NEU 165 Exam 2
1/262
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
263 Terms
Why Study Humans?
We are actually the species that is affected
Many human neurological diseases do not occur spontaneously in animals
Animal models allow invasive manipulations of biology but usually in a limited way – animal models are almost always incomplete models of the disease of interest
BUT: Studies of humans are limited by our ability to perform invasive measurements that alter biology
With one major type of exception
Non invasive approaches (imaging)
X-ray Computed Tomography (CT)
Magnetic Resonance Imaging (MRI)
Positron Emission Tomography (PET)
Non invasive approaches (electrophysiology)
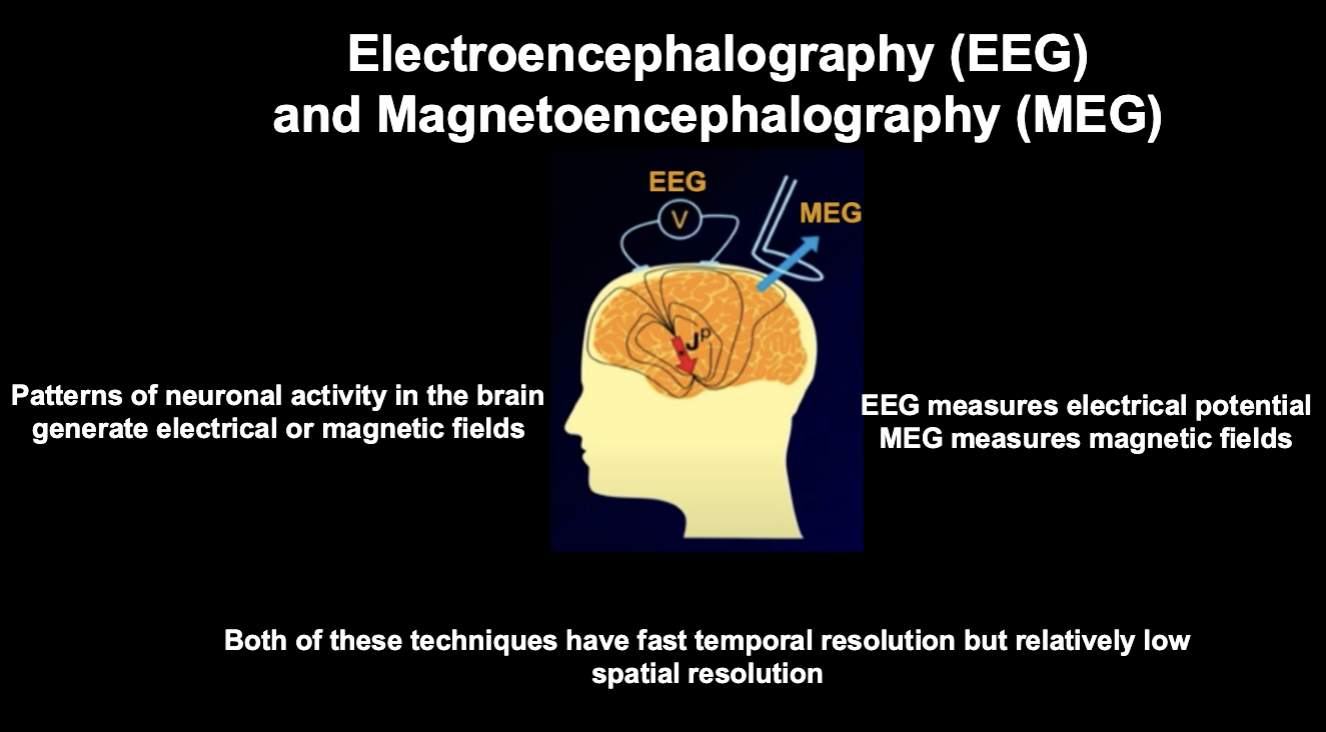
Electroencephalography (EEG)
Magnetoencephalography (MEG)
Non invasive approaches
Neuropsychology
Epidemiology
Biomarkers
Invasive approaches
Electrocorticography (Ecog)
Post mortem measurements (autopsy)
Imaging: Brain structure (x-ray CT and structural MRI)
Neuroanatomy: an image of the brain as if we could hold it in our hand. Allows exploration of size of brain structures, changes over time, individual differences
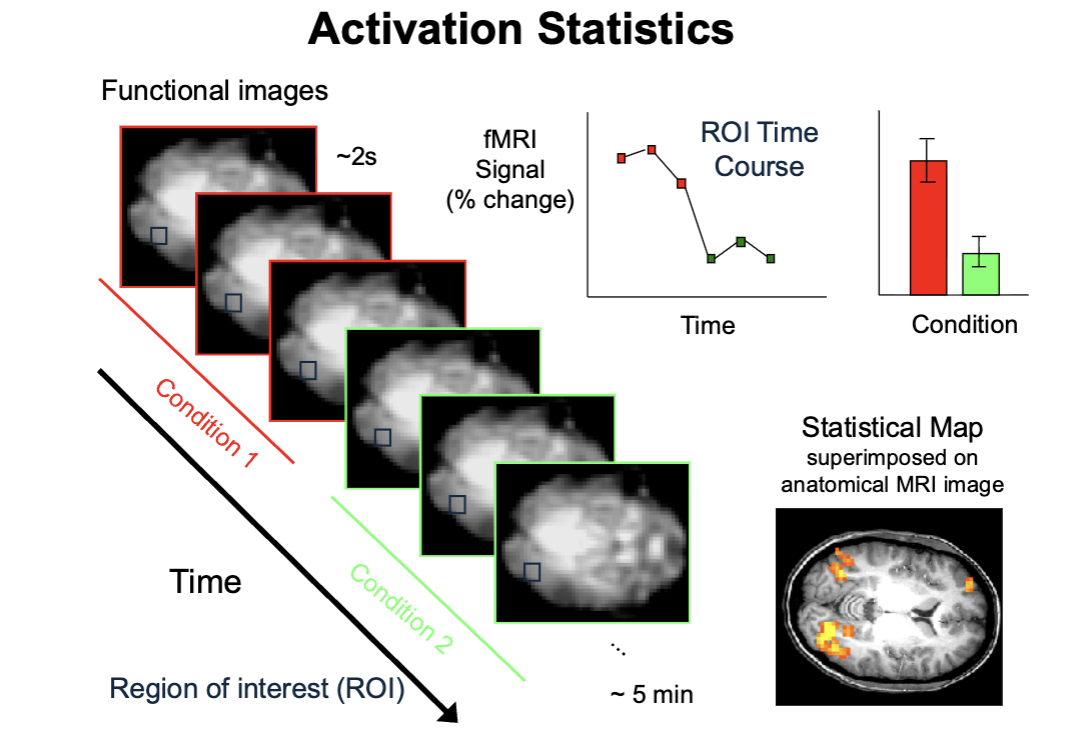
Imaging: Brain function (functional MRI)
What the brain is doing as we think. Relies on alterations in cerebral blood flow, which is driven by metabolic demand
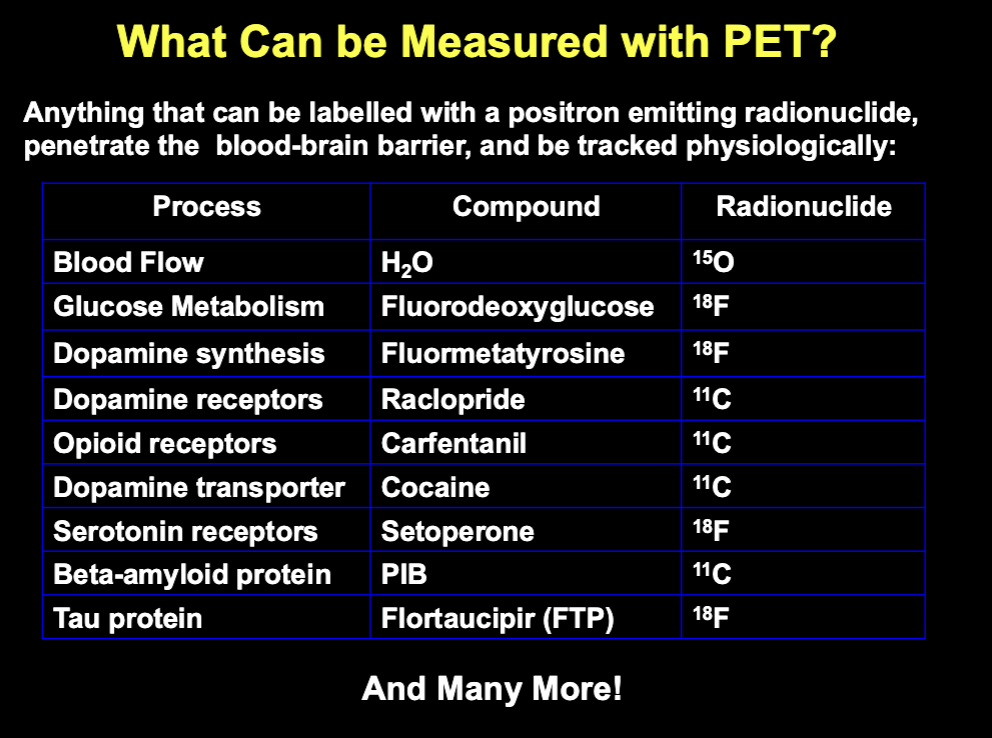
