Week 3 - General senses - Pain
1/15
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
16 Terms
General senses breakdown
General sense → receptor
Touch, proprioception, vibration → mechanoreceptors
Temperature → thermoceptors
Pain → nociceptors
Pain: Definition
“An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage.”
Important to survival
Protective mechanism - notifies tissue damage, preventing further damage
Pain: Nociception stimulus
Triggers:
Initial damage from external causes (e.g blunt trauma) or internal causes (e.g inner tumor)
Ongoing disease causing tissue damage
2 Pain types: based on duration of pain
Acute pain - Disappears when tissue damage is gone
Chronic pain - Longer lasting, can linger even after the disappearance of injury
Pain and psychology are intertwined: Optimism & pessimism can decrease or increase pain respectively. Cultural values can lead to stoicism or downplaying of pain.
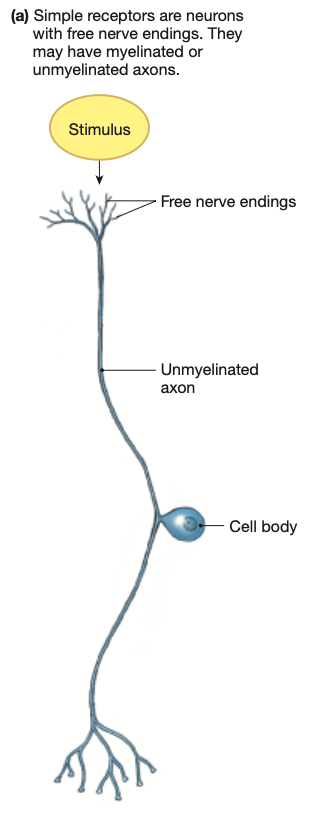
Pain: Nociceptors
Free nerve endings.
Pain receptors are spread thoughout the ENTIRE body SANS for the brain.
4 Pain types: based on type of painful stimuli:
Thermal
Chemical
Mechanical
Polymodal (two or more of the above)
Can be triggered by the stimulus itself OR by chemicals released by neighbouring cells from tissue damage (cytokines)
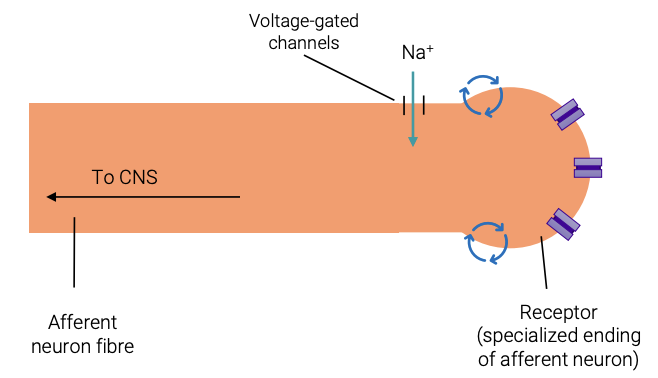
Pain: Nociceptor activation
Initial tissue damage from injury or ongoing disease
Mechanical/electrical/thermal/chemical stimuli or cytokines from damaged cells cause the opening of ion channels within the neuron’s cell membrane
Positive ions flow into the cell, causing depolarisation
If threshold potential reached, action potentials are generated from the opening of Na+ voltage-gated ion channels
Signals sent to CNS
Pain perceived
Pain: Example - Capsaicin
Triggers thermal nociceptors
Capsaicin binds to chemically-activated ion channels on nociceptors sensitive to temperatures above 37 degrees.
