Endocrine Exam 1 Dr.A
1/218
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
219 Terms
hormone definition
biochemical substances released to interstital fluid to regulate cell's biological activity
what is an axis
a series of linked hormonal responses that cause change in the synthesis of other hormones
how are peptide hormones synthesized
they're gene encoded and are produced through transcription and translation
how are steroid hormones synthesized
steroid hormones are produced enzymatically
but you still need to production of enzyme proteins
storage of peptide vs steroid hormones
peptide- secretory granules accumulate pro-hormones
steroids- little/no storage but can store cholesterol precursor
solubility of peptide vs steroid hormones
peptides are soluble in water
steroids are soluble in lipids
transport of peptide vs steroid hormones
peptides are soluble and travel through plasma
steroids need carrie proteins in the plasma and cytoplasm
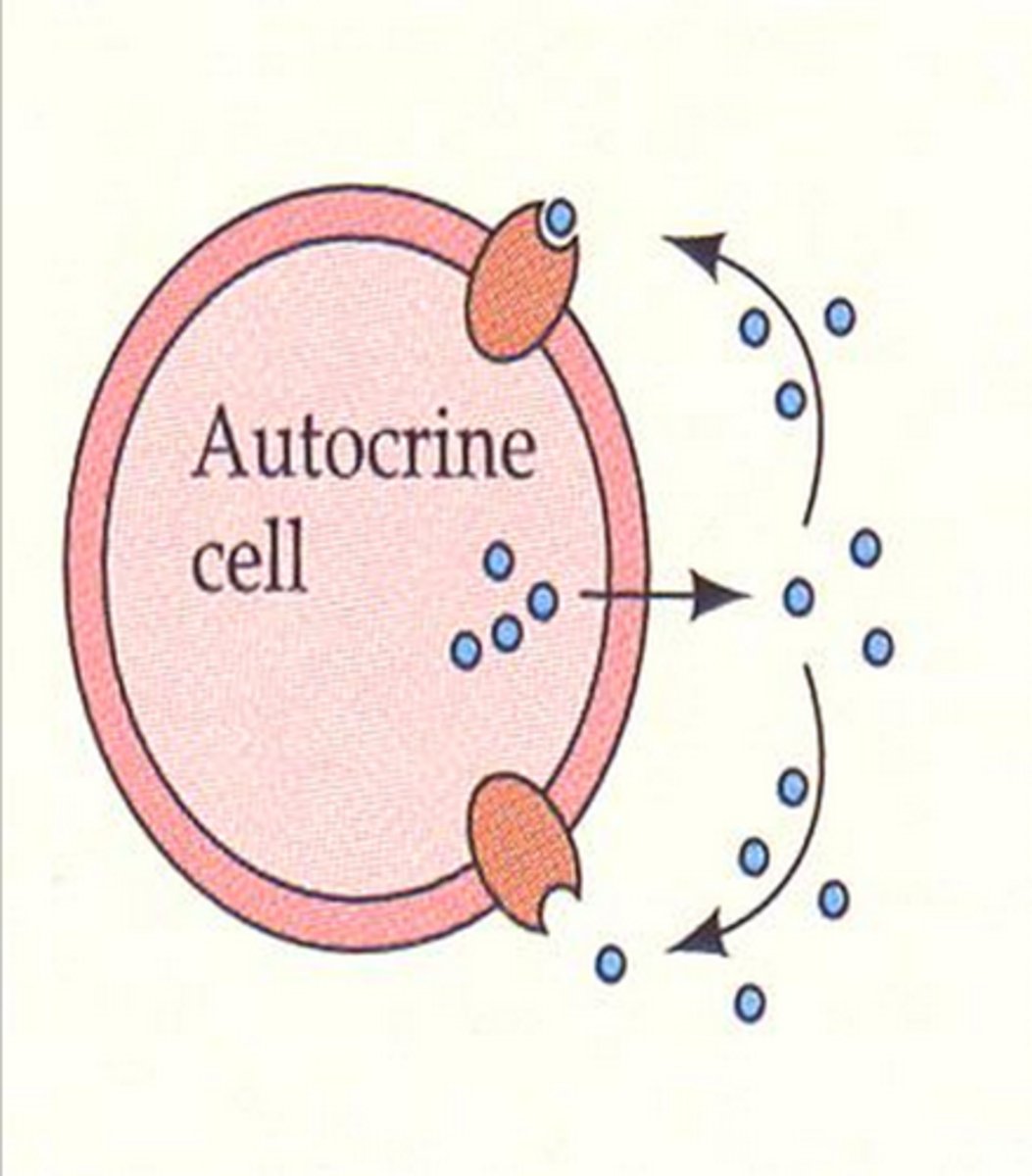
what are the 3 types of signaling regulation
1. autocrine
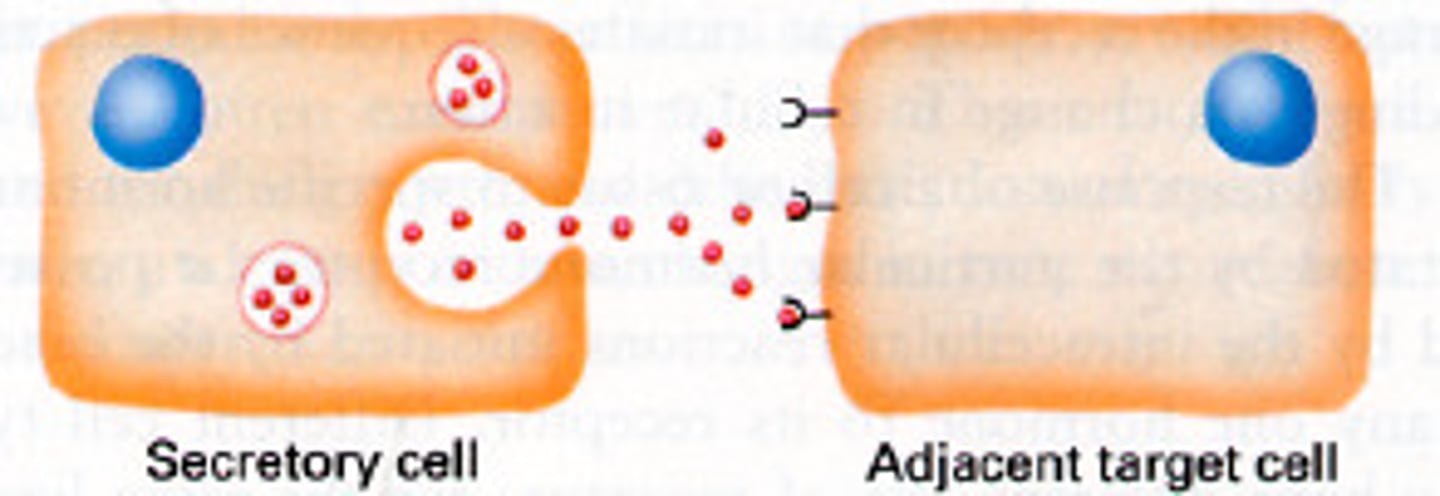
2. paracine
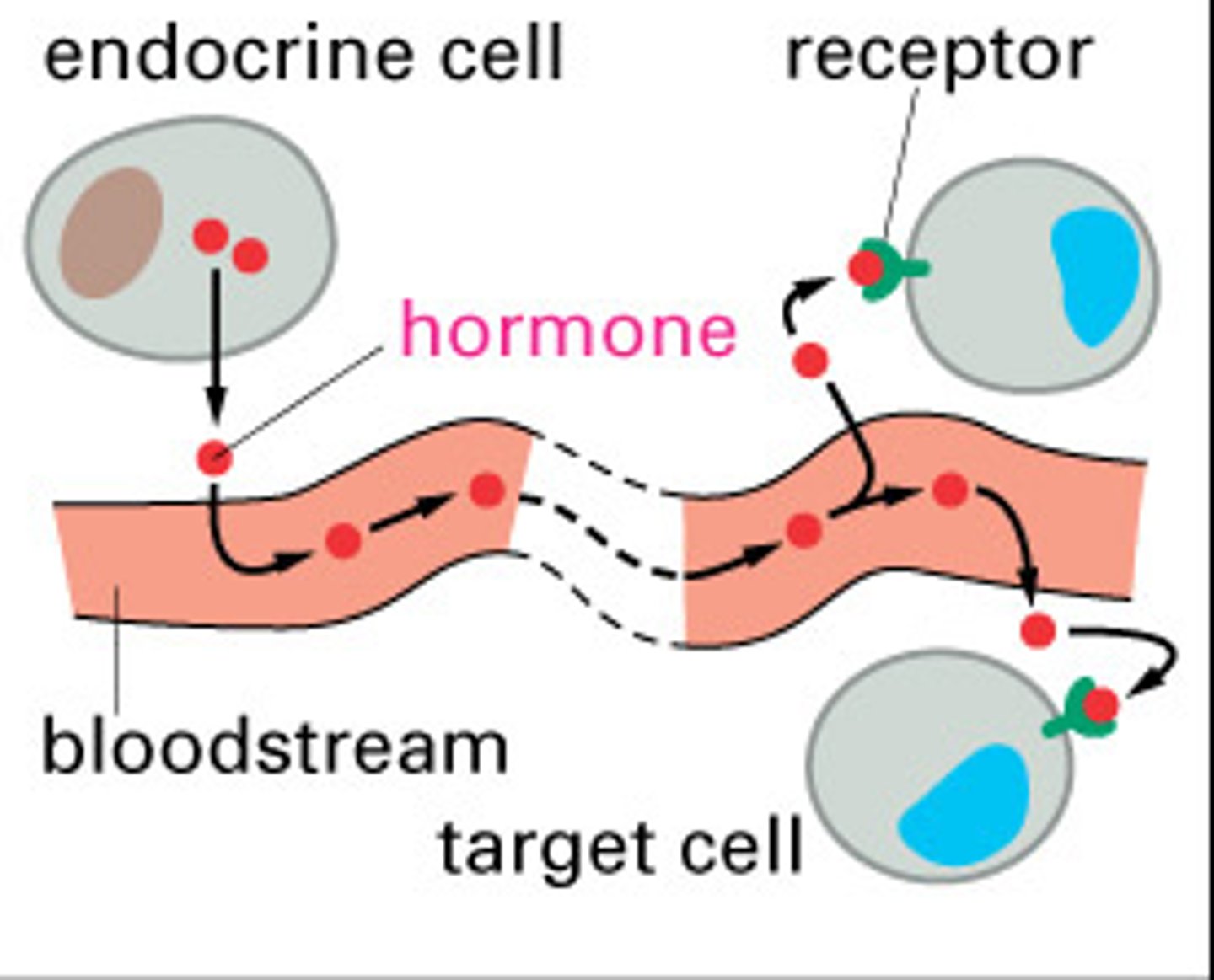
3. endorine
autocrine regulation
cells producing hormone respond to that same hormone
paracrine regulation
cells near producer cell respond to hormone (don't travel a long distance)
endocrine regulation
hormone travels (via blood) to distant responder
endocrine vs nervous signaling- response time
endocrine has a slower response time
have to synthesize hormone and transport it through blood
