Antibacterial Pharmacology III: DNA Disruptors: Sulfonamides, Fluoroquinolones, Nitroimidazoles
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
DNA Disruptors
- sulfonamides
- fluoroquinolones
- nitroimidazoles
Sulfonamide agents
- sulfamethoxasole/trimethoprim (SMX/TMP) (Bactrim, Septra)
- sulfadiazine, sulfisoxazole, sulfacetamide
sulfamethoxazole/trimethoprim (SMX/TMP)
- bactrim, septra
- PO, tablet, IV
- SS: 400 mg/80 mg
- DS: 800 mg/160 mg
- ratio of SMX to TMP will always be 5:1
What will Bactrim dosage be based on?
always based on the trimethoprim component
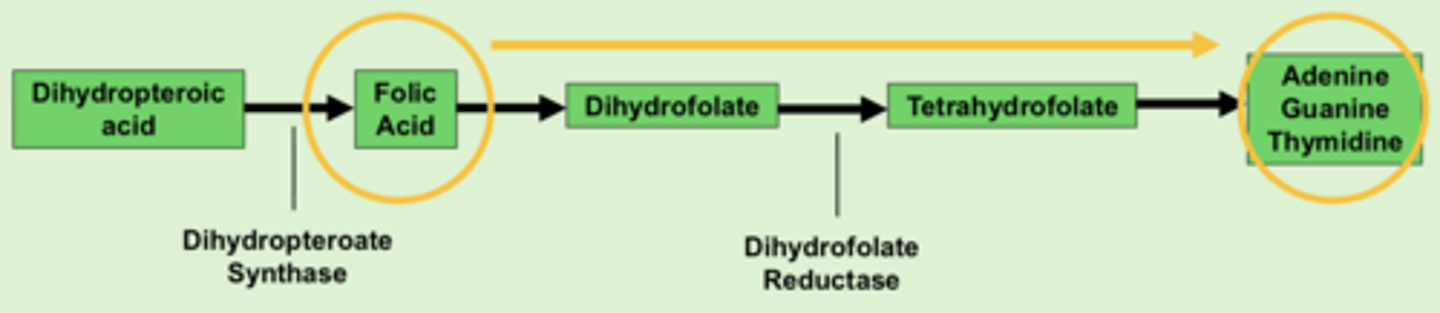
Normal bacterial mechanism: Folic acid
folic acid needed for DNA components (adenine, guanine, thymidine)
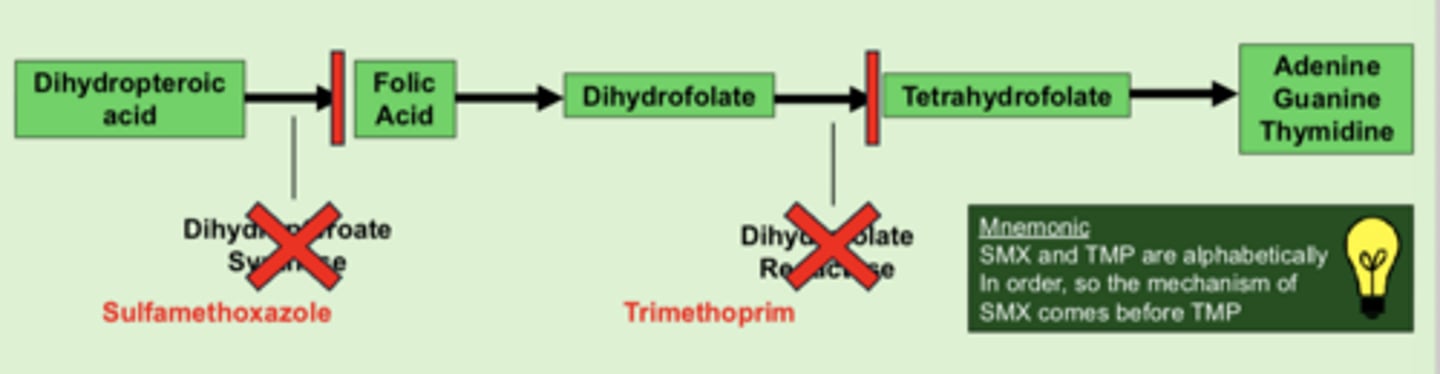
SMX/TMP MOA
- SMX inhibits dihydropteroate synthase --> blocks formation of folic acid
- TMP inhibits dihydrofolate reductase --> blocks formation of tetrahydrofolate
- ultimate result is blocking DNA production
- bacetricidal, time-dependent
SMX/TMP Spectrum of coverage for gram (+)
staph spp. including CA-MRSA
SMX/TMP Spectrum can also cover which OTHER pathogens?
