CL for astigmatism - design & fitting
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
25 Terms
what are the types of astigmatism (2)
regular
residual
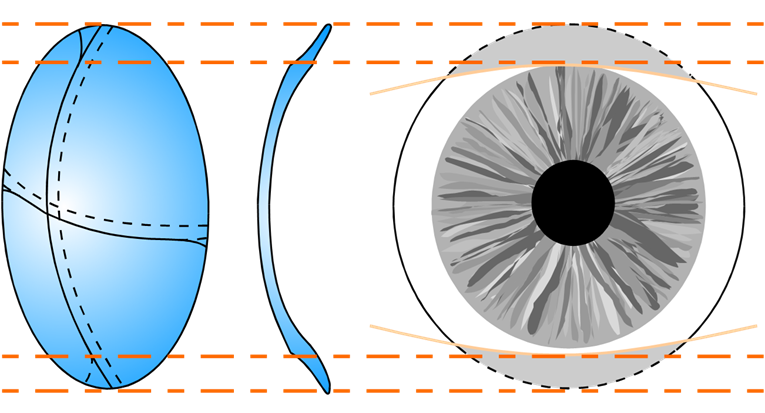
describe regular ocular astigmatism, its different meridians and how it is recorded (6)
represented across 2 meridians - 90 degrees apart
meridian descriptions: refractive power (diopters) and radius of curvature (mm) (keratometry)
astigmatism lies along power meridian - steepest meridian/smallest mm - meridian of greatest curvature/optical power
axis meridian - meridian of least curvature/optical power
Corneal astigmatism is an optical description
Corneal toricity is an anatomical description
describe what residual astigmatism is (2)
the astigmatic refractive error that is left uncorrected when a CL is already placed upon the cornea to correct the existing ametropia
Interpret as, 'with spherical CL' unless stated otherwise
explain how we can induce astigmatism and when this is likely (6)
Tilted &/or decentred CL
Toricity &/or bitoricity of CL - CL itself has a toric surface
CL mislocation (rotation &/or decentration) - laterally/clockwise/anticlockwise
Warpage &/or flexure of CL
This is likely in a SCL if the lens is rotated off axis
likely to be presentable in low VA / OR still uncorrected cyl
explain how astigmatism can be due to the physiological make up of the eye and when this is likely (8)
Un-neutralized corneal astigmatism - stock powers for CLs not coming in 0.25 steps and everything in between - if cornea has small amount of astigmatism it is not possible to correct as CL cyl start at -0.75 and go in 0.50 steps
Posterior corneal astigmatism
Lenticular astigmatism
Tilted crystalline lens
Refractive index anomalies
Oblique aberrations