endocrine vs nervous signaling- nature of response
endocrine has synthetic reactions (new mRNAs & new proteins)
nervous signaling is membrane depolarization or contraction
endocrine vs nervous signaling- duration
endocrine duration is longer
endocrine vs nervous signaling- transport route
endocrine: blood stream
nervous: axon + synapse
length of peptide hormone structure
can be very diverse in length- a few amino acids to 100+ amino acids
what is unqiue about the amino acid structure of peptide hormones?
there is no iniator methionine/AUG codon
proteolytic processing of peptide hormones
some peptide hormones are produced by cleaving precursor proteins
for example, POMC becomes ACTH and MSH
if there is not enough ACTH, what happens to MSH as a result
increase in MSH because there will be more POMC cleaving

steroid hormone structure
complex carbon ring structure derived from cholesterol
how is information communicated from a hormone
peptide hormone can bind on the extracellular domain receptor and transfer the information across the membrane (hormone entry into the cell isn't absolutely required)
what are the 2 ways that enzyme activation can occur when a hormone binds to its receptor
receptor with activity
or
receptor associated with proteins with enzyme activity
what is the general effect of hormone binding to extracellular receptors
cascade event where one binding triggers repeated enzyme activity
GPCR + peptide hormone effect
induces dissociation of trimeric G protein
