Exam 3: Eating and Swallowing
1/75
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
76 Terms
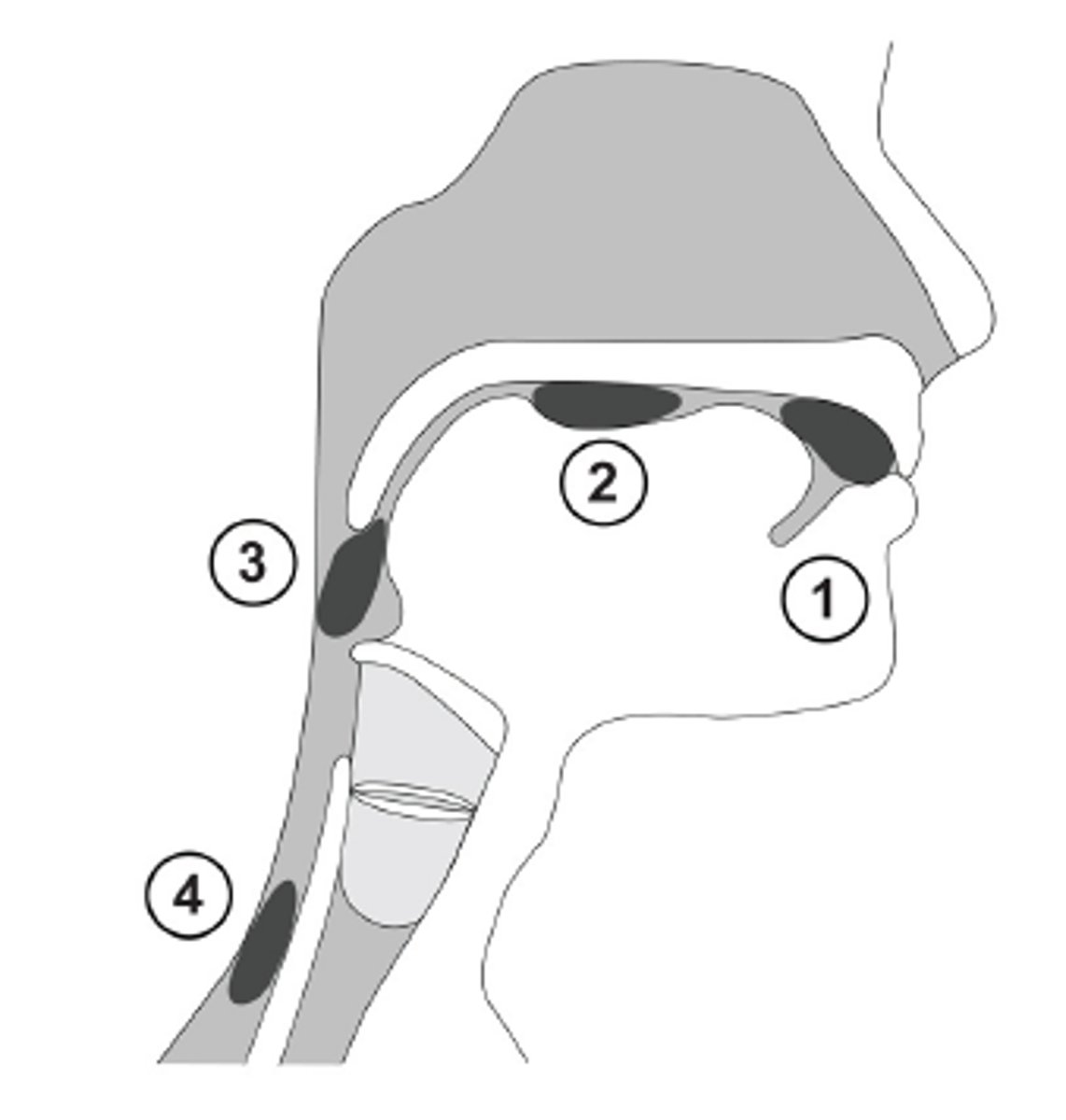
phases of eating and swallowing
1) pre-oral phase
2) oral phase
3) pharyngeal phase
4) esophageal phase
1) pre-oral phase
-visual and olfactory stimulate salivary glands
-2 ADLs connected : feeding and eating
-food is masticated by the teeth/gums and manipulated by the lips, cheeks, and tongue to form a bolus for swallowing
