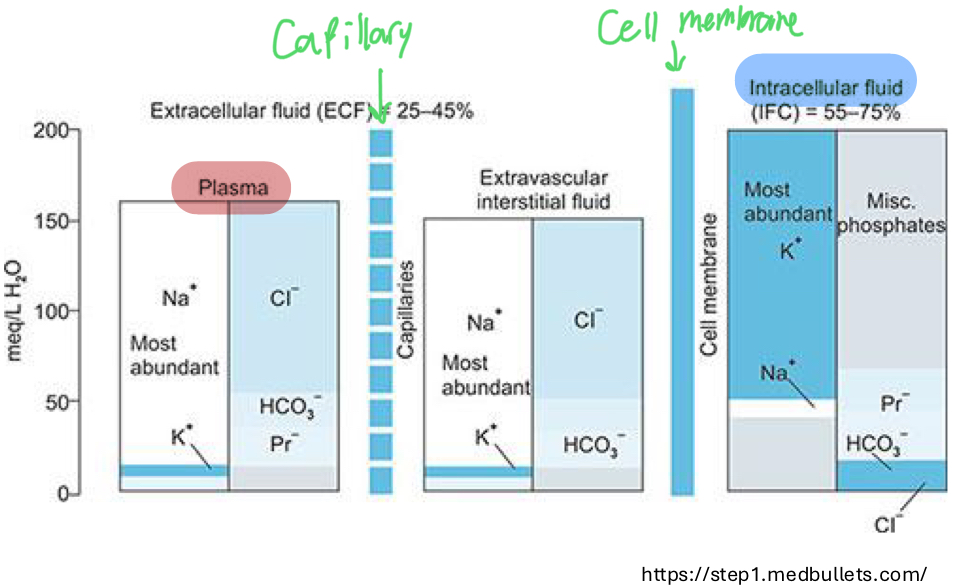
What % of TBW is plasma?
5%
What makes up the majority of TBW?
ICF (40% of BW)
ECF (20%)
Interstitial Fluid (15%)
Plasma (5%)
A key principle of body fluids is permeability, what is the difference between the permeability of the capillary endothelium and the cell membrane?
Cell Membrane
Freely permeable → H20
Capillary endothelium (more “controlling“)
Freely permeable → H2O and various ionic solute
Limits proteins, large MW, and negatively charged molecules
The movement of H2O between ICF and ECF is governed by the ______ gradient, what is this gradient?
Osmotic gradient
The difference in solute concentrations across membranes (hypertonic/hypotonic)
What is the difference between an effective osmole and an ineffective osmole?
Effective
Contributes to osmolarity/fluid shifts, cannot cross cell membrane
Ineffective
Can cross cell membrane (ex Urea)
What is Starlings Principle?
It describes the movement of fluid across capillary walls as a function of
Hydrostatic pressure and Osmotic pressure
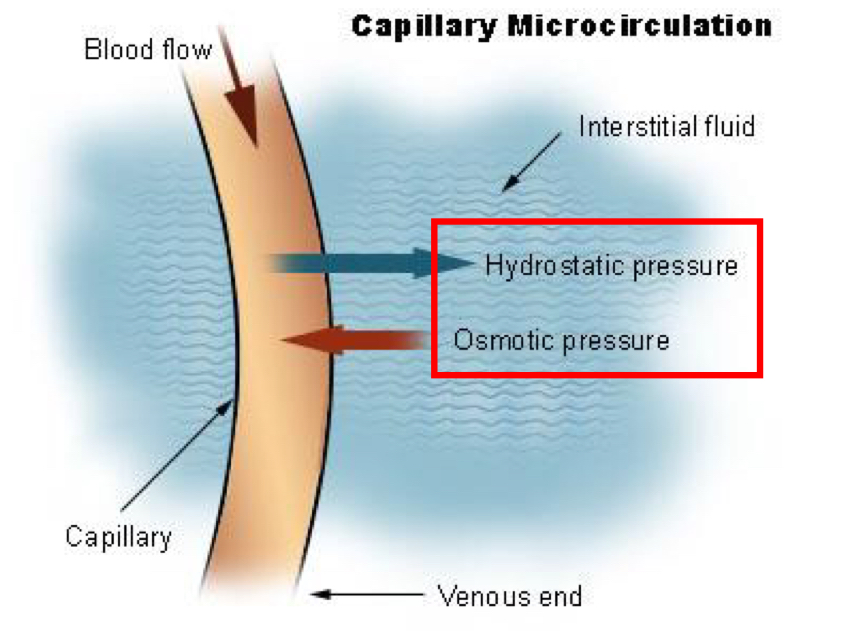
In the vasculature, osmotic pressure is largely drive/controlled by what protein?
ALBUMIN
What is the goal of fluid therapy?