Misalignment of ocular components
This is unlikely in a SCL unless small astigmatism is corrected with a spherical lens - SCL not creating any tear film behind the lens to correct astigmatism in any other way
explain why toric CLs need to be stabilized (5)
due to pressure of eye lids - lids exert pressure onto lens
without stabilization - lens would rotate
Maximise predictability of CL axis location - rx power needs to be at a specific axis - ensure lens is on axis
Make CL axis location independent of Rx
Maximise CL physiological performance
state the methods used for toric stabilization of SCL (5)
•Prism-ballast - most common
•Truncation - least utilized, more common in GP than SCL (only for customized SCL)
•Peri-ballast - popular similar to prism
•Double slab-off
•Reverse prism
SN: these methods also apply to gas permeable lenses
describe the prism-ballast method of lens stabilization (5)
inferior parr of lens is thickened by base down prism - 1 to 1.5D base-down
stabilized by prism-induced CL thickness differences - uses gravity and lower lid to stabilize
As it is thicker in inferior - that portion of CL has lower oxygen transmissibility
discomfort with CL-lid interaction - px can feel this thickness - especially if one eye has toric lens and one has SCL
prism ballast should not be close to pupil size - can induce prismatic effect for px
describe the truncation method of lens stabilization (4)
measure px lid margin - remove portion of lens that is more than lower lid margin
Truncation aligned with lower lid margin can create some CL stabilisation
Truncation can cause some discomfort and is not always successful
More patient visits can be required - Seldom used now
describe the peri-ballast method of lens stabilization (5)