Imaging: Brain chemistry (PET)
Measurement of neurotransmitters, transmitter receptors and reutake sites, enzymes, abnormal protein aggregates
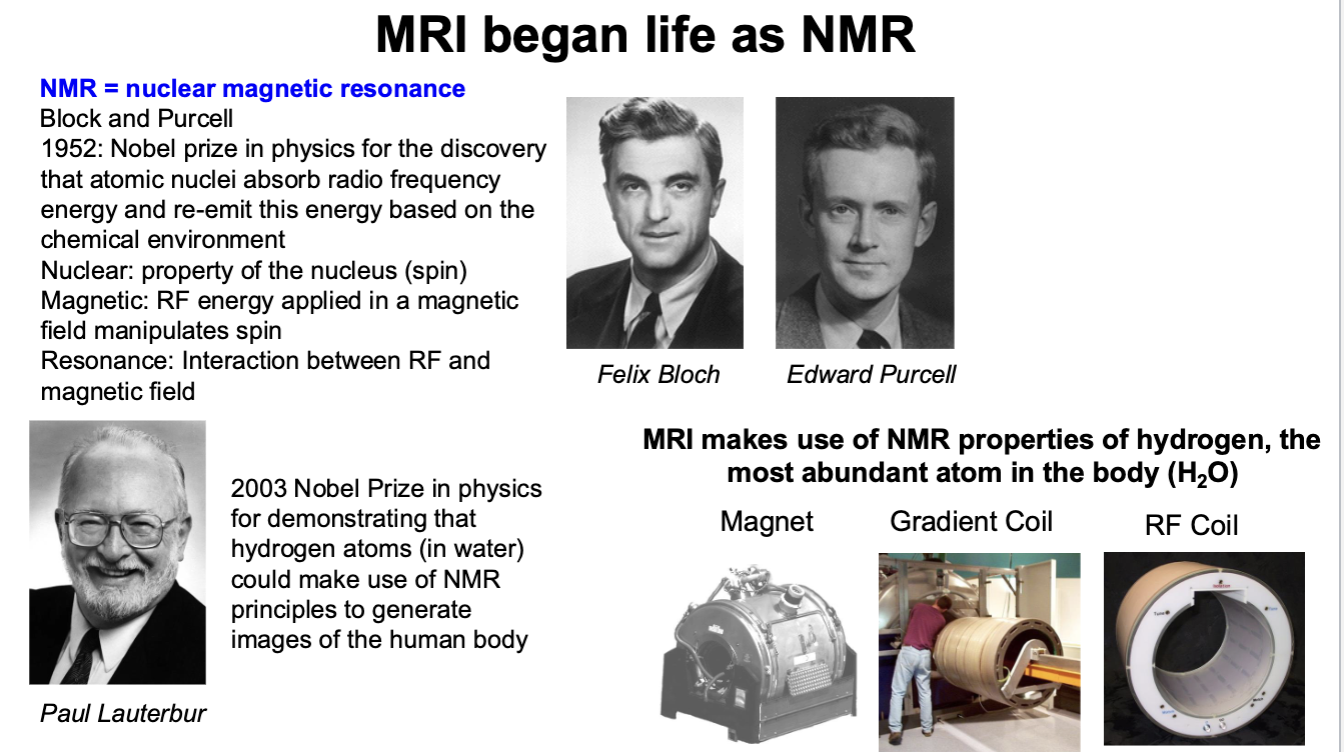
MRI began life as NMR
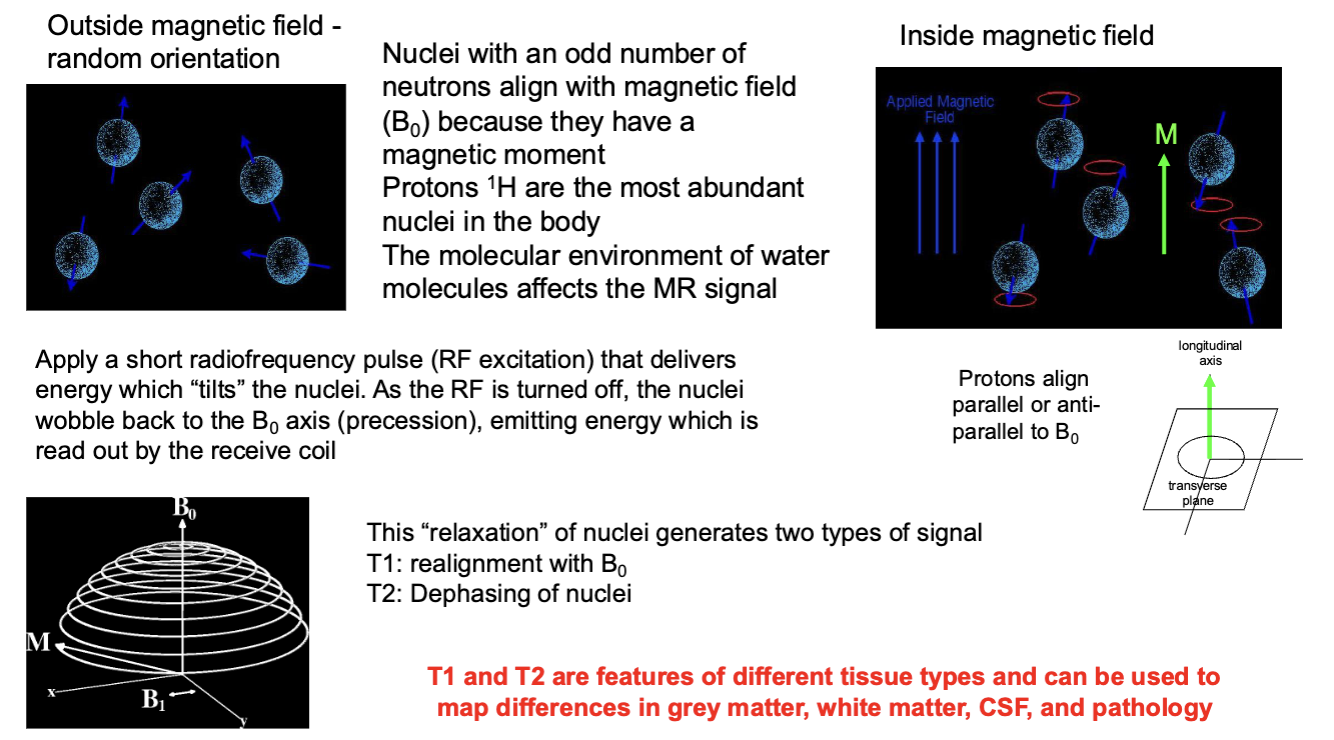
MRI Magnetic Fields Information
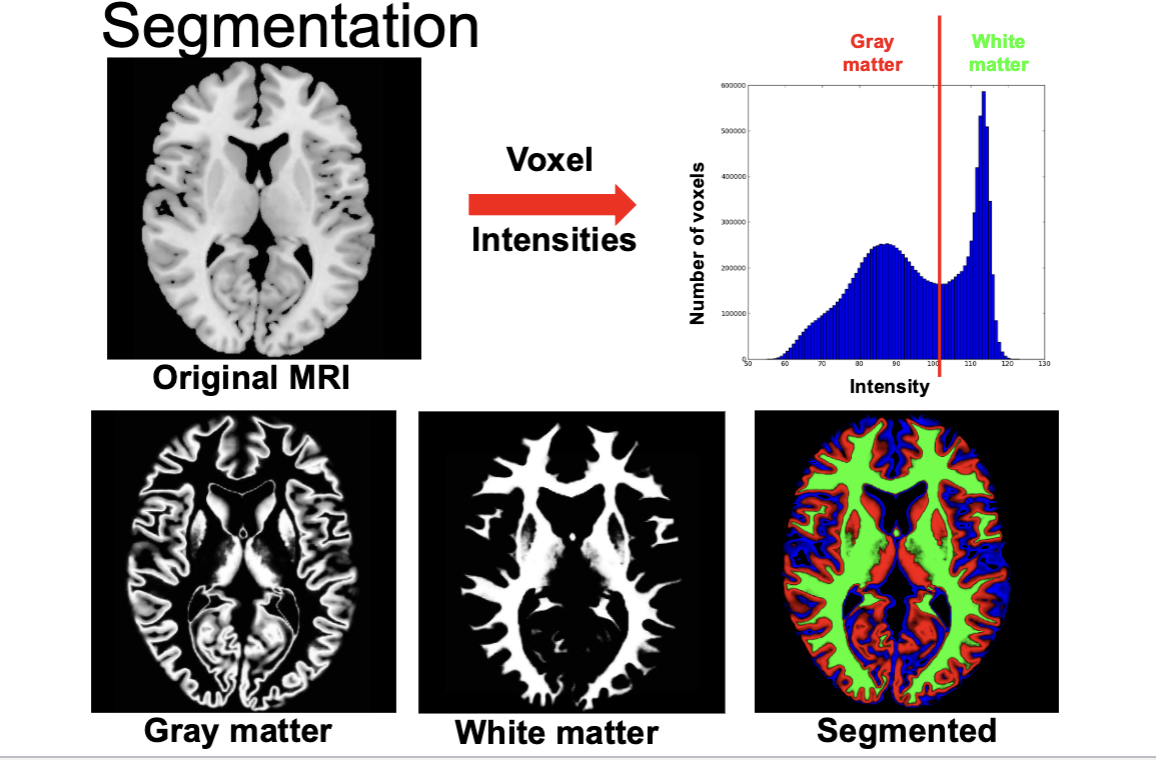
MRI Voxels
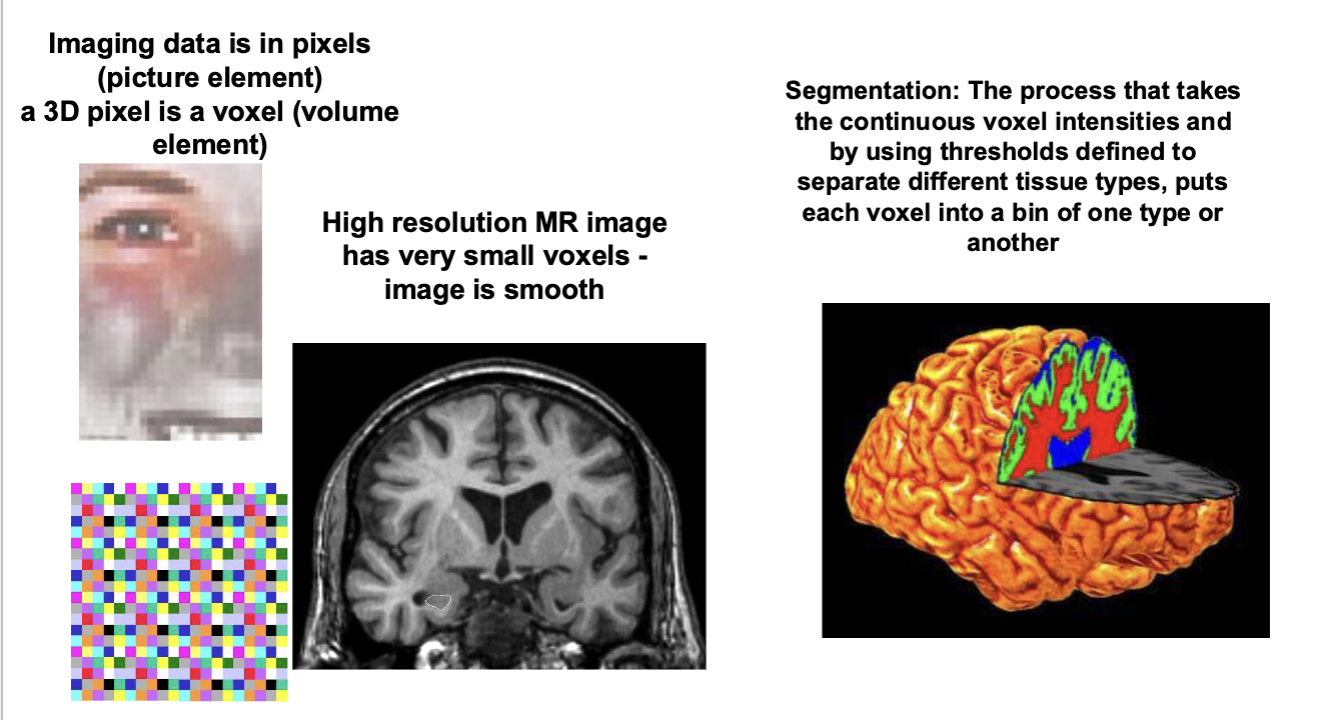
MRI Segmentation
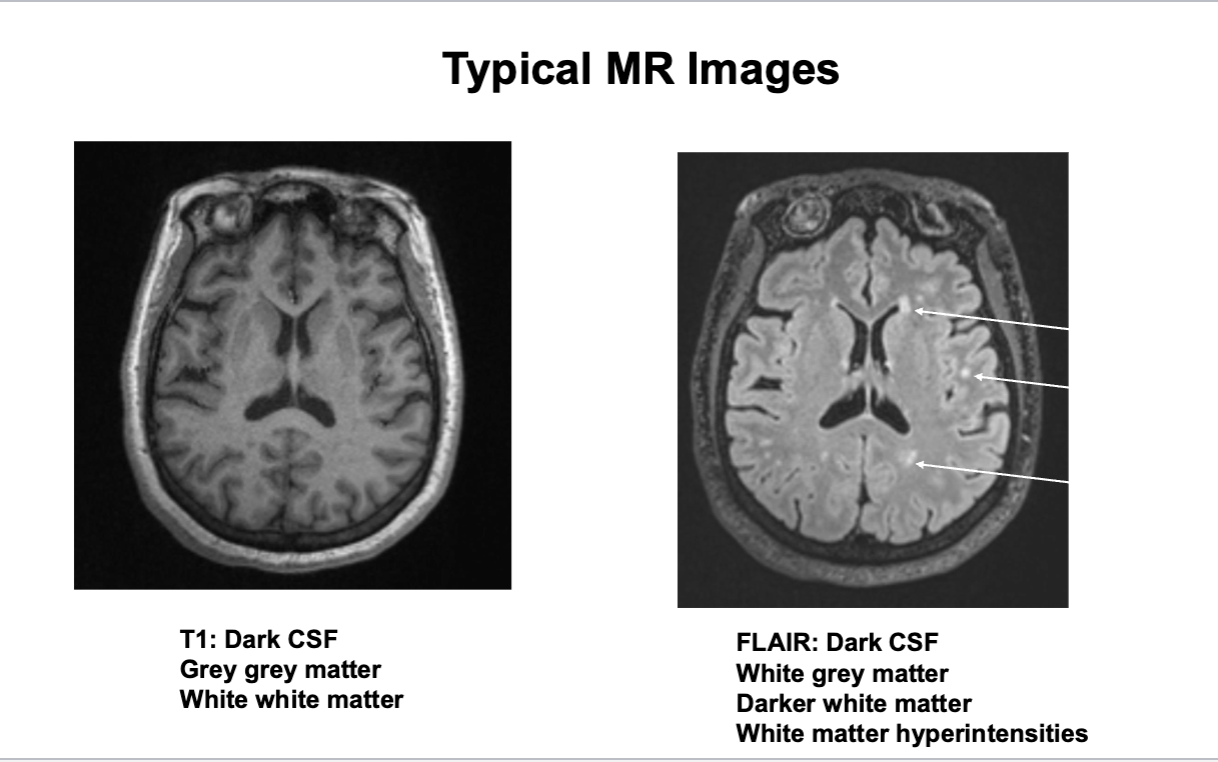
Typical MR Images
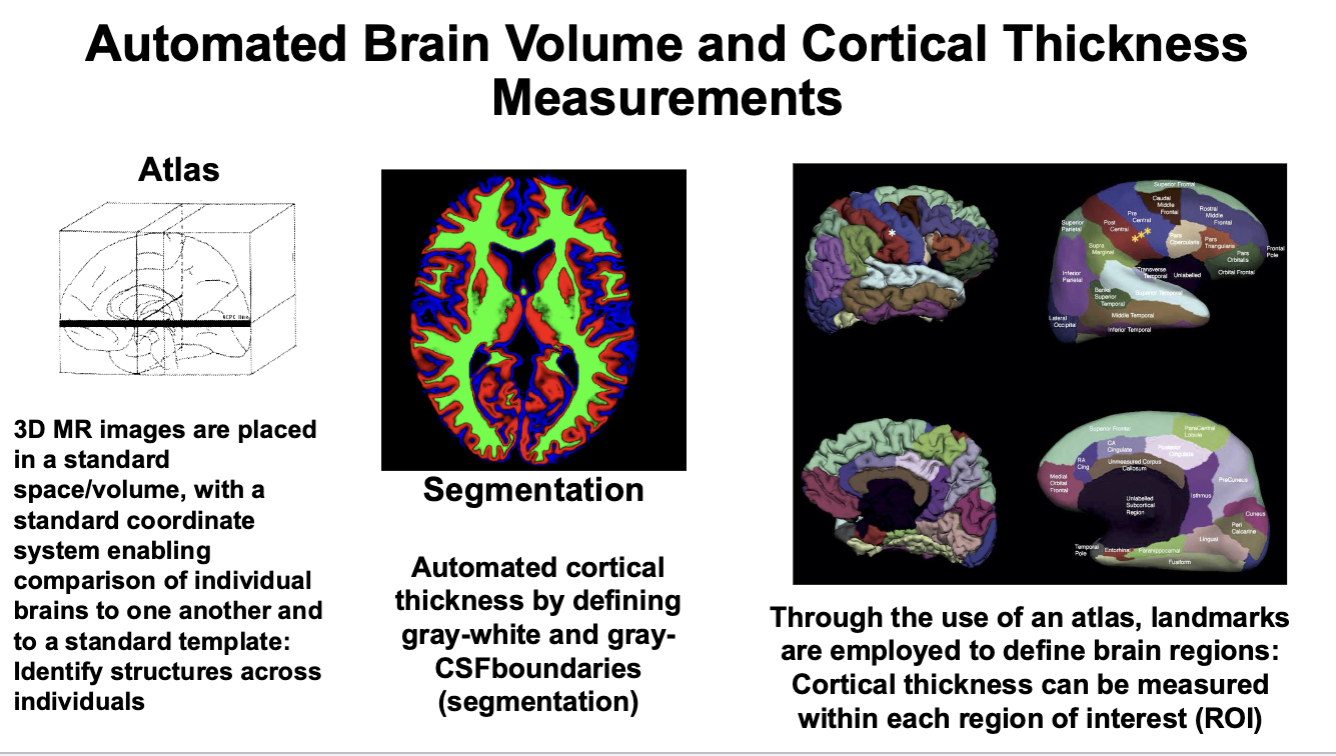
Automated Brain Volume and Cortical Thickness Measurements
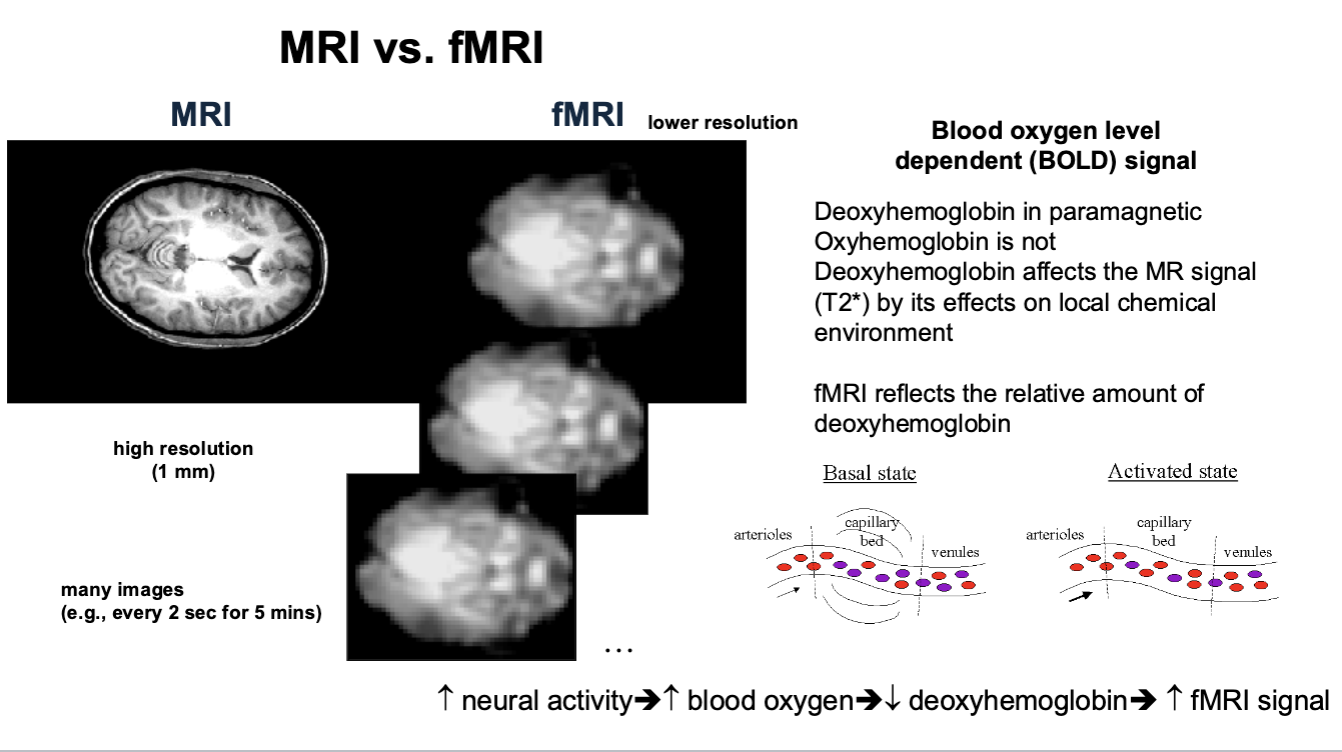
MRI vs. fMRI
fMRI Activation Statistics
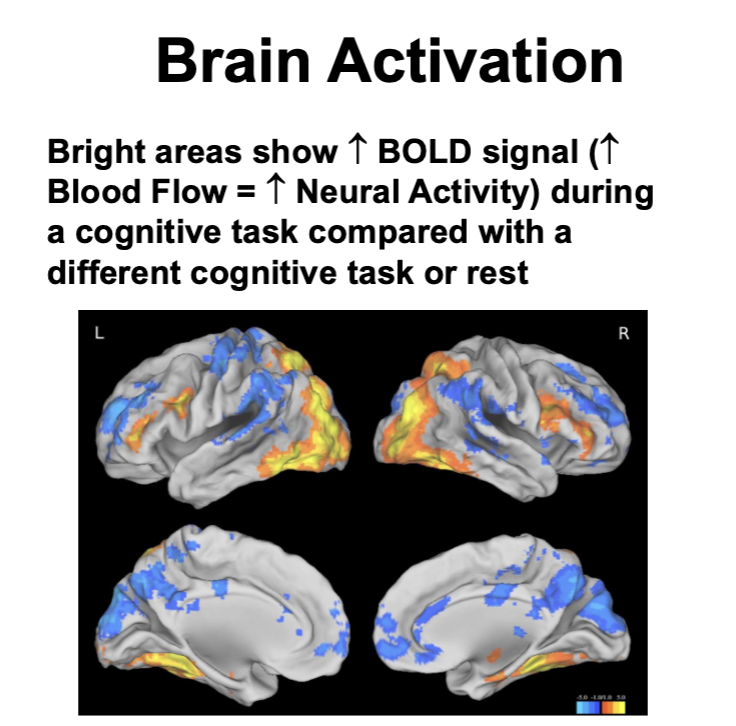
Brain Activation
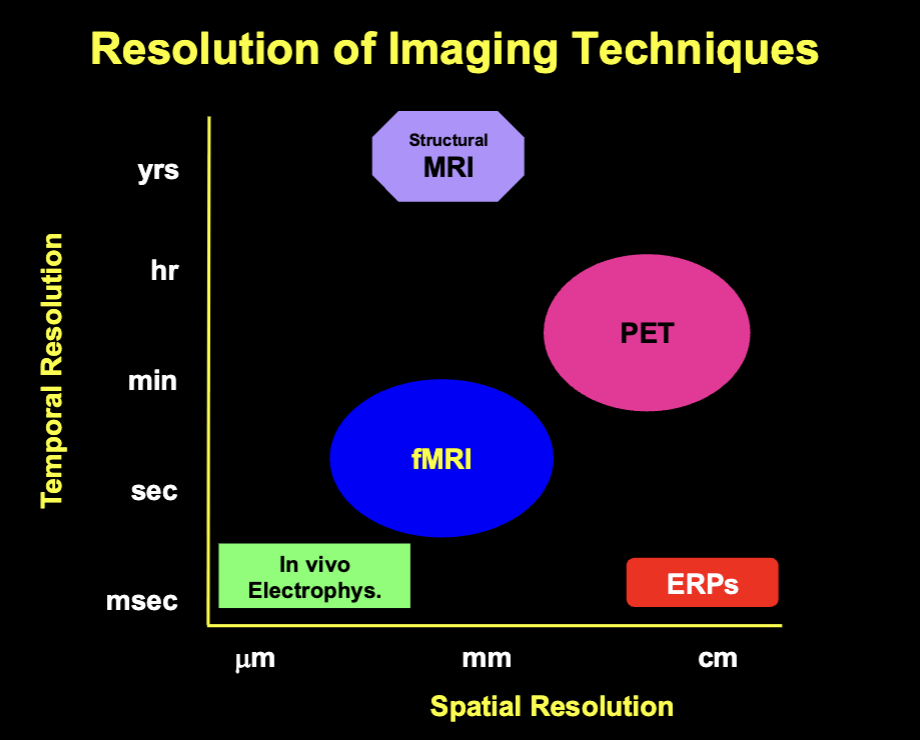
Resolution of Imaging Techniques
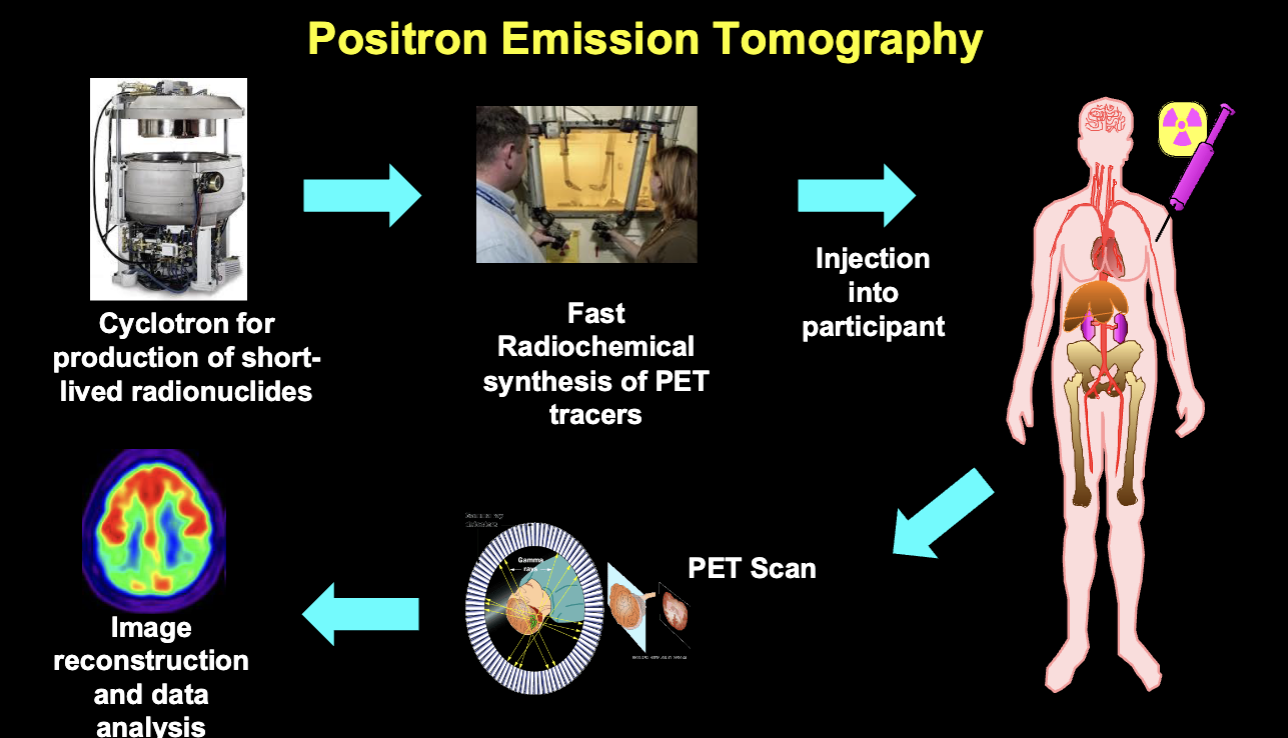
Positron Emission Tomography
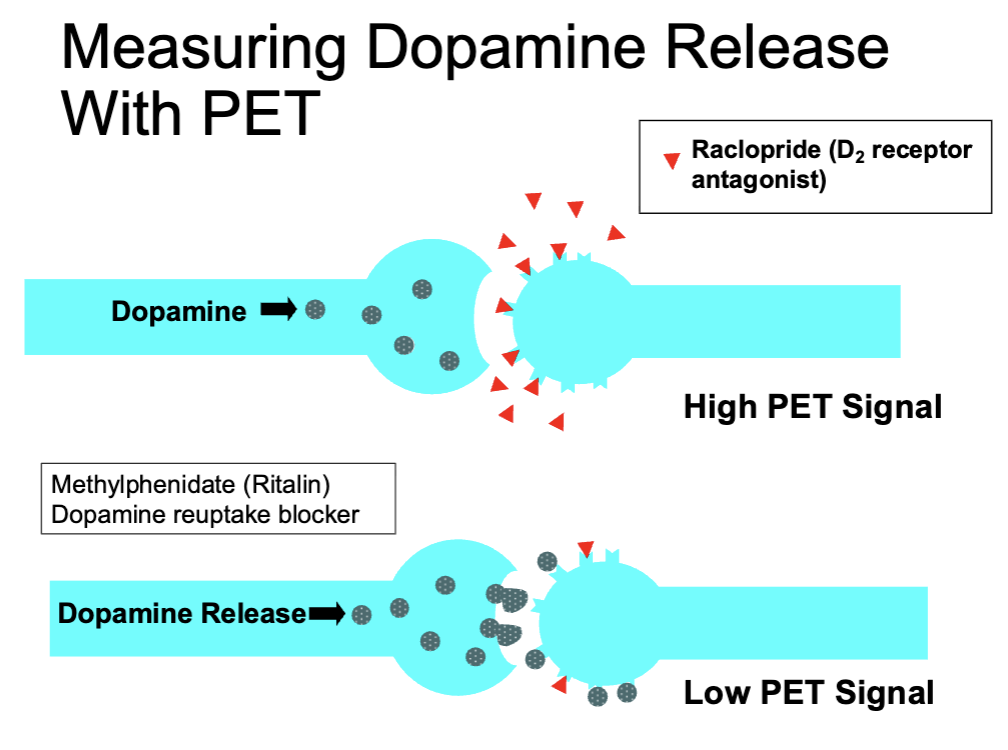
Measuring Dopamine Release with PET
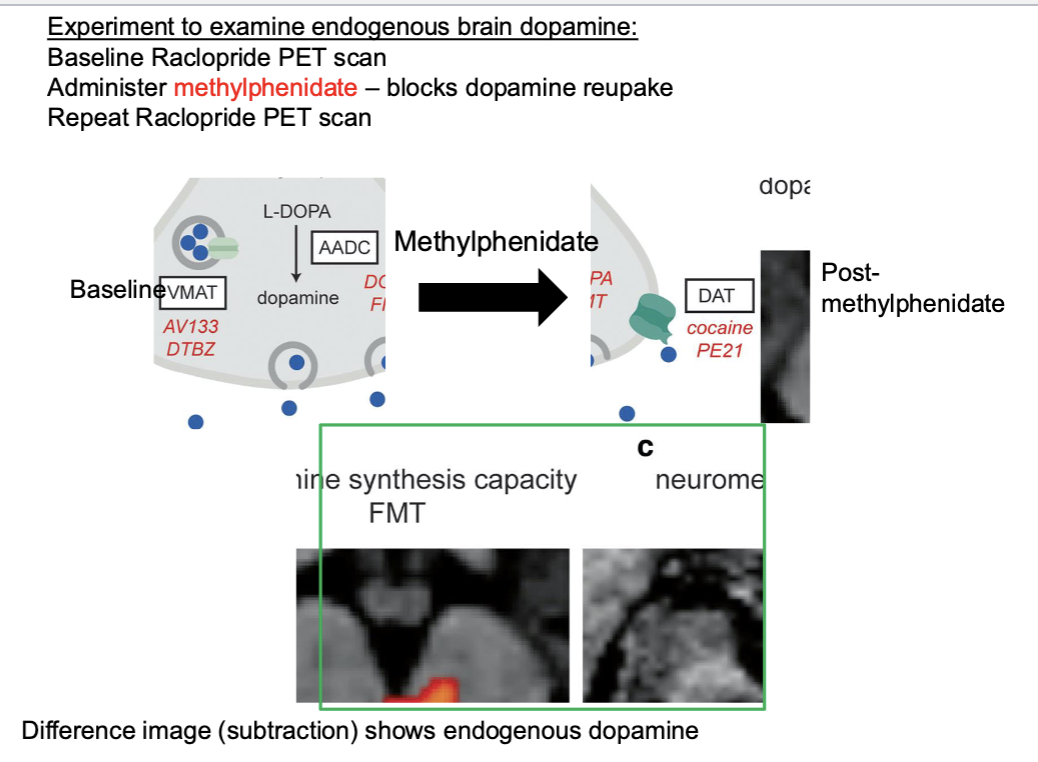
Experiment to examine endogenous brain dopamine
Basic Principles of PET
Radiation
Biological effects are related to
dose
half-life
organ distribution
PET tracers are given in the lowest dose compatible with good signal
Half-life is ~1 min to 2 h
Widely distribiuted in the body
Doses are so low that the risk is not measurable
Risk is usually described in relation to 1 year of background radiation at sea level
PET vs MRI
What can be measured with PET?