signal is transfered and activates enzyme with production of cAMP (2nd messenger)
receptor tyrosine kinase + peptide hormone effect
tyrosine kinase activity can be as aprt of the receptor or a protein associated with the receptor
the hormone binds which casues receptor dimerization --> kinase activation
autophosphorylation or phosphorylation of another kinase
what are the 2 types of intracellular receptors
cytoplasmic or nuclear
2 domains of intracellular receptors
hormone binding domain and DNA binding domain
what happens when the hormone binds to the hormon-binding domain of intracellular receptors
-hormone causes receptor conformation change -> releases HSP (heat shock protein)
-receptor and hormone translocate to nucleus and activate transcription
role of DNA binding domain of intracellular receptors
allow receptor & hormone to bind DNA for transcription
where is the receptor for steroids & liophilic hormones usually found
in the cytoplasm complexed with HSP
HPA axis- anterior pituitary path
releasing/inhibiting hormone from the hypothalamus regulate production of "tropic" hormone in the AP
HPA axis- posterior pituitary path
hormone production occurs in the hypothalamus but is released from PP
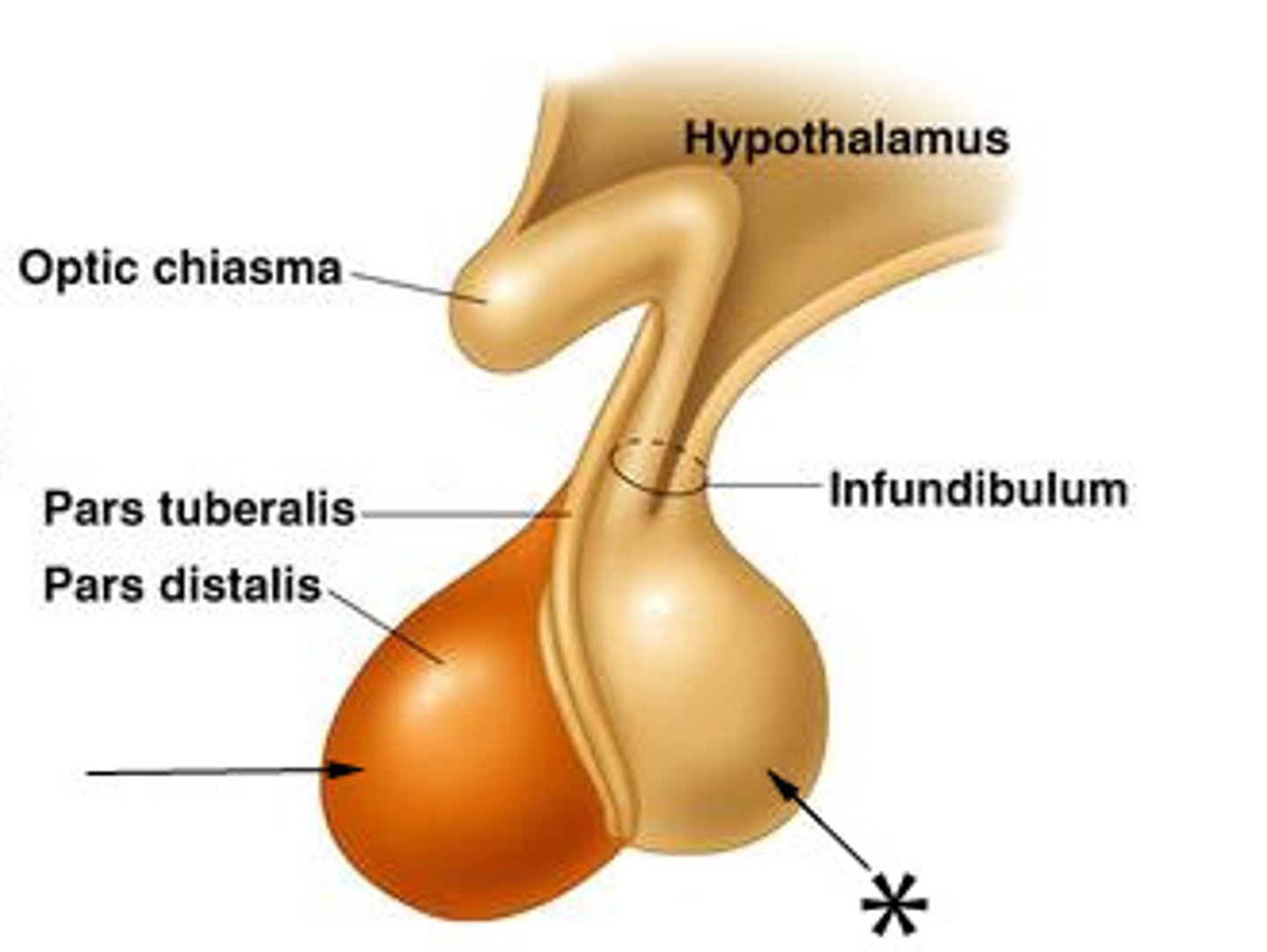
another name for pituitary
hypophysis
another name for the anterior pituitary
adenohypophysis
tropic hormone
causes production of effector hormone in target endocrine glands (i.e. adrenal)
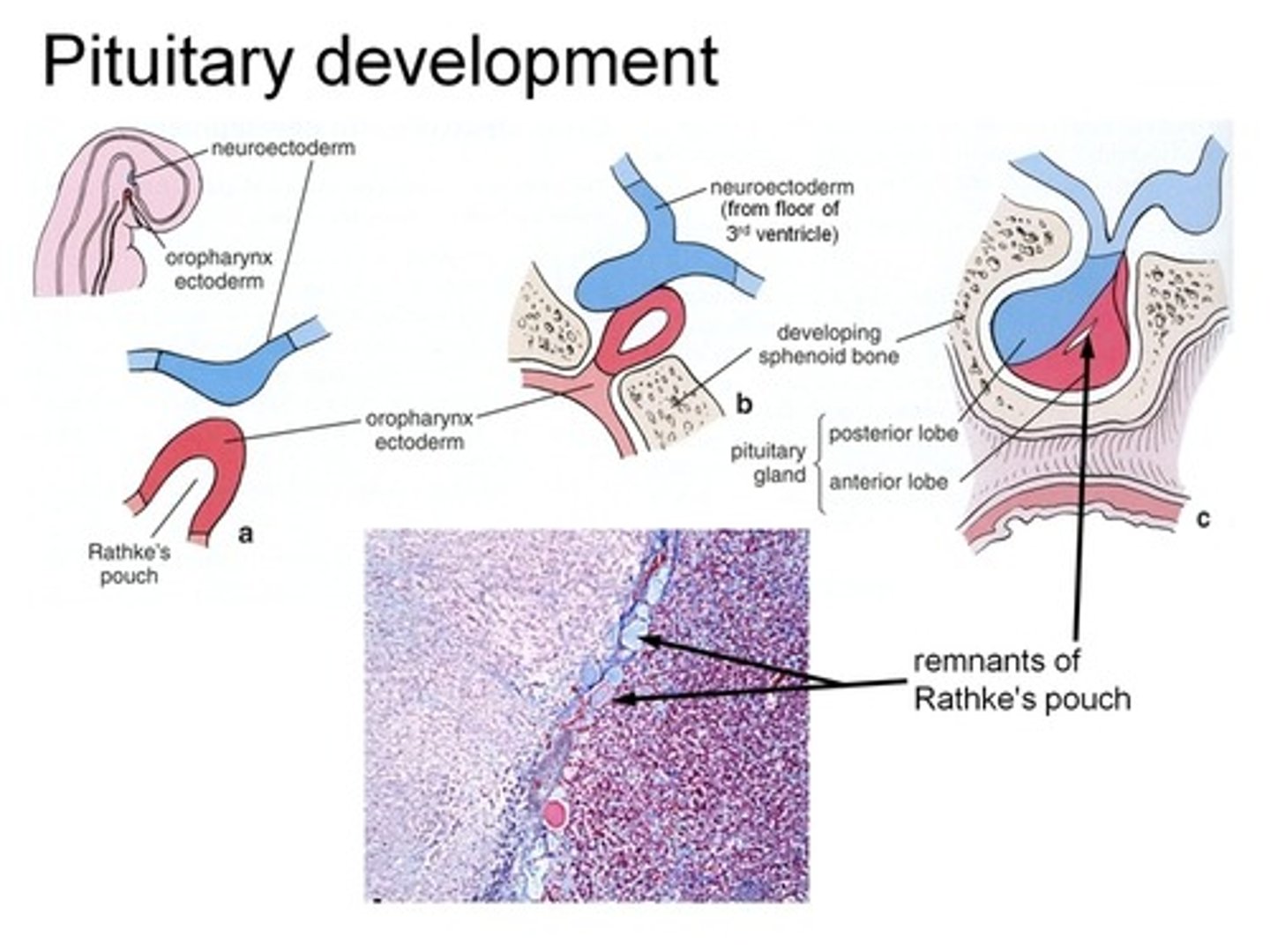
how is the anterior pituitary formed?
