Endo 3 - Radiology (Dr. Monteiro)
1/85
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
86 Terms
Bitewing radiograph
Which type of radiograph evaluates caries, existing restorations, and previously initiated therapy?
Bitewing radiograph
Which type of radiograph has an excellent projection to assess periodontal tissue?
Bitewing radiograph
Which type of radiograph presents an accurate representation of corona pulp anatomy?
Panoramic radiographs
Which type of radiograph is recommended in trauma cases to rule out fractures of teeth and the alveolus?
CBCT
Which type of radiograph is a dimensionally accurate view of tooth and surrounding structures?
Periapical radiograph
_______ are the most commonly used radiograph in endodontics
Mesial
Distal
Parallel
What 3 views can a periapical radiograph be taken from?
Periapical radiograph
Which type of radiograph is NECESSARY for periapical diagnosis, intraoperatively and post-operatively?
Crown
Post D Canal
PARL Mesial and Distal Root
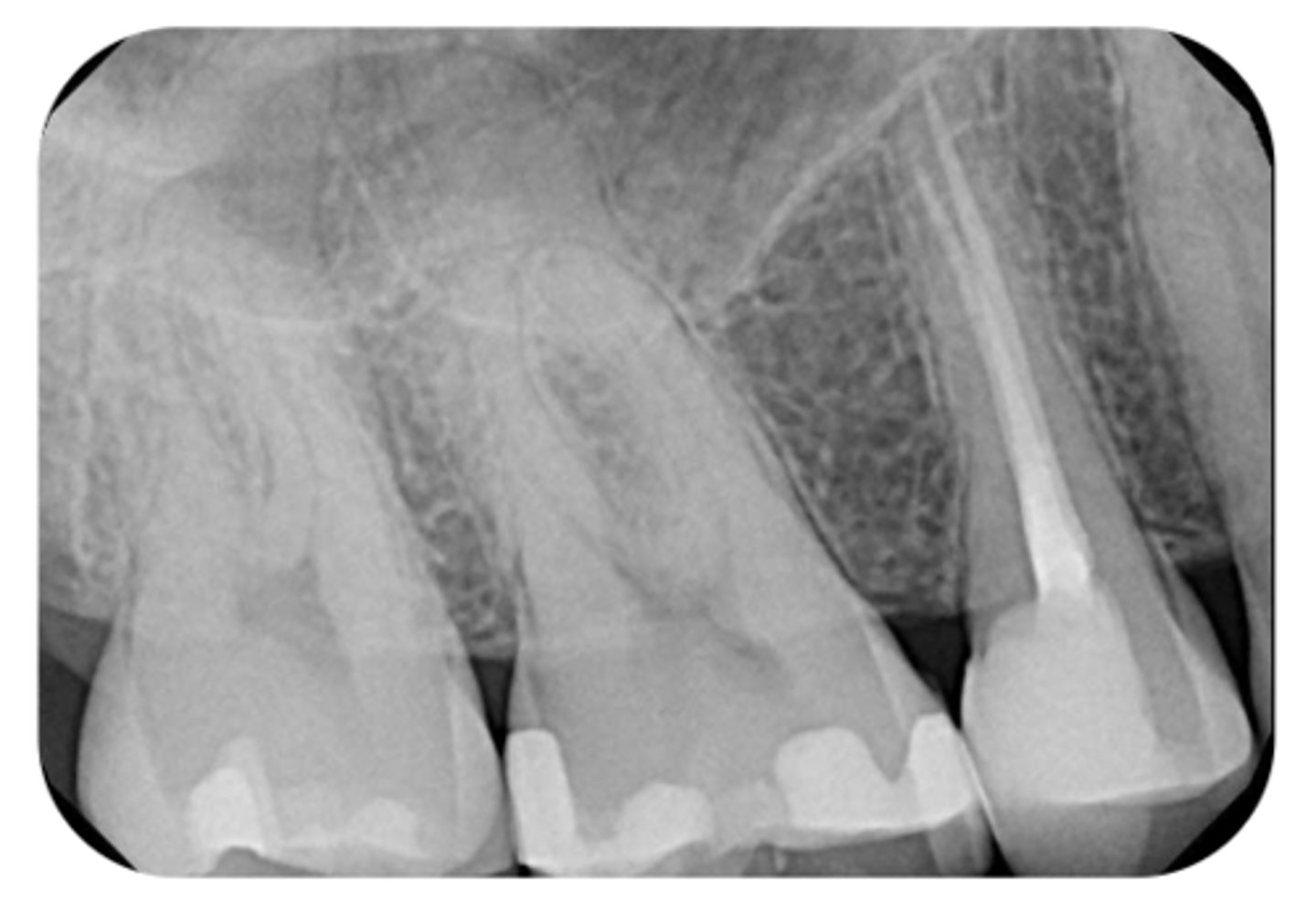
What are the radiographic findings on #19?