-posterior portion of tongue forms tight seal w/ velum (prevents slippage of liquid/food into the pharynx)
-varying amounts of time needed to form bolus (depends on food texture)
**oral-prep phase
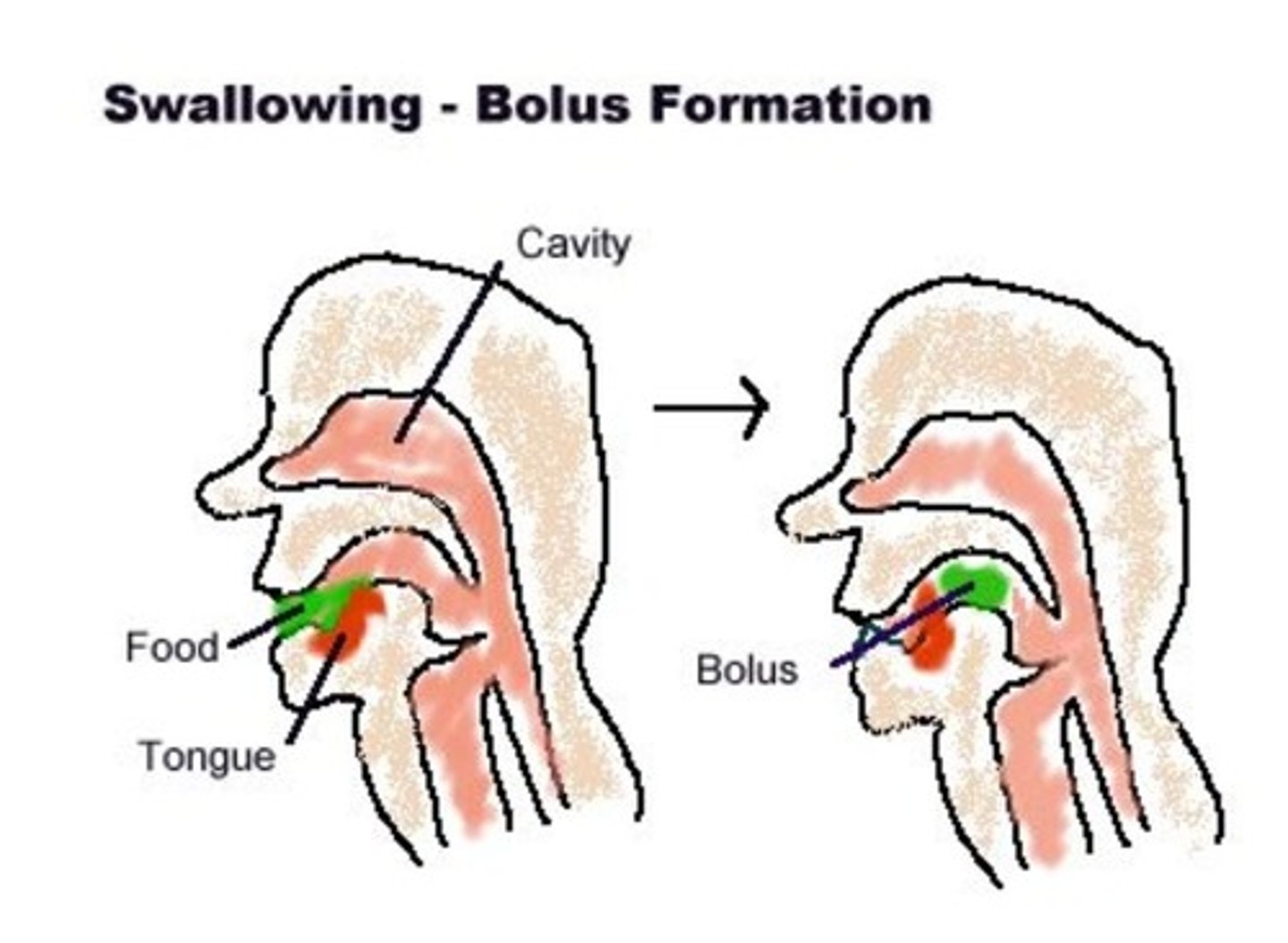
food is masticated by the teeth/gums and manipulated by the lips, cheeks, and tongue to form a bolus for swallowing
a) pre-oral phase
b) oral phase
c) pharyngeal phase
d) esophageal phase
a) pre-oral phase
which phase of eating and swallowing are two ADLs connected?
