Adult Neuro: TBI
0.0(0)
Studied by 0 peopleCard Sorting
1/42
Last updated 6:45 PM on 11/5/22
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
1
New cards
Traumatic Brain Injury
"An alteration in brain function, or other evidence of brain pathology, caused by an external force"
2
New cards
Primary Injury
1. Contact with an internal or external force (skull or penetrating object such as a bullet)
- Results in contusion, laceration, and intracerebral hematomas
- Damage is generally focal in nature where contact occurs
2. Rapid acceleration/deceleration
- Shear, tensile, compression forces
-Causes diffuse axonal injury(DAI), tissue tearing, and intracerebral hemorrhage
-DAI is most common mechanism in individuals with moderate to severe TBI
-Seen with MVA, some sports
-Mechanism is microscopic.... may be minimal findings initially on MRI or CT
- Results in contusion, laceration, and intracerebral hematomas
- Damage is generally focal in nature where contact occurs
2. Rapid acceleration/deceleration
- Shear, tensile, compression forces
-Causes diffuse axonal injury(DAI), tissue tearing, and intracerebral hemorrhage
-DAI is most common mechanism in individuals with moderate to severe TBI
-Seen with MVA, some sports
-Mechanism is microscopic.... may be minimal findings initially on MRI or CT
3
New cards
Secondary Injury
-Cell death as a result of cellular events that follow tissue damage in addition to the secondary effects of hypoxemia, hypotension, ischemia, and elevated ICP
-Develop over hours to days- -Inflammatory responses lead to
cell death
*Primary and secondary mechanisms are not mutually
exclusive and often do not occur in isolation*
-Develop over hours to days- -Inflammatory responses lead to
cell death
*Primary and secondary mechanisms are not mutually
exclusive and often do not occur in isolation*
4
New cards
Coup/Countercoup Injury
-"Blow" and "Counterblow."
- Two separate brain injuries sustained during the same incident.
-A coup injury refers to the brain damage that occurs directly under
the point of impact.
-A contre coup injury occurs on the opposite side of the brain from
where the head is struck.
These injuries can occur separately, but if the blow is strong enough, they usually appear together (as a coup- contrecoup injury).
- Two separate brain injuries sustained during the same incident.
-A coup injury refers to the brain damage that occurs directly under
the point of impact.
-A contre coup injury occurs on the opposite side of the brain from
where the head is struck.
These injuries can occur separately, but if the blow is strong enough, they usually appear together (as a coup- contrecoup injury).
5
New cards
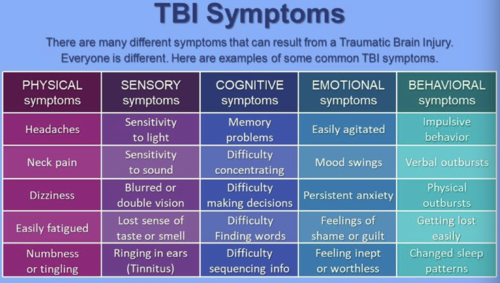
TBI Symptoms
6
New cards
Neuromuscular
-Decreased UE/LE strength and/or paresis
-Impaired coordination
-Impaired postural control
-Abnormal tone, can be spasticity present
-Impaired coordination
-Impaired postural control
-Abnormal tone, can be spasticity present
7
New cards
Cognitive
Most common with frontal lobe injury Deficits in:
-Arousal
-Attention
-Concentration
-Memory
-Learning
-Executive functions (Planning, cognitive flexibility, initiation, self- generation, sequencing)
-Arousal
-Attention
-Concentration
-Memory
-Learning
-Executive functions (Planning, cognitive flexibility, initiation, self- generation, sequencing)
8
New cards
Neurobehavioral
-Often more debilitating in the long run than physical limitations
These include:
-Low frustration tolerance
-Agitation
-Disinhibition
-Apathy
-Emotional lability
-Mental inflexibility
-Physical/verbal aggression
-Impulsivity
-Irritability
These include:
-Low frustration tolerance
-Agitation
-Disinhibition
-Apathy
-Emotional lability
-Mental inflexibility
-Physical/verbal aggression
-Impulsivity
-Irritability
9
New cards
Communication
-Often related closely to cognitive impairments
-Disorganized oral and written communication