Crown
PARL in Mesial and Distal Root
Discontinuation of LD
What are the radiographic findings on #19?

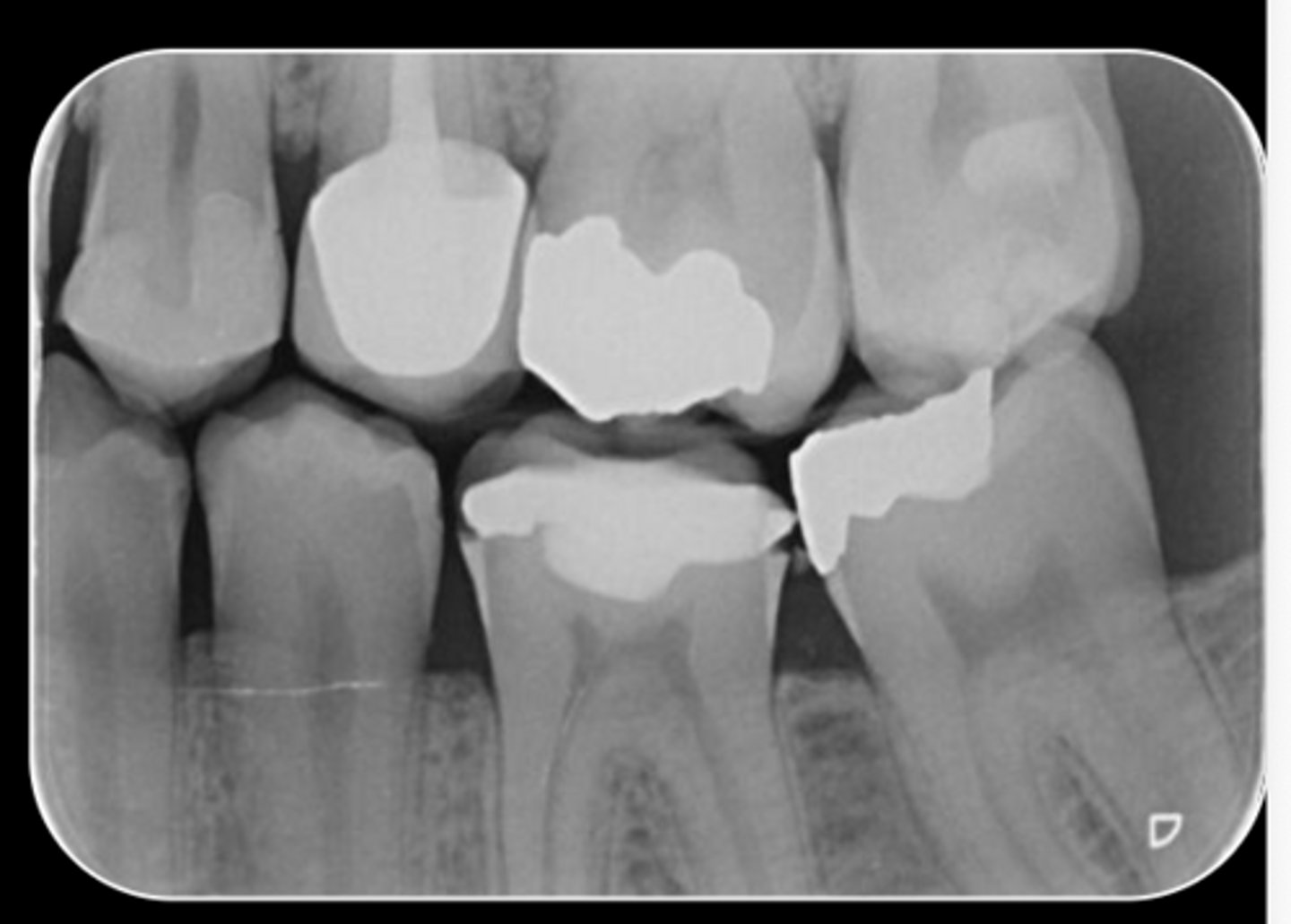
DO Composite
RCT
No PARL
LD intact
PDL normal
What are the radiographic findings on #4?