- Pneumocystis jiroveci (PJP)
- Toxoplasma gondii
SMX/TMP Clinical Use
- Skin and soft tissue infections (SSTI), especially those caused by community-acquired MRSA
- PJP and toxoplasmosis prophylaxis/treatment in immunocompromised pts (HIV)
- Step-down therapy for severe gram-positive infections
SMX/TMP Metabolism
- weak inhibitor of CYP2C9
- SMX/TMP may increase the anticoagulant effects of Warfarin
SMX/TMP dose adjustment
renal adjustment REQUIRED
SMX/TMP ADRs
- hyperkalemia
- hemolytic anemia in G6PD deficiency
- increased anticoagulant effects of warfarin
SMX/TMP Contraindications
- sulfa allergy
- G6PD deficiency
Which of the following statements regarding sulfamethoxazole/trimethoprim (Bactrim) is correct?
A. SMX works by blocking the formation of tetrahydrofolate (later in the pathway), while TMP blocks the formation of folic acid
B. Instead of SMX/TMP, an alternative agent should be considered in a patient with a serum potassium of 4.9 mg/dL
C. It is safe for a patient with G6PD deficiency to take SMX/TMP
D. The ratio of SMX/TMP is 1:5
B. Instead of SMX/TMP, an alternative agent should be considered in a patient with a serum potassium of 4.9 mg/dL
Fluoroquinolone Medications
- ciprofloxacin IV, PO, ophthalmic, otic
- levofloxacin IV, PO
- moxifloxacin IV, PO, ophthalmic
- delafloxacin IV, PO
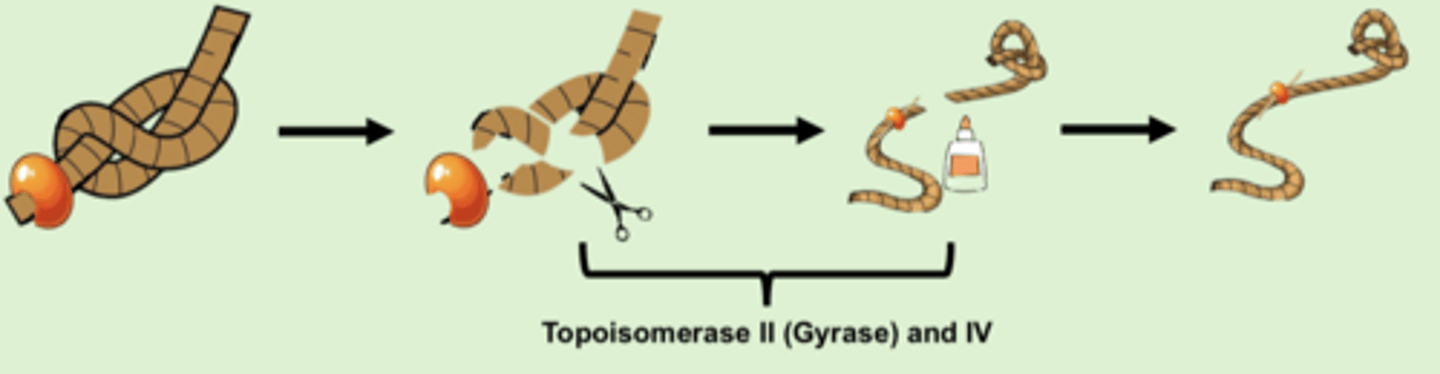
Normal bacterial mechanism that fluoroquinolones impact:
- topoisomerase cuts DNA to allow it to untangle
- once untangled, topoisomerase re-ligates strands together
- topoisomerase II: gram-negative bacteria
- topoisomerase IV: gram-positive bacteria
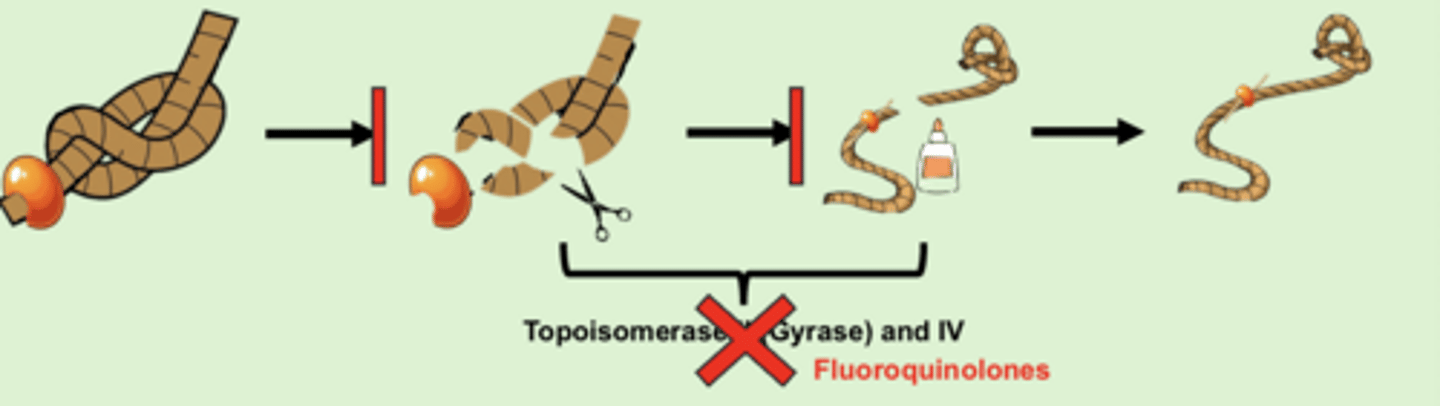
Fluoroquinolone MOA
- fluoroquinolones block topoisomerase
- block topoisomerase II in gram (-) bacteria
- block topoisomerase IV in gram (+) bacteria
- bactericidal, concentration-dependent
Fluoroquinolone spectrum of coverage for gram (+): Respiratory fluoroquinolones
- levofloxacin
- moxifloxacin
- reliable Strep. Pneumoniae coverage
Fluoroquinolone spectrum of coverage for gram (-): What are the ONLY oral agents used for P. aeruginosa coverage?
