BV lab material exam 1
1/99
Earn XP
Description and Tags
labs 1-3
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
100 Terms
What is the primary action of the Lateral Rectus?
Abduction
What is the primary action of the Medial Rectus?
Adduction
What are the primary, secondary, and tertiary actions of the Superior Rectus?
Primary: Elevation | Secondary: Intorsion | Tertiary: Adduction
What are the primary, secondary, and tertiary actions of the Inferior Rectus?
Primary: Depression | Secondary: Extorsion | Tertiary: Adduction
What are the primary, secondary, and tertiary actions of the Inferior Oblique?
Primary: Extorsion | Secondary: Elevation | Tertiary: Abduction
What are the primary, secondary, and tertiary actions of the Superior Oblique?
Primary: Intorsion | Secondary: Depression | Tertiary: Abduction
What does the mnemonic INXS stand for?
INferiors eXtort; Superiors intort (and OBliques ABduct, Recti adduct)
Which muscles extort the eye?
The inferior muscles (Inferior Rectus and Inferior Oblique)
Which muscles intort the eye?
The superior muscles (Superior Rectus and Superior Oblique)
Which muscles abduct the eye (not including LR)
The obliques (Superior Oblique and Inferior Oblique)
Which muscles adduct the eye (besides MR/LR)?
The recti with vertical actions: SR and IR adduct
What cranial nerve innervates the Superior Rectus, Inferior Rectus, Medial Rectus, Inferior Oblique, and LPS?
CN III (Oculomotor nerve)
Where is the CN III nucleus located?
Mesencephalon at the level of the superior colliculus
What does the inferior division of CN III innervate?
IR, IO, MR, and parasympathetic fibers
What does the superior division of CN III innervate?
SR and LPS (levator palpebrae superioris)
What cranial nerve innervates the Superior Oblique?
CN IV (Trochlear nerve)
Where is the CN IV nucleus located?
Lower mesencephalon at the level of the inferior colliculus
How do CN IV fibers exit the brainstem?
Dorsally
Which eye does CN IV serve?
The contralateral SO (crosses over)
What cranial nerve innervates the Lateral Rectus?
CN VI (Abducens nerve)
Where is the CN VI nucleus located?
Beneath the floor of the fourth ventricle at the junction of the pons and medulla
Which eye does CN VI serve?
The ipsilateral LR
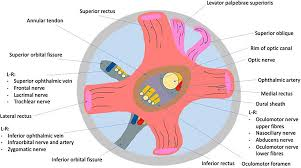
What is the origin of the four recti muscles?
Annulus of Zinn
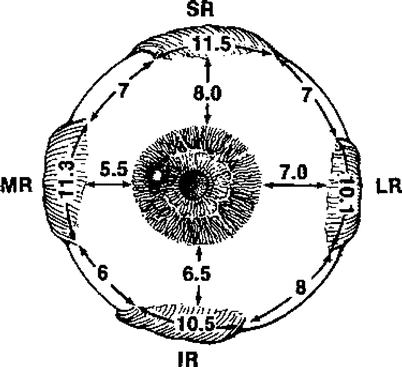
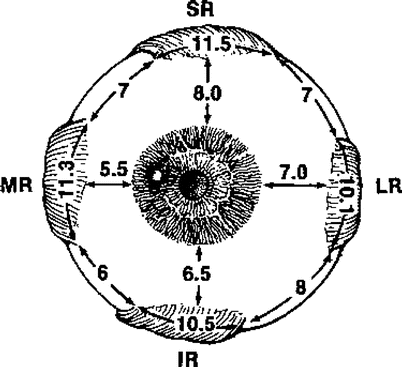
What is the insertion of the Superior Rectus?
~8mm behind the cornea
What is the insertion of the Inferior Rectus?
~6-7mm behind the cornea
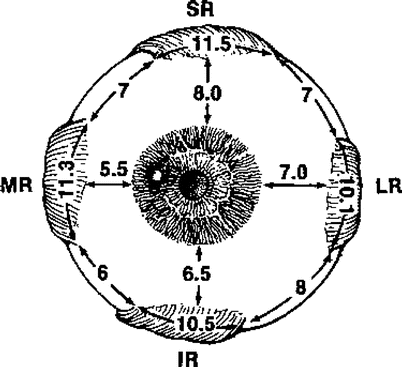
What is the insertion of the Medial Rectus?
~5-6mm behind the cornea
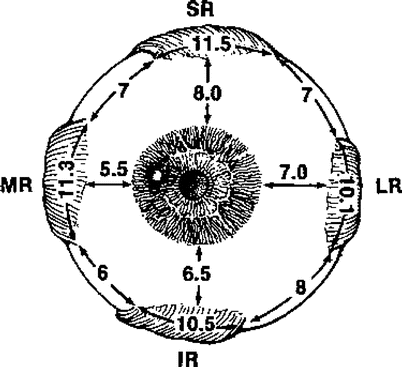
What is the insertion of the Lateral Rectus?