Preserve tissue perfusion by maintaining or restoring effective circulating intravascular volume (maintaining O2 deliver to tissues)
T/F: IV fluids can only serve to benefit the patients
False, its a Drug, it can benefit or harm depending on dose, administration and correct/appropriate usage
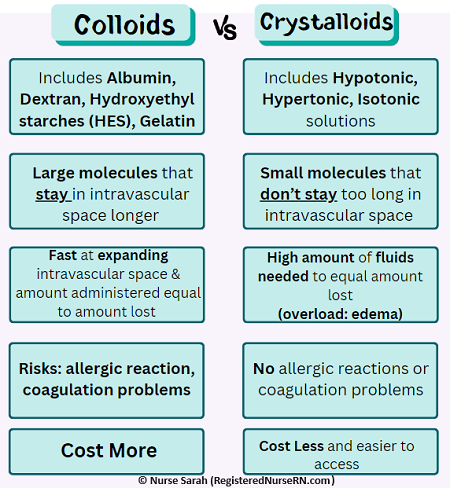
The 2 general categories of perioperative fluids are? What’s the difference between the two?
Crystalloid
Crystalloids (e.g., Normal Saline, Lactated Ringer's) are small-molecule solutions used for initial resuscitation, dehydration, and maintenance fluids
Distributing widely in the body but requiring 3:1 (volume:loss) replacement.
Colloids
Colloids (e.g., Albumin, FFP) contain large molecules that stay in the intravascular space
Offering faster, 1:1 volume expansion but carrying higher risks of allergic reactions, renal damage, and costs
What are the 2 types of Crystalloids? Describe each, which is the fluid of choice for anesthesia?
Isotonic
Osmolality = Plasma
No change to the solute of plasma
Redistributes to ECF after 30-60 minutes → Expands the ECF
Hypertonic
Osmolality > Plasma
Increases solute of plasma, pulls water from the ICF (Intra-cellular) and ISF (interstitial)
Expands plasma volume
What are the indications for the use of Isotonic and Hypertonic Crystalloids?
Isotonic
Anesthesia
Hypertonic
Rapid resucitation of hypovolemia
Cerebral edema/increased intracranial pressure
Bc it will pull the fluid out of ICF/ISF and into the vasculature
Hypertonic crystalloids should always be followed with isotonic fluids, why?
Bc hypertonic crystalloids can cause cellular dehydration the isotonic fluids can mitigate this
How do colloids work?
Colloids contain large molecules that have very limited movement across the capilalry endothelium
They pull water from the ISF → IVF (vasculature) based off of oncotic pressure (protein based)
What are the indications of Colloid fluid therapy?
Hypoproteinemia (hypoalbuminemia)
Hypovolemia
Remember that colloid therapy add a bunch of large molecules to increase the oncotic proterites of the IVF
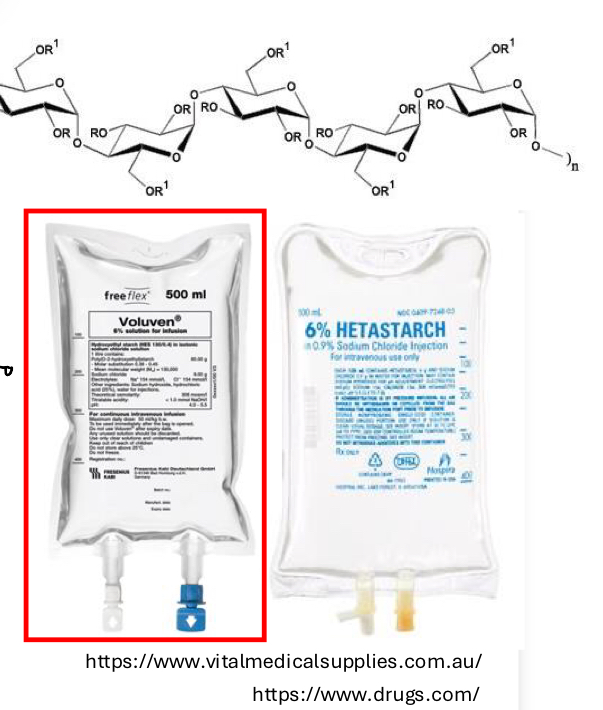
What is the main example of synthetic colloids? What is its advantages/disadvantages
HES (Hydroxyethyl starch)
Advantages
Sustained expansion of vascular compartment compared to isotonic crystalloids (longer effect)
Small volume required to achieve desired effect (Potent)
Disadvantages
Serious adverse effects, weigh your options before using
You should never exceed more than __ mL/kg/day of HES
20
When calculating how to use HES in your patient, you should opt for the ______ dose over the _______ time
Smallest dose over the shortest time
What are the 3 types of Natural colloids?