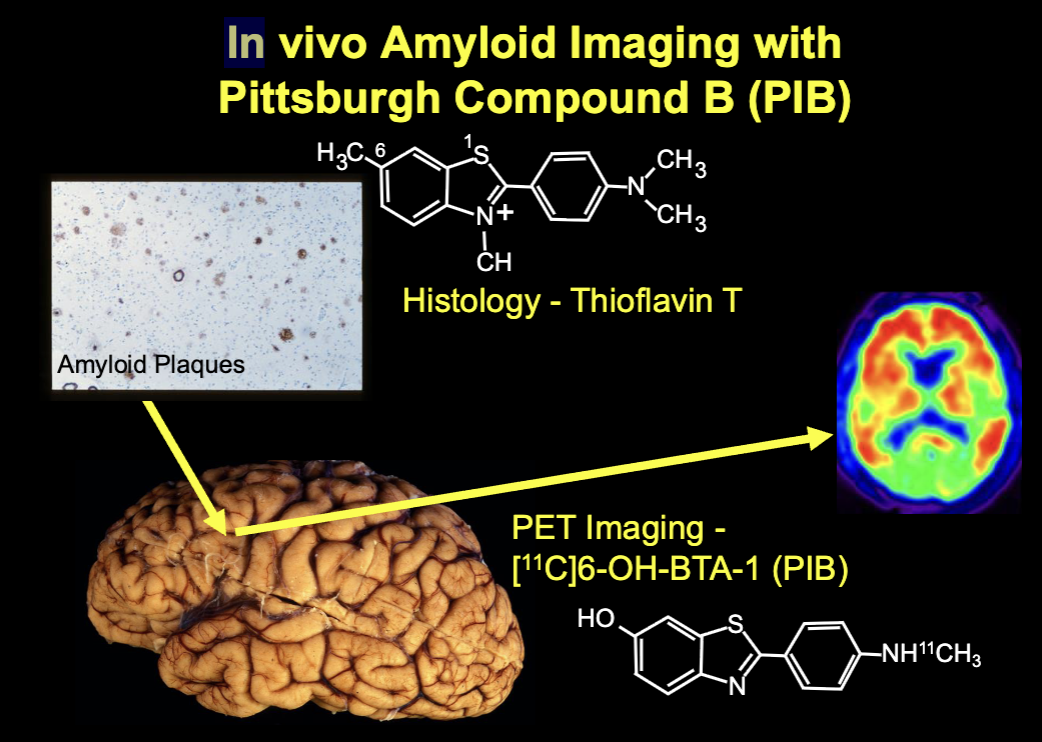
In vivo Amyloid Imaging with Pittsburgh Compound B (PIB)
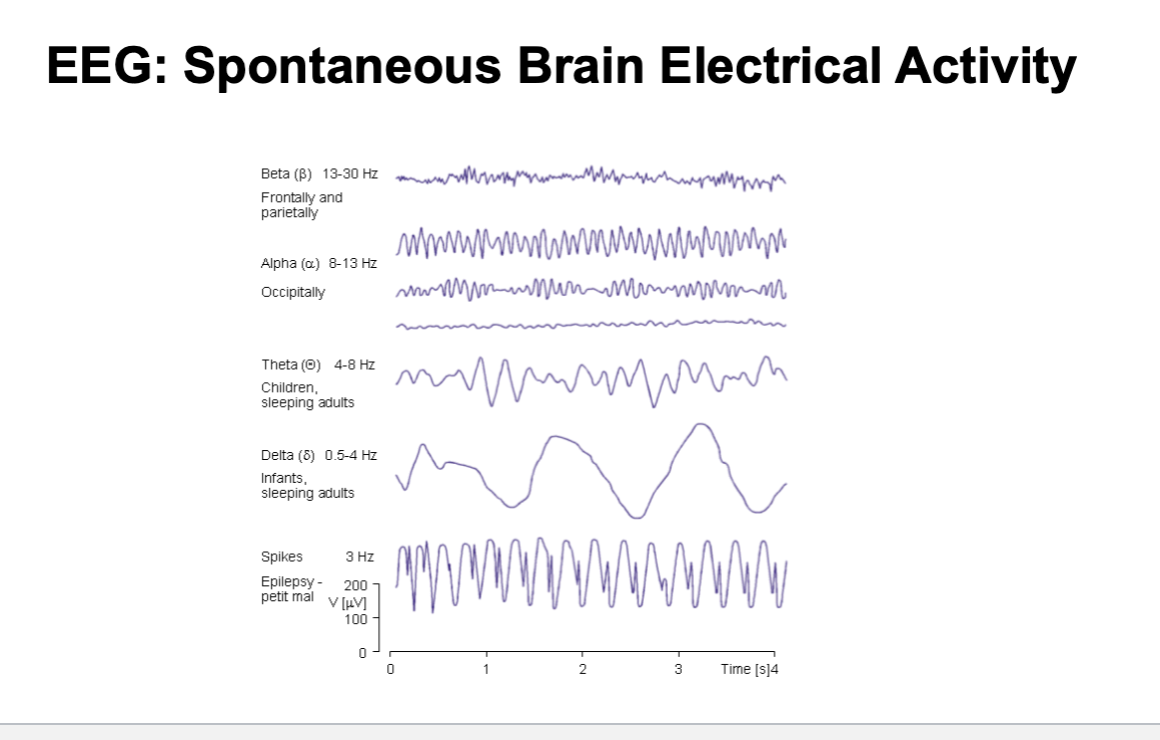
EEG and MEG
EEG Recordings
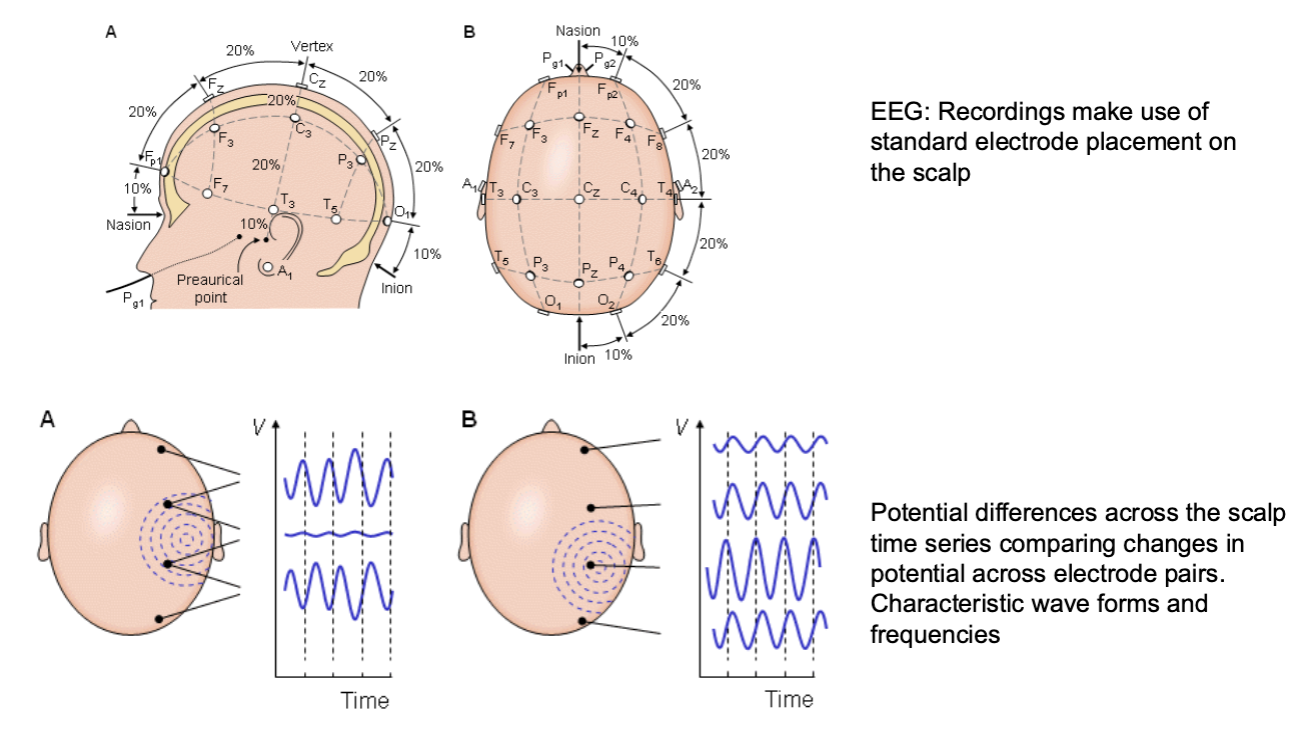
Different Activity on EEG
Postmortem Methods
Neuropsychology
The study of brain-behavior relationships
Development of tools to measure cognitive function, largely using patients with brain lesions: Correlation of lesions with loss of function used to develop tests that tap that function
More recently, studies of normal people using fMRI and other cognitive neuroscience methods to define how the brain performs cognitive tasks
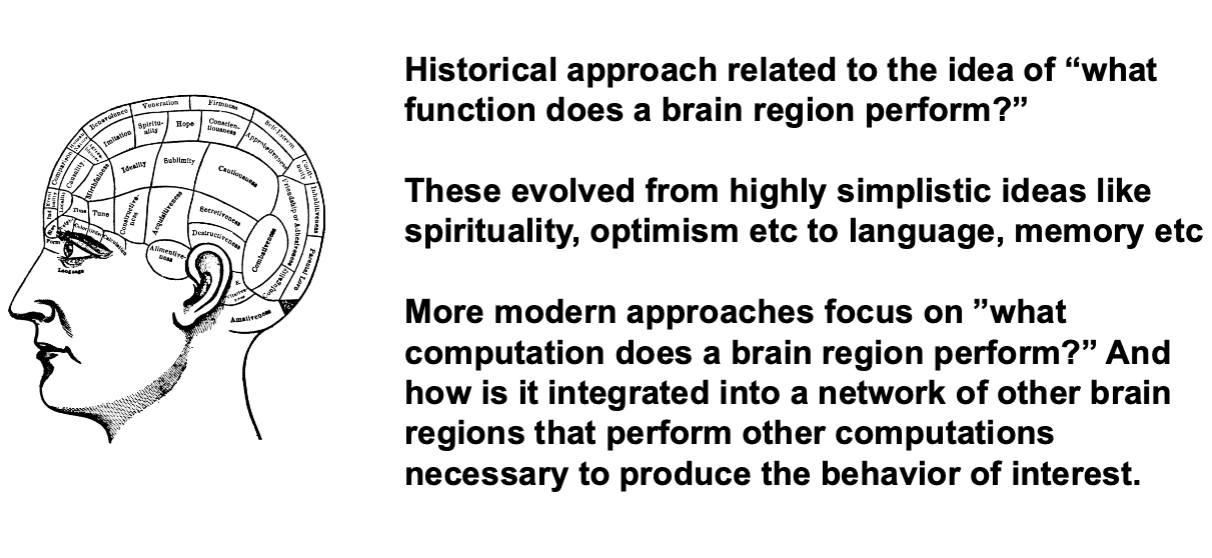
Phrenology and the Evolution of Neuropsychology and Cognitive Neuroscience
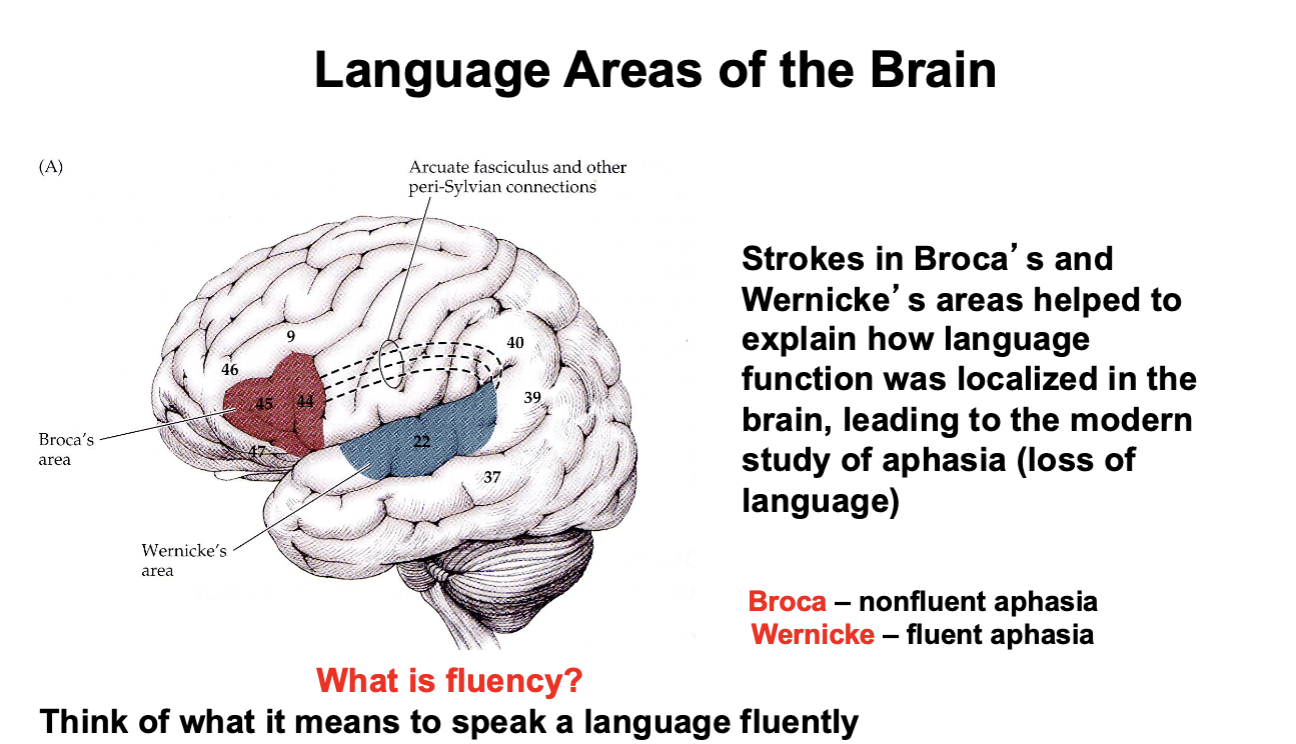
Aphasia
loss of language ability (production, comprehension, auditory, written)
Ataxia
Imbalance, incoordination, unsteadiness
Paresis
weakness (hemiparesis, paraparesis)
Visuospatial dysfunction
disorientation in space, inability to create an internal map of space
Executive function
planning, multi-tasking, judgement
Episodic memory
memory for events
Semantic memory
memory for facts
Working memory
memory over brief time frames for use and manipulation without long term storage