Bitewing
What image should be straight-on, with as little overlap as possible?
bitewing radiograph
which type of radiograph provides the only way to judge extent of decay, restorability and status of restorations?
bitewing radiograph
which type of radiograph shows the position of the bone in relation to the CEJ of the teeth?
bitewing radiograph
Which type of radiograph is necessary for understanding pulp chamber anatomy?
M Caries
Pulp stones
Pulp chamber receeded
What are the radiographic findings on #3?

Fracture Mesial-Distal
Caries approximating pulp chamber
What are the radiographic findings on #14?

Crown
Post
What are the radiographic findings on #13?
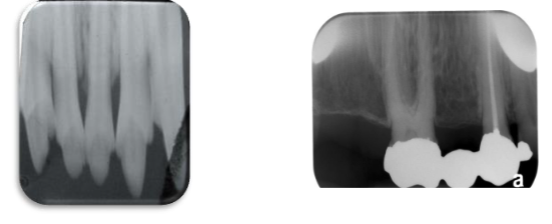
Conventional Film
What type of dental radiograph?
Digital Sensor
What type of dental radiograph?

Pedodontics
Small mouth
Gag reflex
size 1 sensor is indicated for
size 2
What size sensor is primarily used?
Lead apron
What MUST be placed on the patient to take EVERY Radiograph?
CBCT
What type of imaging system?
- 3D rendering of a small area
- Can be useful as an adjunct but is not yet the standard of care
- Used for re-treatments, resorptions cases and unusual anatomy
- Coronal, axial, and sagittal views
paralleling technique
ID the sensor technique
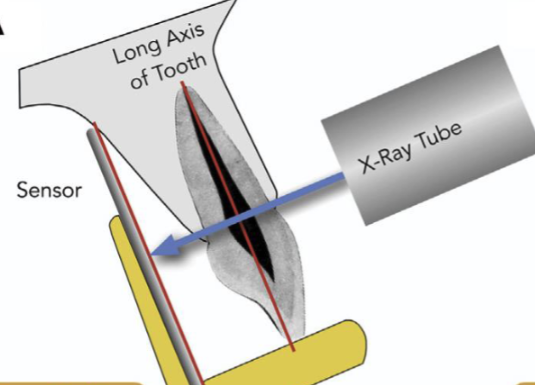
parallel
In the paralleling technique, the film/sensor is laid ________ to the long axis of the tooth.
perpendicular
In the paralleling technique, the source of x-ray beam is ________ to the long axis of the tooth
midline of the palate
(NOT placed against the palatal aspect of the teeth)
To obtain an accurate max radiograph, the sensor should be placed near the _______
foreshortening/missing structures
Improper sensor placement of maxillary radiographs will result in what?
tongue and the mylohyoid ridge
To obtain an accurate mandibular radiograph, the sensor should be placed between the _______ and _______
Relax the floor of the mouth and tongue
When taking a mandibular radiograph, what does the patient have to do?