a) pre-oral phase
b) oral phase
c) pharyngeal phase
d) esophageal phase
a) pre-oral phase
the amount of time it takes to form a bolus depends on what?
the type of food
-soft foods = shorter time
-denser food = longer time
what types of food require greater oral motor control and often present more difficulty for clients with oral preparatory phase swallowing problems?
foods that are a mixture of liquid and solids (such as soup with chunks of vegetables)
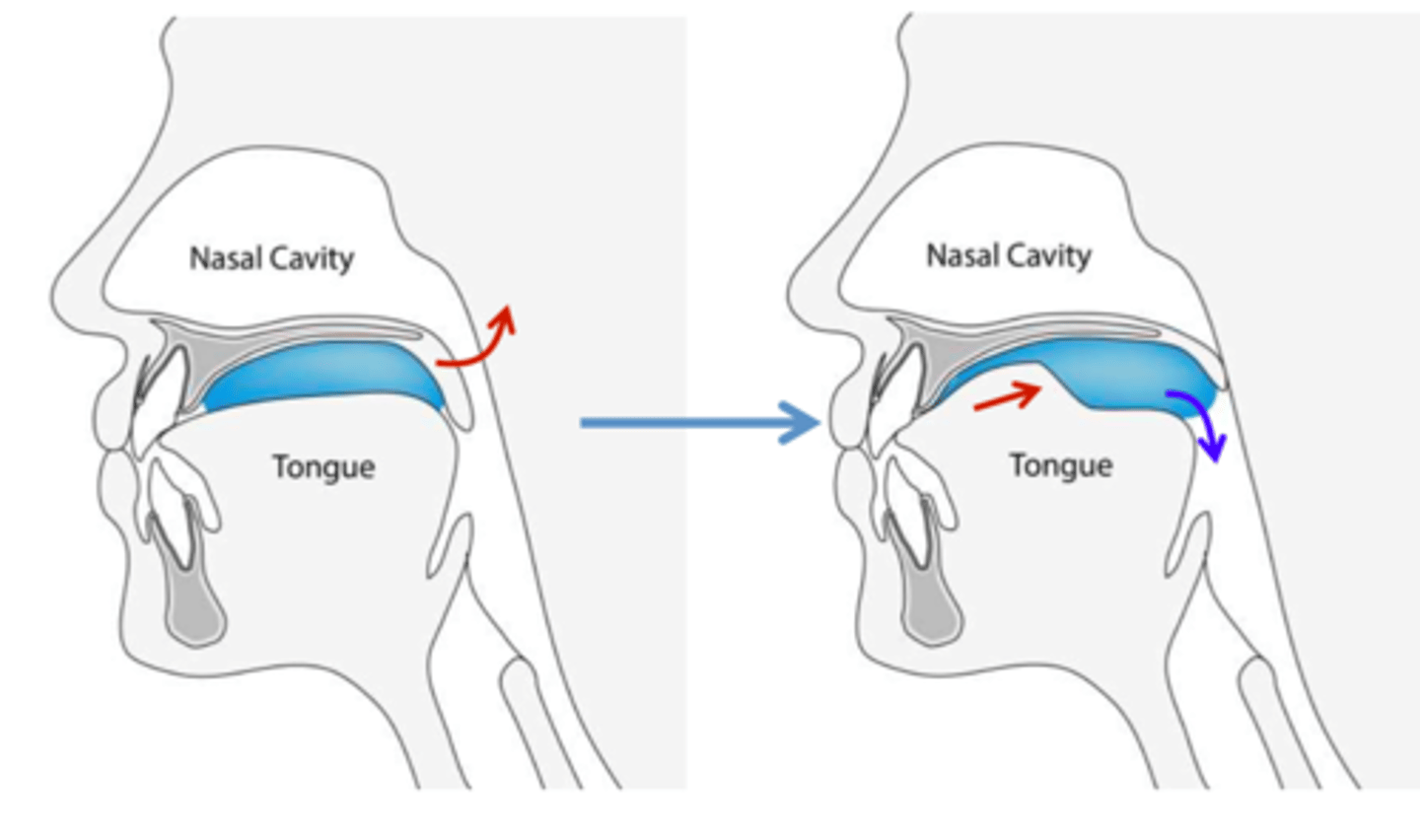
2) oral phase
-tongue initiates posterior movement of the bolus toward the pharynx
-swallow is voluntary so person needs to be alert
oral phase is
a) voluntary
b) involuntary
a) voluntary
oral phase requires intact
-labial musculature to keep food in mouth
-lingual mvmt ro propel bolus towards pharynx
-buccal musculature to prevent food from entering lateral sulci
-ability to breathe through the nose
tongue initiates posterior movement of the bolus toward the pharynx; swallow is voluntary so person needs to be alert
a) pre-oral phase
b) oral phase
c) pharyngeal phase
d) esophageal phase
b) oral phase
swallow is voluntary so person needs to be alert
a) pre-oral phase
b) oral phase
c) pharyngeal phase
d) esophageal phase
