154 Second Examination
1/47
Earn XP
Description and Tags
CKD, Asthma, Shock/Sepsis, Colorectal Cancer, GERD/PUD
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
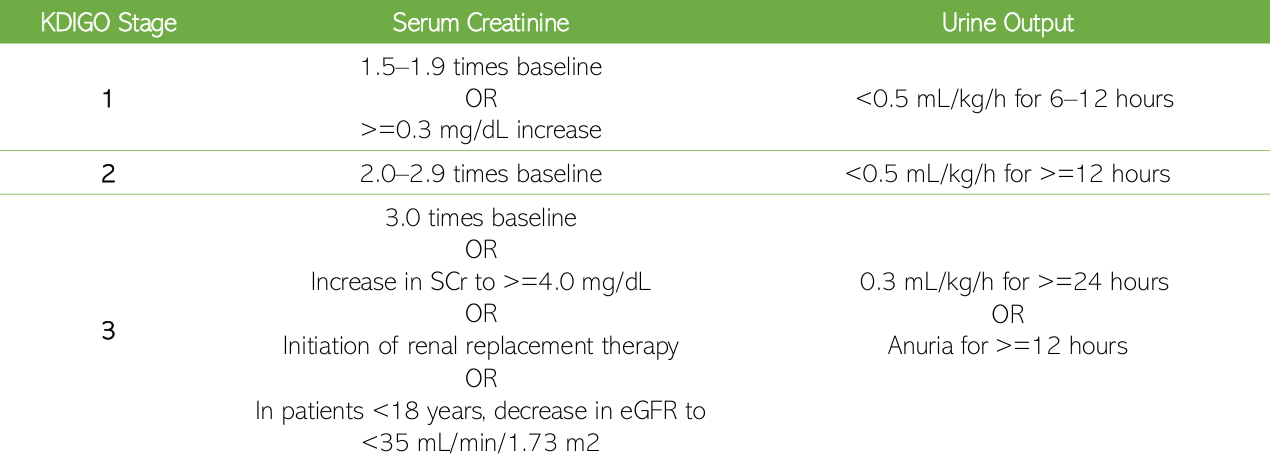
KDIGO Category for AKI [table]
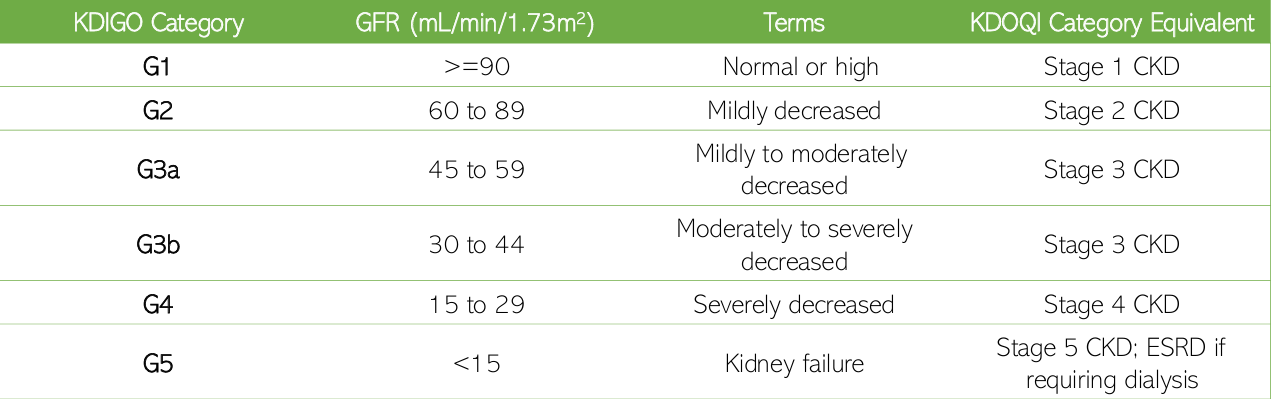
KDIGO Category for CKD [table]
Cause
GFR category
Albuminuria category
basis of KDIGO 2013
CGA staging
Acid-base balance
Water balance
Electrolyte balance
Toxin removal
Blood pressure control
Erythropoiesis
vitamin D activation
vital process associated with the renal system
AWETBED
Glomerular filtration
Tubular reabsorption
Tubular secretion
3 major processes in urine formation
Renal Insufficiency → Azotemia → Uremia → End-stage Renal Disease
progression of CKD
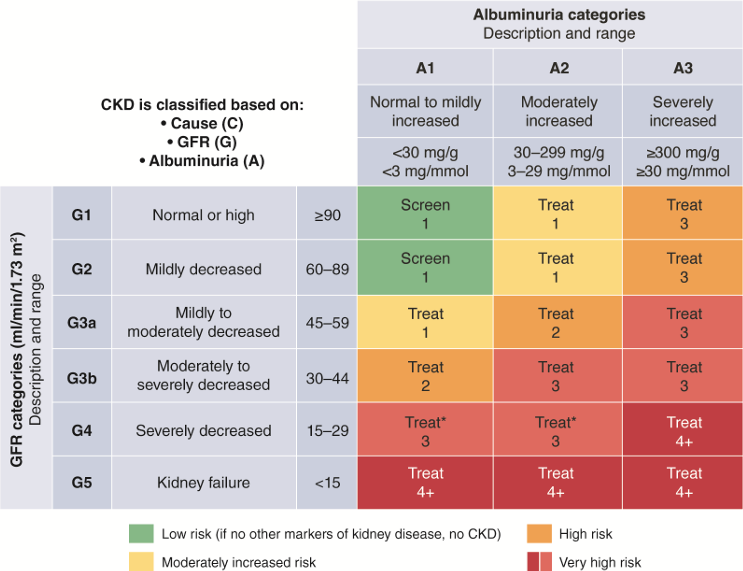
As GFR stage increases, the risk of the patient also increases
As albumin leakage increases, the risk of the patient also increases
trends in CGA Staging [table]
DM
HTN
Dyslipidemia
Age
Obesity
Smoking
Family history
Male sex
Protein-rich diet
Pregnancy
risk factors for CKD
edema
↑ blood levels of K, Mg, PO4
↓ blood levels of Ca, albumin
metabolic acidosis
clinical manifestations of CKD
mGFR (measured GFR)
gold standard for evaluating GFR
Creatinine or Cystatin C
eGFR estimates GFR using which parameters?