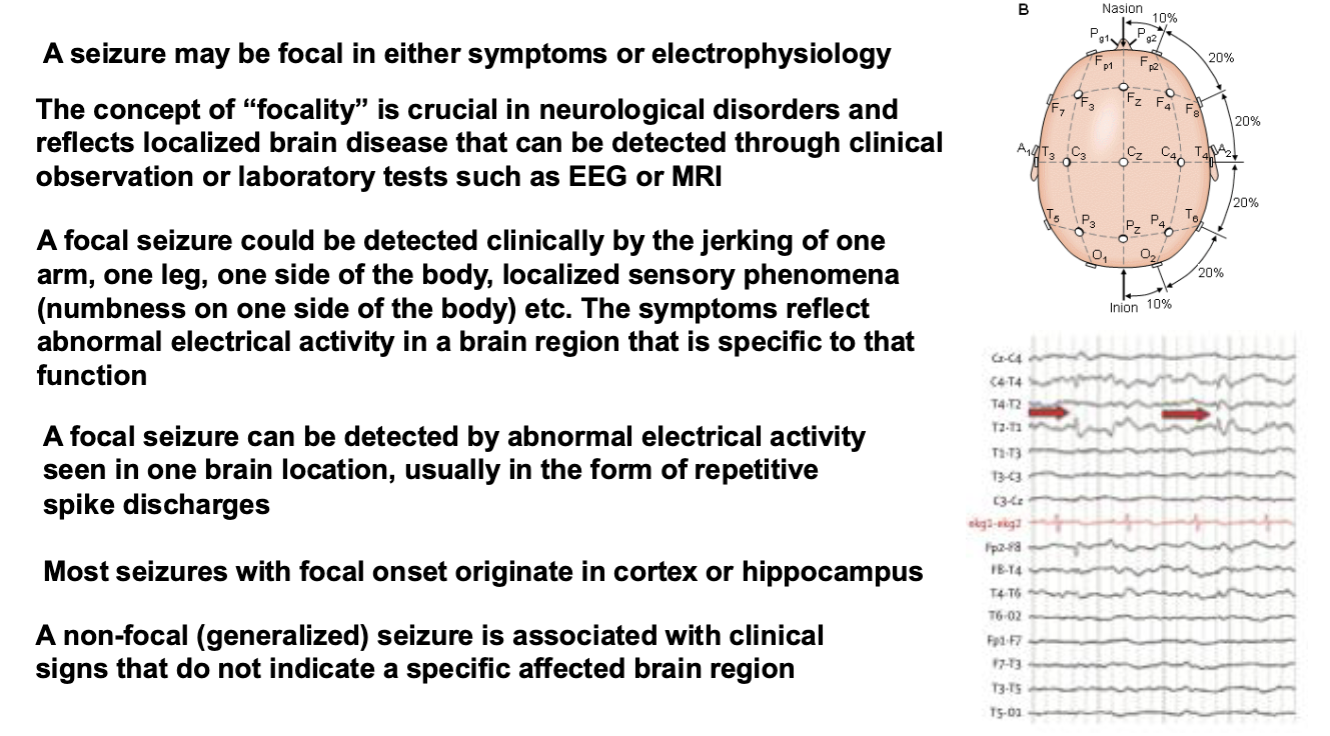
“Focality” In Neurological Disease
Stroke as a Brain Lesion Model
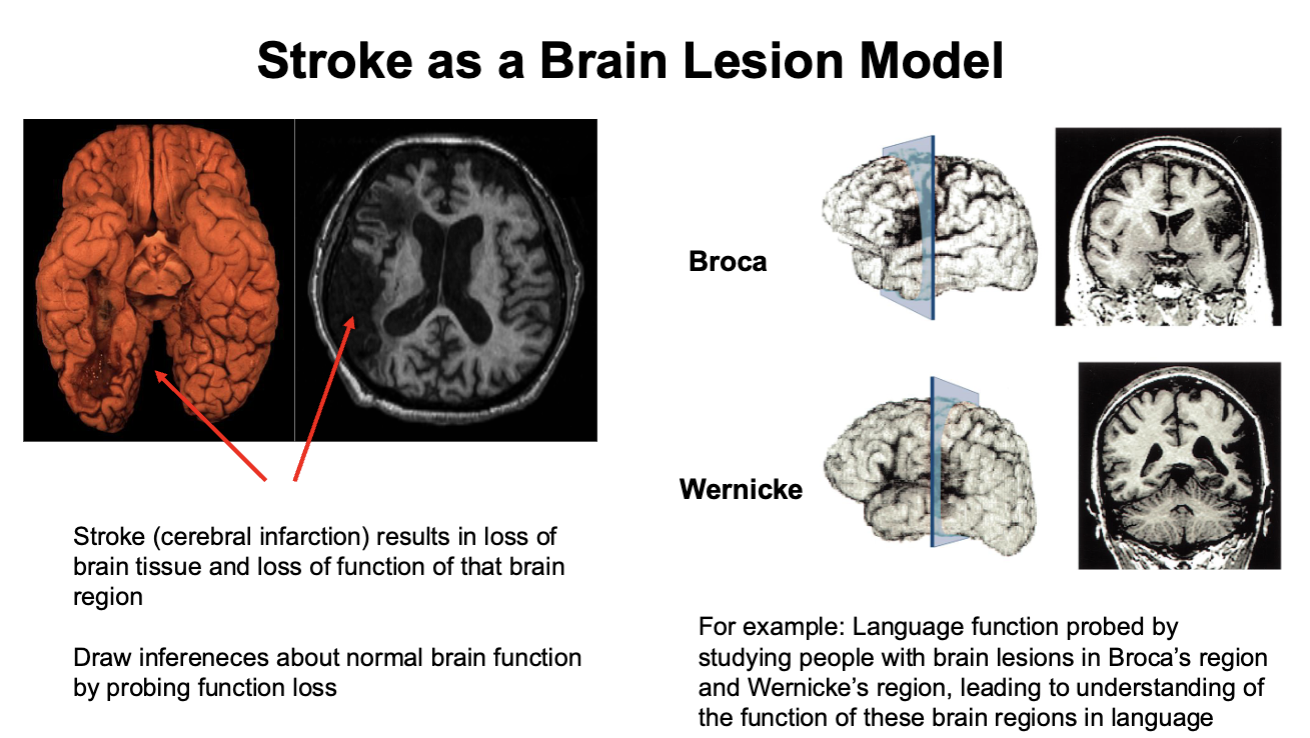
Language Areas of the Brain
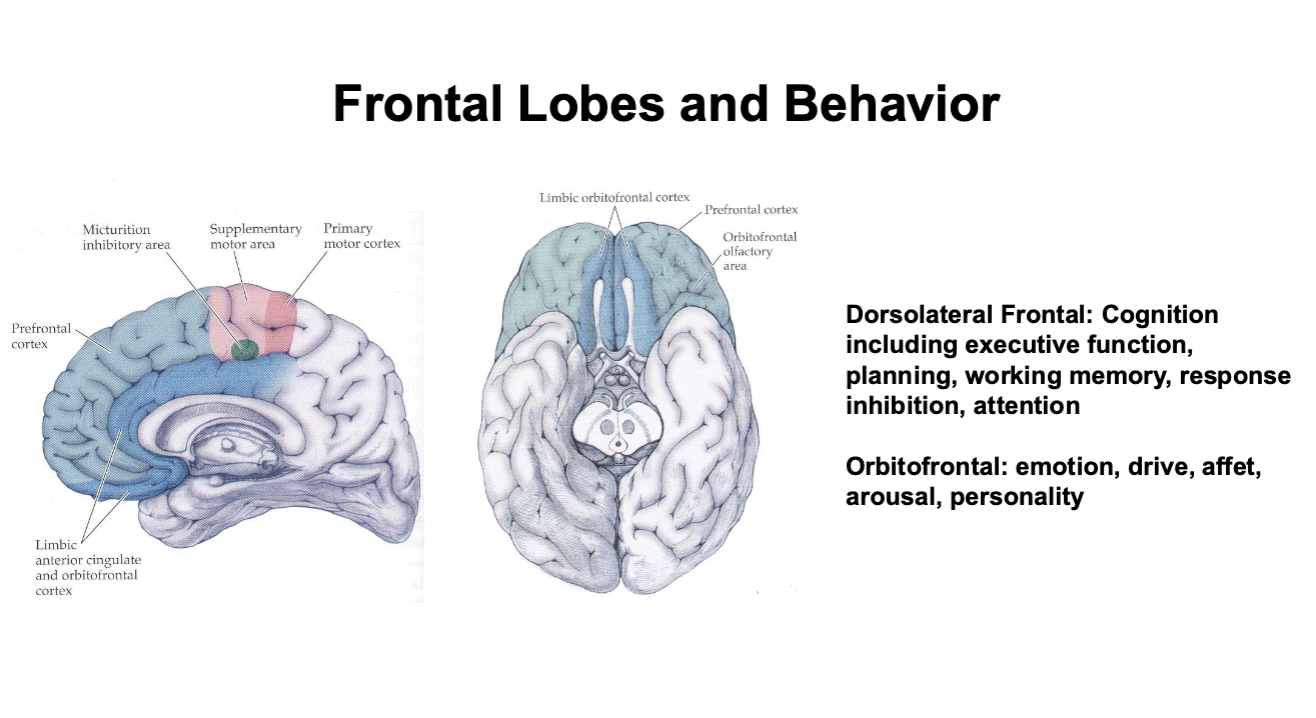
Frontal Lobes and Behavior
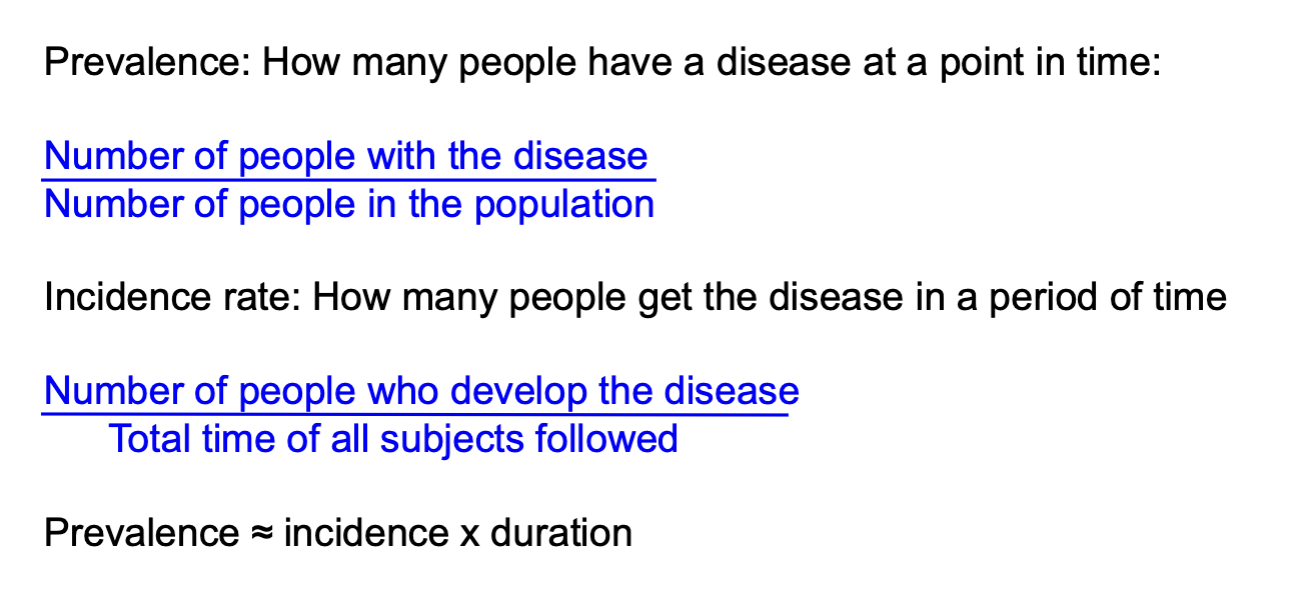
Epidemiology
Prevalence and Incidence Rate
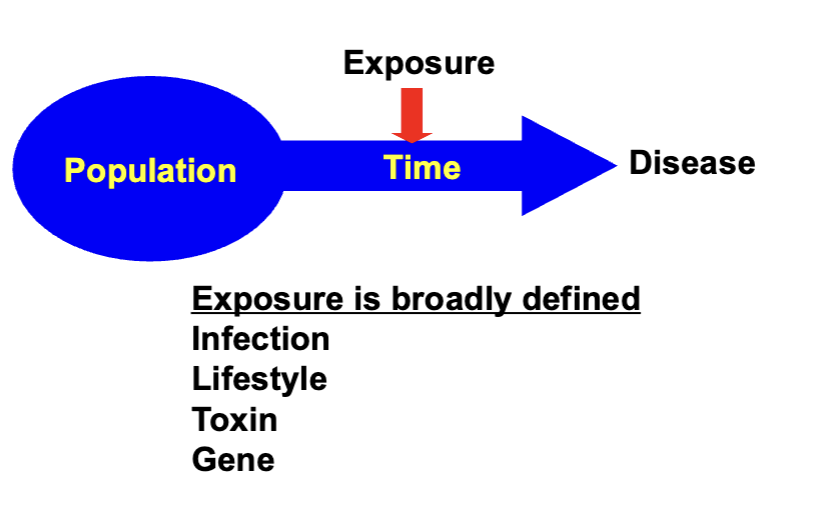
Analytic Epidemiology: Defining Risks for Disease
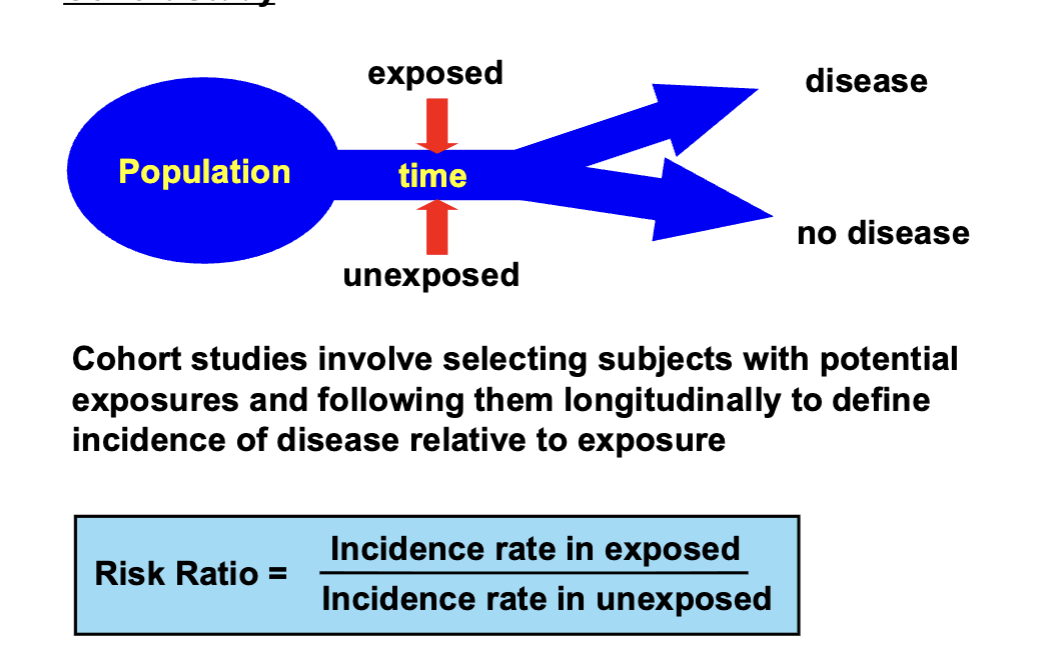
Cohort Study
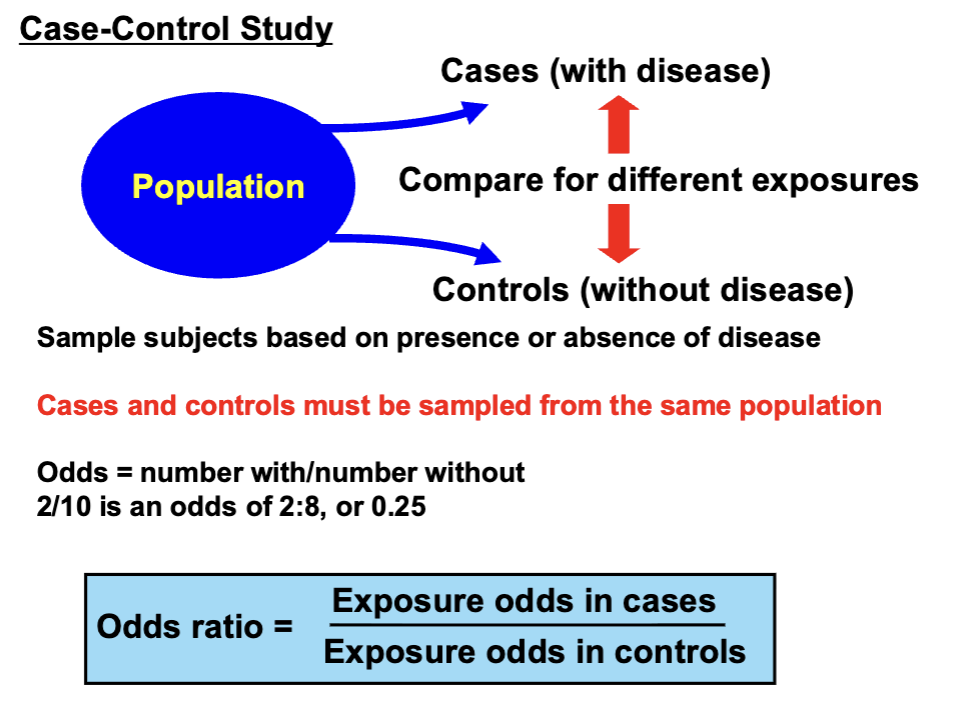
Case-Control Study
Problems with Observational Studies
What is a Biomarker?
Reflects a normal or abnormal biological process
Reflects an exposure or outcome
Objective
Quantitative
May or may not reflect an underlying mechanism
Can be used for diagnosis, monitoring, intervention efficacy, prediction
NOT
A clinical assessment of symptoms or performance
A Biomarker May Reflect an Exposure or Outcome Without Explaining Mechanism
Electrocardiogram and heart attack
Diagnostic but doesn’t tell us anything about how it happened
CSF myelin and MS
MS is a disorder of myelin, but how this happens is unclear simply from detecting it in CSF
Biomarkers as Surrogates
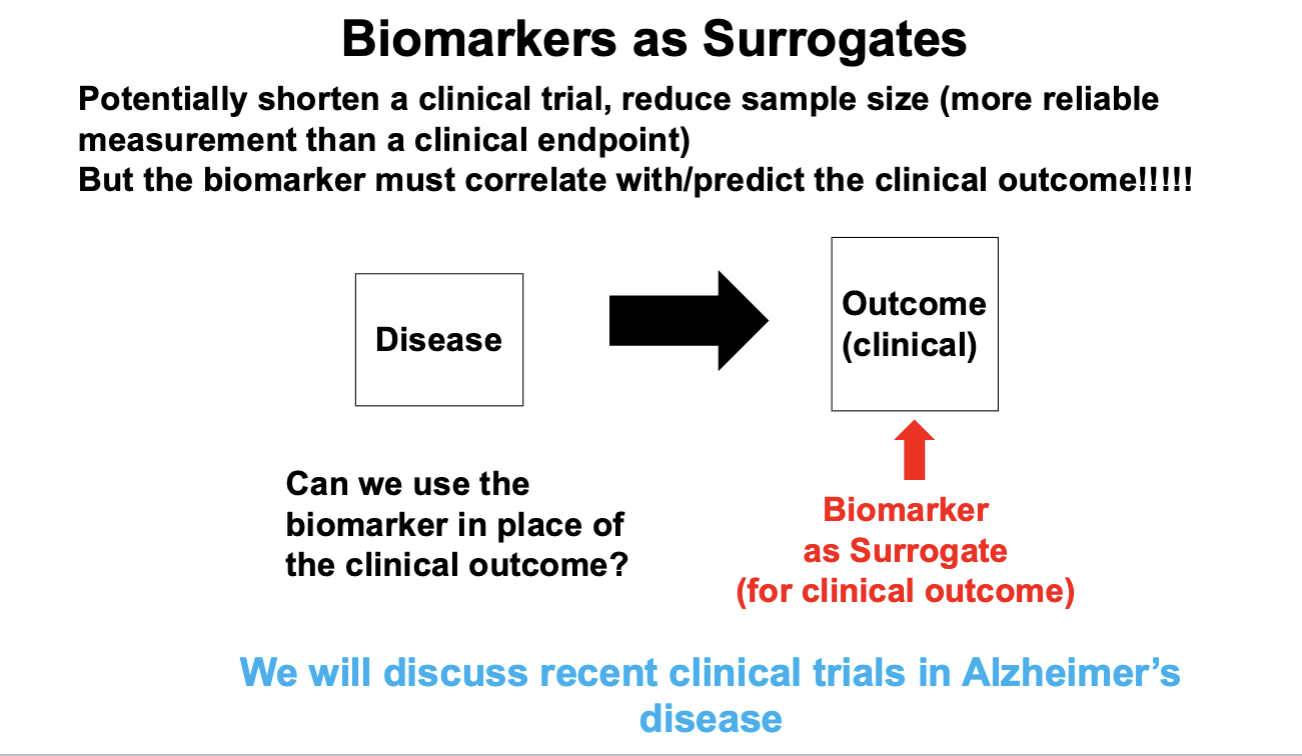
What are common surrogate biomarkers and why are they accepted?