b) oral phase
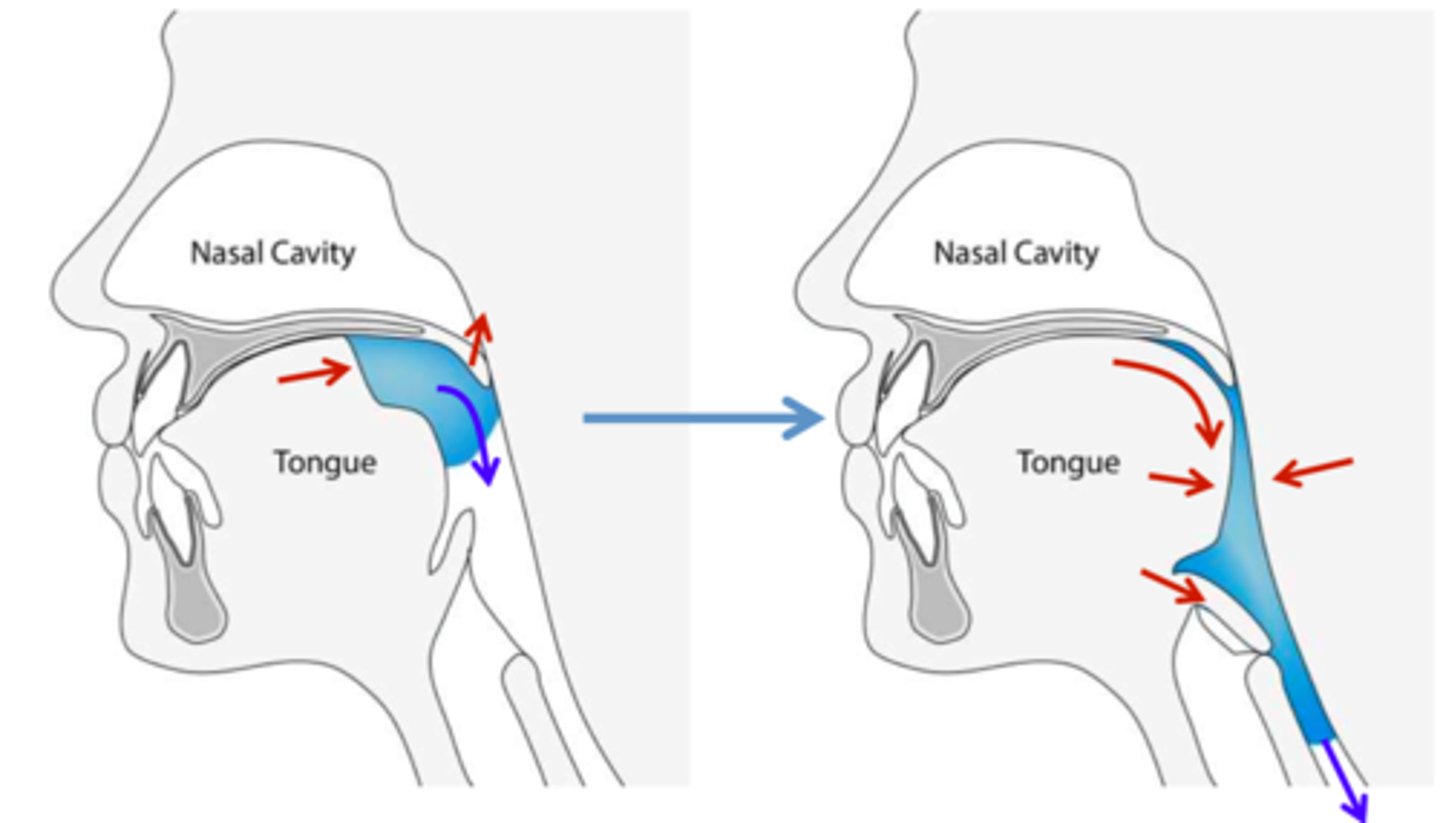
3) pharyngeal phase
-voluntary and involuntary components
-swallow response
-closure of larynx and epiglottis to prevent material from entering airway
-mvmt must be rapid and efficient, so respiration is only briefly interrupted
swallow response; closure of larynx and epiglottis to prevent material from entering airway
a) pre-oral phase
b) oral phase
c) pharyngeal phase
d) esophageal phase
c) pharyngeal phase
mvmt must be rapid and efficient, so respiration is only briefly interrupted
a) pre-oral phase
b) oral phase
c) pharyngeal phase
d) esophageal phase
c) pharyngeal phase
voluntary and involuntary components
a) pre-oral phase
b) oral phase
c) pharyngeal phase
d) esophageal phase
c) pharyngeal phase
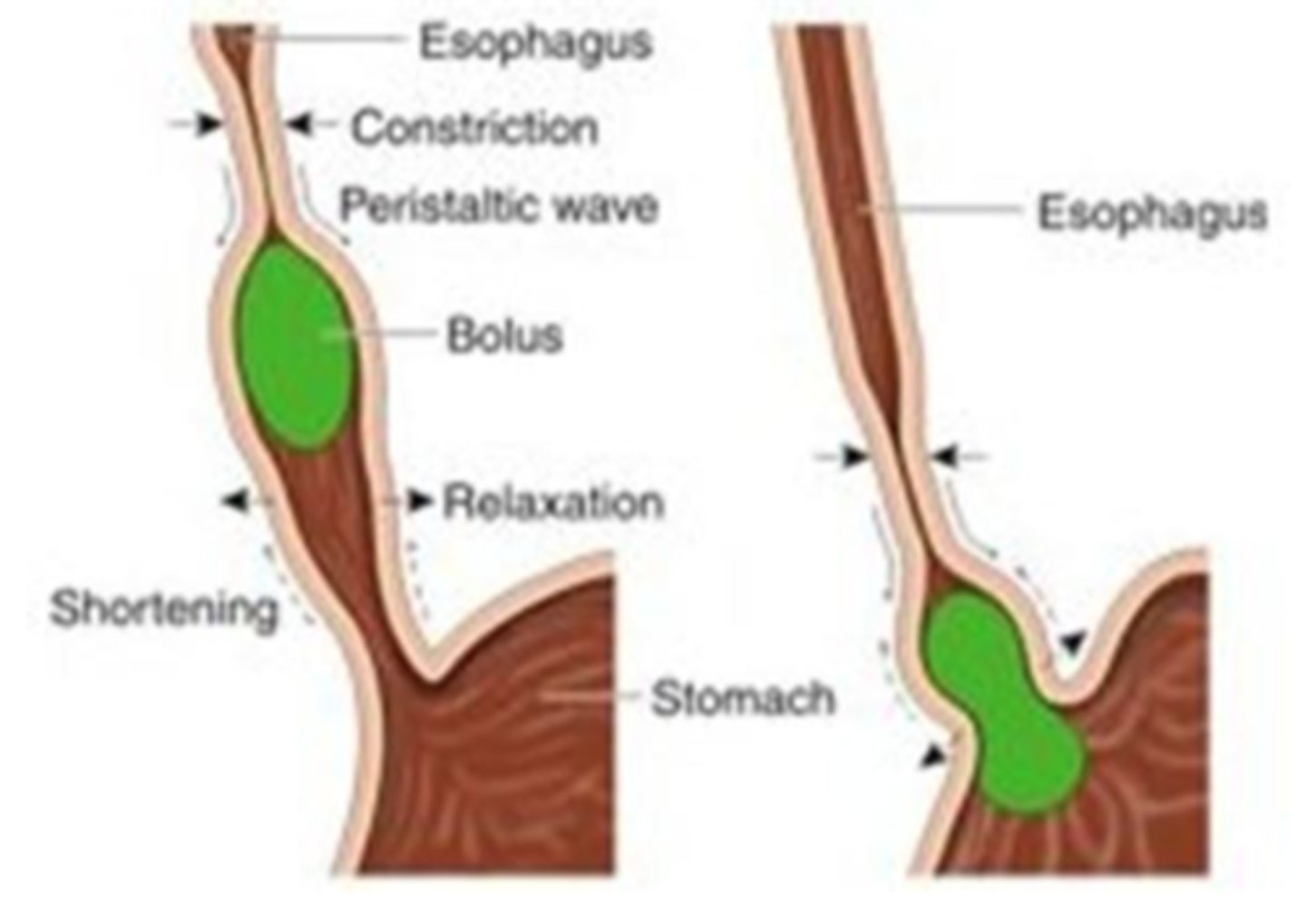
4) esophageal phase
-muscles of esophagus contract and bolus is transported to the stomach
-epiglottis returns to relaxed position and airway opens
muscles of esophagus contract and bolus is transported to the stomach
a) pre-oral phase
b) oral phase
c) pharyngeal phase
d) esophageal phase
d) esophageal phase
epiglottis returns to relaxed position and airway opens
a) pre-oral phase
b) oral phase
c) pharyngeal phase