embryonic origin from the Rathke's pouch
tubular invagination of pharyngeal epithelium
arises independent of the hypothalamus
how is the aneterior pituitary connected to the hypothalamus
via the portal system
another name for posterior pituitary
neurohypophysis
origin of posterior pituitary
comes from embryonic brain and is an ouotgrowth of the hypothalamus
retains axonal tracts coming from the hypothalamus
how is the posterior pituitary connected to the hypothalamus
physically connected
hormones directly delivered here
have neurons/nuclei that travel between them
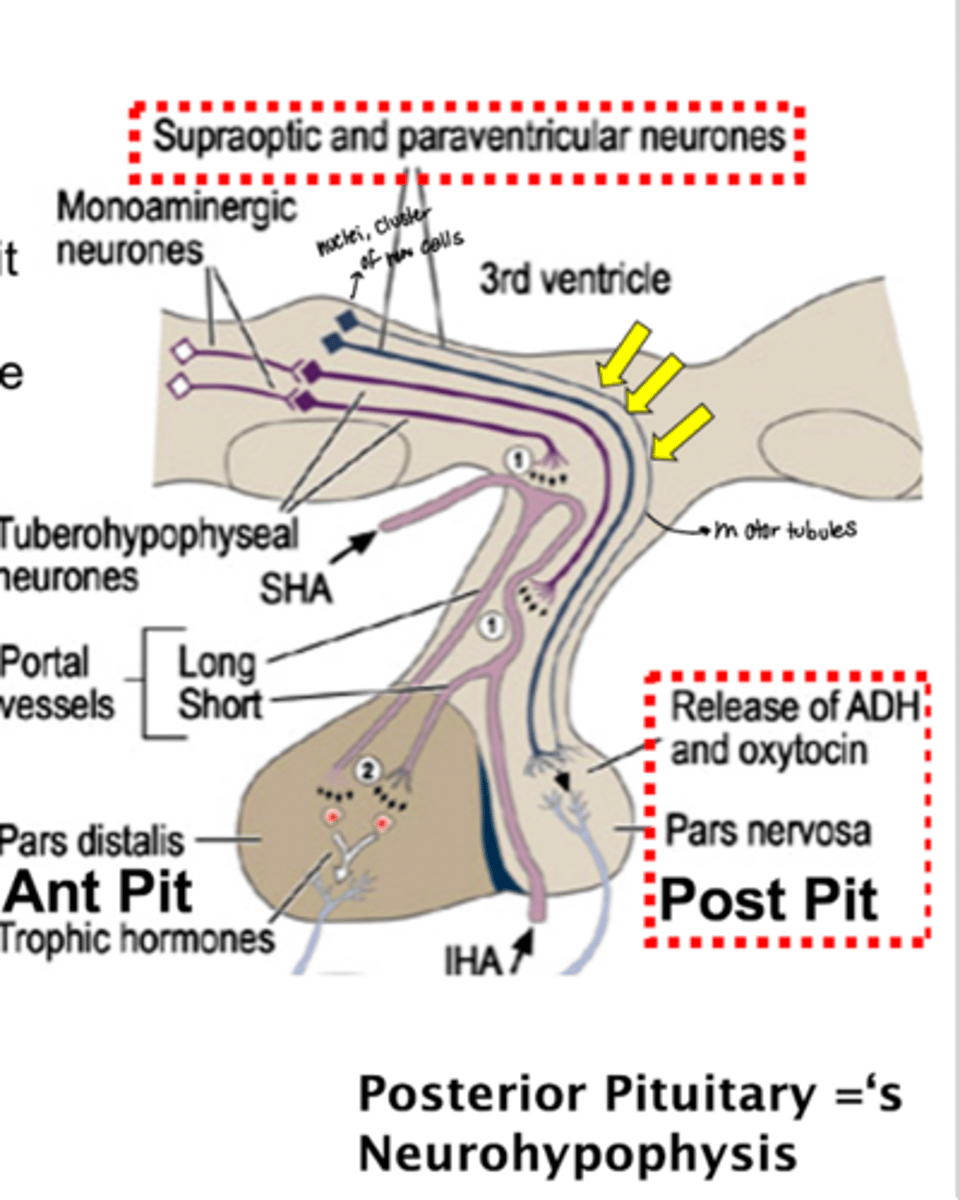
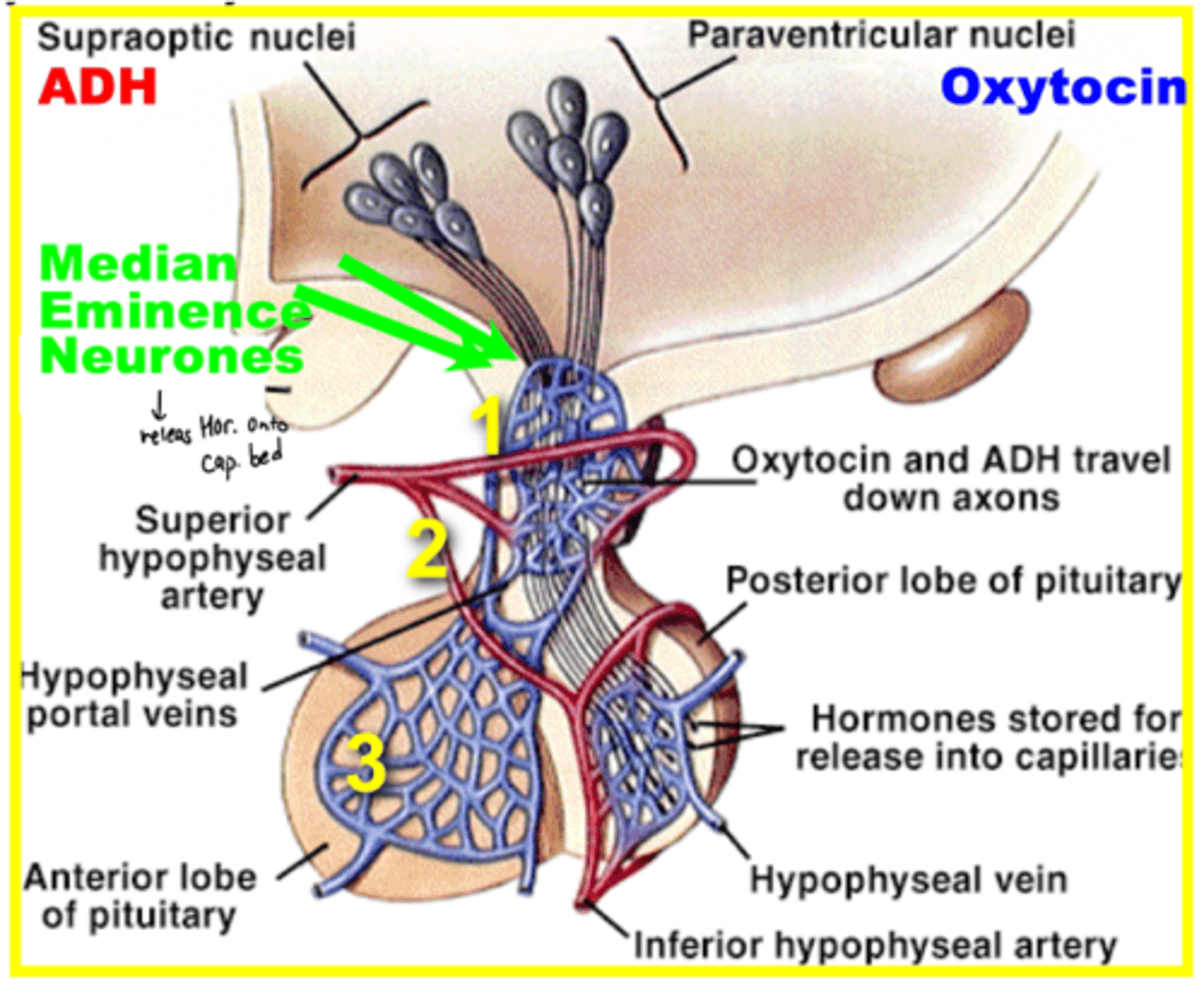
what cells produce ADH in the PP
supraoptic nuclei
what cells produce oxytocin in the PP
paraventricular nuceli
how are hormones made and then sent to the posterior pituitary from the hypothalamus
1. synthesis in neuron cell body on eER
2. packaged into secretory grancules
3. transported along axon
4. released onto surface of posterior pituitary
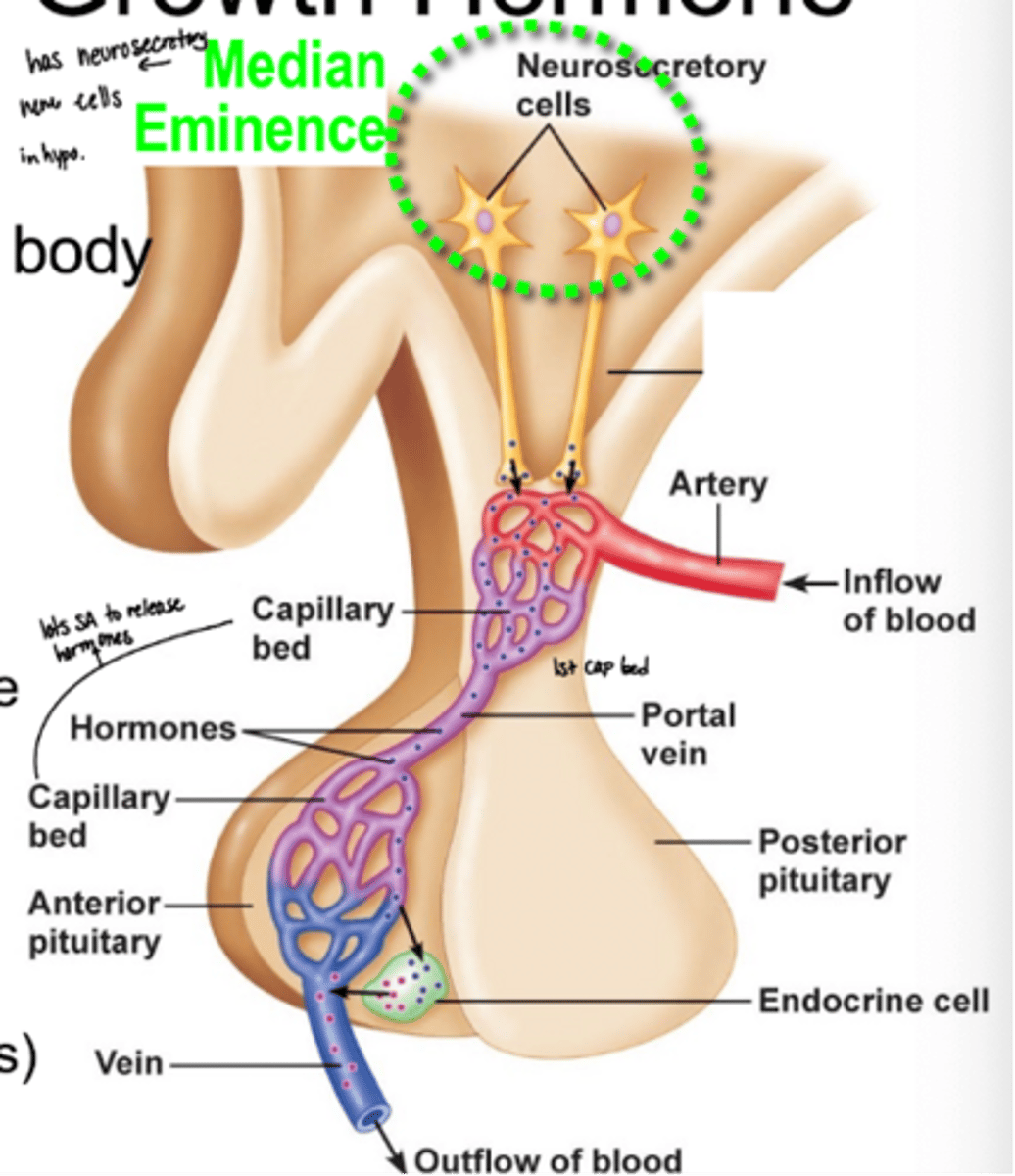
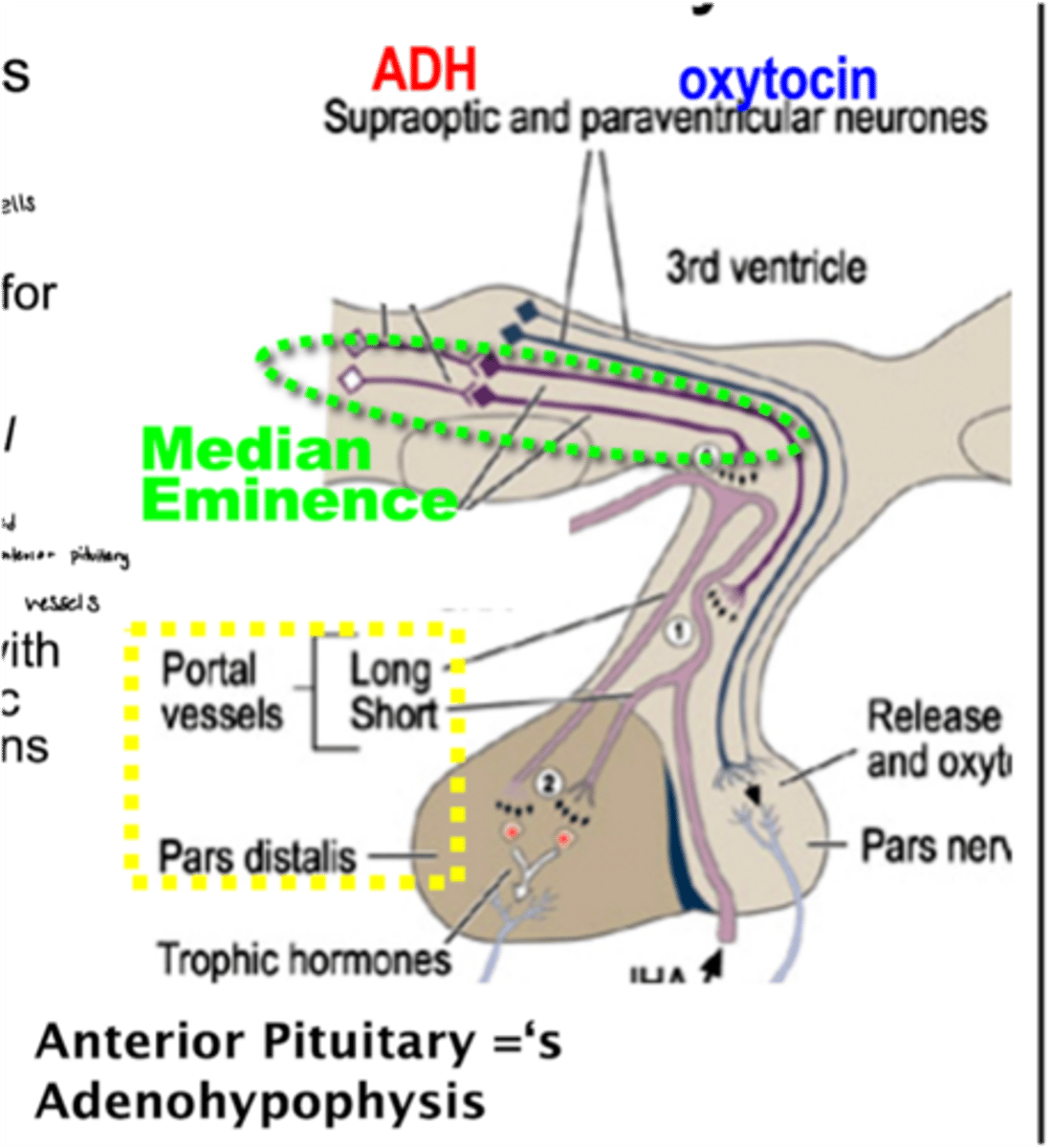
median eminance
multiple hormones are made here for delivery to the anterior pituitary