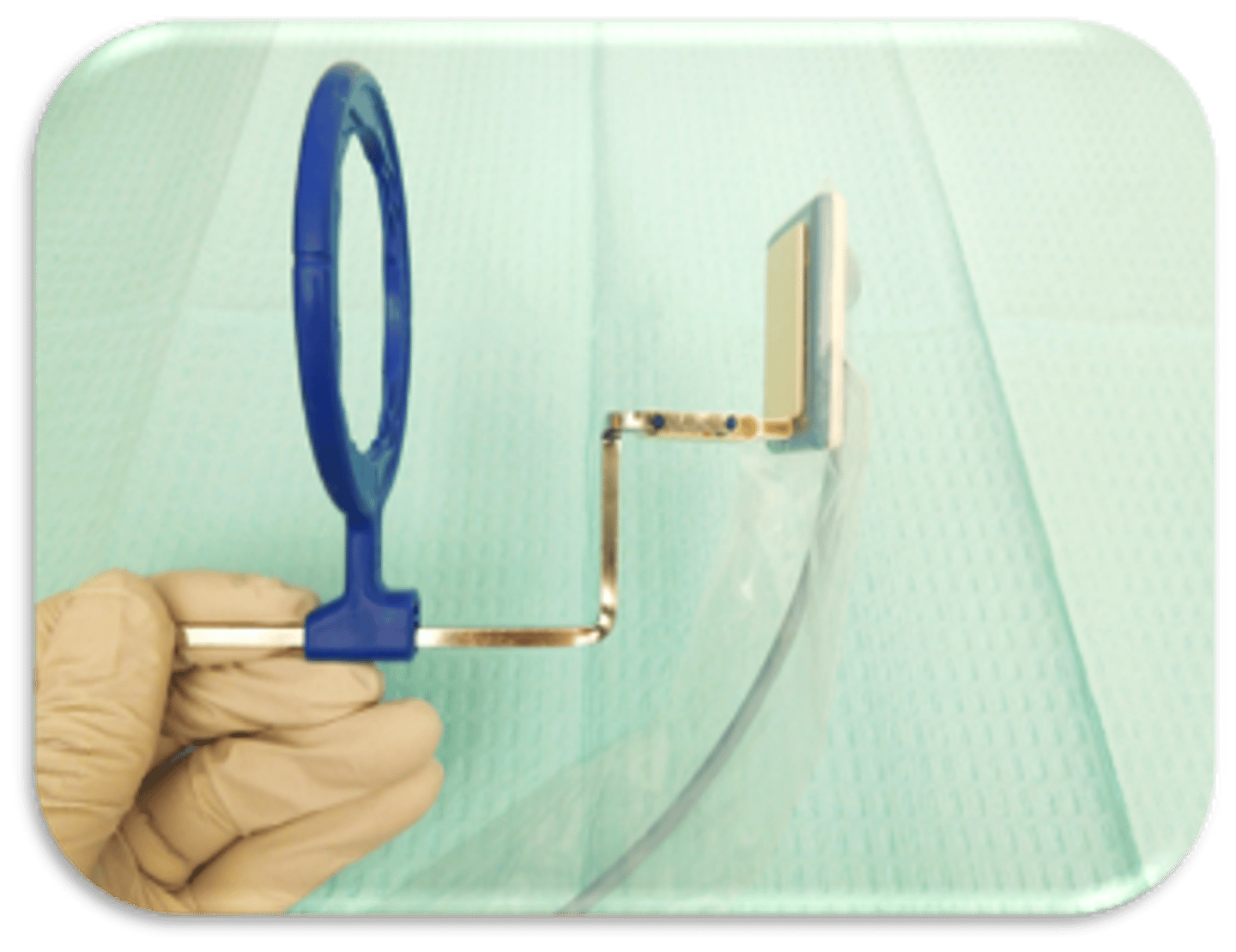
anterior PA
This device is used to capture what type of radiograph?
