lecture 1 assistive devices and application
1/50
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
51 Terms
assistive devices (AD)
- parallel bars
- walkers
- crutches
- canes
parallel bars provide
greatest stability/max support with patients with decrease standing balance, fear/anxiety
parallel bars measurement and fit while standing:
- 2 inch lateral clearance on each side of hips
- height of bars to greater trochanters or wrist crease (ulnar styloid process
- elbow flexion of 20-25 degrees while holding bars
parallel bars abbreviation
// Bars
walkers types
PUW (pick up walker), FWW (front wheel walker), HW (hemiwalker)
walkers provide
maximum stability and support with mobility
disadvantage of walkers
- more stability means compromised mobility which leads to decrease in ambulation speed
- impedes normal flow of gait pattern
- difficult to use on stairs
- spatial awareness and transfer difficulty
measurement and fit of walker
- handles to wrist crease (ulnar styloid process)
- 20-25 degree elbow flexion
- stand as upright as possible, shoulders relaxed, head up
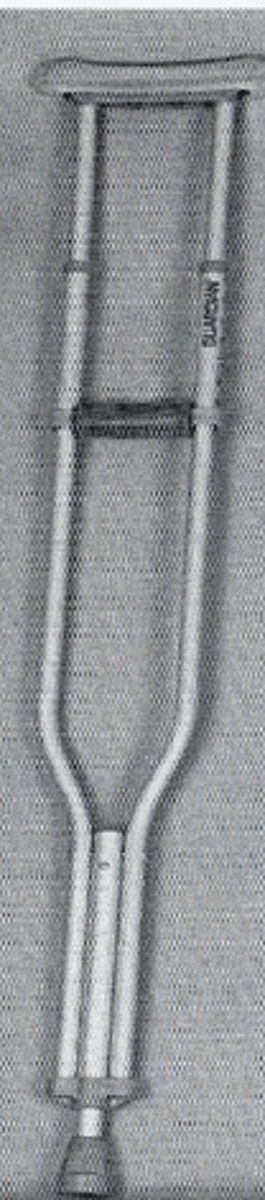
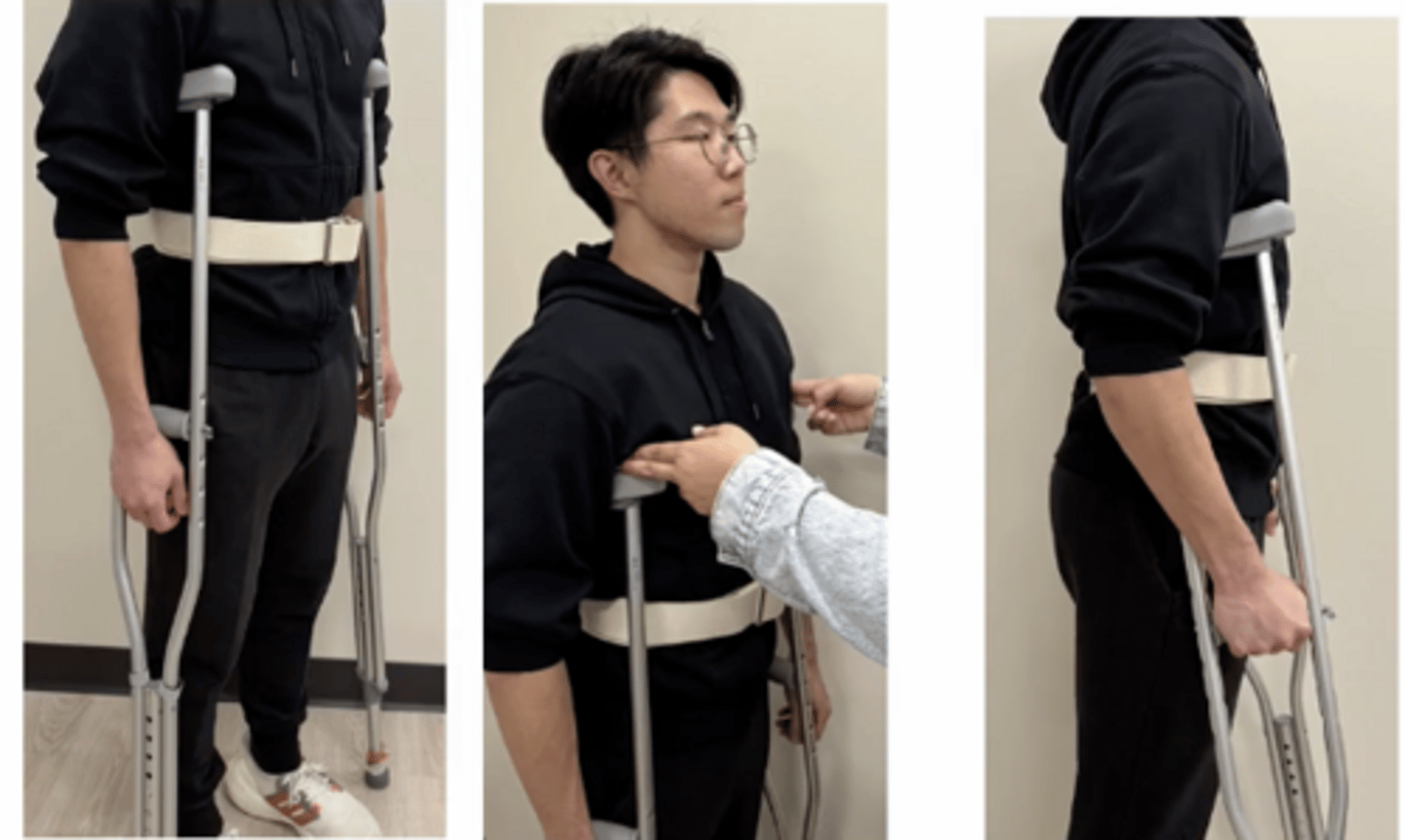
axillary crutches (AC)
- provides more mobility with a smaller base of support
- patient needs good standing balance and functional strength of trunks and UEs
disadvantage of axillary crutches (AC)
- if not used correctly, the pressure through the axilla can compress nerves and blood flow
- if balance and coordination is compromised
measurement and fit of axillary crutches
- space for 2-3 fingers in axilla (2 inches)
- crutch tips 2 inches lateral and 4-6 inches anterior to toe of shoe
- 20-25 degree of elbow flexion
estimating crutch length in sitting position
- shoulders abducted, one elbow in 90 degrees flexion
- measure distance from olecranon of flexed arm to tips of extended fingers of other arm
in supine position estimating crutch length
measure distance from anterior axillary line to a point 4-6 inches lateral to heel
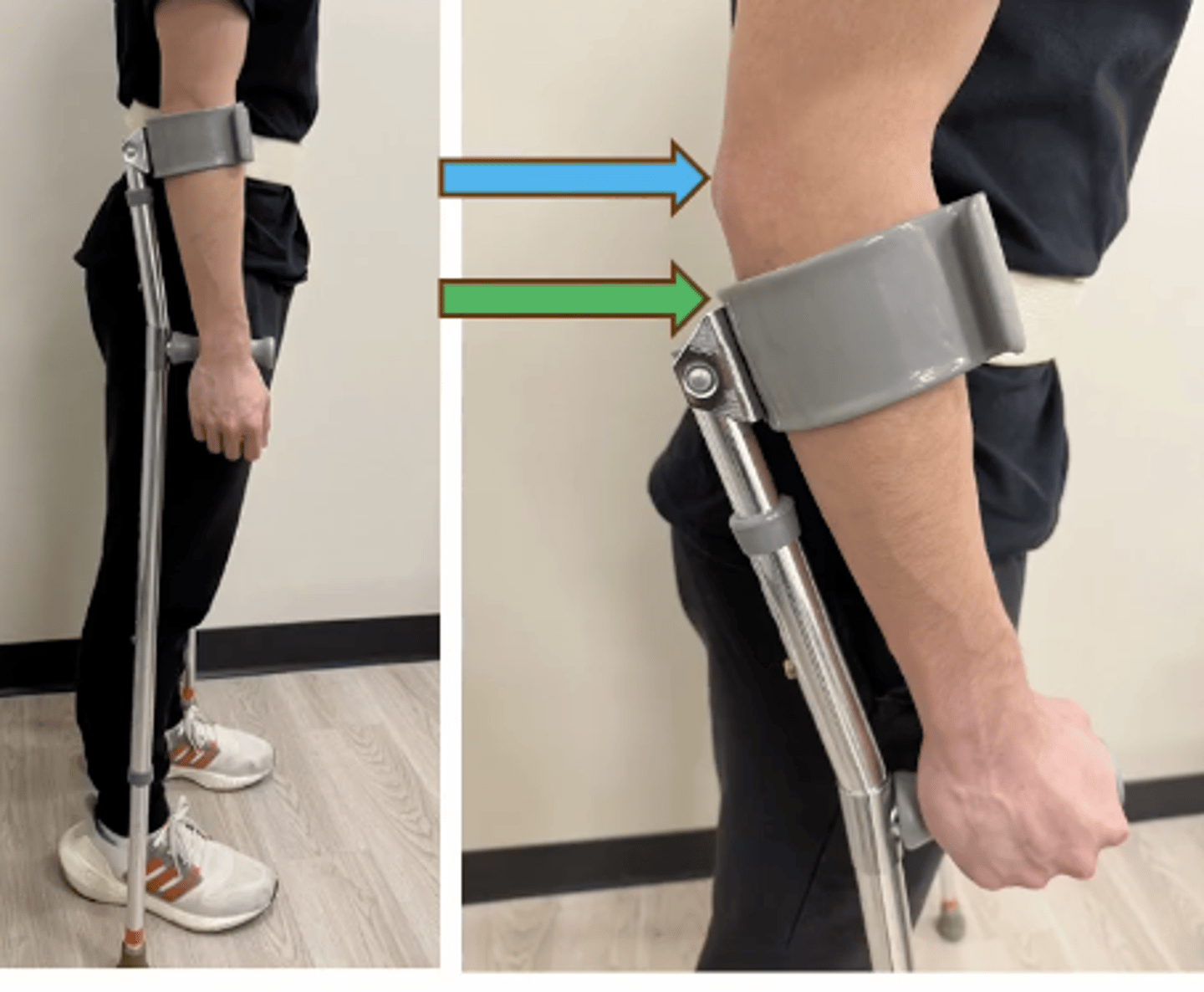
forearm crutches aka
loftstrand or Canadian crutches

