Immunology Exam 1 study guide (Days 1-3)
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
List the WBCs and explain the role of each in the immune system
Neutrophil—Most abundant WBC, performs phagocytosis
Basophils—release histamine that maintain allergic reactions
Lymphocytes—Target immune response; T, B, & NK cells
Eosinophils—Release cytokines, phagocytosis, neutralizes products of allergic reactions
Monocytes—cleanup crew, develop into macrophages
Differentiate between T cells, B cells, and NK cells, explaining their functions in the immune response
T-cells: Mature in the thymus
T cells have 3 subsets that aid in killing infectious cells in the immune system and keep you healthy
B-cells: Mature in the bone marrow
Major role in antibody production
NK-cells: Mature in both the bone marrow and the 2nd lymphoid organs
kill virus infected cells
List the primary and secondary organs of the lymphoid system
Primary: Bone Marrow, Thymus
Secondary: Lymph nodes, Spleen, MALT, SALT
Differentiate between innate and adaptive immunity
Innate immunity:
Prior exposure not required, memory not generated, immediate effects
Adaptive immunity:
Memory is generated; the immune system remembers prior exposure.
List & explain the mechanisms of innate immunity
physical barriers, chemical shields, patrolling white blood cells, and blood proteins to prevent infection and alert the adaptive immune system
What are PRR’s, PAMPs, and TLRs and what is their role in the immune system
PRRs: Pattern Recognition Receptors that are mainly found on surface of macrophages, sense cellular infection
PAMPs: Molecules unique to infectious organisms, innate immune system quickly recognizes pathogens by using these
TLRs: specialized sensor proteins of the innate immune system. They act as the body's alarm system, recognizing specific molecular signatures found on viruses, bacteria, and fungi to trigger a rapid inflammatory defense and activate the adaptive immune response
Steps of phagocytosis
engulf and destroy large particles, microorganisms, and cellular debris
Primary cells involved in phagocytosis
Neutrophils
Monocytes
Macrophages
Dendritic cells
What is an acute phase reactant, and how does it participate in the immune response
Acute-phase reactants are serum proteins that increase or decrease rapidly in response to infection or injury
Enhance contact between microbes and phagocytic cells
two key acute phase reactants
C-reactive protein (CRP)
Complement C3
How is adaptive immunity activated by the innate system
Antigen presentation
What steps are included in inflammation
recognition of the threat, recruitment of immune cells, removal of the harmful agent, regulation of the response, and tissue repair
List the 5 factors which affect the immune response
Age
Overall health
Route of exposure to an antigen
Antigen dose
Genetic composition (MHC genes)
Antigen vs. Immunogen vs. Hapten
Antigens are substances specifically recognized by the immune system
Immunogens are substances capable of stimulating an adaptive immune response
Haptens are small substances that are nonimmunogenic by themselves unless combined with a carrier
MHC Class I vs Class II Molecules
MHC Class I molecules are expressed on ALL nucleated cells and process endogenous antigens
Highest on lymphocytes and myeloid cells
MHC Class II molecules are found primarily on APCs and process exogenous antigens
What is the role of CD4 & CD8 T cells in immune response
CD8 T cells bind to antigen class I MHC complex and destroy the target cell
CD4 T cells stimulate B cells to divide and differentiate into antibody-producing plasma cells
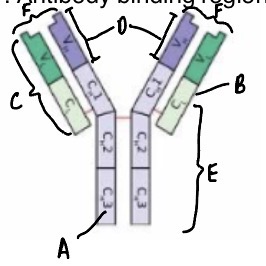
Immunoglobulin structure
List & give characteristics for each of the different antibody classes
IgG
predominant immunoglobulin in the serum, only immunoglobulin capable of crossing the placenta
IgM
Largest Ig with its pentamer structure. It is the primary response antibody, first to appear during an immune response
IgA
Major Ig in the body’s secretions, occurs as a dimer. present in breastmilk and transfers immunity to newborn infant
IgD
Can serve as a receptor for antigen on the surface of B cells
IgE
Binds to mast cells that mediates allergic reactions and defense against large parasites
Primary vs. Secondary antibody response
Primary antibody response
1st exposure to antigen: memory cells are generated; low-affinity antibody; longer lag phase
Secondary antibody response
Memory response; shorter lag phase; high affinity antibody
Cell mediated immunity vs. Humoral immunity
Cell mediated immunity
T Cells are the main component; cytotoxic T cells destroy cancer cells; helper T cells secrete cytokines
Humoral immunity
B lymphocytes & antibodies; antibodies mark antigens for phagocytosis
What is the role of B cells in the immune response
As plasma cells, they produce antibodies in BM & peripheral lymphoid organs
B cells respond quickly to blood borne pathogens
What is the role of T cells (CD4 and CD8) in the immune response?
T cells interact with APCs to initiate adaptive immune response
T cells circulate throughout the bloodstream
What is the role of T regulatory cells?