d) esophageal phase
d) esophageal phase
eating and swallowing assessment involves......
1) medical chart review
2) cognitive-perceptual status
3) physical status
a medical chart review involves
-looking for prior incidents of aspiration
-the pt's hydration and nutrition status (do they have an altered diet texture? NG or G tube? - indicates serious dysphagia)
when assessing cognitive-perceptual status, the patient must....
-be alert, oriented, and able to follow simple directions
-have memory for recalling safe strategies for eating
-have visual, visual-perceptual skills, and motor planning for feeding
close supervision during an eating and swallowing assessment is required for patients with...
-confusion
-dementia
-poor awareness of eating task
-poor attention span
-impaired perception and memory
when assessing physical status, the patient must have....
head control
-ROM and motor control (including quality of mvmt)
-effect of positioning on abnormal muscle tone
-needed to provide stable base for jaw and tongue mvmt
-needed for anatomical positioning for safety during swallow to reduce risk of aspiration
an oral assessment includes.....
1) outer oral status
2) inner oral status
an outer oral status assessment includes.....
1) sensation
2) musculature
3) oral reflexes
what are indicators of impaired sensation?
-drooling
-food remaining on lips
-food falling from mouth w/o awareness
what should you assess for sensation?
-light touch and localization (occlude vision and use cotton swabs)
-temperature sensation (occlude vision and use hot/cold tubes)
what should you look for when assessing for musculature status?
-any asymmetry
-masked appearance
-frowning
-grimacing
damage to the brainstem or cortical structures may cause.....
re-emergence of oral reflexes
i.e. rooting, bite, and suck-swallow
re-emergence of rooting, bite, and suck-swallow reflexes will __________ with safe eating and swallowing
a) interfere
b) not interfere
a) interfere
gag, palatal, and cough reflex ____________ be present for safe swallow
a) should
b) should not
a) should
which reflexes should not be present for safe swallow?
a) rooting, bite, and suck-swallow reflex
b) gag, palatal, and cough reflex
a) rooting, bite, and suck-swallow reflex
which reflexes should be present for safe swallow?
a) rooting, bite, and suck-swallow reflex
b) gag, palatal, and cough reflex
b) gag, palatal, and cough reflex
an inner oral status includes.....