Renal ultrasound
which test is best used to detect structural abnormalities (e.g. obstruction)?
Perirenal hematoma
caution in patients with high bleeding risks
primary precaution when doing a biopsy
protein (albumin)
principal marker of kidney damage
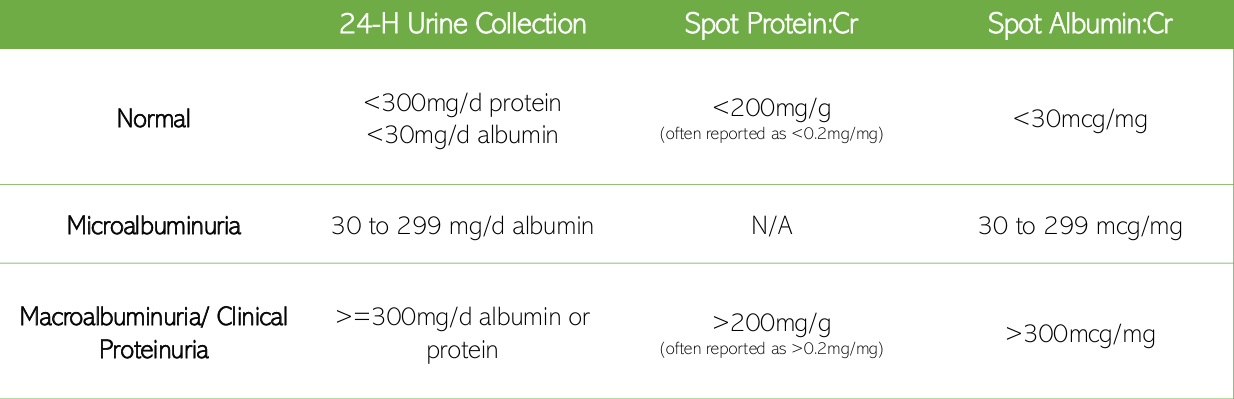
quantitative detection of urine protein/albumin [table]
Glomerular filtration rate (GFR)
Gold standard quantitative index of kidney function
Male: 107 to 147 mL/min/m2
Female: 98 to 138 mL/min/m2
Normal GFR levels (male and female)
< 60 mL/min/m2
GFR levels in CKD
Creatinine Clearance (CrCl)
Most widely used indirect measure of GFR
age
gender
weight
race
GFR estimation is based on which parameters?
AGWR
Cockcroft and Gault
preferred equation for drug dosing
Modification of Diet in Renal Disease (MDRD)
recommended by National Kidney Foundation for CKD staging
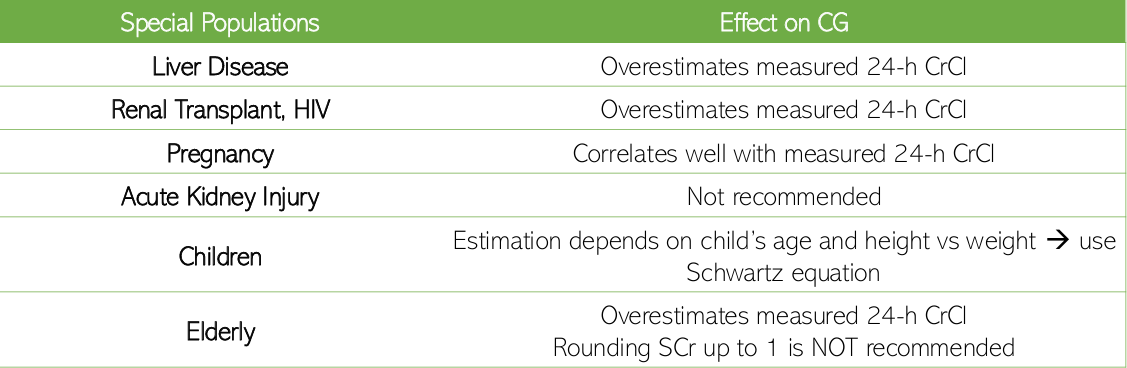
effect of special populations on CrCl [table]
Increase:
Decreased P-gp transport
Mg(OH)2 and NaHCO3
increases solubility ➝ absorption of weakly acidic drugs
Decrease
Gastroparesis
Increased gastric pH
Chelation
Vomiting and diarrhea
Bowel wall edema
Effect of CKD on absorption
Increase:
Decreased albumin ➝ increased acidic drugs
Decrease:
Increased alpha-1 acid glycoprotein ➝ decreased alkaline drugs
Effect of CKD on distribution
Liver:
Slowed Phase I (CYP3A4)
Slowed Phase II (slower conversion to a water-soluble compound)
Kidneys:
Reduced renal metabolism ➝ accumulation
Effect of CKD on metabolism
Decrease:
Glomerular filtration
Tubular reabsorption
Tubular secretion
Metabolite excretion
Effect of CKD on excretion
Digoxin ➝ altered tissue binding ➝ reduce the LD
Edema ➝ increased Vd ➝ increase the LD
Most drugs require the normal loading dose. What are the exceptions?