Suppress immune response to self-antigens and harmless antigens
Secrete inhibitory cytokines that inhibit proliferation of other T-cell populations
Define affinity and avidity
Affinity
Initial attraction force between a single Fab site on an antibody molecule and a single epitope on an antigen
Avidity
Sum of attractive forces between an antigen and an antibody
Explain the Zone of Equivalence, Prozone, and Postzone in agglutination reactions.
Zone of Equivalence
Number of multivalent sites of antigen and antibody is approximately equal
Prozone
Antibody excess; no cross-linkages are formed; Antigen combines with only one or two antibody molecules
Postzone
Antigen excess; No lattice network is formed; Small aggregates are surrounded by excess antigen
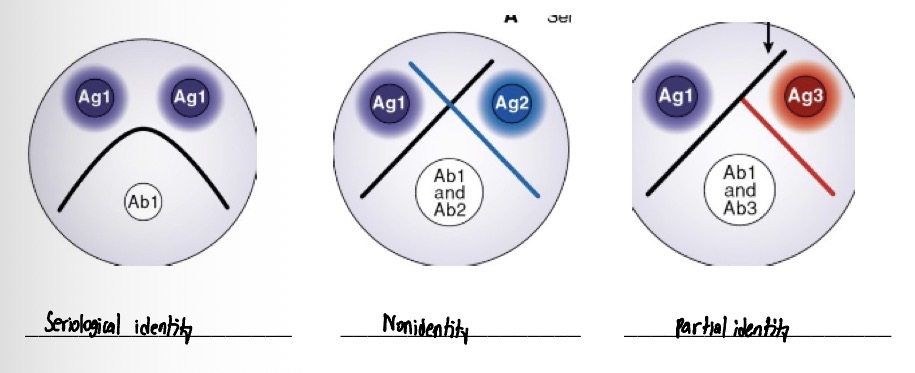
Explain the difference between Radial Immunodiffusion and Ouchterlony double diffusion.
Radial immunodiffusion is a single diffusion technique whereas Ouchterlony double diffusion is a double diffusion technique with three possible patterns as results
Explain Immunofixation electrophoresis
Proteins in patient serum are electrophoresed, then antibody is applied directly to gel
Precipitates form where antigen-antibody combination has taken place
Differentiate between Immunoturbidimetry and Nephelometry
Immunoturbidity involves decreasing light transmission as antigen concentration increases leading to turbidity. Nephelometry is light that is scattered at a measured angle, indicating the amount of an antigen or antibody present
Identify the following patterns
Explain the following agglutination methods:
a. Direct agglutination
b. Passive agglutination
c. Reverse passive agglutination
d. Agglutination inhibition
Direct agglutination
Uses particles coated with naturally occurring antigens to test for antibodies in patient serum
Passive agglutination
Uses particles coated with antigens not normally found on their surface; Antigen is attached to carrier particle, agglutination occurs if antibody is present
Reverse passive agglutination
Antibody is attached to carrier protein, agglutination occurs if antigen is present in patient serum
Agglutination inhibition
Competition between particulate antigens vs. soluble antigens in the patient sample for limited antibody-combining sites; Bacteria serves as the carrier of antibody
List the five general ways used to detect the causative agent of a bacterial infection
1) Culture of causative agent
2) Microscopic examination
3) Biochemical testing
4) Detection of bacterial antigens
5) Molecular detection of bacterial DNA or RNA
Pharyngitis symptoms and lab tests
Symptoms
throat pain, difficulty swallowing, fever, and swollen lymph nodes
Lab tests
Throat culture, Mononucleosis Test, RADT
impetigo symptoms and lab tests
Symptoms
red sores that quickly burst, leaking fluid and forming distinctive amber or "honey-colored" crusts
Lab tests
Blood or urine tests, biopsy, skin or nasal swab
Scarlet fever symptoms and lab tests
Symptoms:
a distinctive sandpaper-like red rash, a high fever, and a swollen "strawberry" tongue
Lab tests:
Throat cultures
Blood or antibody tests
Rheumatic fever symptoms and lab tests
Symptoms
Fever, joint pain, inflammation of the heart
Lab tests
ASO titer
Rapid strep test
Poststreptococcal glomerulonephritis symptoms and lab tests
Symptoms
Malaise, abdominal discomfort, edema
Lab tests
Urinalysis, serum complement levels
Explain the principle, interpretation, and clinical significance of the antistreptolysis O (ASO).
Principle
Nephelometric methods are currently used that measure light scatter produced by immune complexes formed after binding of patient ASO to streptolysin-coated particles
Interpretation
Generally (<200) IU/mL for adults and (<150 - 200) IU/mL for children, though this varies slightly by laboratory.
Clinical significance
acute rheumatic fever (where \(>80\%\) of patients have elevated ASO) and post-streptococcal glomerulonephritis
Explain the principle, interpretation, and clinical significance of the streptozyme tests.