- levofloxacin
- ciprofloxacin
- ONLY PO agents for P. aeruginosa (rest are IV)
What else do fluoroquinolones cover?
- cover ATYPICAL pathogens
- moxifloxacin has coverage for anaerobic pathogens
Fluoroquinolone Clinical Use
- empiric coverage of complicated UTIs, but increasing resistance
- respiratory infections (CA-pneumonia) for levofloxacin and moxifloxacin
- step-down therapy for severe gram (-) infections
Levofloxacin IV to PO conversion
1:1, same dose and frequency
Absorption of fluoroquinolones is reduced by...
positive cations (Ca, Fe, Mg, Al)
Fluoroquinolone renal
- renal adjustments REQUIRED except moxifloxacin
- moxifloxacin does NOT require renal dose adjustment
Fluoroquinolone ADRs
- tendon inflammation and rupture
- QT prolongation
The physician comes to you, explaining that they are preparing to discharge a pt. They ask for your assistance in converting the pt's IV therapy to oral therapy. The pt was being managed with intravenous levofloxacin, 750 mg once daily for 5 days for community-acquired pneumonia. Today is day 2 o ftherapy. Which of the following doses is appropriate for the patient's outpatient oral levofloxacin management? What other fluoroquinolone could have been used for this lung infection?
A. 500mg po once daily
B. 250mg po once daily
C. 750mg po once daily
D. 750mg po twice daily
- C. 750mg po once daily
- moxifloxacin
Nitroimidazole medications
- metronidazole IV, PO
- tinidazole
Nitroimidazole MOA
- metronidazole is a prodrug
- in an anaerobic environment, the nitro group is reduced into a reactive metabolite that damages DNA so it cant be converted to RNA
- bactericidal, AUC:MIC dependent
Nitroimidazole Spectrum of coverage
- primarily covers anaerobic pathogens
- lacks coverage of gram-positive, gram-negative aerobic pathogens, and atypical pathogens
- RARELY used as monotherapy
Metronidazole IV to PO conversion
1:1
Metronidazole metabolism
- weak inhibitor of CYP3A4
- increases anticoagulant effects of warfarin
Metronidazole renal
NO renal adjustment required
Nitroimidazole ADRs
- metallic taste
- disulfiram-like reaction w/ alcohol
- increased anticoagulant effects of warfarin
T/F: You are working in the inpatient pharmacy and receive an order for IV Metronidazole 500mg TID. After reviewing the patient's labs, you note a serum creatinine of 2.5 mg/dL. Because of renal impairment, this pt may be at risk of toxicity, so an alternative agent should be chosen for anaerobic coverage
FALSE
Which DNA disruptors provide MSSA coverage?
- fluoroquinolones
- sulfonamides
Which DNA disruptor provides MRSA coverage?
sulfonamides- SMX/TMP
Which DNA disruptors provide coverage for P. aeruginosa?
- levofloxacin
- ciprofloxacin
Which DNA disruptors provide coverage for anaerobics?
- moxifloxacin
- metronidazole
Which DNA disruptors provide coverage for atypicals?
fluoroquinolones
Which DNA disruptor is used in PJP & toxoplasmosis prophylaxis/treatment in immunocompromised pts?
SMX/TMP
Which DNA disruptor class can cause QT prolongation?
fluoroquinolones
Which classes of DNA disruptors can increase warfarin's anticoag effect?
- sulfonamides- CYP2C9
- nitroimidazoles- CYP3A4
DNA dirsputors NOT renally adjusted
- moxifloxacin
- metronidazole
T/F: All DNA disruptor classes' MOA are bactericidal
TRUE
What are each of the DNA disruptor classes' MOA's dependent on?
- SMX/TMP - time-dependent
- fluoroquinolons - concentration-dependent
- nitroimidazoles - AUC:MIC-dependent