Biomarkers for Brain: Challenges
Can’t get tissue
Blood-brain barrier makes blood measures difficult
CSF requires lumbar puncture
Imaging is technically complicated and expensive
EEG can be technically complicated and expensive and non-specific
Biomarker Discovery
Advantages of Biomarkers
Simpler than a clinical evaluation by an expert (usually)
Permit testing/screening of large samples
Predict outcomes
Develop therapeutics faster
Personalized medicine
Limitations of Biomarkers
Must be validated with a ”gold standard”
Not always present
Standardization may be difficult
Expensive
Can be non-specific
Need replication in diverse samples
Poor Validation is Common
Selection of extreme or highly typical cases
Samples don’t reflect who actually gets the disease – lack of diversity
Statistical differences may have no clinical meaning
Subject to bias
Incorporation bias - test is used to make the diagnosis (circularity)
Progression bias (gold standard at a different timepoint)
Verification bias (not all subjects get the gold standard)
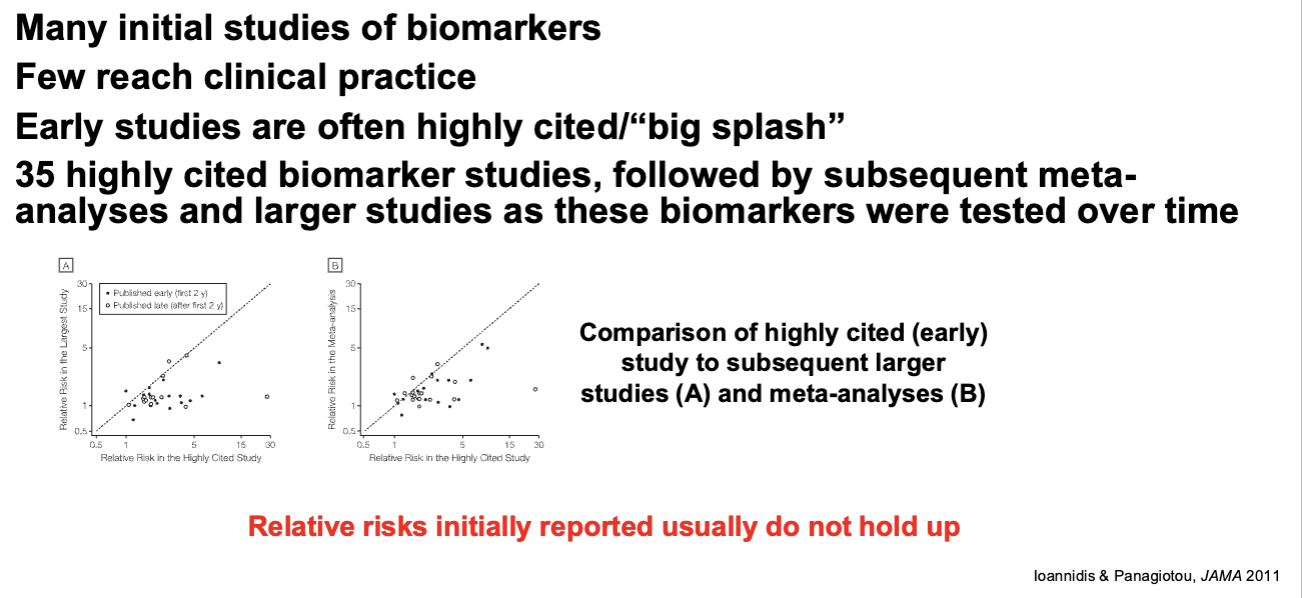
Initial biomarker reports are always more optimistic than later ones
Wrong “gold standard”
Early Measures of Biomarker Success are Rarely Confirmed
Neurological Diseases
Most neurological diseases are complex
May have a single phenotype – i.e., a syndrome
Caused by multiple mechanisms
A “cure” for most neurological diseases is simplistic: there maybe multiple cures because of multiple etiologies
In some cases, a “final common pathway” could exist that may be treatable despite multiple etiologies
Diagnoses of neurological disease has evolved from clinical phenomenology to laboratory and biomarker-based
Seizures
Seizure: a transient event caused by abnormal excessive or synchronous neuronal activity in the brain
Seizures often (but not invariably) occur in conjunction with a precipitating event leading to temporary or permanent brain injury
Seizures may not recur
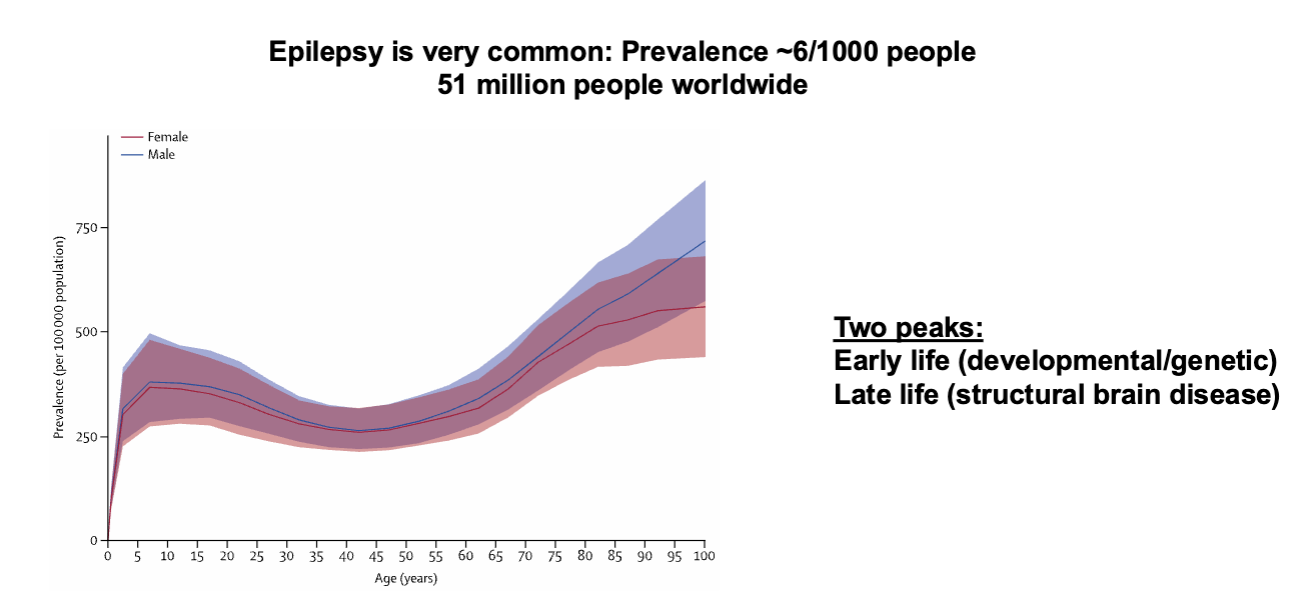
Epilepsy
Epilepsy: Chronic, long term predisposition to repeated seizures
Epilepsy can follow from a single seizure if the problem persists after the resolution of the acute brain injury