Principle
The test uses sheep red blood cells (RBCs) coated with a cocktail of five key streptococcal exoantigens
Interpretation
Positive Result: The presence of visible clumping or agglutination of the red blood cells indicates the presence of antibodies to one or more of the streptococcal antigens. Results can be reported qualitatively (positive/negative) or as a titer depending on the dilution. [1, 2, 3, 4]
Negative Result: A smooth, homogeneous suspension of cells without any clumping indicates the absence of these streptococcal antibodies (or levels below the limit of detection
Clinical significance
The Streptozyme test is highly useful as a screening tool to identify past or recent Group A streptococcal infections, especially when evaluating patients for post-streptococcal complications
What disease state is associated with an elevated cold agglutinin titer and what is the minimum titer needed to be considered significance
CAD, minimum titer is ≥1:64
What are cryoglobulins and what disease are they associated with
abnormal antibodies (immunoglobulins) in the blood that clump together, or precipitate, at cold temperatures and dissolve again when the body warms up
Cryoglobulinemia
Name two Rickettsial infections and how they are transmitted
RMSF
Transmitted by ticks
Murine Typhus
Flea-borne disease
What testing methodology is used as the gold standard for Rickettsial diseases?
IFA
Name the two most common spirochete diseases?
Syphilis
Lyme Disease
List the clinical stages of syphilis and the symptoms present.
Primary stage
Development of a chancre
Secondary stage
Malaise, Fever, rash
Latent stage
Asymptomatic
Tertiary stage
Neurosyphilis
What syphilis testing is used for:
a. CSF =
b. Serum=
C. Confirmatory testing=
a.) Neurosyphilis
b.) Routine syphilis screening
c.) initial syphilis screenings
Distinguish treponemal from nontreponemal tests for Syphilis
Nontreponemal
These tests do not look for antibodies against the syphilis bacterium itself. Instead, they detect "reagin" antibodies, which are produced by the body in response to cellular damage and lipids (such as cardiolipin) released during a syphilis infection
Treponemal
These tests detect antibodies that specifically target the proteins of the syphilis bacterium
Explain the testing methodology associated with the VDRL and RPR
VDRL
Patient serum is mixed on a slide with a cardiolipin-lecithin-cholesterol antigen suspension and clumping is used to identify the results
RPR
Patient serum is mixed on a card with charcoal particles with cardiolipin antigen
Differentiate between the FTA-ABS and TP-PA treponemal tests
FTA-ABS
A manual, indirect immunofluorescence assay. Patient serum is placed on a slide containing killed T. pallidum bacteria. If the patient has syphilis antibodies, they bind to the bacteria. A fluorescently tagged anti-human antibody is added, causing the spirochetes to glow under a fluorescence microscope
TP-PA
An agglutination assay. Patient serum is mixed with gelatin particles coated with T. pallidum antigens. If antibodies are present, they cause the particles to clump (agglutinate) together and form a flat mat at the bottom of a microtiter well, whereas a negative result causes the particles to settle into a tight button
Which organism causes lyme disease?
B. burgdorferi, (black legged ticks)
What are the clinical manifestations of Lyme disease and what test method is most often used for identification?
Stage 1
Localized rash
Stage 2
Early dissemination
Stage 3
Late dissemination with arthritis or neurologic symptoms
Tests
EIA or IFA
Explain the differences between competitive and non-competitive binding in immunoassay.
Competitive binding
All reactants are mixed together simultaneously; The amount of bound label is inversely proportional to the concentration of the labeled antigen
Non-competitive binding
Patient antigen is captured by antibody bound to a solid phase; the amount of label is directly proportional to the amount of antigen in the patient sample
Differentiate between heterogeneous and homogeneous assay
Heterogenous
Involves physical separation of bound and free components
Homogenous
Do not require a physical separation step
Explain the following testing methodologies for immunoassay:
A. Enzyme immunoassay (EIA)
B. Radioimmunoassay (RIA)
C. Chemilluminescent immunoassay (CLIA)
D. Immunoflourescent assay (IFA
A. Highly sensitive assays that use enzymes as labels, which react with suitable substrates to produce breakdown products that may be chromogenic fluorescent, or luminescent
B. Measures trace amounts of analytes that are small in size. Is extremely sensitive and precise
C. Combines antigen-antibody immune reactions with chemiluminescent detection to quantify or qualify specific target molecules (like hormones, tumor markers, and infectious diseases) in patient samples
D. uses fluorescently labeled antibodies to detect specific antigens or antibodies in a sample
What is a capture or sandwich assay
a highly sensitive laboratory method used to detect and measure specific target proteins or antigens in a sample
What is a High-dose hook effect?
an analytical error in immunoassays (like an ELISA or pregnancy test) where extremely high concentrations of a target substance paradoxically produce a falsely low or negative result