Hence, leads to “burning sensation” and “hotness”
Capsaicin stays bound to the membrane for a long time, leading to a large amount of action potentials being sent for a long duration
In this period, pain from OTHER stimuli is sensed less intensely
Hence, capsaicin is a topical analgesic (painkiller)
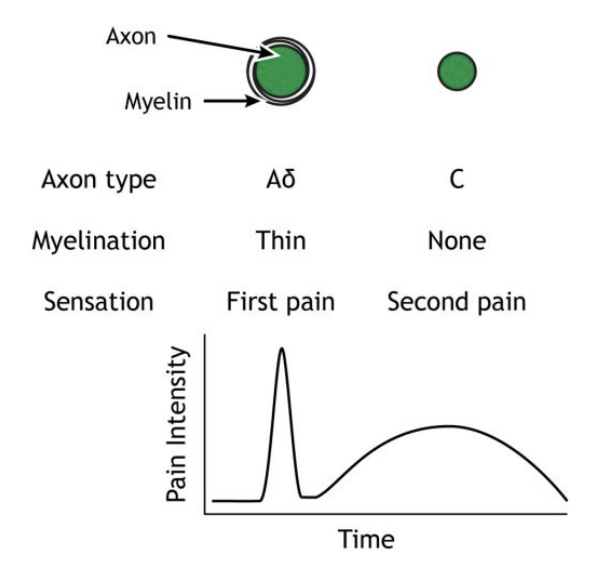
Pain: 2 nociceptor types: based on phases after immediate injury:
2 Nociceptor types (a.k.a 2 types of Pain receptors)
Aδ fibers. (“a-delta”) - FIRST pain
Type C fibres - SECOND pain
Pain: Nociceptor types - Aδ fibers
Activates in response to intense pressure, cuts on the skin, or extreme hot & cold temperatures
Small receptive fields = identifies precise location of injury
“First pain” - Initial tense, sharp and localised pain
Neurons are lightly myelinated, small in diameter
Myelin increases action potential speed, small diameter lower speed - signals transmitted slowly
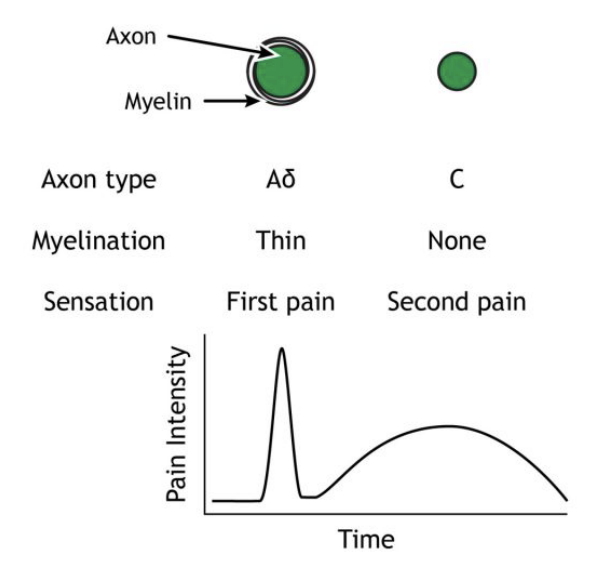
Pain: Nociceptor types - Type C fibres
Activates in response to all painful stimuli
Large receptive fields = provides course/rough info on location of injury
“Second pain” - Mild burning or aching pain, more widespread
Neurons are unmyelinated, very small in diameter