how are hormones made and then sent to the anterior pituitary from the hypothalamus
1. made in the median eminence
2. travel through the hypothalamic-hypophysial portal system
3. arrive at anterior pituitary
4. AP responds with production & release of tropic hormones
what controls how much hormone is produced from the anterior pituitary
the hormone produced from the hypothalamus that travels to the AP
signaling requirement for the hypothalamic-hypophysial portal system
hormones must be able to cross the BBB which is formed by cell-cell junctions
what is the portal system
blood vessel cells with fewer tight junction which allows for more movement across the vessel wall
(think hypothal--> AP)
unique arrangement of blood vessels in the hypothalamic hypophysial portal system
1. capillaries (hypothalamus)
2. veins (connecting stalk)
3. capillaries (anterior pit)
which 2 hormones are hypothalamus-posterior pituitary hormones
ADH (vasopressin) and oxytocin
which hormones are hypothalamus- anterior pituitary hormones
GnRH --> FSH + LH
what are the 3 diagnostic hormones and where are they made
-GHRH
-TRH
-CRH
all made in the hypothalamus and go to the AP
potential problems with the clinical use of diagnostic hypothalamic hormones
-isolate, puroify, & stabilize hormones (deliver peptide across BBB is hard)
-delivery of sufficient amount to traget cell
-downstream effector hormone may be more specific (may not be specific dor the hormone you want to target)
what downstream effect does CRH (corticotropin releasing hromone) have?
CRH --> POMC --> ACTH
therapeutic hypothalamic hormones that go to the posterior pituitary
ADH and oxytocin
therapeutic hypothalamic hormones that go to the anterior pituitary
GnRH (or synthetic analogs) and SRIF (somatotropin release- inhibiting factor/ somatostatin)
how is the PP and hypothalamus connected
there is an ANATOMICAL CONNECTION between the 2
synthesis steps of ADH/vasopressin
1. 9aa peptide acts as a signal sequence that directs the protein to the surface of the ER
-made as a precurosr protein in the supraoptic nuclei of the hypothalamus
-precursor transported+ processed along nerve tract to PP
2. signal peptidase cuts the end off
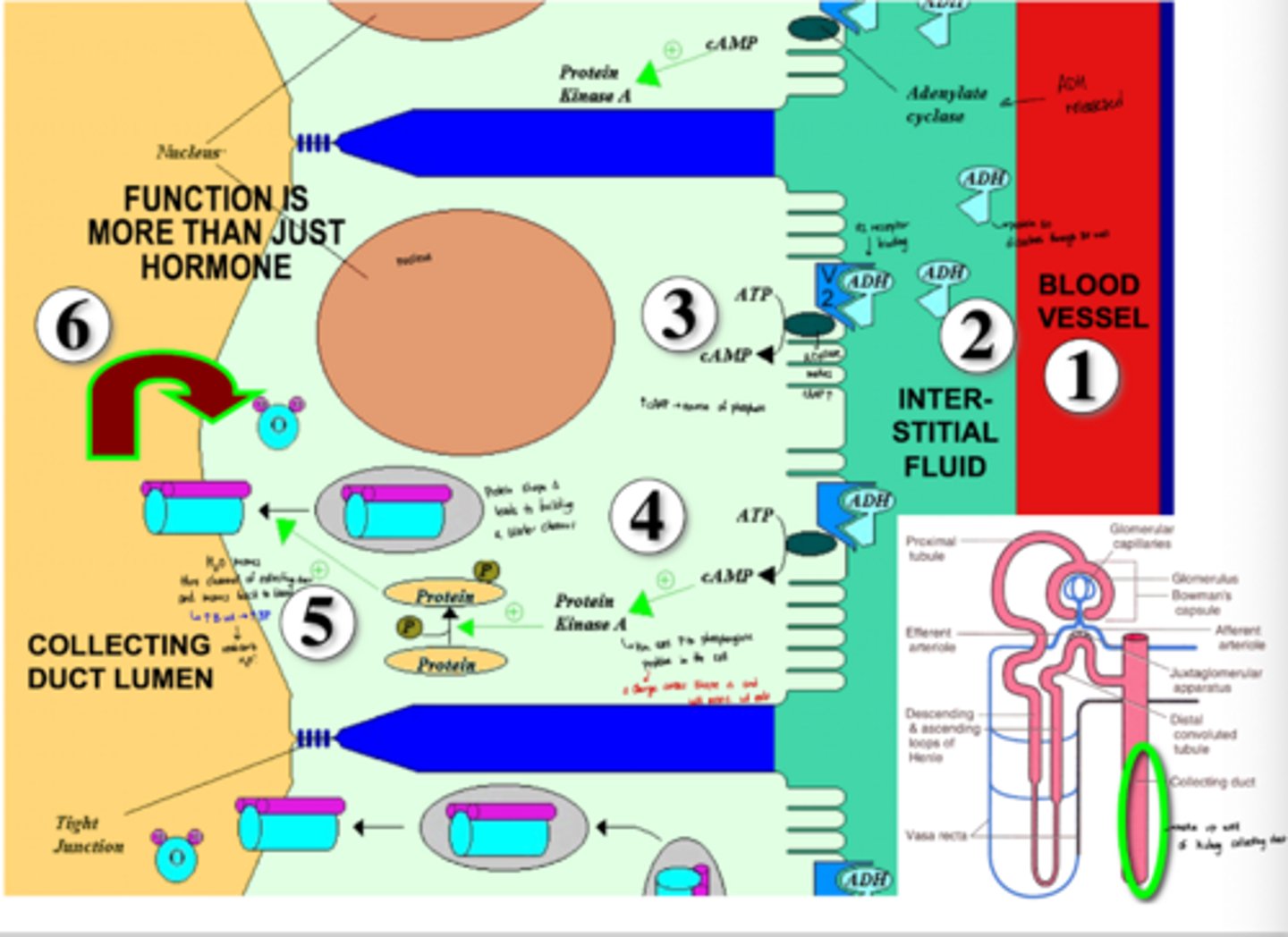
what are the 2 types of ADH receptors, where are they and what do they do?