-Word retrieval difficulties
-Disinhibited and socially inappropriate language
Often have:
-Difficulty reading social cues
-Difficulty communicating in distracting environments
-Significant impact on social integration and quality of life
-Disorganized oral and written communication
-Word retrieval difficulties
-Disinhibited and socially inappropriate language
Often have:
-Difficulty reading social cues
-Difficulty communicating in distracting environments
-Significant impact on social integration and quality of life
10
New cards
Secondary Impairments
DVT
Heterotopic Ossification
Pressure ulcers
Pneumonia
Chronic pain
Contractures
Poor endurance
Muscle atrophy
Spasticity
Heterotopic Ossification
Pressure ulcers
Pneumonia
Chronic pain
Contractures
Poor endurance
Muscle atrophy
Spasticity
11
New cards
Activity Limitations Related to Execution of Task
Difficulties with:
- Walking
- Carrying/handling objects
- Changing and maintaining body position
- ADL's
*Experience longer lasting impairments in problem solving, memory, and cognitive comprehension when compared to physical/motor related limitations
- Walking
- Carrying/handling objects
- Changing and maintaining body position
- ADL's
*Experience longer lasting impairments in problem solving, memory, and cognitive comprehension when compared to physical/motor related limitations
12
New cards
Examination
• Integument integrity
• Sensory integrity
• Motor function
• Range of motion (including tone assessment)
- Decorticate rigidity: UE are flexed, LE extended
- Decerebrate rigidity: UE and LE are extended
- Spastic hypertonia
- Hypotonia
• Reflexintegrity
• Ventilation and respiration/gas exchange
• Sensory integrity
• Motor function
• Range of motion (including tone assessment)
- Decorticate rigidity: UE are flexed, LE extended
- Decerebrate rigidity: UE and LE are extended
- Spastic hypertonia
- Hypotonia
• Reflexintegrity
• Ventilation and respiration/gas exchange
13
New cards
Outcome Measures*
Outcome Measures*
14
New cards
Alertness
responds fully and appropriately to stimuli, can open eyes, look at examiner
15
New cards
Lethargy
appears drowsy, can open eyes and look at examiner, responds appropriately but falls asleep easily
16
New cards
Obtundation
opens eyes to look at examiner, responds slowly and is confused, decreased alertness
17
New cards
Stupor
can be aroused with painful stimuli, verbal responses slow or absent, minimal awareness of self
18
New cards
Coma
cannot be aroused, eyes remain closed
19
New cards
Coma Recovery Scale
*23 items with 6 subscales Auditory, visual, motor, oromotor, communication and arousal
20
New cards
Disorders of Consciousness Scale (DOCS)
*23 items which assess social knowledge, taste/swallowing, olfactory function, proprioception, tactile sensation, auditory and visual function
21
New cards
Spasticity / Contractures
-Serial casting is common for plantarflexor and biceps contracture
-Allows prolonged stretch
-Much watch for skin breakdown as patients cannot communicate discomfort
-May not be appropriate for patients that may hurt themselves or others with the cast
-Allows prolonged stretch
-Much watch for skin breakdown as patients cannot communicate discomfort
-May not be appropriate for patients that may hurt themselves or others with the cast
22
New cards
Increased Cranial Pressure
-The encasing of the brain in the cranium is problematic following an injury that results in swelling and increased fluid
-Normal ICP is 7-17 mm/Hg, elevations of to 25-30 can result in herniation if not treated
-With symptoms of increased ICP the HOB is often placed to 30 degrees to decrease pressure
-With increased ICP additional ischemia and resultant brain injury is common
-Treatment for this pressure may be a craniotomy (patient will have to wear a helmet, activity limitations)
-Normal ICP is 7-17 mm/Hg, elevations of to 25-30 can result in herniation if not treated