Seizure Classification
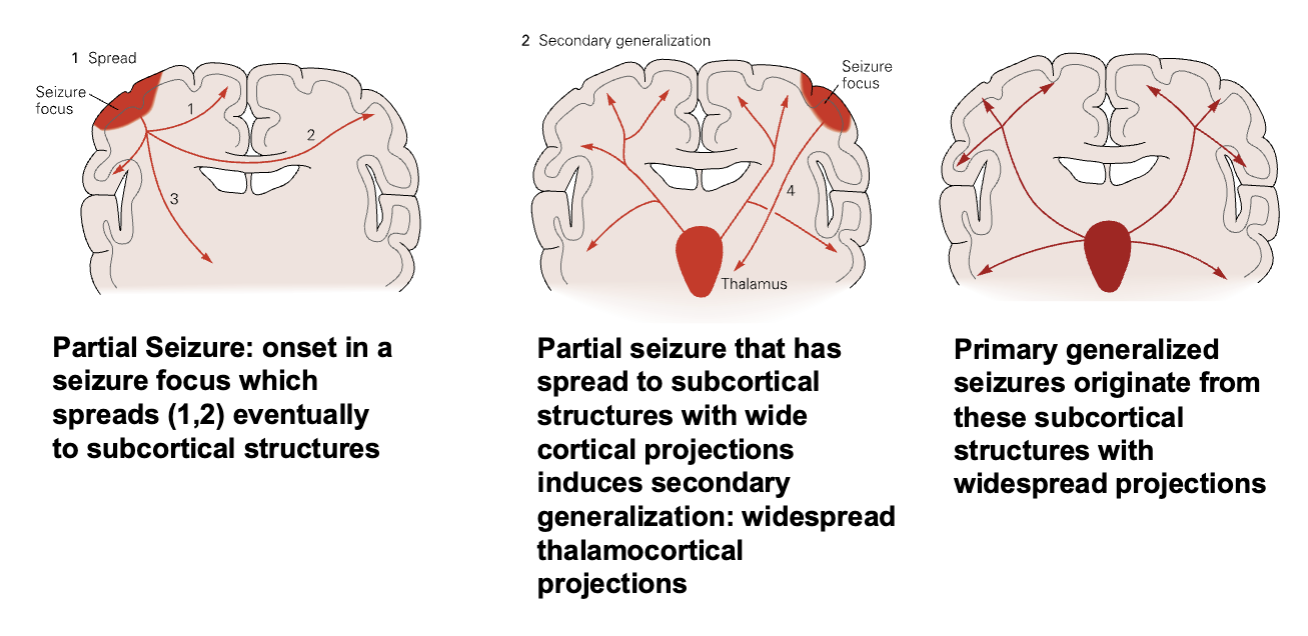
Seizure onset
Focal (also called “partial”)
Generalized
Focal followed by generalization
Level of awareness (of the patient)
Aware (also called “simple”)
Unaware (also called “complex”)
The seizure phenomena may be motor (tonic/clonic), sensory (tingling, flashes of light, sounds), cognitive (altered state or level of consciousness)
Seizure Types
Focal Seizures
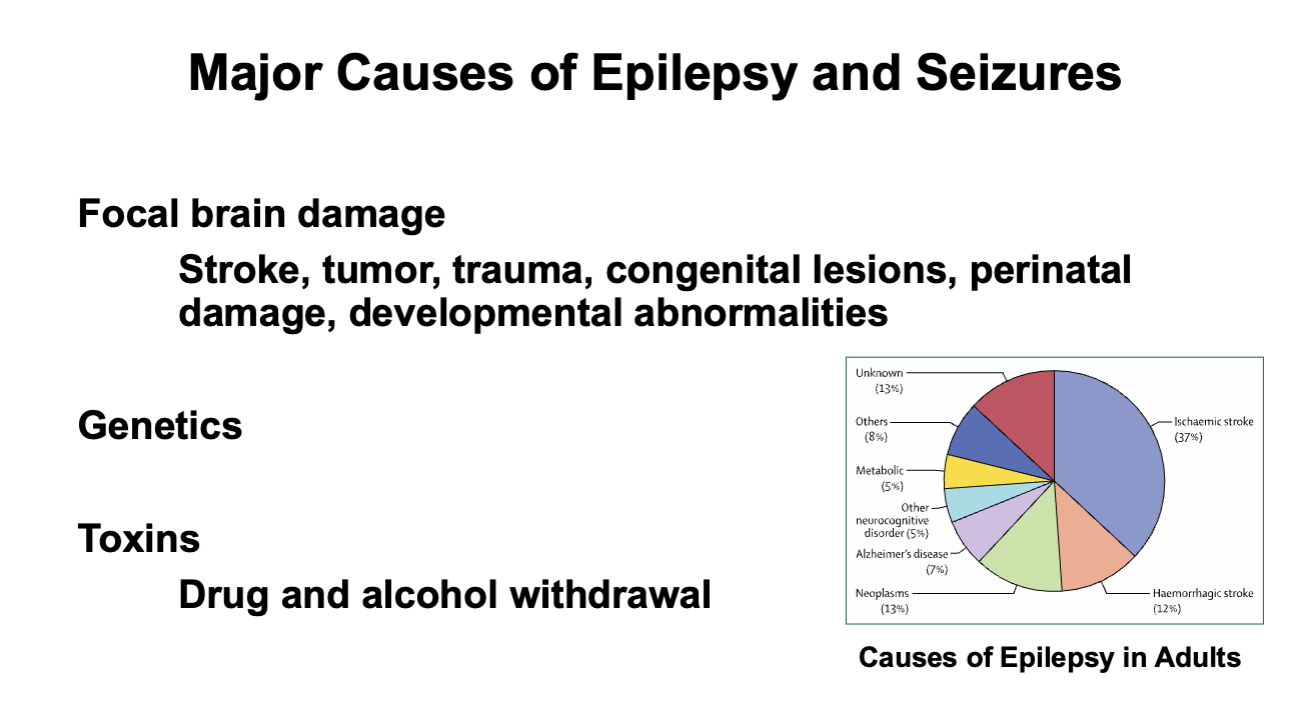
Major Causes of Epilespy and Seizures
Epilepsy Prevalence by Age
Electrophysiology
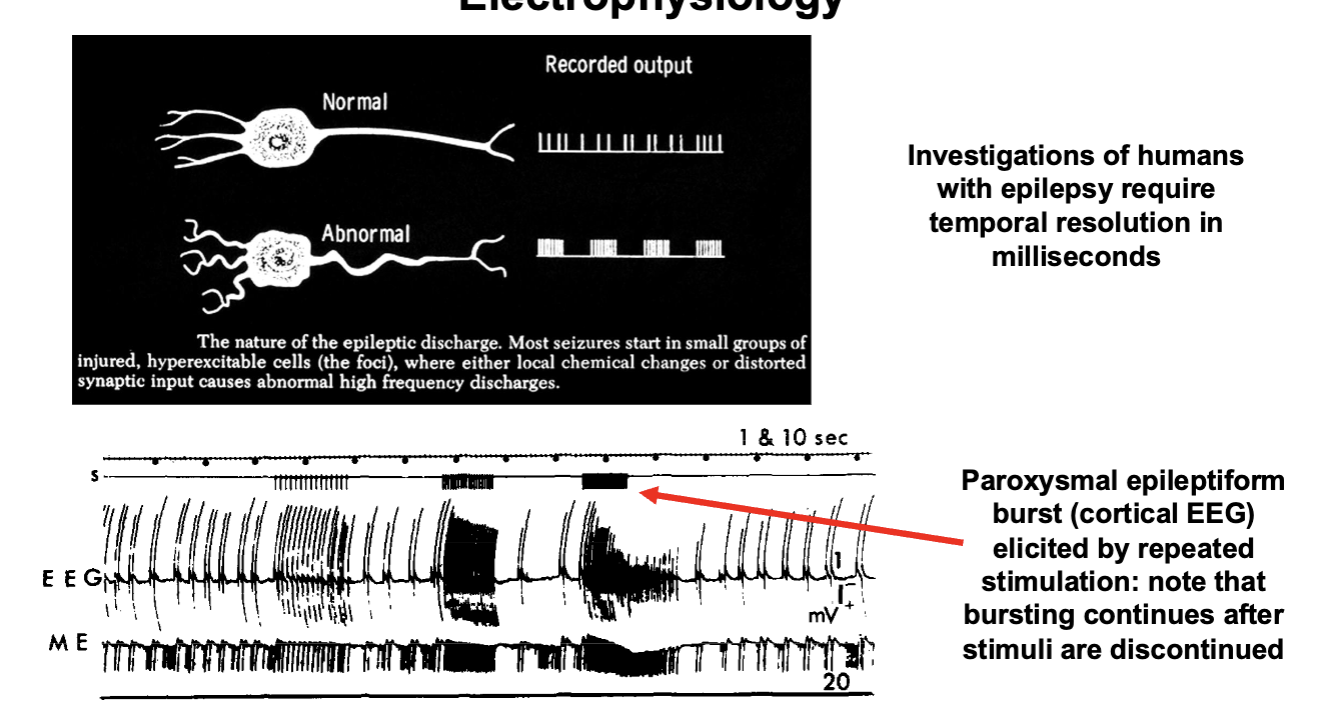
How Does Epilepsy Occur?
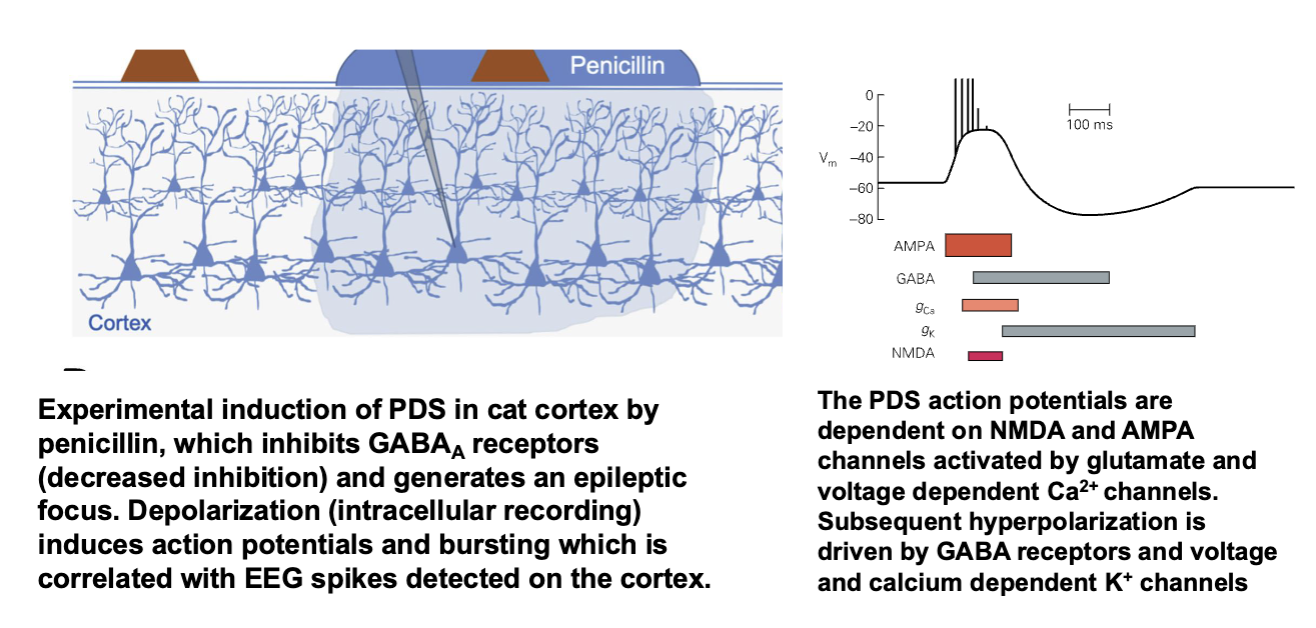
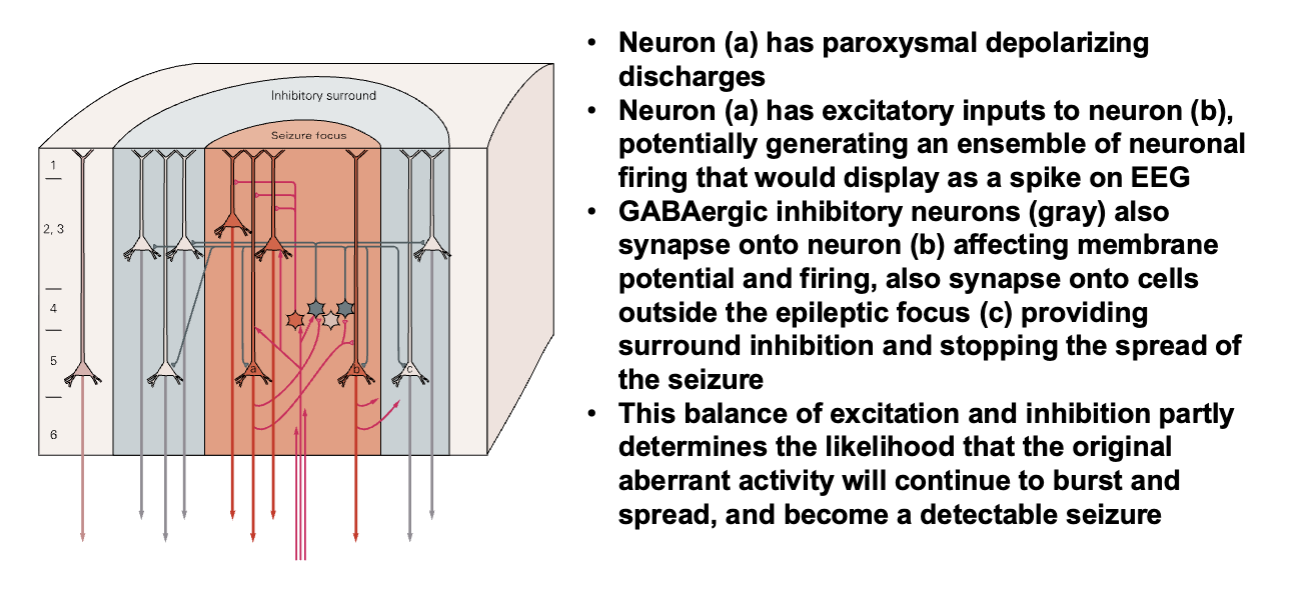
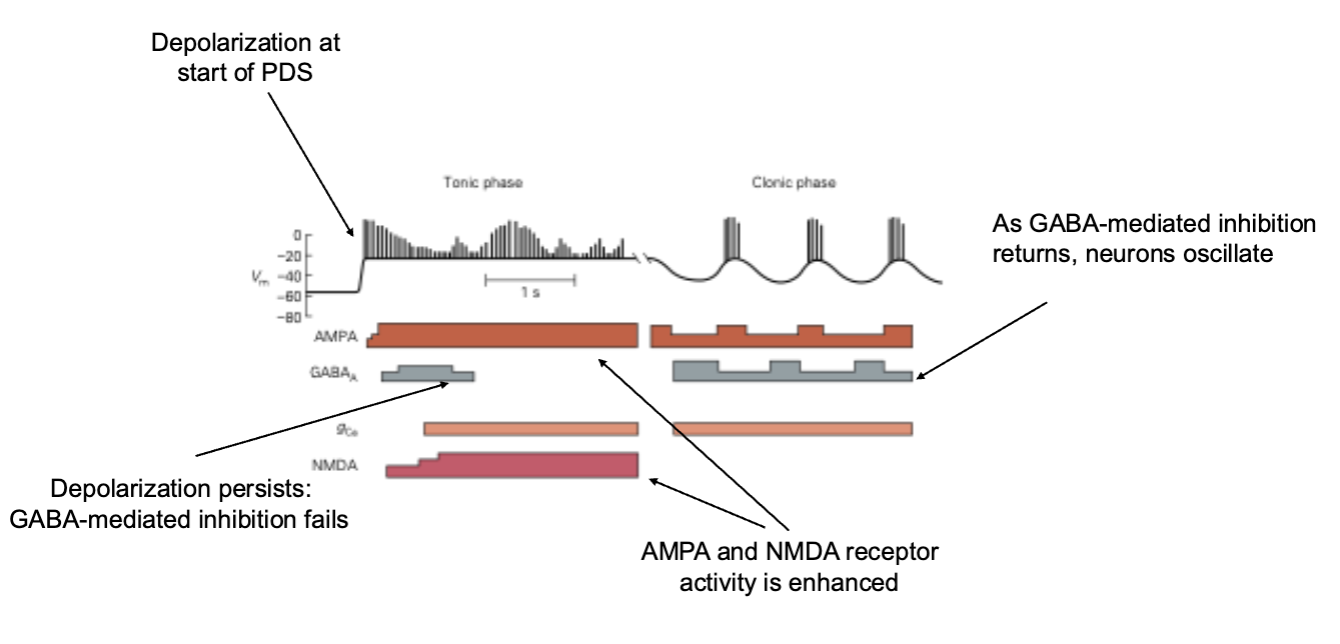
Paroxysmal Depolarizing Shift
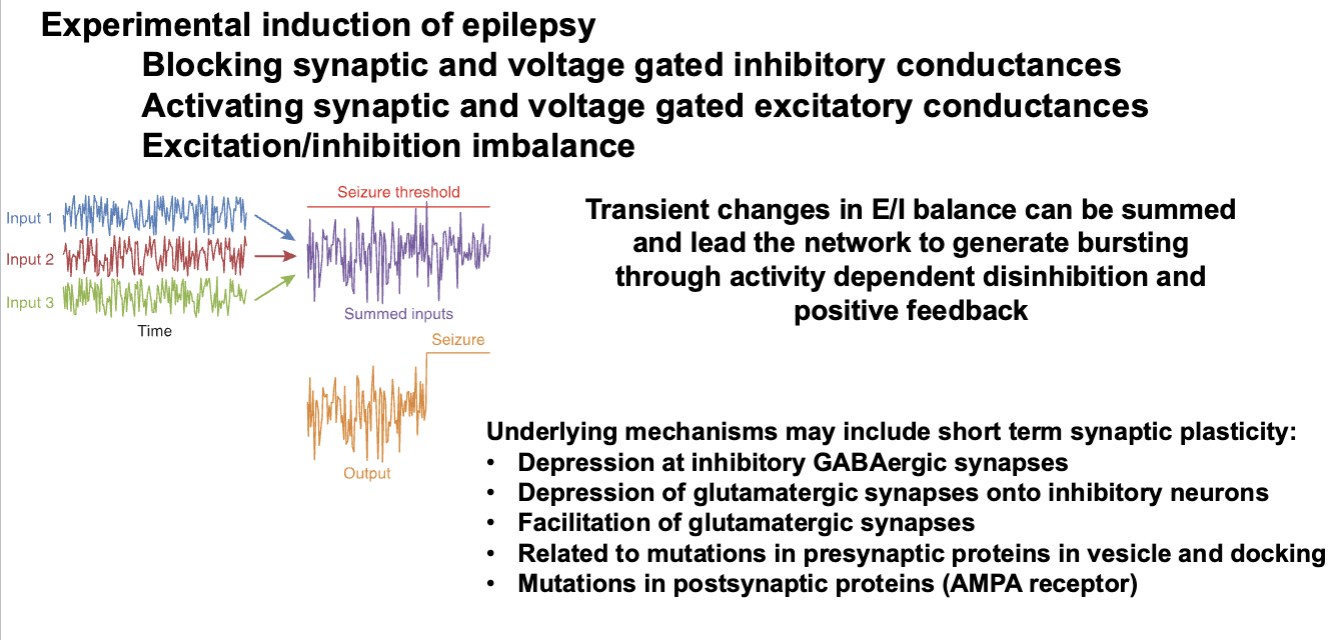
Excitation and Inhibition in a Seizure Focus
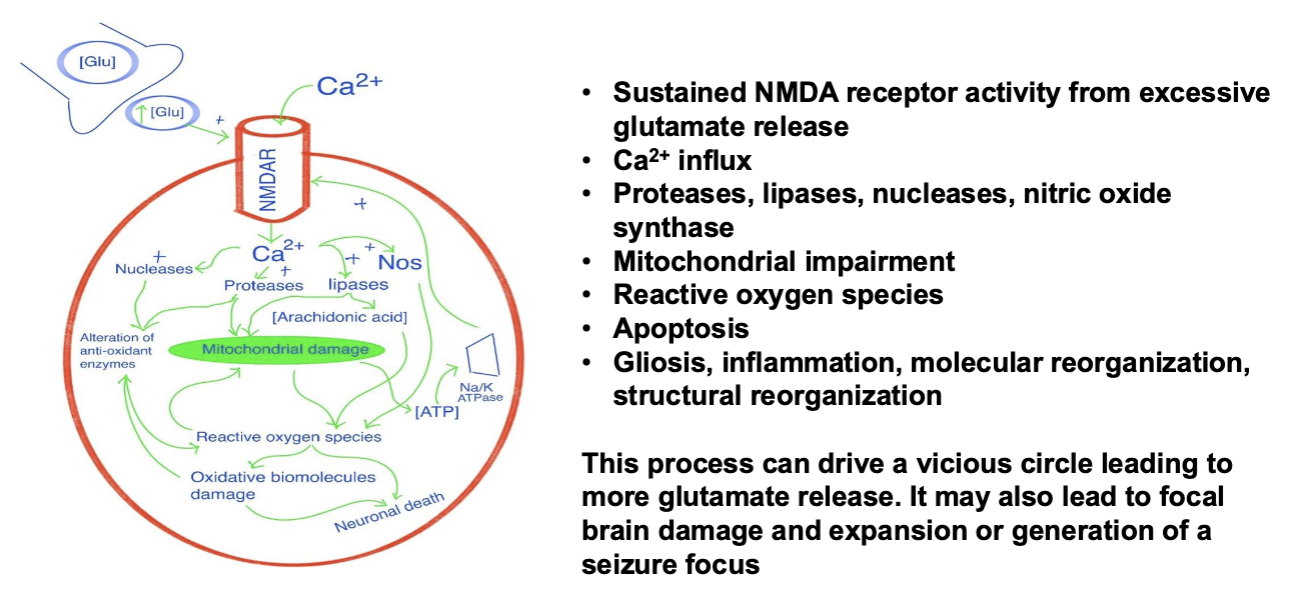
Excitotoxicity
Genetics of Epilepsy
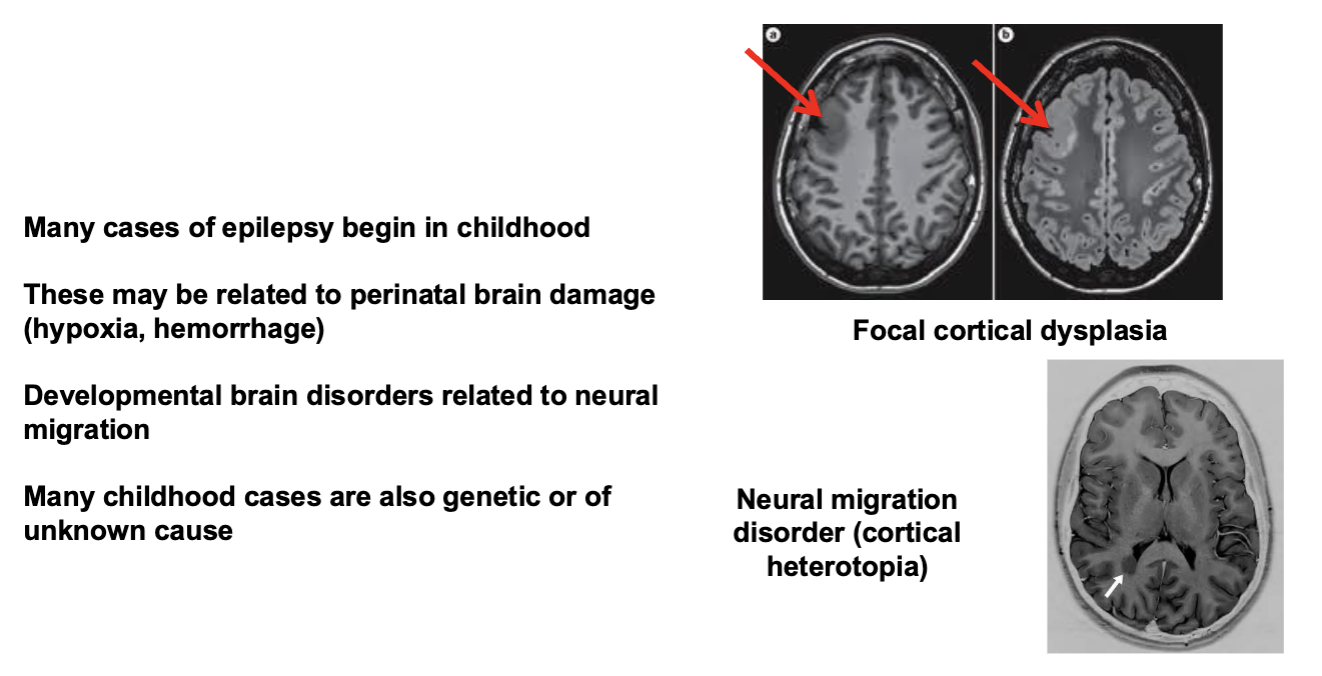
Brain Development and Epilepsy
Tonic-Clonic Seizures
Childhood Absence Epilepsy
3 Hz spike/wave synchronous discharges
Complex Partial Seizures
Seizue focus in the temporal lobe
Anti-Epileptic Drugs
Medications are usually effective and are the first line treatment
Many drugs are more effective in focal onset seizures, others generalized seizures, other in both
Side effects are common and can include fatigue/drowsiness, changes in mood, mental slowing
Some patients require multiple drugs and in some patients drug therapy does not provide acceptable relief
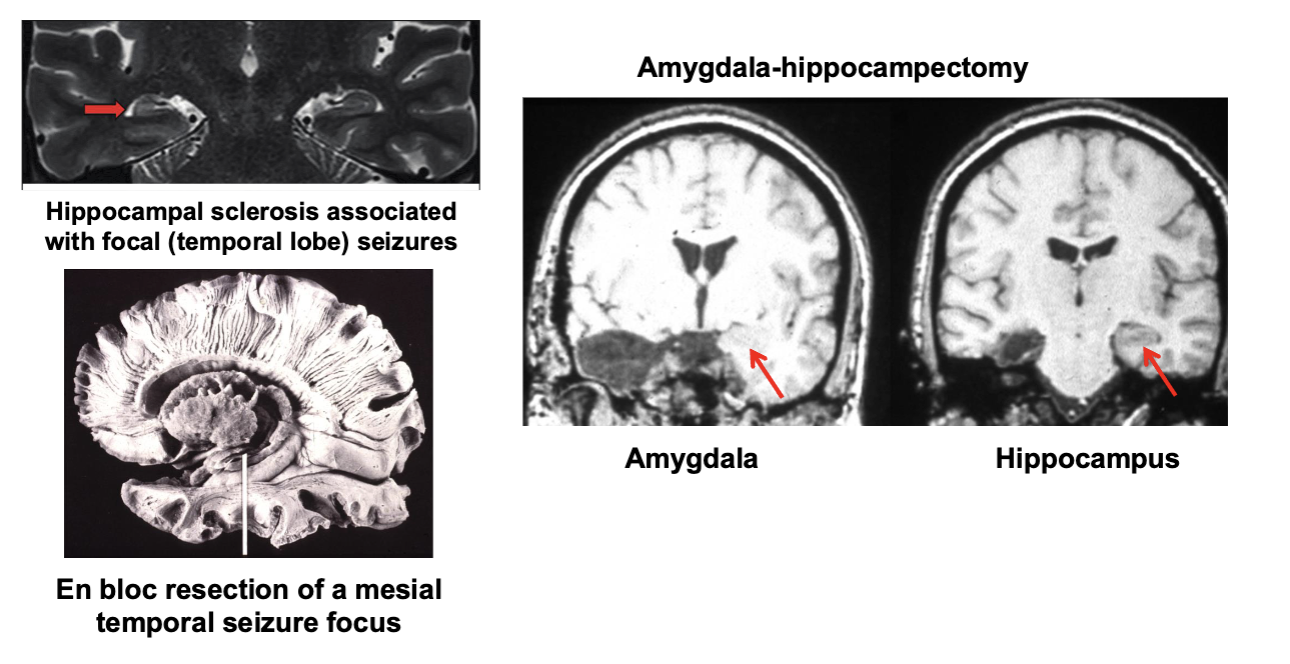
Surgical Treatment
May be useful in medically refractory cases
Requires a seizure focus – the point of the surgery is to remove (resect) the focus
Evaluation performed to clearly identify a focus and be sure that it is safe to remove it
After surgery there is usually a reduction in seizure rates and greater likelihood of control with medication
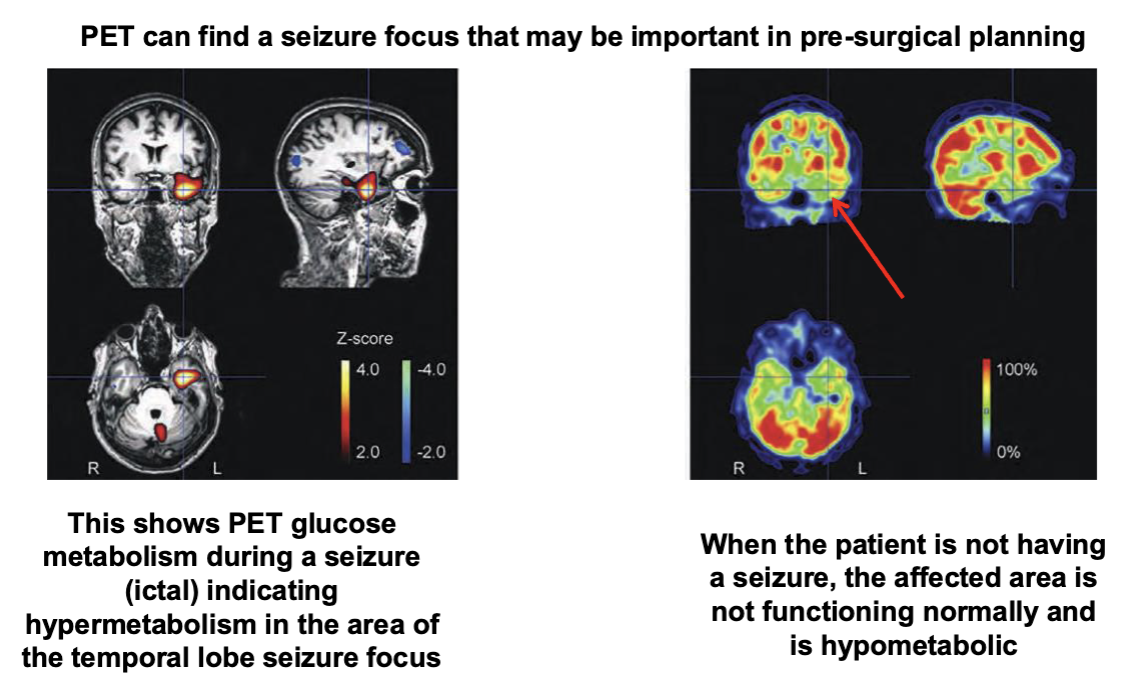
PET and Epilepsy
Surgery for Temporal Seizure Foci
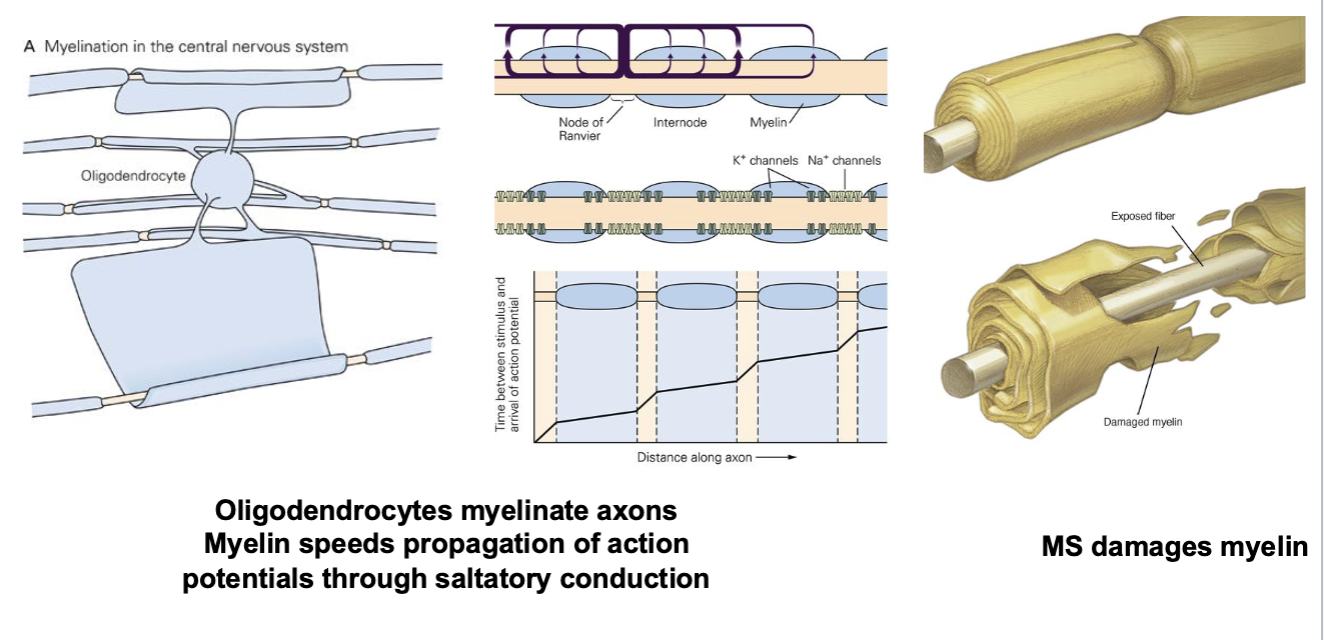
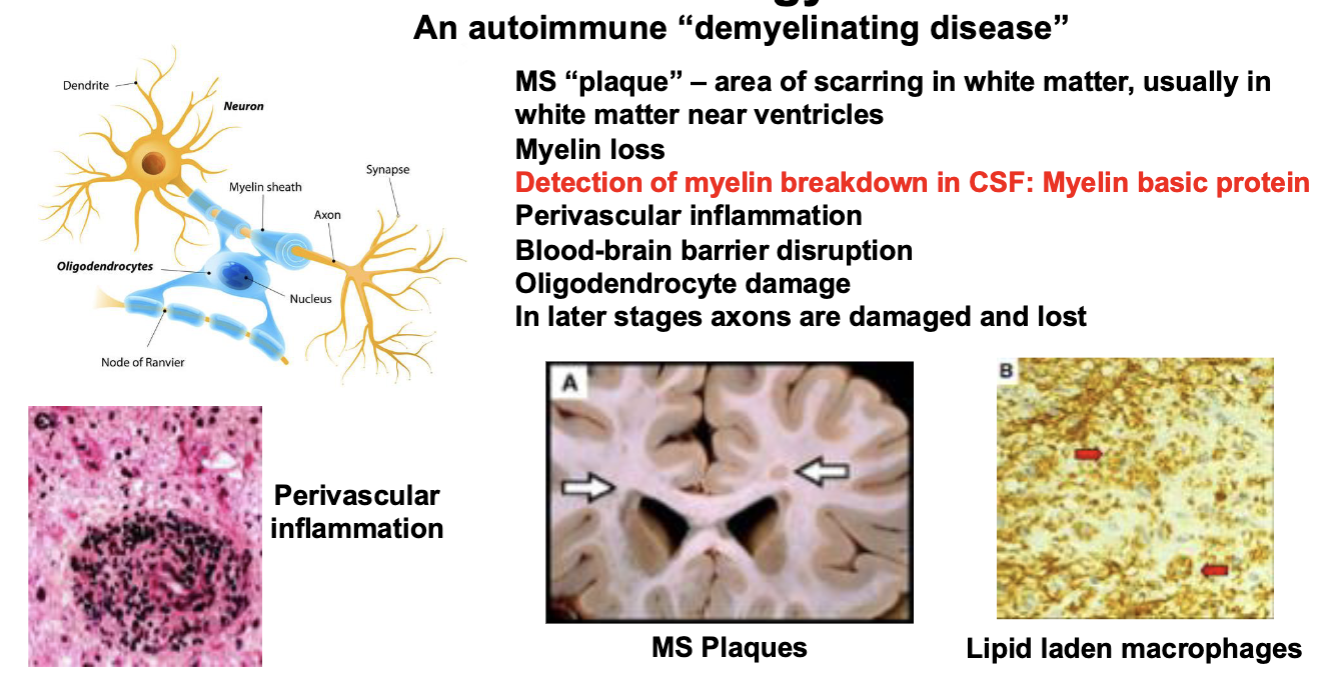
What is Multiple Sclerosis (MS)?