1) dentition
2) tongue movement
why should we look at dentition when assessing inner oral status?
-a bad fit of dentures can interfere with safely eating and swallowing
-bad fit can also rub on gums and cause sores/injuries
what is the typical shape of a tongue?
slightly concave with groove running down midline
a flattened, bunched, or rounded tongue is unsafe because
it interferes with safe eating and swallowing
what is the resting position for the tongue?
midline, slightly behind front teeth
a retracted tongue may indicate......
abnormal tone or soft-tissue shortening
a tongue deviated to the right or left with protrusion indicates........
muscle weakness on the affected side
what questions should you ask yourself during an eating and swallowing assessment?
1) alert and able to participate in a swallowing assessment?
2) adequate trunk and head control, with or without assistance?
3) adequate tongue control to form bolus and move it through oral cavity?
4) larynx mobile enough to elevate quickly and with sufficient force during swallow?
5) can client handle saliva with minimal drooling?
6) does client have a productive cough, strong enough to expel any material that may enter the airway?
**if yes to all, then proceed with various food consistencies during assessment
food texture progression (easy to hard)
1) pureed
2) soft
3) mechanical soft textured
4) thick drink
5) semi-thick drink
6) thin, flavored liquid
7) water
pudding, applesauce
pureed foods
banana, mac and cheese
soft foods
ground tuna with mayo, chopped meat with gravy
mechanical soft textured
nectar blended with half a banana
thick drink
fruit nectar, yogurt drink
semi-thick drink
juice
thin, flavored drink
what type of food consistency should be given for decreased oral motor control, chewing difficulties, and apraxia?
a) pureed
b) thick liquids
c) mechanical soft
a) pureed
what type of food consistency should be given for poor endurance, breathing difficulties, and difficulty attending to task?
a) thick liquids
b) pureed
c) mechanical soft
b) pureed
what type of food consistency should be given for delayed swallow or impaired motor control?
a) thick liquids
b) pureed
c) mechanical soft
a) thick liquids
instrumental swallow assessments
video-fluoroscopic swallow study (VFSS)
-radiation
fiberoptic endoscopy (FEES)
-no radiation
-highly effective in detecting aspiration and pharyngeal dysphagia
indicators of eating and swallowing dysfunction
-difficulty or inability to shape food into cohesive bolus
-prolonged chewing
-loss of food or liquid from nose
-coughing or frequent throat clearing before, during, or after the swallow
-wet or gurgling voice quality after eating or drinking
-food residue remaining in mouth
-discomfort or pain when swallowing
-difficulty breathing while eating
-unusual head or neck mvmts while swallowing
symptoms of aspiration
change in skin color, wet/gurgling voice, weak cough, coughing or choking on food, prolonged or delayed swallow, uncoordinated speech, drooling
intervention goals
-facilitation of appropriate positioning during eating
-improve motor control at each stage of swallow
-maintenance of adequate hydration and nutrition intake
-prevention or reduction of aspiration risk
-re-establishment of oral eating to safest, optimum level on the least restrictive diet
proper positioning for eating
-seated on a firm surface
-trunk flexed slightly forward (100° hip flexion) with back straight
-arms placed forward on table
-head erect, in midline, with chin slightly tucked
what position is contraindicated for oral feeding?