-With symptoms of increased ICP the HOB is often placed to 30 degrees to decrease pressure
-With increased ICP additional ischemia and resultant brain injury is common
-Treatment for this pressure may be a craniotomy (patient will have to wear a helmet, activity limitations)
23
New cards
Increased IP Symptoms
-Altered level of consciousness - progresses from restlessness to unresponsiveness
-Altered vital signs: increased BP, decreased HR, increased temp
-Headache
-Vomiting
-Pupillary changes
-Progressive impairment of motor function
-Seizure activity
-Altered vital signs: increased BP, decreased HR, increased temp
-Headache
-Vomiting
-Pupillary changes
-Progressive impairment of motor function
-Seizure activity
24
New cards
Post-Traumatic Amnesia (PTA)
• State of confusion occurring immediately following a TBI presenting as disorientation and inability to remember events that occur after the injury
• Length of PTA is best indicator of potential long term memory impairment
-Timeframe is determined based on first day of injury until the patient can store new memories
-Can measure using Mini Mental Assessment of Galveston Orientation and Amnesia Test
• Length of PTA is best indicator of potential long term memory impairment
-Timeframe is determined based on first day of injury until the patient can store new memories
-Can measure using Mini Mental Assessment of Galveston Orientation and Amnesia Test
25
New cards
Seizures
• Immediate seizures occur within 24 hours of the injury
• Early seizures occur within one week (Will see in 25% of those with confusion and 50%
with penetrating injuries)
• Post traumatic epilepsy-recurrent seizures more than one week post injury (Epilepsy is repeated seizures)
• Early seizures occur within one week (Will see in 25% of those with confusion and 50%
with penetrating injuries)
• Post traumatic epilepsy-recurrent seizures more than one week post injury (Epilepsy is repeated seizures)
26
New cards
Restraints
•Bed Alarms
•Wrist and Leg Restraints
•Enclosure Beds
•Seating and Positioning Adjustments
•Wrist and Leg Restraints
•Enclosure Beds
•Seating and Positioning Adjustments
27
New cards
Restraints Considerations
-Enclosure bed is good to keep pt safe but allow freedom of movement which can decrease agitation
• Need to wean off as soon as possible
• Consider abdominal binder over a g-tube (put on backwards)
-Stockinet over a pic line versus a four point restraint
-Let them show their motor restlessness by unlocking the wheelchair and let them move it around. Use a wrap around seatbelt
• Need to wean off as soon as possible
• Consider abdominal binder over a g-tube (put on backwards)
-Stockinet over a pic line versus a four point restraint
-Let them show their motor restlessness by unlocking the wheelchair and let them move it around. Use a wrap around seatbelt
28
New cards
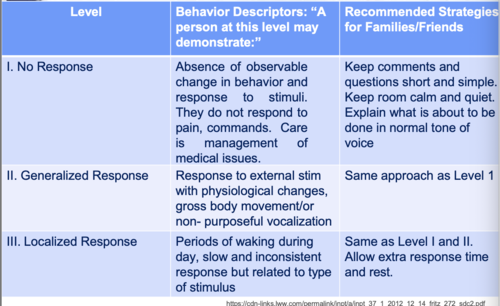
Rancho Levels I-III
STIMULATION Intervention
STIMULATION Intervention
-Several times a day for brief sessions
-Familiar voices
-Avoid sensory overload
-Get patient upright
-Keep track of stimulus and results
• Note what works best
-Do familiar activities
-Familiar voices
-Avoid sensory overload
-Get patient upright
-Keep track of stimulus and results
• Note what works best
-Do familiar activities
29
New cards
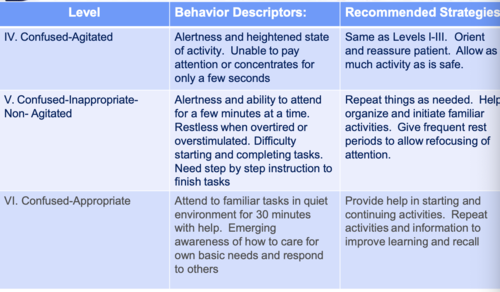
Rancho Levels IV-VI
STRUCTURE Intervention
STRUCTURE Intervention
• Progresses from agitated to confused inappropriate to confused appropriate
• Agitation has a strong fear base: calming, soothing
• Lability is common. Note but don'tfocus on crying, re-orient
• Calm voice - do not react to antics. It is NOT about you so don't take it personal
-Lack cognitive understanding and very scared
-Need to decrease agitation to increase attention to external environment
-IDENTIFY what elicits agitation and what calms
-Allow more time to process information
• How much time?