An “autoimmune” disease in which the individual’s immune system is directed against the CNS particularly against myelin
The neuropathology of MS involves inflammation that particularly affects white matter (myelin) as well as neurons and glia, particularly oligodendroglia
MS produces a variety of symptoms that reflect the location and severity of the damage. The symptoms are often focal reflecting a specific CNS location
There are different types of MS based on genetics, clinical profile, and treatment response
Clinical Features of MS
Subacute onset (days) of neurological symptoms
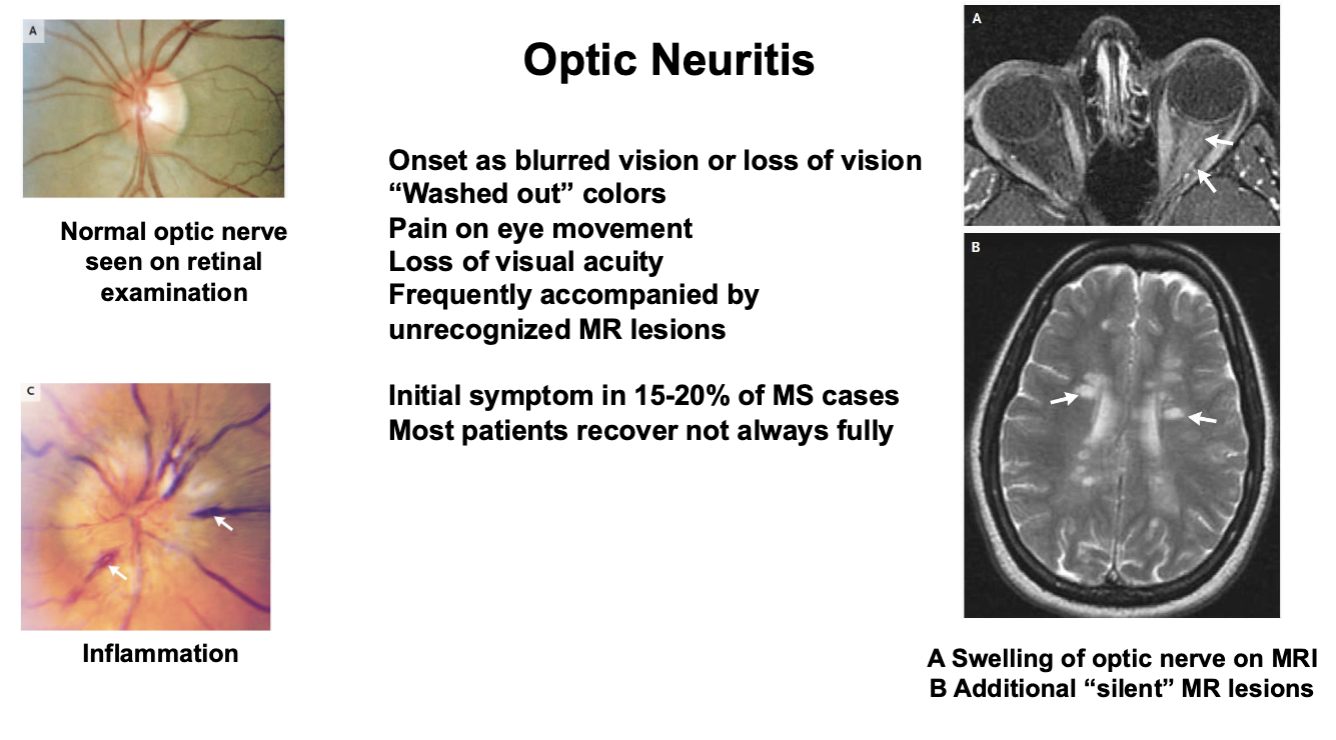
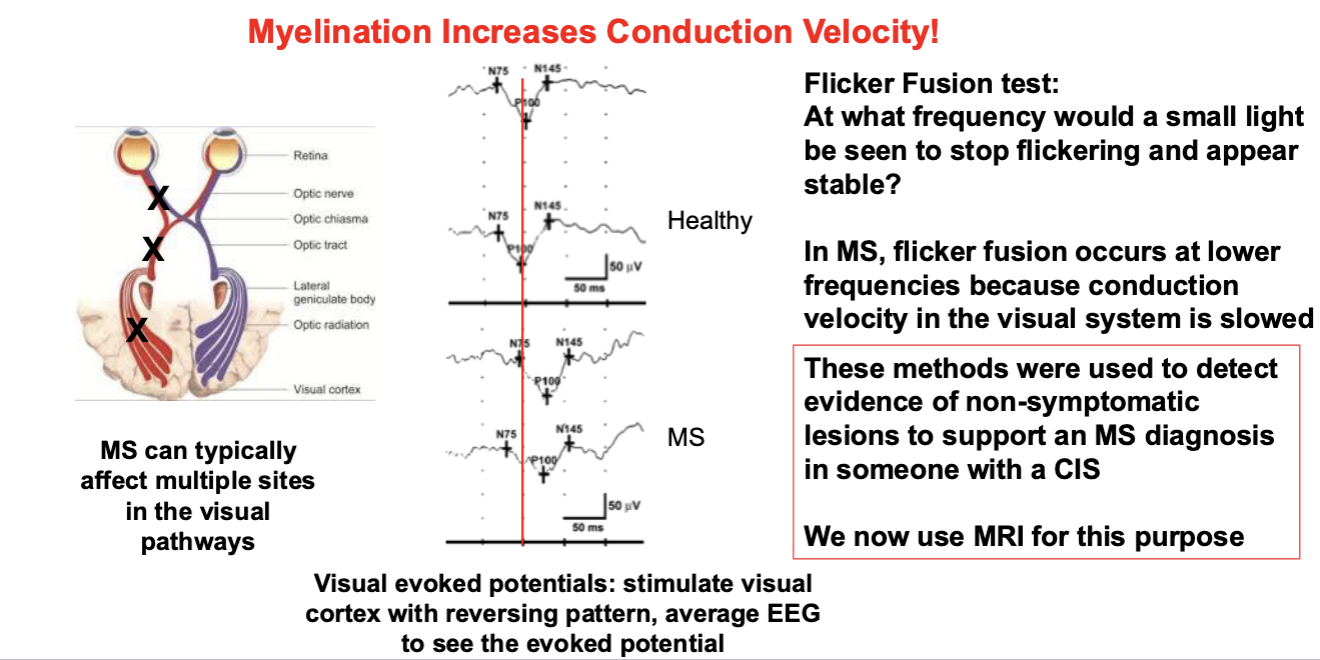
Vision loss (optic neuritis)
Double vision
Sensory loss following neurological distribution
Asymmetric limb weakness
Ataxia/incoordination
Fatigue
Evidence of multiple lesions
Disseminated in space (different parts of the CNS) and time
Clinically isolated syndrome (CIS)
Single episode of a neurological syndrome most commonly optic neuritis
Myelin
MS Pathology
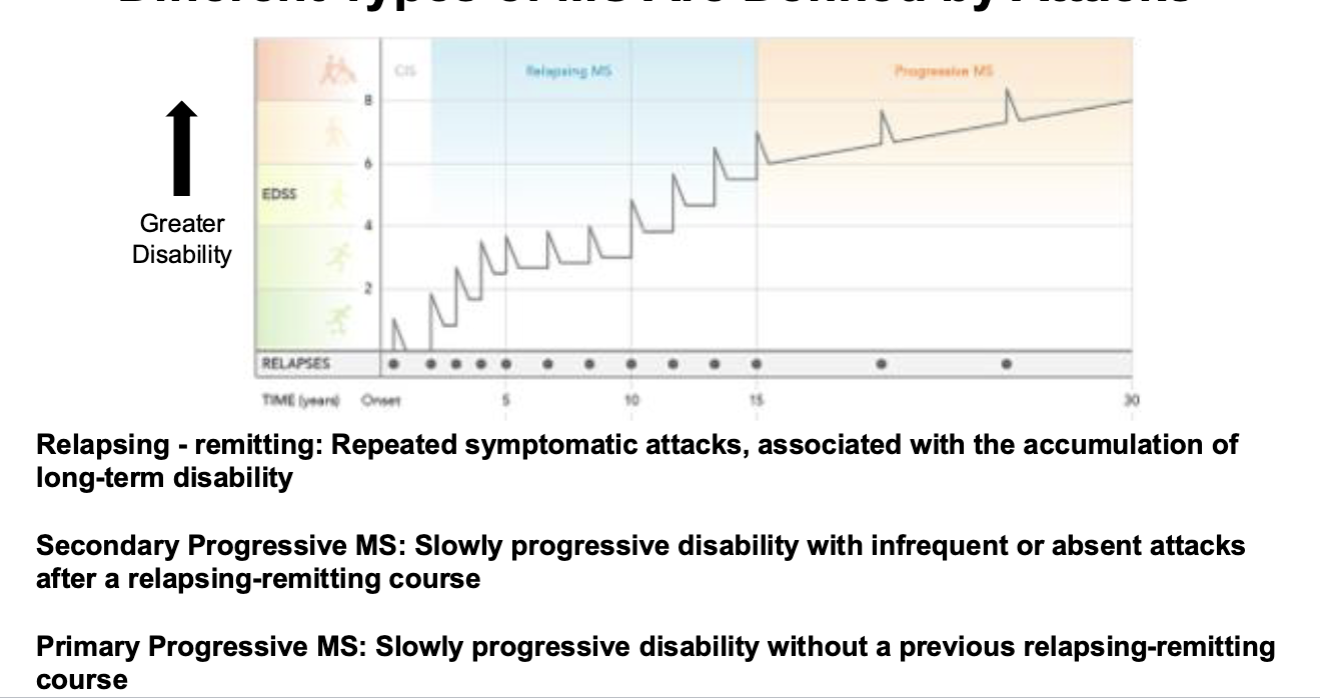
MS Types
Relapsing-remitting
Most common
Attacks may be followed by complete recovery
Secondary progressive
Before the availability of disease modifying therapy, most patients developed this after relapsing-remitting
Primary progressive
Difficult to diagnose
Less common
Fewer brain lesions, more common in spine
Different Types of MS Are Defined by Attacks
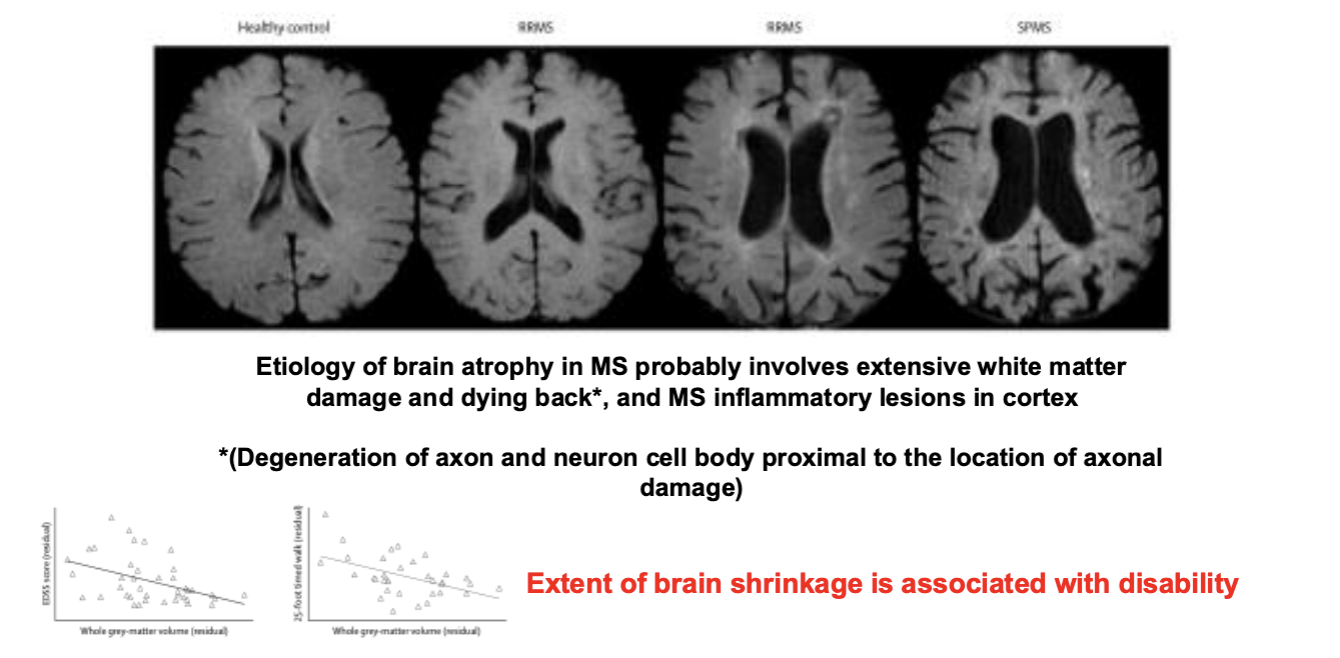