forearm crutches are good for
patients who need good standing balance and functional strength of trunk and UE
disadvantage of forearm crutches
- less stable
- difficult to remove because of cuff
- only 2 points of contact for BOS, pt feels less secure
forearm crutch measurement
- handle at ulnar styloid process
- top of cuff 1-1.5 inches from olecranon while holding hand grip
canes types
- WBQC (wide base quad cane)
- NBQC (narrow base quad cane)
- SPC (single point cane)
canes are not for
patients with weight bearing limitations
canes are carried on the sided of the
unaffected LE
disadvantages of cane
- less stable, less BOS
- not for pt without weight bearing
measurement of cane
- handle at ulnar styloid process
- 20-25 degree elbow flexion
forearm trough
attachment for crutches/waker that allows weight to be carried mainly through forearm vs wrist/hand
indications of use for forearm trough
- painful wrist/hand
- weak hand grip 2 degree pain or deformities
- elbow contractures
- below elbow amputation
disadvantage of forearm trough
- not able to fully use their triceps to unweight themselves
- trouble adjusting velcro straps on trough
- weight of AD is heavier
- impossible to use safely on stairs

measurement of forearm trough on walker
- adjust walker to proper height of patient first
- look for 90 degree elbow flexion with shoulder relaxed
- neutral position on handles or slightly pronated