They are all blood components
RBC products
Plasma Products
Albumin Products
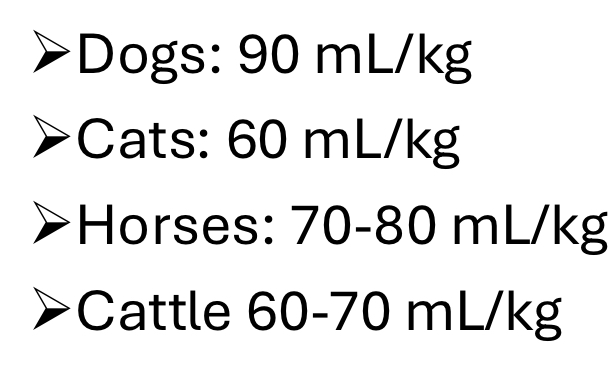
A 25kg dog underwent an OHE, during the procedure they accidentally dropped a pdicle and estimated that blood loss was 250 mLs, what % blood volume was lost?
B.V = 90 mL/kg (for dogs) * 25 kg = 22550 mL
% blood volume lost = (250/2250)*100 = 11%
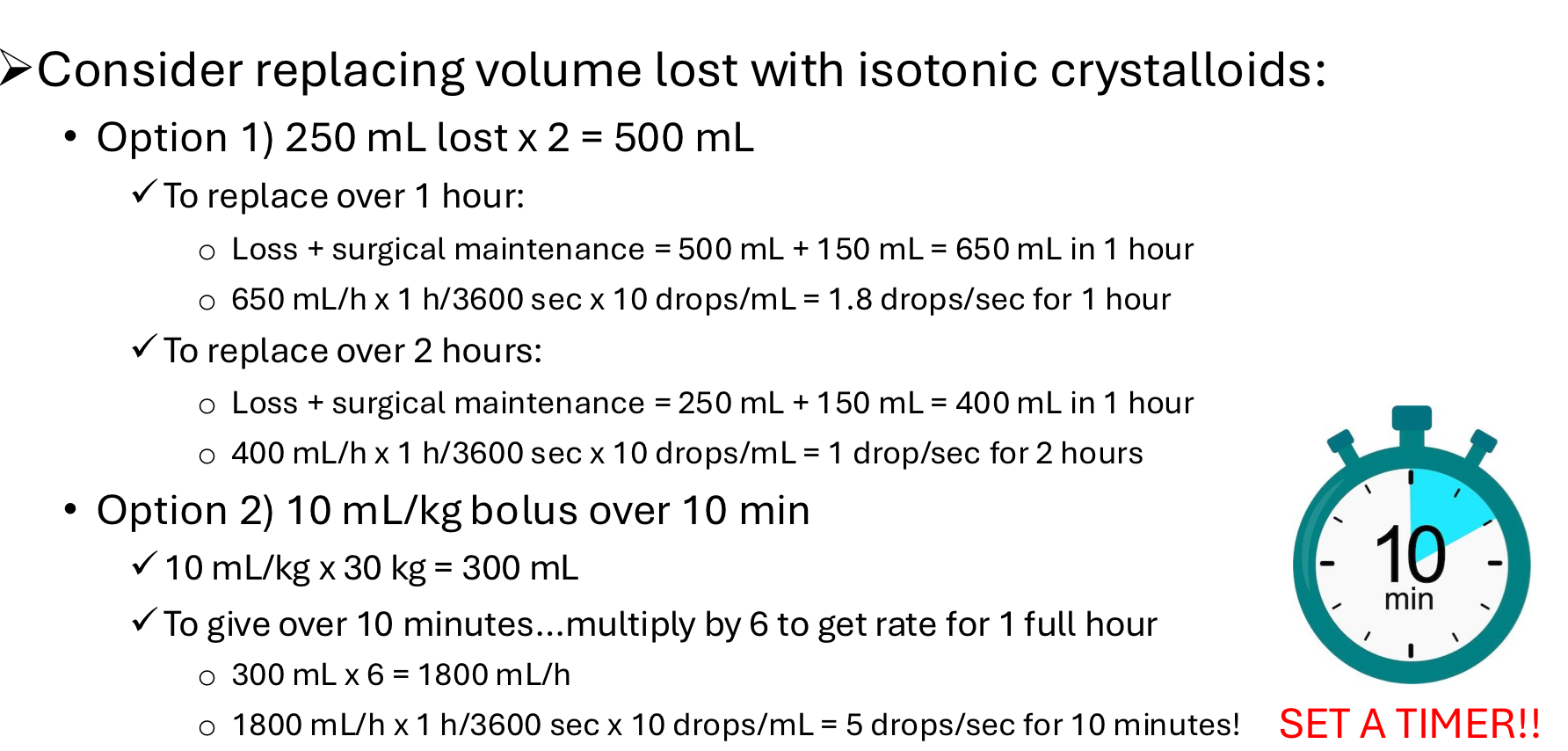
Given the following question, should you administer fluids to the patient? If yes what kind?
If <10% of blood volume is lost then you can use isotonic crystalloids for replacement
T/F: During fluid therapy once you calculated the dose the patient needs you will not need to adjust that dose during or after procedures
False, always assess and reassess your patient, you may need to adjust your dosages