~7mm behind the cornea
What is the origin of the Superior Oblique?
Body of the sphenoid (trochlea)
What is the insertion of the Superior Oblique?
Posterior globe
What is the origin of the Inferior Oblique?
Anterior floor of the orbit (near lacrimal fossa)
What is the insertion of the Inferior Oblique?
Posterior globe
How do you isolate the vertical action of the Superior Rectus and Inferior Rectus clinically?
Abduct the eye (toward the ear), then have patient look up (SR) or down (IR)
How do you isolate the vertical action of the Superior Oblique and Inferior Oblique clinically?
Adduct the eye (toward the nose), then have patient look down (SO) or up (IO)
Why must the SO be adducted 54° to isolate its vertical action?
Because of the angle between the muscle plane and the optical axis; adducting aligns the SO so that its action becomes purely vertical (depression)
What is Sherrington's Law of Reciprocal Innervation?
Contraction of an agonist muscle occurs concurrently with relaxation of the antagonist muscle in the same eye (e.g., LLR and LMR)
What is Hering's Law of Equal Innervation?
During any eye movement, the magnitude of rotation of the two eyes is equal; yoke muscles receive equal innervation
Does Hering's Law apply to conjugate and disjunctive movements?
Yes, both conjugate (same direction) and disjunctive (opposite directions, like convergence)
What are yoke muscles?
Pairs of muscles in each eye that receive equal innervation to produce conjugate gaze: OD MR / OS LR, OD LR / OS MR, OD SR / OS IO, OD IO / OS SR, OD SO / OS IR, OD IR / OS SO
Define Paralysis
Total loss of innervation or muscle function
Define Paresis
Partial paralysis
Define Palsy
Could mean either paralysis or paresis
When the fixating eye is paretic, what happens to the covered (normal) eye?
The normal eye's yoke muscle overshoots (overshoot = normal eye covered)
When the fixating eye is normal, what happens to the covered (paretic) eye?
The paretic eye's yoke muscle undershoots (undershoot = paretic eye covered)
Why does the yoke muscle overshoot when the paretic eye is fixating?
Extra innervation is sent to the paretic eye to fixate, and by Hering's Law that same excess innervation goes to the yoke muscle, causing it to overshoot
What are the 4 elements of a tropia?
Laterality (which eye), frequency (constant or intermittent), direction (which EOM), magnitude (measured with prism)
What is 3rd CN palsy presentation?
Eye is down and out (SO and LR are unopposed) + ptosis (LPS isn't innervated)
What is Park's Three Step Test used for?
To determine the paretic muscle responsible for a vertical deviation
Park's Step 1: What do you assess and what does it tell you?
Direction of vertical deviation in primary gaze — gives 4 possible paretic muscles (e.g., R hyper = RIR, RSO, LSR, LIO)
Park's Step 2: What do you assess and what does it tell you?
Whether deviation is greater in right or left gaze — deviation increases when the paretic muscle is more purely vertically acting (recti in abduction, obliques in adduction)
Park's Step 3: What do you assess and what does it tell you?
Whether deviation is greater with right or left head tilt — deviation increases when the paretic muscle is forced to work (superiors intort, inferiors extort)
Park's Test result: R hyper, greater in R gaze, greater in R tilt → paretic muscle?
LIO
Park's Test result: R hyper, greater in R gaze, greater in L tilt → paretic muscle?
RIR
Park's Test result: R hyper, greater in L gaze, greater in R tilt → paretic muscle?
RSO
Park's Test result: R hyper, greater in L gaze, greater in L tilt → paretic muscle?
LSR
Park's Test result: L hyper, greater in R gaze, greater in R tilt → paretic muscle?
RSR
Park's Test result: L hyper, greater in R gaze, greater in L tilt → paretic muscle?
LSO
Park's Test result: L hyper, greater in L gaze, greater in R tilt → paretic muscle?
LIR
Park's Test result: L hyper, greater in L gaze, greater in L tilt → paretic muscle?
RIO
How does an RSO palsy patient present using Park's Three Step Test?
R hyper deviation in primary gaze, deviation increases in left gaze, deviation increases with right head tilt
What head position does an RSO palsy patient prefer and why?
Left head tilt — it takes the RSO out of its action, reducing the deviation
What are the clinical signs/considerations for RSO palsy management?
Check if new vs. longstanding (longstanding = expanded vertical vergence range, no diplopia); if new, consider tumor or increased intracranial pressure; prism or surgery may be options
What is 4th nerve palsy associated with clinically?
Head tilt (to the opposite side to compensate)
What is Brown's Syndrome?
A restrictive condition where the SO tendon sheath (or trochlea) prevents the IO from elevating in adduction — looks like IO palsy but is restrictive, not neurogenic
How do you differentiate Brown's Syndrome from RIO palsy?
Forced duction test — full movement in non-restrictive (true palsy), restricted in Brown's; ductions are also full in paresis
What is Incomitant deviation?