Uses thickness ∆s as the stabilising component
Thinner superiorly, thicker inferiorly - prevents lid rotating in lower lid margin
Prism-free optic zone - no prismatic effect
Can cause discomfort with CL-lid interaction at the thicker inferior half
↓ CL O2 transmissibility in thicker regions
describe the double-slab off method of lens stabilization (6)
utilizes thin and thick zones - thinner zones have a higher oxygen permeability as opposed to thicker zones - Thin zone superiorly & inferiorly
creates thicker zones in the palprebral apperture - when lens rotates thick part knocks on lid to not allow it to rotate
thicker zones - prevent it from going under lid - lid forces (upper & lower) maintain orientation
Better comfort due to ↓ CL thickness
CL is symmetrical
Can exhibit less rotational stability is low spheres, WTR astigmatism and less successful on px with lid laxity - loose lids - elderly px
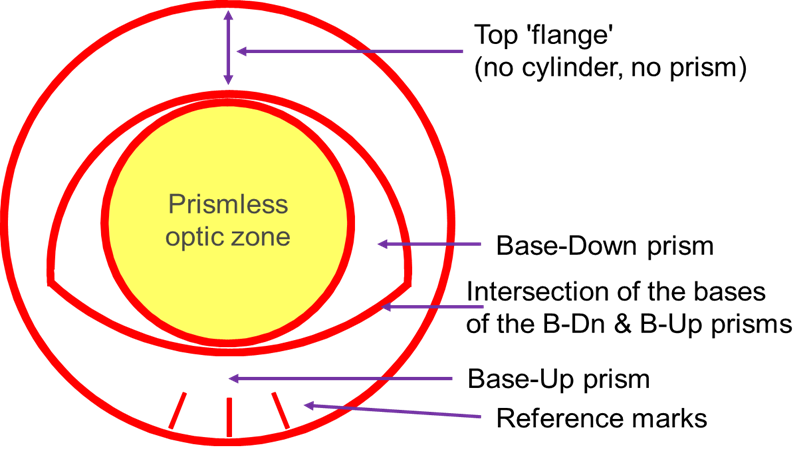
describe the reverse prism method of lens stabilization (2)
utilizes both base up (inferiorly on lower lid margin) and base down prisms (palprebal apperture)
Result in thinner and more comfortable lenses than just the thicker base down prism ballast design
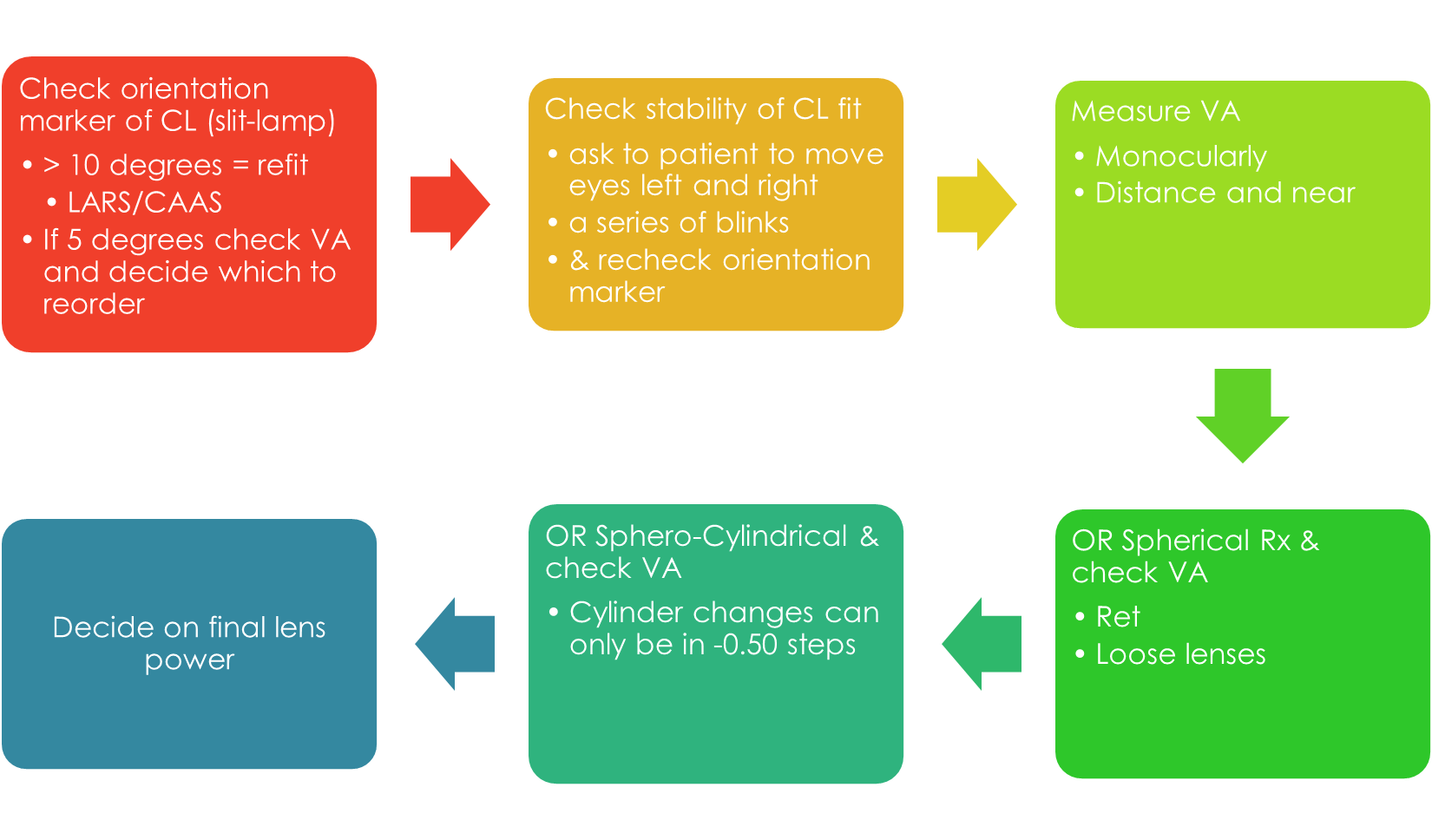
explain how we assess the orientation of the CL (3)
Done by observing reference points or marks on the CL to assess CL orientation in situ
not all companies have the same markers - if a px has tight lids, markers may escape under top lid so know where the markers are before inserting them into eye
some companies have 1 marker at 6oclock, 2 at 12 and 6, 3 at 6 etc.. - not expected to know them all
when is it applicable to fit a px with a toric CL (4)
px with refractive astigmatism - if cyl is more than 0.75 we advise toric lenses