supine
hand placement to assist with eating
side hold position by therapist/caregiver
-for mod-max A
front hold position
-for min A
oral feeding requirements
-be alert
-able to maintain adequate trunk and head positioning with assistance
-have beginning tongue control
-manage secretions with minimal drooling
-have a reflexive cough
a person must complete the oral and pharyngeal phases combined in under ________ seconds
10 seconds
a person must swallow with minimal aspiration of _______ % or less of the time
10%
diet progression levels
level 1 - pureed (mod-severe swallow difficulties)
level 2 - mechanical soft (mild-mod swallow difficulties)
level 3 - advanced (intact swallow response)
level 1
pureed
eamples of level 1 foods (puree)
-pureed bread mixes
-custard
-smooth cereal
-pureed eggs
-mashed potato with gravy
-pureed noodles
-pureed soups
-smooth puddings, custards, yogurt
level 2
mechanical soft
examples of level 2 foods (mechanical soft)
-oatmeal
-soft pancakes with syrup
-scrambled eggs
-soft banana
-cream soups
-cooked fruit w/o seeds
-well cooked veggies
-moistened ground meat
-moist Mac and cheese
-tofu
-tuna or egg salad w/o big chunks
-soft fruit pies
-canned fruit
-soft moist cakes
level 3
advanced
examples of level 3 foods (advanced)
-well moistened cereals
-bread with butter or syrup
-any egg
-all canned and cooked fruit
-rice and fried potatoes
-all soups
-tender veggies
-thin sliced tender or ground meats
-casserole
liquids progression (easy to hard)
1) spoon thick (commercial thickener)
2) honey-like
3) nectar-like
4) thin
principles of oral feeding
-visual component of feeding (present food w/i visual field)
-allow pt to bring food to mouth as independently as possible
-eating is a social activity
-continual assessment critical with feeding/swallowing
Which of the following correctly lists the progression of food textures from easiest to hardest for individuals with dysphagia?
A) Water → Pureed → Soft → Mechanical Soft Textured → Thick Drink → Semi-thick Drink → Thin, Flavored Liquid
B) Pureed → Soft → Mechanical Soft Textured → Thick Drink → Semi-thick Drink → Thin, Flavored Liquid → Water
C) Soft → Pureed → Mechanical Soft Textured → Semi-thick Drink → Thick Drink → Water → Thin, Flavored Liquid
D) Pureed → Mechanical Soft Textured → Soft → Thick Drink → Semi-thick Drink → Thin, Flavored Liquid → Water
B) Pureed → Soft → Mechanical Soft Textured → Thick Drink → Semi-thick Drink → Thin, Flavored Liquid → Water
A 72-year-old stroke patient is beginning to transition from tube feeding to oral intake. The speech-language pathologist has cleared them to start eating by mouth. Which food texture would you expect to be introduced first, and why?
A) Soft foods, because they require minimal chewing effort
B) Water, because it's easy to swallow and hydrating
C) Pureed foods, because they require no chewing and are easiest to control in the mouth
D) Thin, flavored liquids, because flavor stimulates swallowing reflex
C) Pureed foods, because they require no chewing and are easiest to control in the mouth
You are working with a client recovering from a traumatic brain injury. They are currently tolerating mechanical soft foods. What would be the appropriate next step in their dietary progression?
A) Pureed foods
B) Water
C) Soft foods
D) Thick drink
D) Thick drink
Rationale: The next step after mechanical soft foods would be to challenge their liquid tolerance, starting with thick drinks.
A patient reports frequent coughing and throat clearing after drinking water. Based on the standard progression of liquids, what consistency should the OT recommend trying instead?
A) Thin, flavored liquid
B) Semi-thick drink
C) Thick drink
D) Mechanical soft food
C) Thick drink
Rationale: Thickened liquids move more slowly and are easier to control, reducing the risk of aspiration. Giving a different thin liquid (even if flavored) is not a safer option—it’s the same problematic consistency, just with added taste.
You observe that your client can handle semi-thick drinks without signs of aspiration. What should you trial next in the progression?
A) Water
B) Pureed foods
C) Thin, flavored liquid
D) Mechanical soft foods
C) Thin, flavored liquid
Rationale: Thin, flavored liquids come just before water and are an important step in building tolerance to thin textures.
A client with Parkinson's disease is currently on a pureed diet. They are showing improved oral-motor control and fewer signs of aspiration. As the OT collaborating on the dysphagia team, which food texture would be the most appropriate to trial next?
A) Water
B) Semi-thick drinks
C) Mechanical soft foods
D) Soft foods
D) Soft foods
Rationale: After pureed, the next progression is soft foods, which introduce mild chewing while still being easy to manage.