factors to consider when choosing an AD
- diagnosis/prognosis
- UE involvement
- balance and coordination
- prior level of function (PLF)
- cognition
- past medical history (PMH)
- environment
- pain level
- weight bearing status
weight bearing status should always be
confirmed with MD order
types of weight bearing status
- NWB
- TTWB/TDWB
- PWB
- WBAT
- FWB
NWB
non weight bearing on affected extremity
TTWB/TDWB
toe touch or touch-down, mainly for balance assist only not full weight bearing
PWB
partial weight bearing, less than 50% pt weight or MD will specify %
WBAT
weight bearing as tolerated, may be limited secondary pain but no limitations
FWB
full weight bearing
assistance levels
- independent (indep) or I
- modified independent
- supervised (sup)
- standby assist (SBA)
- contact guard assist (CGA)
- min assist
- mod assist
- max assist
- dependent
independent (indep)
Pt requires no physical supervision or assist to consistently perform the activity safely
modified independent
pt is safe and independent with the assistance of equipment
supervised (sup)
pt requires assistance of another person to perform activity i.e: verbal cues
standby assist (SBA)
assisting person is close, but not touching the patient, providing occasional verbal/tactile cues
contact guard assist (CGA)
- caregiver is close with hand on gait belt
- pt will very likely need some form of protection during the activity
min assist
pt performs 75-90% or more of the activity with assist to complete the task
mod assist
pt performs 50-74% of the activity with assist to complete the task
max assist
pt performs 25-49% of activity with assist to complete the task
dependent (dep)
pt requires TOTAL physical assist
it is important during assistance to
try to define what the verbal cues or assist is for i.e: pacing, sequencing, posture, weight shifting
why is it important to document and define level of assist
- establish functional goals in your treatment plan with your patient
- ensure proper carryover by other staff
- record improvement or change in your patient's progress toward their set goals (insurance, MD)
hemi walker

pick up walker

front wheel walker

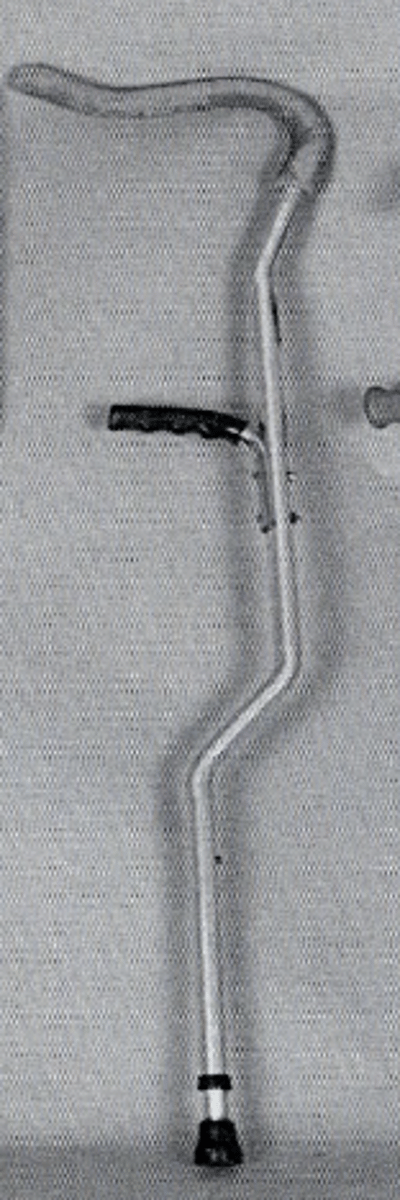
tricep crutches

offset crutch