MS is Also Associated with Brain Atrophy
Optic Neuritis
MS Diagnosis pre-MRI Relied on Principles of Neuroscience
Diagnosis of MS
Characteristic clinical presentation
Disseminated lesions in space and time
MRI evidence of white matter lesions
CSF measurement of myelin destruction (myelin basic protein), inflammatory proteins, and cellular evidence of inflammation (lymphocytes)
MS Epidemiology
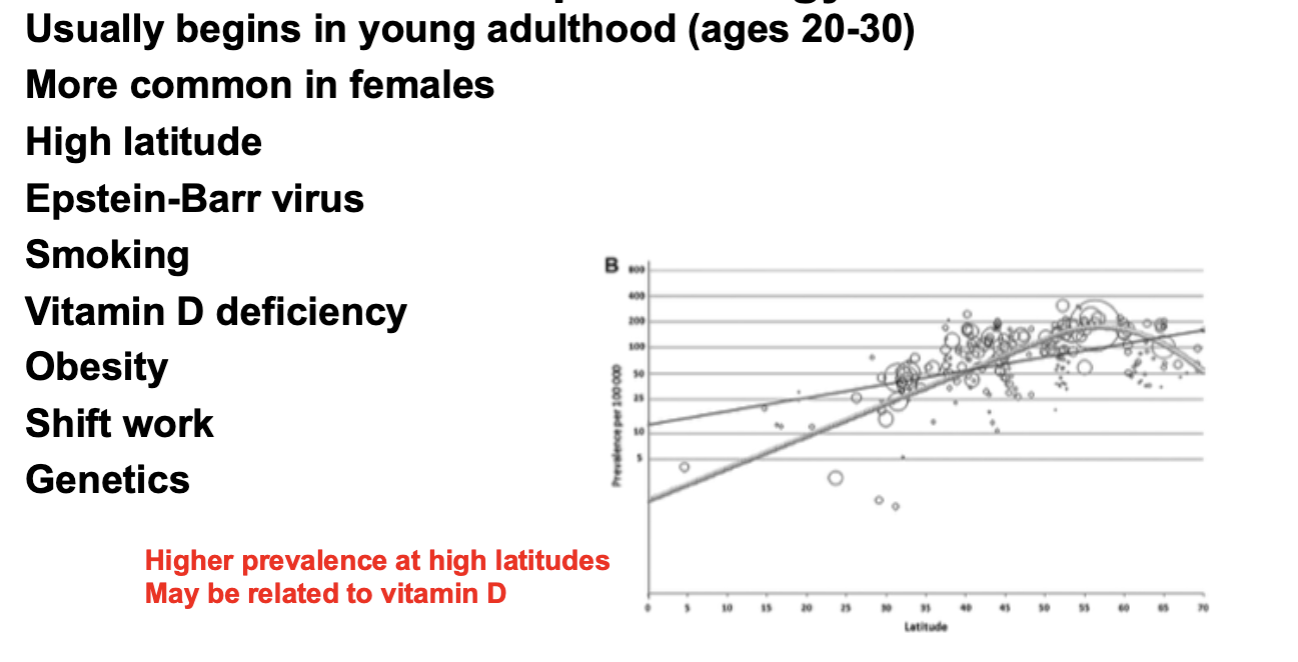
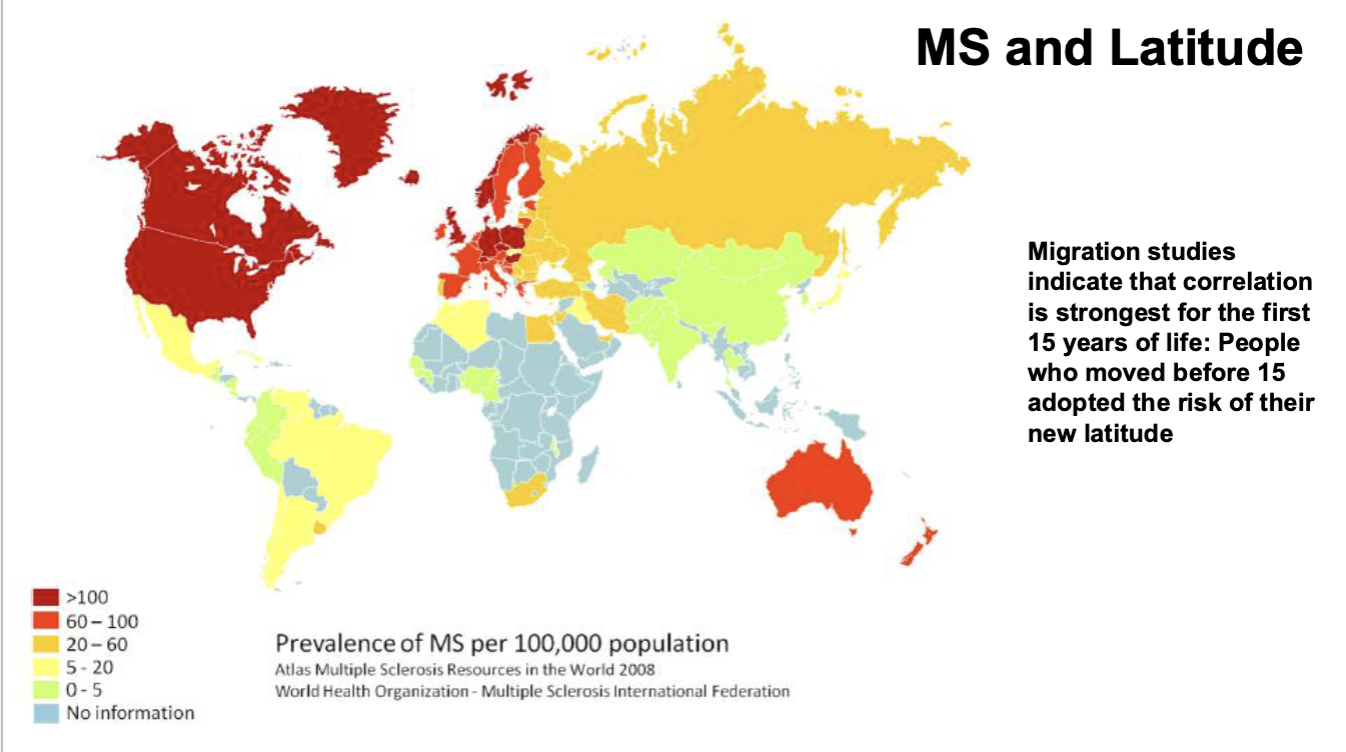
MS and Latitude
Genetics and MS
Over 200 different genetic polymorphisms have been associated with MS in large GWAS series
These genes generally have very small effects (odds ratios of ~1.2): they probably work in combination
Many of the loci appear to regulate expression of genes associated with immune function
Discordance is often seen in monozygotic twins, suggesting a strong environmental factor
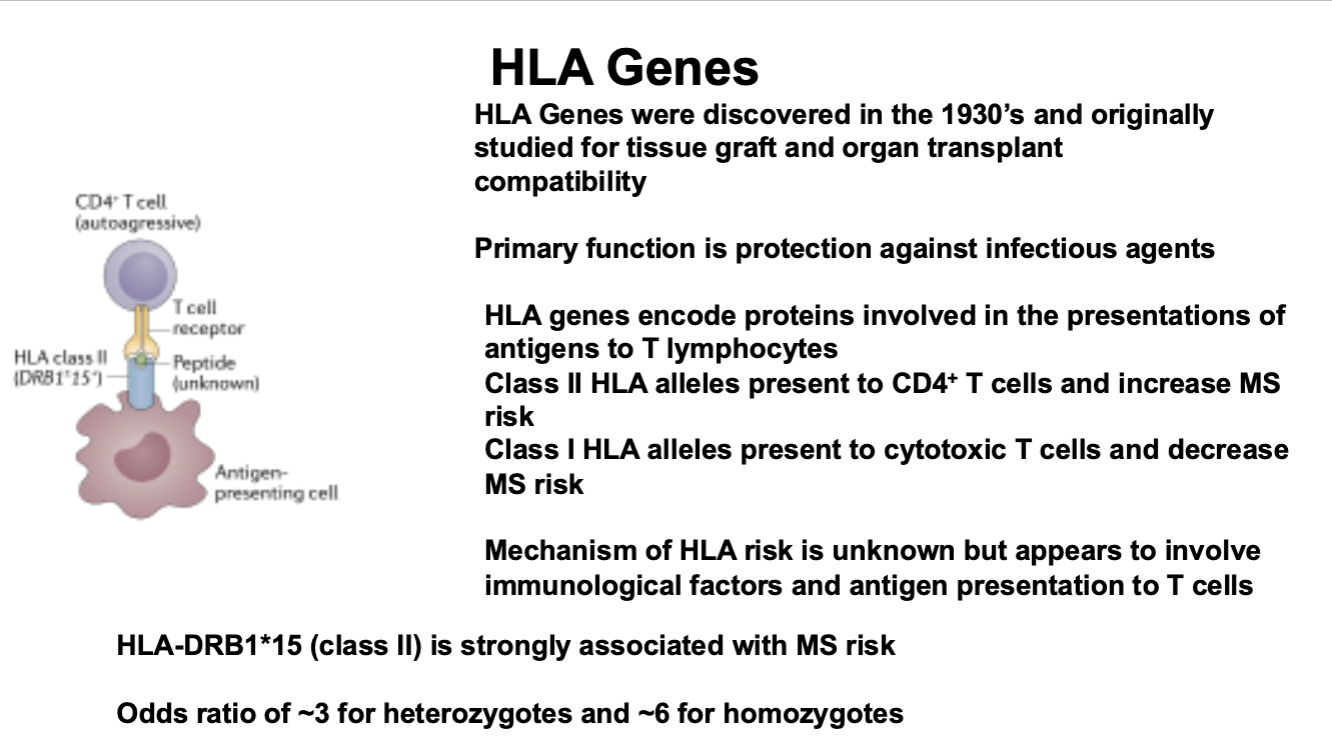
Most important genetic associations with the Major Histocompatibility Complex (MHC) also known as Human Leukocyte Antigen (HLA) complex
HLA Genes
The Inflammatory Process in MS
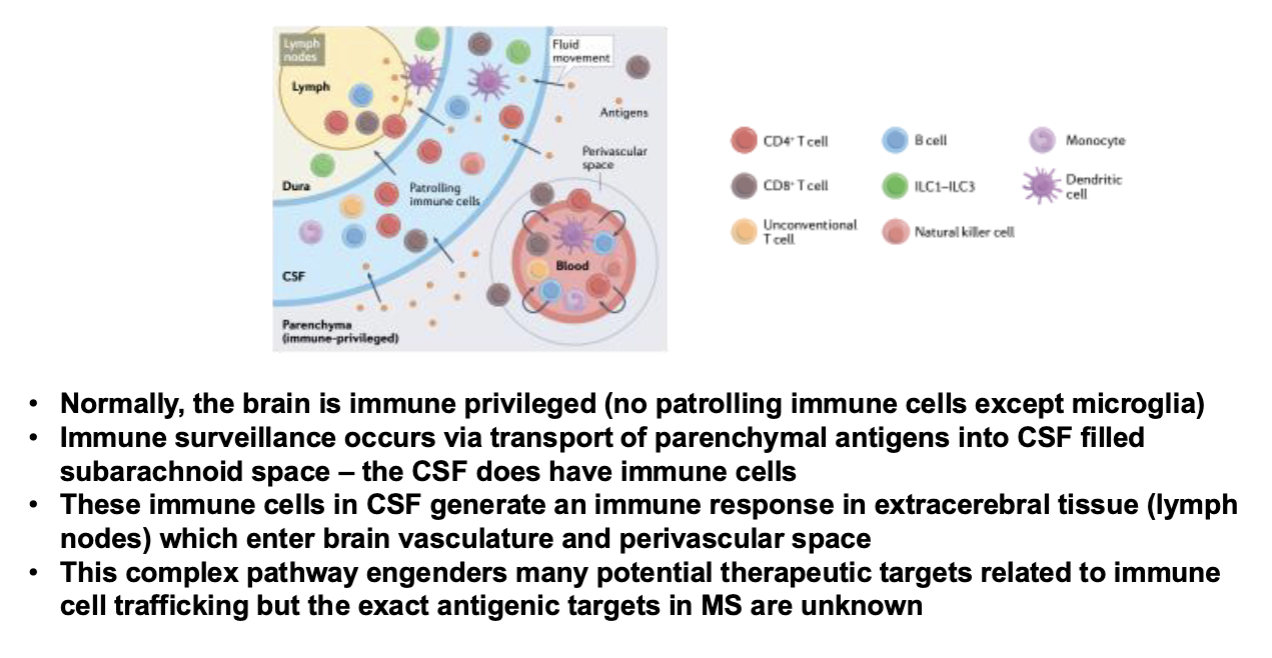
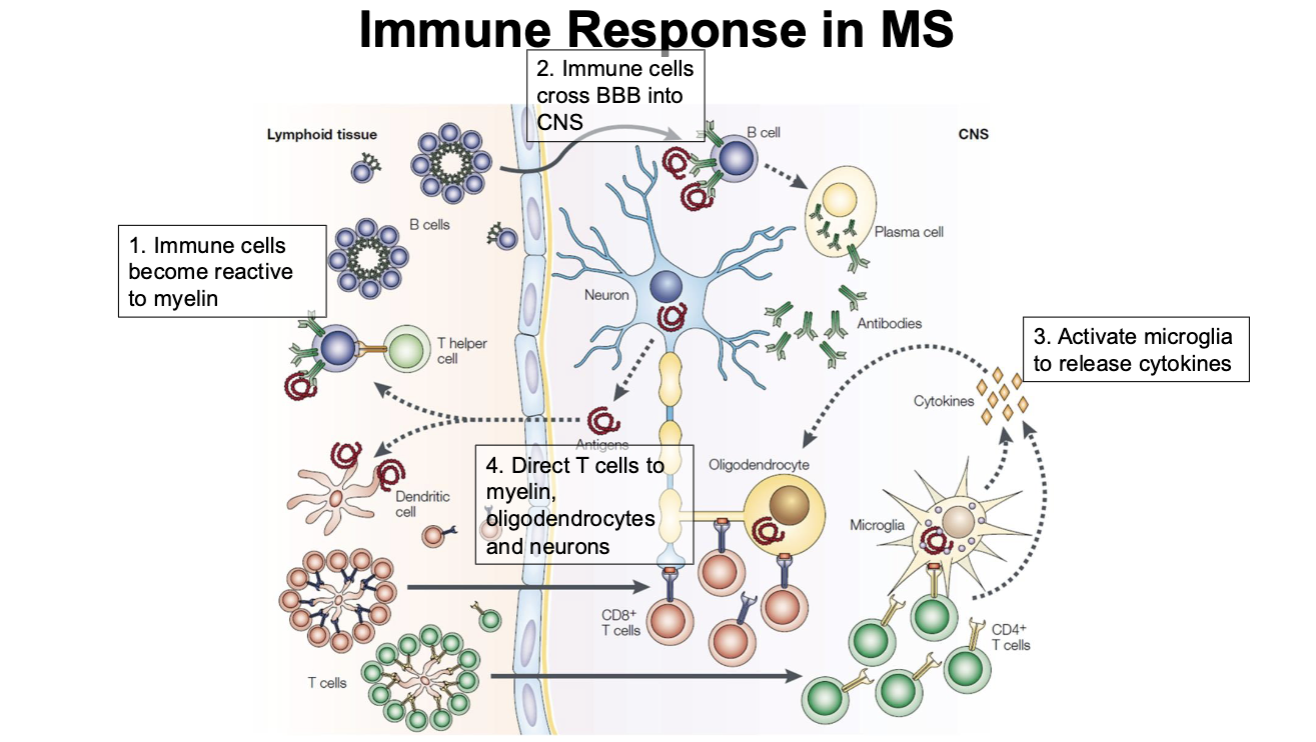
Immune Response in MS
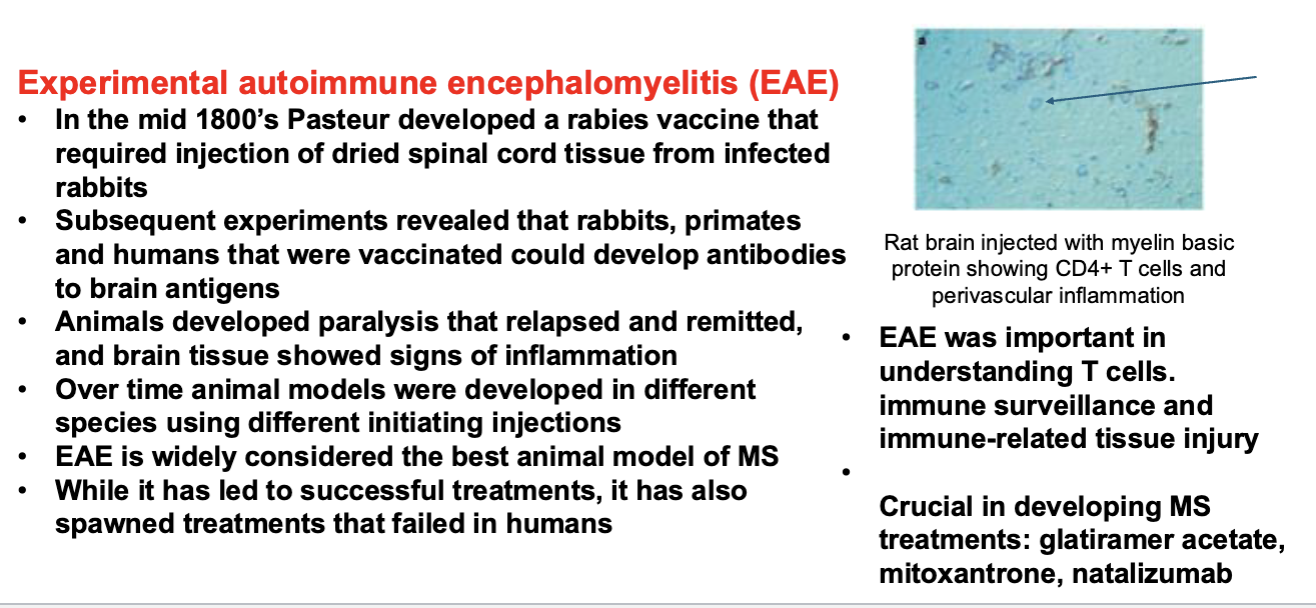
Drug Development in MS: EAE
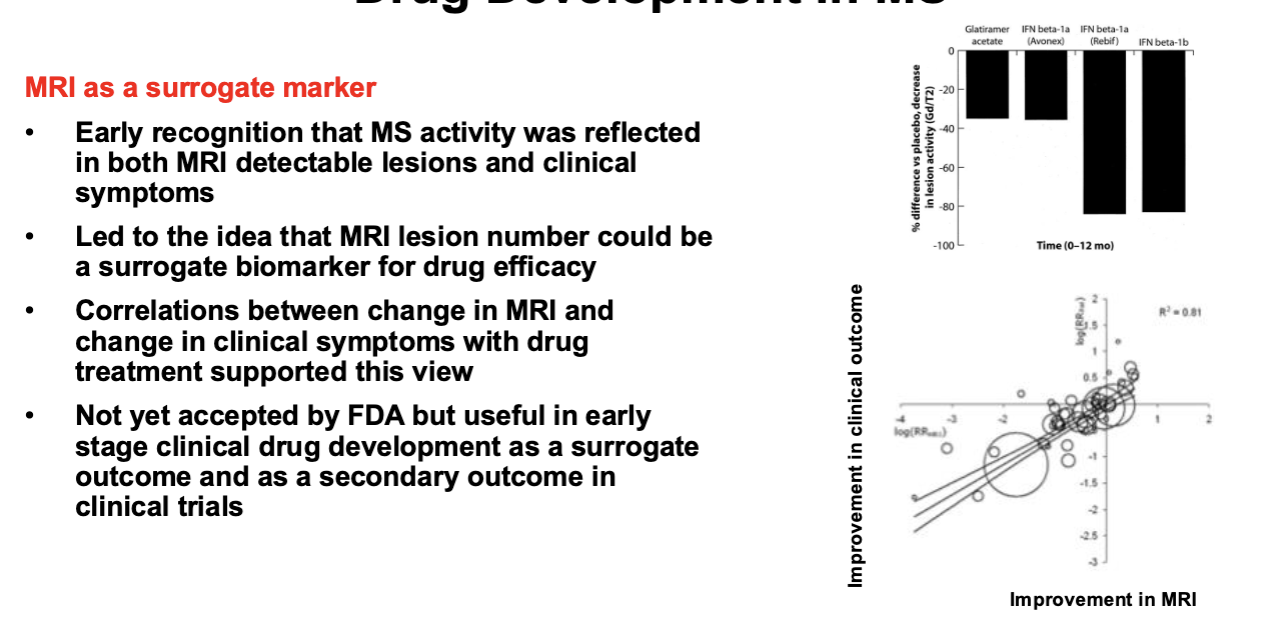
Drug Development in MS: MRI Surrogate Marker
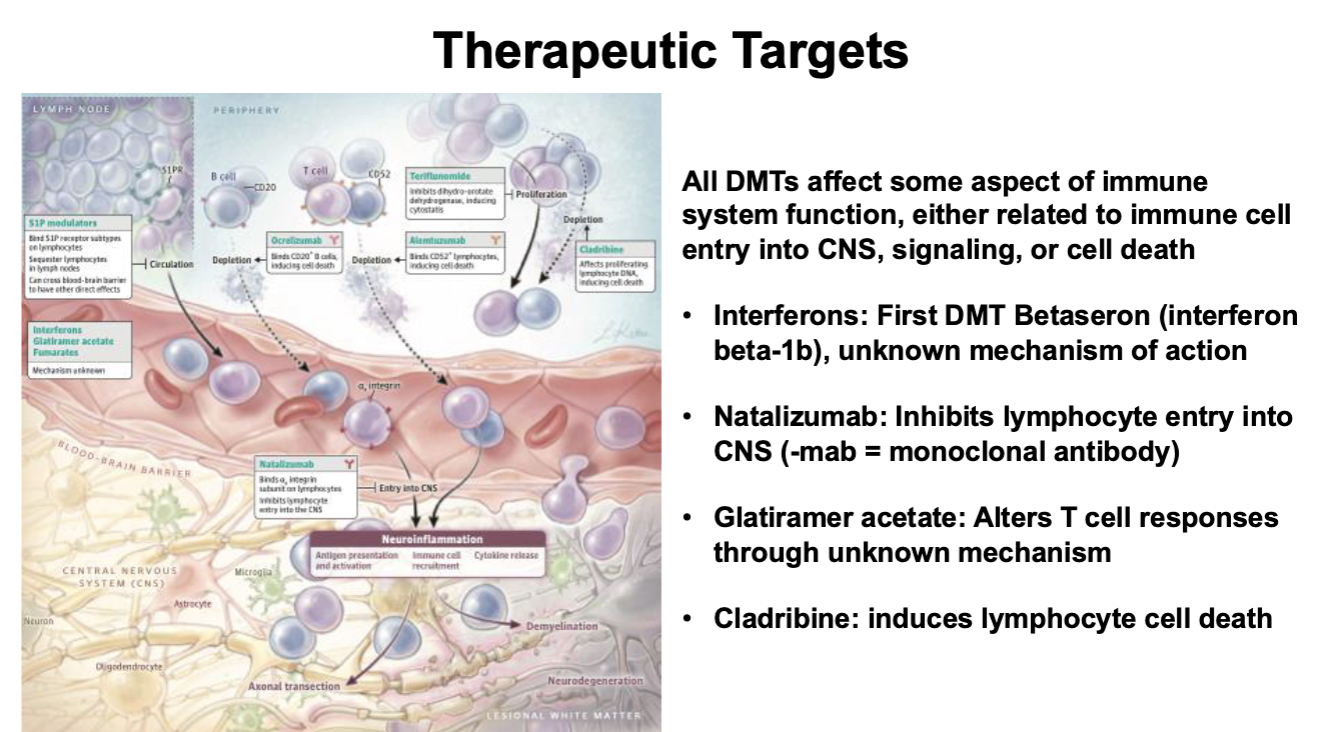
Treatment for MS
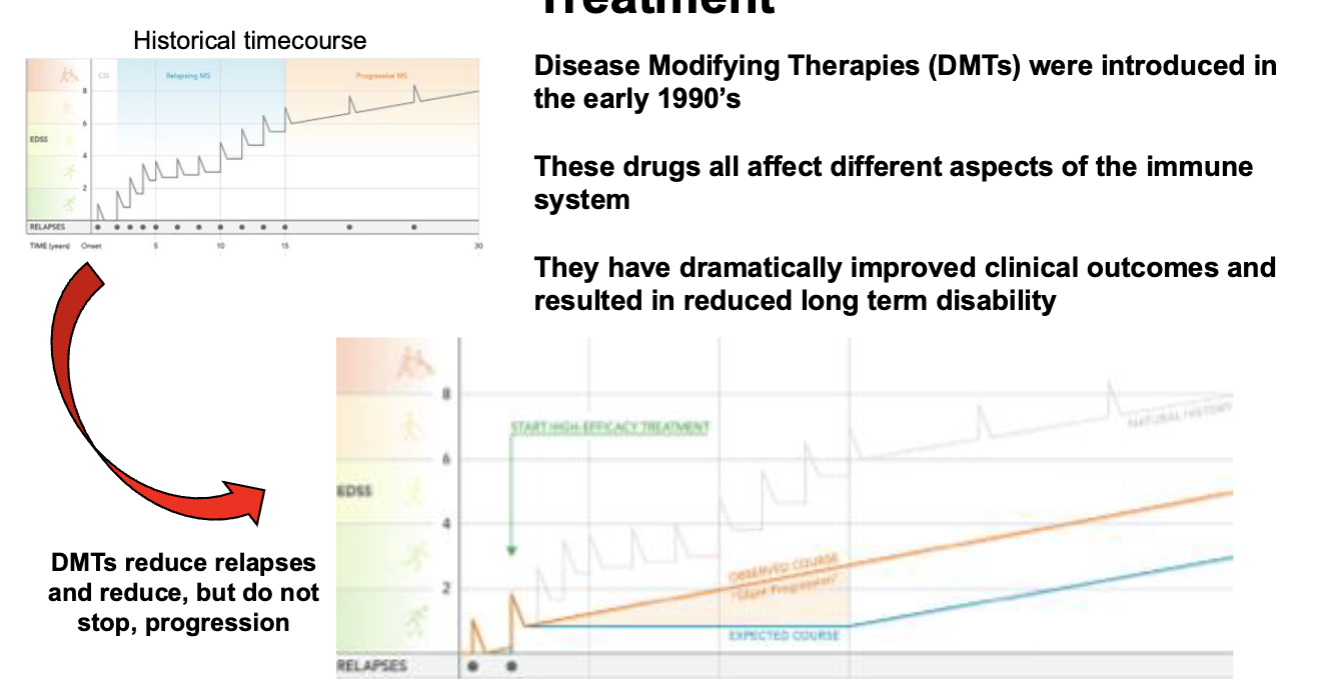
Therapeutic Targets for MS