No myelin decreases action potential speed, extreme slim diameter further slows speed - signals transmitted very slowly
Over 70% of pain signals sent by Type C fibres
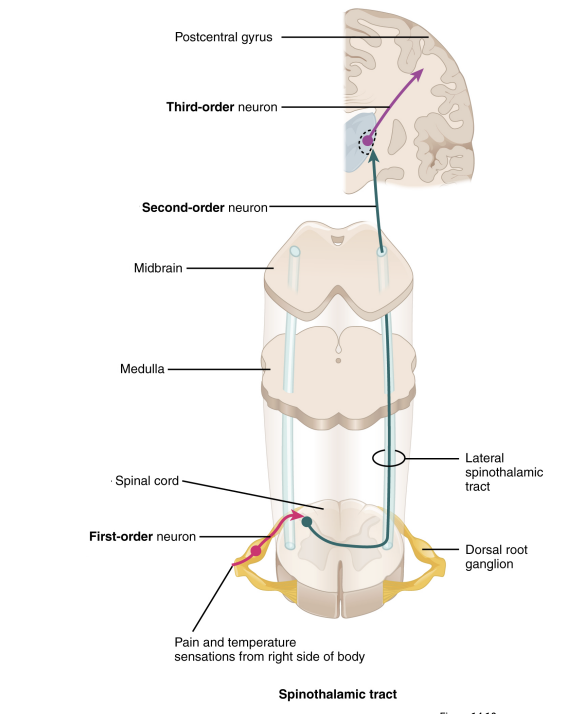
Pain: Neural pathways - Spinothalamic tract
Thermoreceptor stimulated
First-order neuron:
Action potential travels to the spinal cord,
Immediately synapses at the spinal cord on the side of sensation
Second-order neuron:
Decussates in spinal cord, crossing over to the other side and up the spinal cord (travels contralateral to the sensation)
Synapses in the thalamus
Third-order neuron:
Travels to the various region in the brain
Somatosensory cortex (“sensory homunculus”)
Anterior cingulate cortex
Frontal lobe
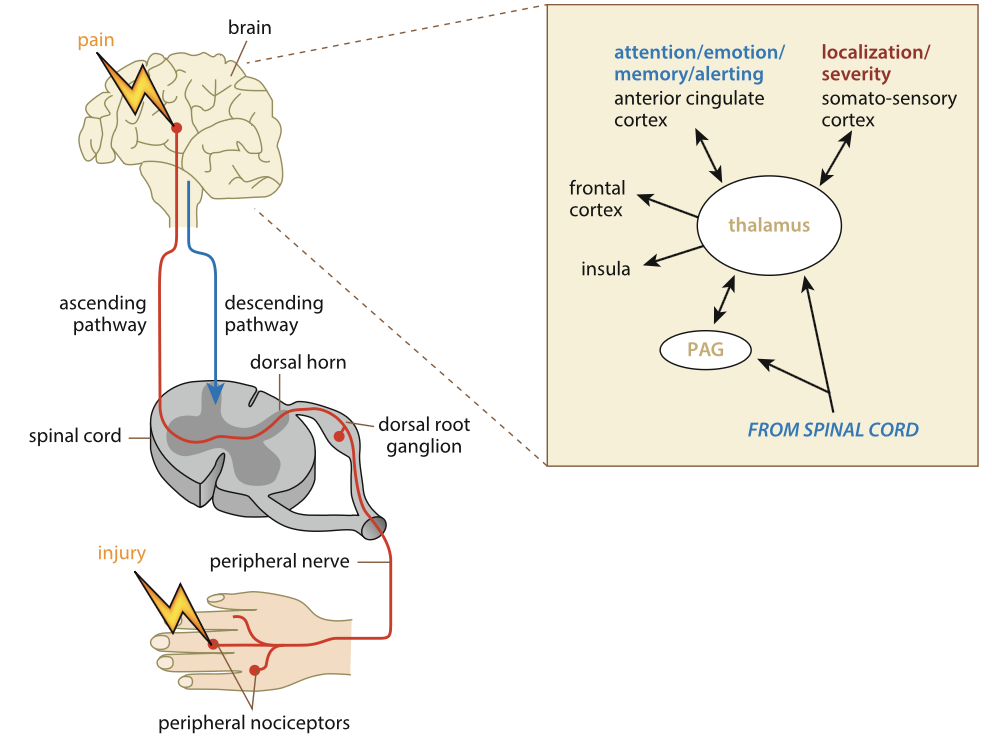
Pain: Neural inhibition - Gate-control theory
Not all pain signals make it to the brain, some are stopped halfway by inhibition (i.e painkillers). There are many locations where inhibition can occur:
Opioid interneurons
Descending pathways (PAG = periaqueductal gray matter)
Gate-control theory: Both of these inhibitory systems work in tandem to prevent excess pain signals from reaching the brain, becoming a “gate” that must be opened with enough force to warrant notifying the brain.