-Avoid unnecessary functional skills
• Agitation has a strong fear base: calming, soothing
• Lability is common. Note but don'tfocus on crying, re-orient
• Calm voice - do not react to antics. It is NOT about you so don't take it personal
-Lack cognitive understanding and very scared
-Need to decrease agitation to increase attention to external environment
-IDENTIFY what elicits agitation and what calms
-Allow more time to process information
• How much time?
-Avoid unnecessary functional skills
30
New cards
What to Consider? (Intervention)
-Consistency
-Expect no carryover
-Model calm behavior
-Expect egocentricity
-Be flexible and have options
-Safety
-Environment (start with closed environment to limit distractions)
-Reorientation is important
-Unsafe behavior must be addressed and tell them that behavior is not appropriate or ok. BRIEFLY - immediately move on. Do not give them lengthy clarification of why
-Redirection is a blatant change of direction. Can seem rude but very effective to redirect activity
EX: If they perseverate on going to the bathroom but have already gone
--> You could quickly interrupt and say "Hey, so you are a painter...what is the best way to pick out the best color for my house?"
-Always be calm. Give choices
-Use motivator at the end of walkway, or music, or family videos/pictures
-If the patient refuses to walk with you and you want to work on obstacles, put a chair in the way as you walk to the bathroom.
-Incorporate your activities in anything they are willing to participate in
• Do not be territorial over your areas! PT's can take a patient to the bathroom
-Expect no carryover
-Model calm behavior
-Expect egocentricity
-Be flexible and have options
-Safety
-Environment (start with closed environment to limit distractions)
-Reorientation is important
-Unsafe behavior must be addressed and tell them that behavior is not appropriate or ok. BRIEFLY - immediately move on. Do not give them lengthy clarification of why
-Redirection is a blatant change of direction. Can seem rude but very effective to redirect activity
EX: If they perseverate on going to the bathroom but have already gone
--> You could quickly interrupt and say "Hey, so you are a painter...what is the best way to pick out the best color for my house?"
-Always be calm. Give choices
-Use motivator at the end of walkway, or music, or family videos/pictures
-If the patient refuses to walk with you and you want to work on obstacles, put a chair in the way as you walk to the bathroom.