V1: in blood vessel smooth muscle for contraction
V2: in kidney tubule cells to help with water recovery
how does ADH binding to V2 cause feedback regulation?
increase in BP has negative feedback on ADH production
V2 + ADH binding downstream steps
-they bind and adenyl cyclase is actived
-adenyl cyclase increases phosphate sources
-protein kinase A then uses phophates to phosphorylate proteins in the cell
-phosphorylated proteins change shape and aggregate
-aggregation of proteins water water channels in the kidney cell membrane
-more water is reabsorbed through the lumen and the blood volume increases
-increase in blood volume increases BP
ethanol effect on ADH
inhibits ADH release which causes dehydration/hangover
nicotine, morphine, and barbiturate effect on ADH
increase ADH release
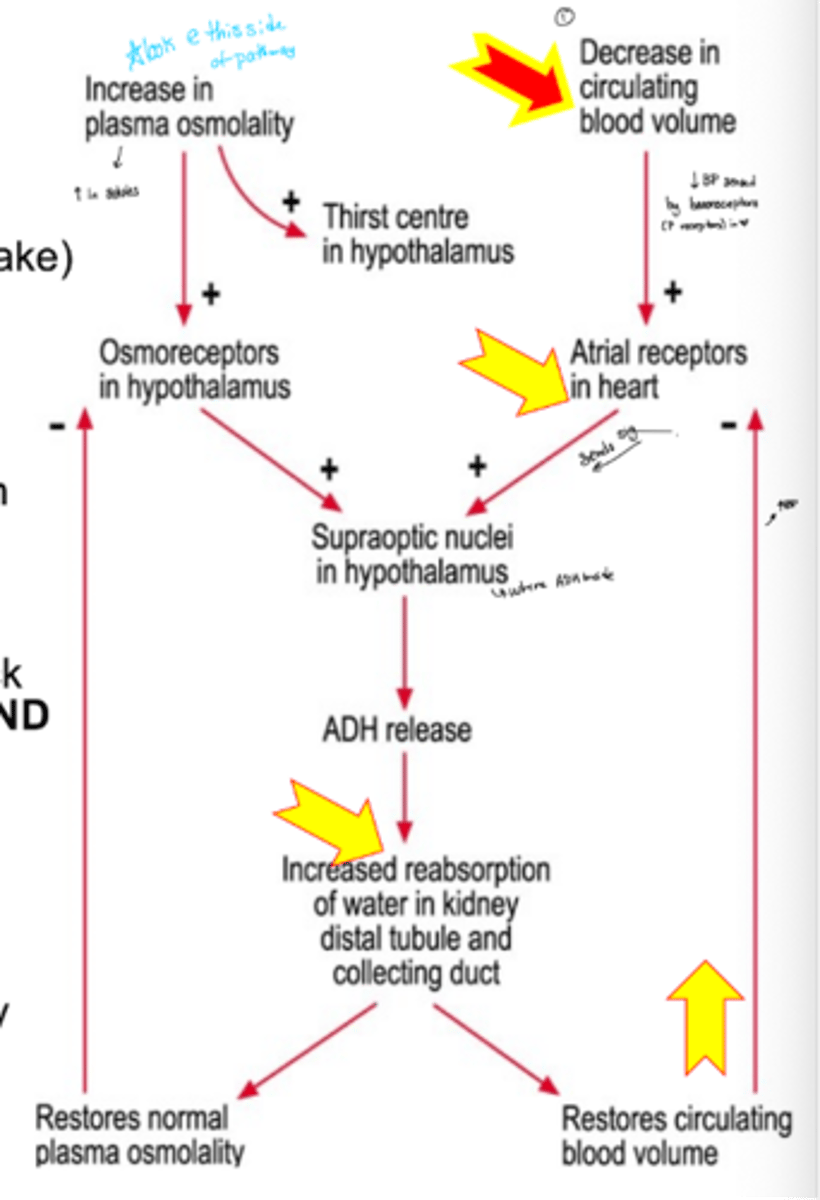
ADH steps with a decrease in osmotic pressure
osmotic pressure is low due to insufficient water intake
§ Sensed by osmoreceptors in the hypothalamus
§ Supraoptic nuclei in hypothalamus releases ADH
§ Increased reabsorption of water in kidney restores osmolality
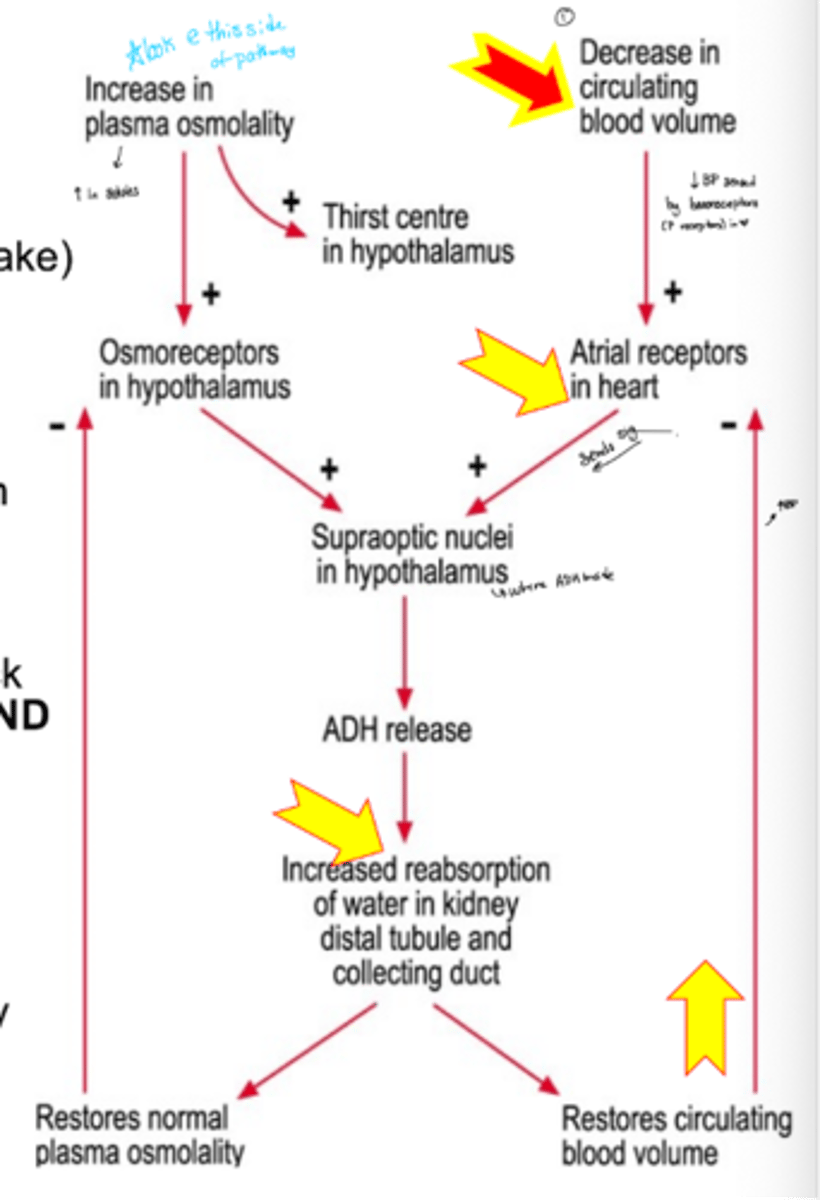
ADH steps with a decreased blood pressure
§ Sensed by baroreceptors in the heart
§ Signal sent to supraoptic nuclei in hypothalamus
§ Supraoptic nuclei releases ADH
§ Water is reabsorbed which increases blood volume/ BP
clinical application of ADG
diabetes insipidus
o Very low ADH--> high urine output--> high thirst
o Successfully treated if ~20% normal ADH level restored with a synthetic peptide
what is oxytocin and what does it do?
it is a small peptide hormone
has the ability to increase uterine muscle contraction (bind to smooth muscle in uterus)
oxytocin in pregnancy
-induces labor late in pregnancy by increasing receptors on uterine smooth muscle
-contraction of breast myoepithelial cells to promote milk secretion
how is oxytocin peripherally produced?
produced late in pregnancy by the placenta
local concentration in uterus>>> maternal circulating hormones
how is oxytocin produced in the brain?
it is synthesized by the hypothalamus' paraventricular nuclei
which route of administration can not be used with oxytocin
it is a peptide so not PO
MOA of oxytocin in clinical uses
can be used for contraction in labor and delivery
it is being investigated for its neuromodulation effects in autism therapy
what does GnRH stand for?
gonadotropin releasing hormone
how is GnRH made in the body
made in the hypothalamus from a pre-prohormone precursor
where does GnRH have an effect?
stimulates the GnRH receptor on gonadotrope cells in the anterior pituitary
downstream effect of GnRH
binds to receptor inAP
activates the 2nd messenger system
LH + FSH (gonadotrope hormones) are produced
what does the amount of LH or FSH depend on?
the frequency and level of GnRH
what is the pattern of GnRH release like?
its release is pulsatile which means it causes oscillating levels in hormonal delivery (15 mins per 90 mins)
amplitude + frequency increase with puberty
how does receptor attenuation occur?