If spherical SCLs failed to mask corneal astigmatism - unsatisfactory VA with best sphere
px may switch to toric if - GP CLs leave residual astigmatism due to physiological aspects - GP CLs cause discomfort
if px has a large rx (-12/-8 etc) - they won’t have perfected vision in gls – not necessary to incorporate all of cyl power as it won’t have impact on vision
explain how we select a trial for toric CLs (6)
Measure Rx & vertex distance
Select CL power (BVP) to match corneal-plane Rx
Vertex correct each meridian >4D
Select BOZR &/or TD — {(K1 + K2)/2} +0.9mm — HVID +2mm
Always lowest minus possible - for CYL component as only come in 0.50 steps (if px has a -1.00 cyl we would select a -0.75 cyl not -1.25 - select lowest minus)
5 degrees in refraction show patient choice of 10 degrees either way - E.g. refraction 45, decide on preference between 40 or 50 in trial frame
what do the stock powers and axis go up in for toric lenses (4)
start at -0.75 and go up in 0.50 steps to -2.25
axis goes up in 10 degree steps
some companies do go above -2-.25 to the likes of to -5.75 - in this case the axis do then start going up in 5 degree steps - however this is not the norm
Online calculators can generate the order for u from px prescription
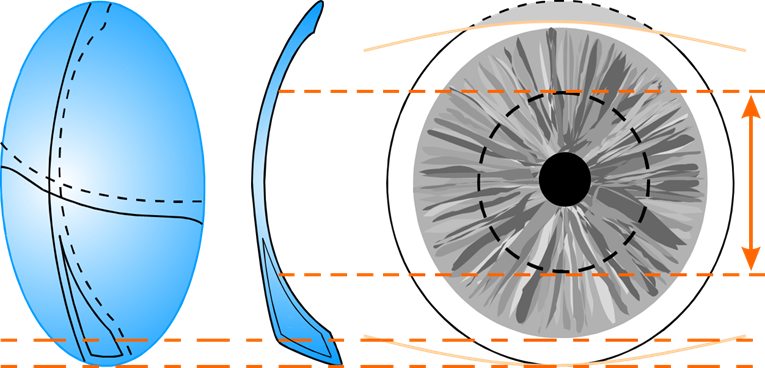
what makes a good, tight and loose fit for toric CL
Good fit:
◦Full corneal coverage, good centration & movement, quick reorientation after blinking/lateral gaze
◦Full corneal coverage, 0.2 - 0.5 mm movement
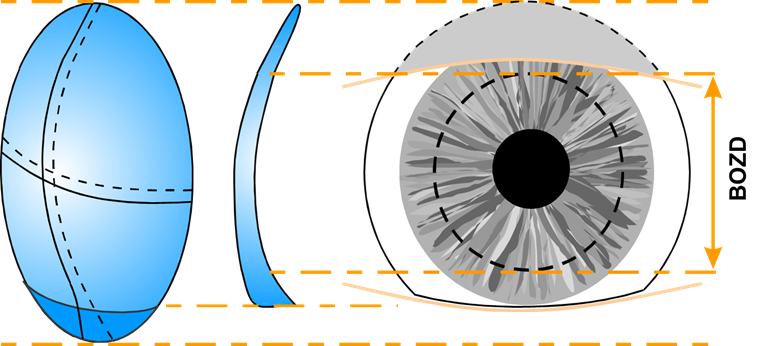
Tight fit:
◦Good centration, initially comfortable, little or no movement. Slow reorientation if mislocated
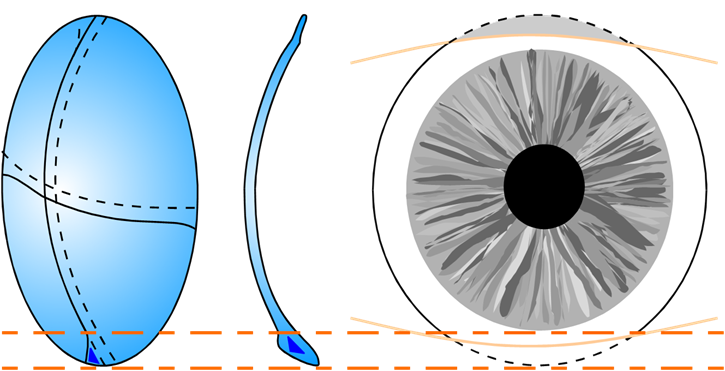
Loose fit:
◦Excessive movement, poor centration,
uncomfortable.