-Incorporate your activities in anything they are willing to participate in
• Do not be territorial over your areas! PT's can take a patient to the bathroom
31
New cards
Use Motivators (Intervention)
-Be specific and clear of your expectations
"you need to participate for 2 minutes then you can have a break"
-Take note if you give them too much to do and behaviors escalate....make sure to adjust the bar
-Have a visible timer present so client can see the time pass
-Set concrete expectation
-If completed they can do what they wanted (ie. Lay down, etc)
"you need to participate for 2 minutes then you can have a break"
-Take note if you give them too much to do and behaviors escalate....make sure to adjust the bar
-Have a visible timer present so client can see the time pass
-Set concrete expectation
-If completed they can do what they wanted (ie. Lay down, etc)
32
New cards
Family Education
-Need to educate the family so they can learn the cues since they need to learn how to deal with behaviors and functional limitations once patient returns home
33
New cards
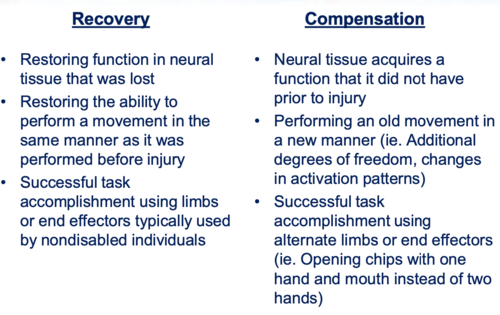
Recovery Vs Compensation
34
New cards
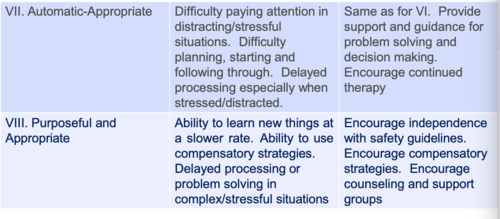
Rancho Levels VII-VIII
COMMUNITY Intervention
COMMUNITY Intervention
-Focus on functional skills
-Self-management activates involving
-ADLs and IADLs
-Home and community interaction and problem solving
-Consider context, tactile and gestural cues, hand over hand
-Self-management activates involving
-ADLs and IADLs
-Home and community interaction and problem solving
-Consider context, tactile and gestural cues, hand over hand
35
New cards
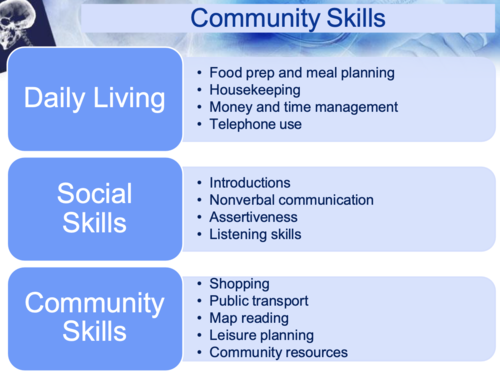
Community Skills
36
New cards
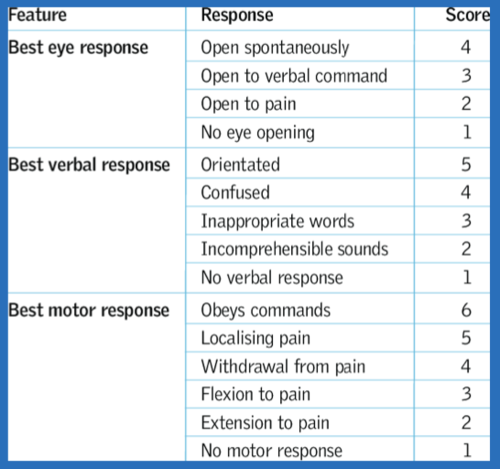
Glasgow Coma Scale
-adults in coma >1 month and children in a coma up to 3 months
-50% chance of waking up
-60% chance of having severe injury
-50% chance of waking up
-60% chance of having severe injury
37
New cards
Severe TBI
3-8
38
New cards
Moderate TBI
9-12
39
New cards
Mild TBI
13-15
40
New cards
Rancho Levels of Cognitive Function 1-3
41
New cards
Rancho Levels of Cognitive Function 4-6
42
New cards
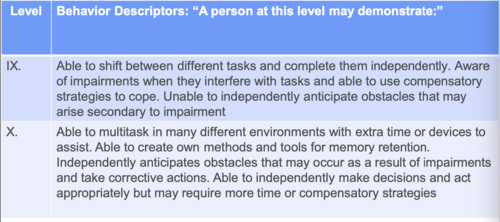
Rancho Levels of Cognitive Function 7-8
43
New cards
Rancho Levels of Cognitive Function 9-10