GnRH receptors become desensitizes when there are constant high levels of GnRH instead of the normal pulsatile release
what is the effect of GnRH receptor attenuation?
receptor activity becomes down-regulated
cells dependent on testosterone and estrogen for mitotic stimulus are then decreased
when is continuous high therapeutic levels of GnRH advantageous?
o Advantage if desired effect is to decrease secretion of FSH and LH
§ Treat with synthetic agonist with a longer half life
§ Eventually causes attenuation of GnRH receptor on membrane on ant pit cells
§ Attenuation is not immediate - may need several days of high GnRH therapy
what are the initial consequences of high GnRH treatment (trying to achieve receptor attenuation)?
initially causes rapid cell growth before attenuation occurs then cells decrease once the receptor is desensitized
how can GnRH be used for amenorrhea?
GnRH can be used to increase gonadotrope hormones (FSH and LH)
causes induction of ovulatiion
**only if pituitary has normal function and the ovary is responsive
how is GnRH administered for amenorrhea?
pulsed IV delivery
cannot be given at a constant high because this will cause receptor attenuation
how do we treat gonadotrope-dependent cancers with GnRH?
through "pharmacological castration" where GnRH receptors are attenuated so they produce less gonadotrooins
how do we treat emdometriosis with GnRH?
we can attentuate receptors to decrease the amount of gonadotropin released
decreases the size and pain associated with excess cell grwoth
leuprolide
GnRH peptide agonist analog used to cause attenuation and decrease FSH/LH secretion
how is leuprolide structurally different from GnRH
has a D-Leu instead of L-Leu
Conformation change makes it less recognizable by breakdown enzymes
function of female FSH
ovarian follicle growth & synthesis of estrogen
function of male FSH
sperm development by supporting Sertoli cell function
steroli cell
support cell to HELP stimulate sperm production
function of female LH
ovulation & synthesis of progesterone (& continued estrogen) within corpus luteum
function of male LH
testosterone synthesis in Leydig cells
FSH + LH structure
made of 2 polypeptide chains with same alpha but different beta chains
each chain is modified post-translationally
how are FSH and LH different
they have different beta chains which determines their identity
how are FSH and LH chains modified post-translationally
Added carbohydrate groups that affect hormone solubility, stability & recognition by receptor
where are LH and FSH receptors
on the cell surfaces in the testes and ovaries
describe the structure of FSH and LH receptors
have an exttracellular domain made of beta sheets
7TMR
receptors are specific for FSH or LH
are GPCR coudpled do adenyl cyclase --> cAMP
why are FSH and LH administered via injection?
Difficult to prevent digestive tract breakdown of orally administered peptide/protein compound
what are the 2 ways that AP hormones can be regulated?
via hypothalamic relseasing factors (hormones) OR inhibiting factors (hormones) both from the median eminence (neurosecretory cells in the hypothalamus)