The amount of deviation changes depending on the direction of gaze
What is Duane's Retraction Syndrome?
Co-contraction of MR and LR causing retraction of the globe on adduction
What is Type I Duane's Retraction Syndrome?
Abduction impaired, retraction on adduction
What is Type II Duane's Retraction Syndrome?
Adduction impaired, retraction on adduction
What is Type III Duane's Retraction Syndrome?
Both abduction and adduction impaired, retraction on adduction
What do ALL types of Duane's Retraction Syndrome have in common?
Retraction on adduction
What is the prevalence and most common type of Duane's Retraction Syndrome?
~1 in 3000; 75% are Type I
Why does Duane's occur neurologically?
The CN VI nucleus doesn't form properly, so the LR ends up being innervated by CN III instead, causing co-contraction
What are the two types of EOM fibers?
Twitch muscle fibers (global layer, high glycolytic enzymes) and slow muscle fibers (orbital layer, rich in oxidative enzymes for prolonged contraction)
What is the global layer of EOM?
Contains twitch muscle fibers with high glycolytic enzymes; responsible for fast, phasic movements
What is the orbital layer of EOM?
Contains slow muscle fibers rich in oxidative enzymes; supports prolonged, tonic contraction
What is the histological classification of extraocular muscle?
Striated muscle
What are muscle pulleys?
Connective tissue rings that tether EOMs to the orbit, keeping them from slipping when the eye moves away from primary gaze; they alter non-primary gaze kinematics
What is the passive vs. active pulley theory?
Passive: pulleys are fixed; Active: muscles adhere to pulleys and actively change pulley position as the eye moves (still being researched)
Define a saccade
An abrupt voluntary shift in fixation from one point to another (e.g., as occurs in reading); stimulus is target displacement on the retina
What is the PPRF?
Paramedian Pontine Reticular Formation — the conjugate gaze center in the pons; generates conjugate eye movements to the ipsilateral side
What is the MLF?
Medial Longitudinal Fasciculus — a highly myelinated tract connecting the CN VI nucleus to the contralateral CN III nucleus for fast, simultaneous conjugate gaze signals
What is the normal saccade pathway for a rightward saccade?
Left frontal cortex → inhibits omnipause neurons → releases inhibition of right PPRF → right PPRF signals right CN VI (fires right LR) AND sends interneuron via MLF to left CN III nucleus (fires left MR)
What do omnipause neurons normally do?
Tonically inhibit the PPRF, preventing unwanted saccades
What is INO (Internuclear Ophthalmoplegia)?
A lesion of the MLF causing adduction lag on the affected side during conjugate gaze, because the signal from CN VI nucleus cannot reach the contralateral CN III nucleus
What are the clinical signs of INO?
Adduction lag on the affected side, possible nystagmus on abduction of the fellow eye (due to Hering's Law), convergence is unaffected
Why is convergence unaffected in INO?
Convergence uses a different pathway that does not travel through the MLF
How does INO differ from a partial CN III / MR palsy?
In INO, convergence is preserved (MR works); in partial CN III palsy, convergence would also be impaired
What are the etiologies of INO?
MS (multiple sclerosis) and vertebrobasilar disease
What is Binocular INO (BINO)?
Lesions in both MLFs — right eye cannot move left in left gaze AND left eye cannot move right in right gaze, but both eyes can still converge (MRs work, MLFs do not)
What is a Left VI (CN VI) palsy?
Impaired abduction of the left eye; deviation is greater when the paretic left LR is forced to work (i.e., in left gaze); the deviation is always larger when the paretic eye is fixating
What head turn compensates for a Left VI palsy?
Left head turn — brings the eyes into right gaze relative to the head, keeping the left eye out of its field of action
What is the primary/secondary angle of deviation concept in palsies?
Primary deviation = deviation when the normal eye fixates (smaller); Secondary deviation = deviation when the paretic eye fixates (larger, due to excess innervation per Hering's Law)
How do duction (monocular) and version (binocular) testing help evaluate EOMs?
Both should produce full and smooth movements; careful comparison of the two eyes in diagnostic action fields (Broad H test) helps detect paretic muscles
define one and a half syndrome
taking out ipsilateral pprf, cn 6 nucleus, and mlf
nly thing were left with is contralateral eye being able to abduct
T/F: Pursuit eye movements also go through the conjugate gaze pathway
true
What is the DEM test
Developmental Eye Movement Test
assesses saccadic eye movements during reading
three substests where A&B are vertical (controls for number knowledge) and C is horizontal (stimulates reading)
What does the DEM test calculate?
Total time
adjusted time
ratio between horizontal adjusted time and vertical adjusted time
high ratio suggests saccadic dysfunction rather than number recognition problem
What is the King-Devick Test
measures saccadic eye movements
pt reads #’s on cards as fast possible. three test levels
How is the King-devick test scored
scored by time and errors, then compared to age norms of ages 6-14 (NYSOA)
failure = >1std dev away from norm
What is the most common use for King-Devick test
commonly used for concussion screening