Prevents harmless signals from being perceived as pain
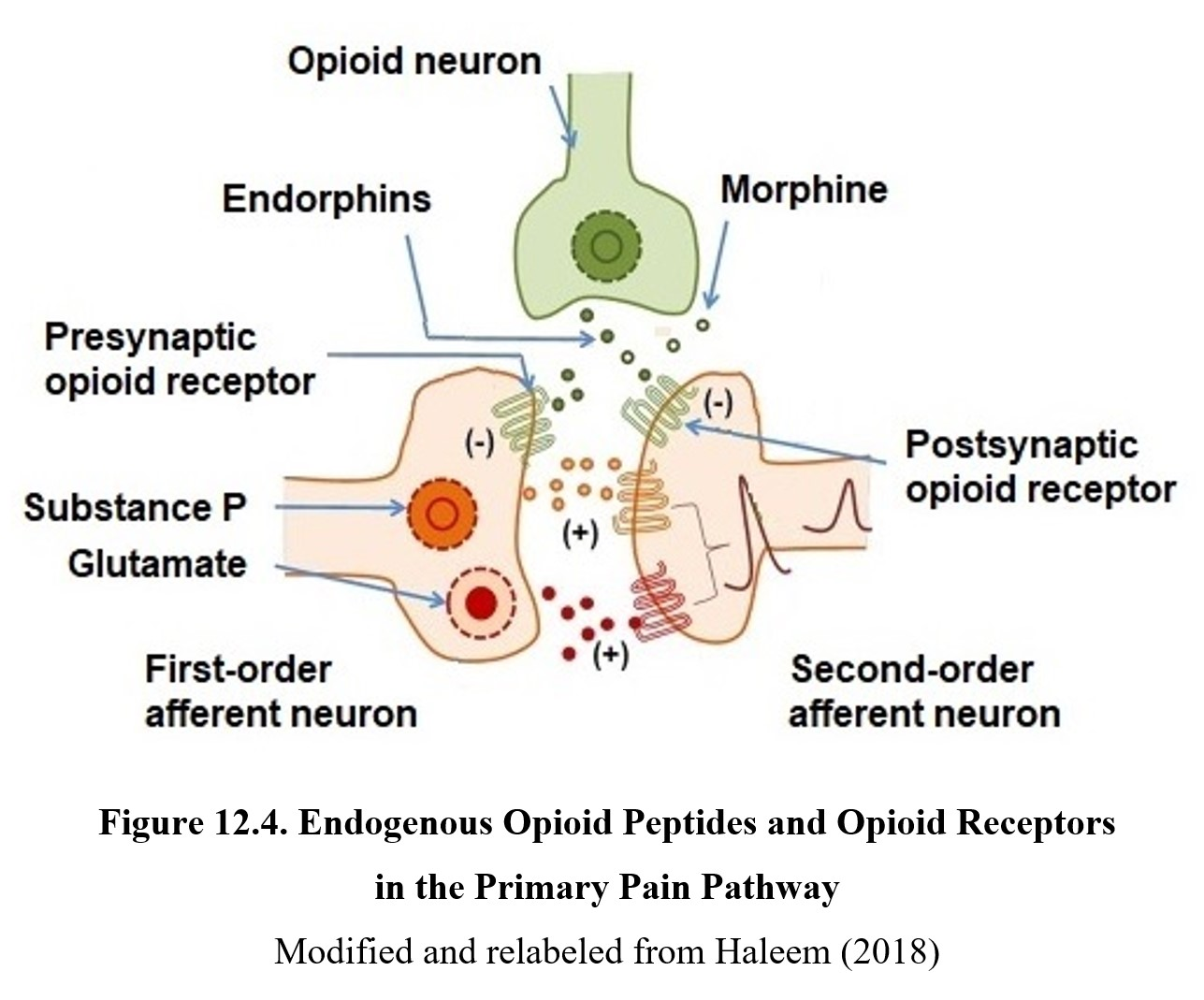
Pain: Neural inhibition - Opioid interneurons
Opioid: Chemical with pain-relieving effects
Littered throughout the spinal cord are opioid interneurons that when activated, release opioids which inhibit pain signals
Prevents transmission of pain signals between the first & second order neurons on the spinothalamic tract.