Prevent progression and complications
Treat underlying cause
DM, HTN, Dyslipidemia
Lifestyle modifications
Renal dose adjustment
Avoid nephrotoxins
Reduce incidence of complications from potential infections
Vaccination
Goals of Therapy
PTLRR
Add ACEi > ARB if with HTN or albuminuria
Add SGLT2 > Metformin > GLP-1 > DPP4 if with DM or albuminuria
Add statin if with ASCVD
Add-on: Antiplatelets > Ezetimibe / PCSK9i > Fenofibrate
Goals of Therapy for patients with DM, HTN, albuminuria, ASCVD
Exercise 30 minutes 5x per week
Weight loss if BMI > 25 kg/m2
Smoking cessation
Alcohol moderation (two/one drinks a day for men/women)
Modified DASH diet
Low K+
Low Na+ if with HTN
Non-pharmacological recommendations
EWSAM
Adjust medication doses
D/C if eGFR < 60 mL/min/1.73 m2 and hypovolemic
Metformin
RAAS blockers
Diuretics
NSAIDs
Lithium
Digoxin
Avoid herbal supplements
Updated vaccination
Influenza yearly
Pneumococcal if eGFR < 30 mL/min/1.73 m2
Hepatitis B if eGFR < 30 mL/min/1.73 m2
Use aspirin for ASCVD
Unless bleeding risk
Pharmacological recommendations (general)
8.5 - 10.5 mg/dL
Normal Total Serum Ca2+ levels
4.4 - 5.4 mg/dL
Normal Ionized Serum Ca2+ levels
0.1 - 1% is in the ECF
99% of total body stores of Ca2+ is in skeletal bone
How much (in %) of the total body calcium (or phosphate) is reflected in plasma?
2.5 - 4.5 mg/dL
Normal Serum Phosphorus levels
Calcium-sensing receptors
Vitamin D receptors
FGF-23 receptors
The parathyroid gland contains which 3 important receptors?
Hypocalcemia
Hyperphosphatemia
Low calcitriol
3 stimuli that tells the parathyroid gland to release PTH?
Increase Ca2+ levels
Bones: release calcium into the blood
Kidneys: reabsorb calcium back into the blood
Intestines: absorb more calcium from food or medicines
Action of PTH on different parts of the body
Nephron loss
Impaired phosphate excretion = higher phosphate levels
More phosphate can complex with Ca2+ = lower Ca2+ levels
Impaired vitamin D activation
Active form of vitamin D is calcitriol
Impaired vitamin D activation = lower calcitriol levels
Calcitriol stimulates intestinal calcium absorption
Lower calcitriol = lower Ca2+ levels
How does CKD lead to hypocalcemia?
Primary
No underlying cause
Hyperactive Parathyroid gland
Secondary
With underlying cause
Usually CKD (nephron loss)
Progressive and starts at GFR < 60 mL/min/1.73 m2
May lead to hyperplasia of parathyroid gland
More PTH = higher Ca2+ levels → Hypercalcemia
Tertiary
Due to long-standing secondary hyperparathyroidism
Even if CKD is corrected, the parathyroid gland fails to return to normal and has become autonomous
More PTH
Differentiate the 3 types of hyperparathyroidism
converted from 25–(OH)–D3 via 1–alpha hydroxylase in the kidneys
precursor of calcitriol
Increase Ca2+ levels
Suppress PTH production
Action of calcitriol
Nephron loss
Lower total 1–alpha hydroxylase = lower calcitriol
Common in CKD 4 - 5
Lower sunlight exposure, dietary intake, and dermal synthesis of vitamin D
How does CKD lead to lower calcitriol?
osteocytes
FGF-23 is produced by?
Hyperphosphatemia
High calcitriol
High PTH
3 stimuli for FGF-23 production?
Decrease phosphate reabsorption
Inhibit PTH production
Inhibit 1-alpha hydroxylase = lower calcitriol levels
Action of FGF-23