◦CL orientation unstable & inconsistent
what do the markers on the CL show and how do we assess them (3)
CL marks are for reference only, they do not indicate the axes of cylinder optically, they of no particular significance
Measure rotation using: narrow slit-lamp beam with protractor scale
align the beam with the marker and read the angle off the scale of slit lamp
how do we interpret the orientation of markers what does it mean - what do we do with this information (5)
if marker is exactly at 6 o clock - orientation is perfect no need to re order trial lens
if the orientation is 4 degrees or less - cannot order new trial as only go up in 10 degree steps - if 5 or over then need to alter lens - rotation is too much for px visual outcome using:
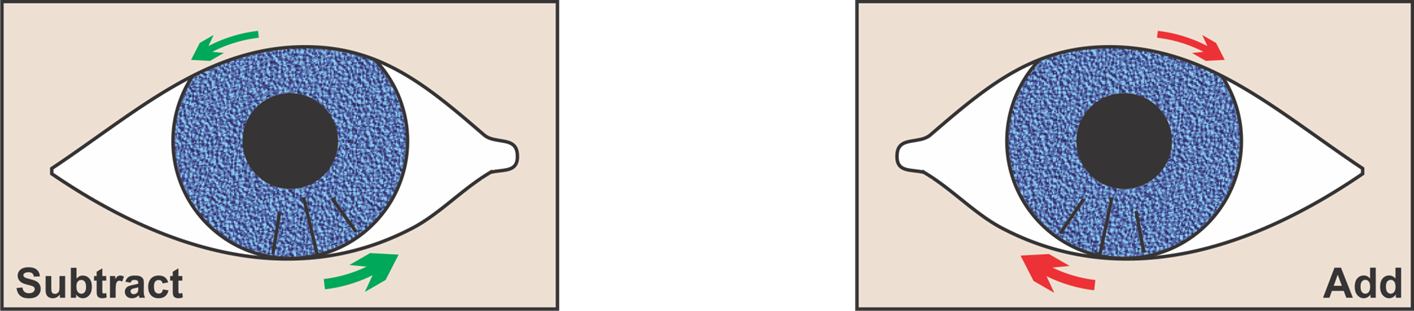
LARS - left = add / right = subtract
if the marker is 15 degrees to the RIGHT from where it should be (6 o clock position) - then subtract 15 from the axis of trial lens - eg if trial lens was 70 - 15 = 65, however axis come in 10 degree steps so it would be 60.
if the marker was 15 degrees to the LEFT - add 15 to the trial lens axis - if trial lens axis was 180 add 15 - would be 15 but would order 10 as only come in 10 degree steps
what patients do not do well with toric CL and why (4)
Low spherical component, esp. WTR astigmatism: e.g. +0.25 / –2.25 x 180
Oblique cylinders: e.g. –2.00 / –1.75 x 50
above 2 is due to - the rotation and stability of CL – more difficult to generate a stable lens due to curvature
High cylinders: any movement off-axis will generate poor vision - e.g. +2.00 / –5.75 x 80
what should we do if the lens rotates again on the new trial order (5)
LEAVE IT
Once you have compensated for the rotation in the first trial, the second lens should fit the same orientation - it will still be rotated - not at 6 o clock - it is meant to be rotated - only now the rotation has already been accounted for
The lens acts as intended (based on spectacle refraction) even if the reference marker is rotated
This only holds true if the rotation is the SAME as the first trial
This is often due to a persons anterior eye surface and not the lens design
power crosses do at home on paper notes - but key points (6)
only need to vertex correct if either meridian is greater than 4
use the formula to vertex correct
draw power crosses to help
remember if the stock power for cyl is over -2.25 we can now offer axis in 5 degree steps - would show px either one and ask which one they prefer
if the calculation says -1.00 cyl or 172 axis - remember things like cyl only starts in -0.75 so that’s what would acc be ordered and then 170 for axis as axis only go in 10 degree steps
plus powers become more plus - minus powers become more minus - due to focal lengths
when do we need to over refract for toric lenses
Only over-refract a lens that has less than 5 degrees rotation - to determine if optimal power
if u try to OR a lens that has not been compensated for - no point - only OR on a compensated lens
explain OR of a toric lens (6)
Use loose lenses in a trial frame
Check sphere power - BVS
Check axis and cylindrical power - JCC
Ensure if there is an over-refraction that the change can be accommodated in a new lens - 0.50 jumps in soft lenses - use the 0.50 JCC as no point using the 0.25 ones
10 degree jumps in soft lenses
Consider extended range if the astigmatism is not generating the BCVA in spectacles - communicate this may take a while to the px
routine for toric SCL assessment