Pain: Neural inhibition - PAG (Periaqueductal gray matter)
PAG (Periaqueductal gray matter): Found in the brain stem, origin of descending inhibitory pathway from the brain. Descending neural pathway from brain to spinal cord.
When pain signals reach the brain, neurons in the PAG are activated
PAG neurons send inhibitory signals down the spinal cord
Prevents further pain signals from reaching the brain
Acts on the second-order neuron in the spinothalamic tract
Pain: Pain threshold & tolerance
EVERYONE has the SAME pain threshold.
e.g 44-46 degrees is sensed as painfully hot for all humans
Pain tolerance can vary widely.
Just because you can tolerate something, does not mean it is not being sensed regardless
Persistent pain stimuli can decreases pain tolerance (e.g chronic pain)
Cultural and psychological factors
Tolerance increases with age and modified by emotions and mental state
Pain and psychology are intertwined
Pain: 2 Pain types: based on location of painful stimuli:
Somatic pain: Skin, muscles, joints
Superficial somatic pain: sharp, prickling pain, localised on the epidermis, tends to be brief in duration
Deep somatic pain: burn, itch or ache, localised to joints, muscles and deeper dermis layers, longer lasting, can be chronic (arthritis)
Visceral pain: Inner organs
Dull aching, gnawing, vague burning (like hunger)
Stimuli can be extreme stretching of tissue, ischemia (restriction of blood supply to tissues), muscle spasms, noxious chemicals
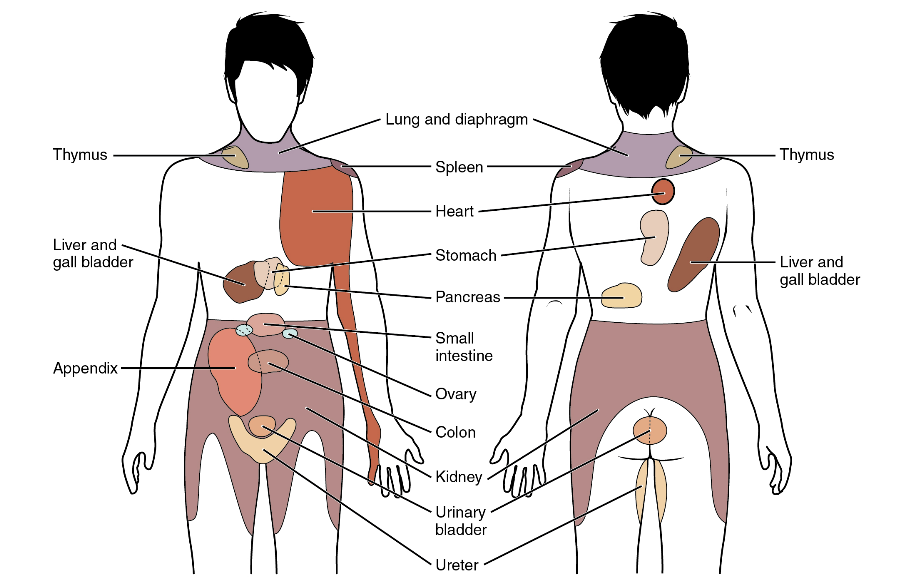
Pain: Somatic & visceral pain: Referred pain
Both somatic & visceral pain share many neural pathways. Visceral pain is much less common and hence, the brain can often mistake visceral pain for the much more common, somatic pain.
Referred pain = somatic pain perceived when stimulus is actually visceral.
Lack of acuity in the brain mixes up perception of somatic & visceral pain
Crucial for mapping the body, helping clinicians identify visceral pain before major damage occurs.
e.g males experiencing shoulder pain, may actually have visceral heart pain
Diagram: map of somatic pain that correlates to visceral pain