bisecting angle technique
ID the sensor technique:
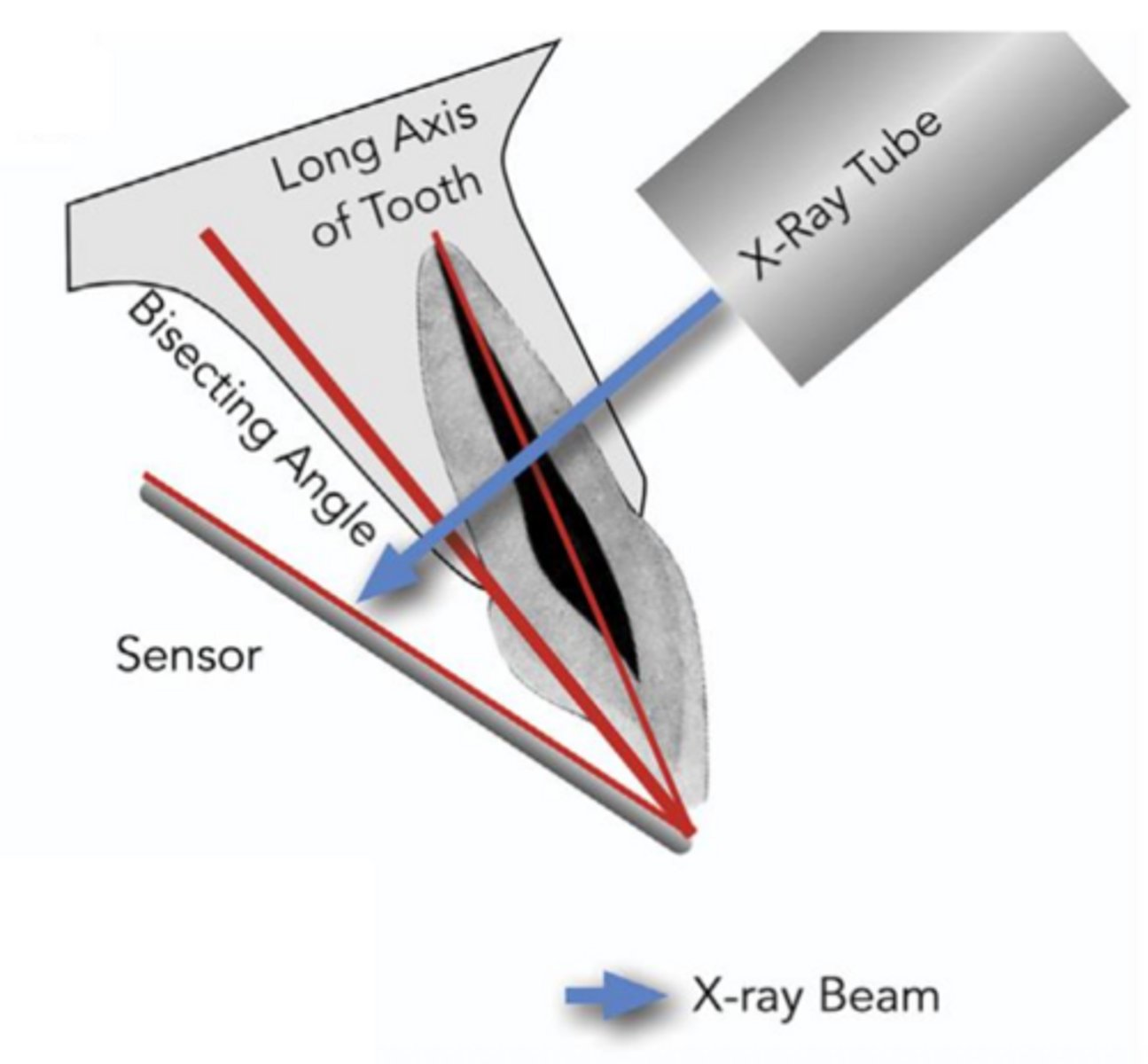
perpendicular
In the bisecting angle technique, the X-ray beam is directed ________ to the imaginary line which bisects the angle formed by the long axis of the tooth and the long axis of the film/sensor.
next to
In the bisecting angle technique, the film/sensor is placed _______ the tooth.

foreshortening
In the bisecting angle technique, if the vertical angulation is excessive, it will result in image _______
elongation
In the bisecting angle technique, if the vertical angulation is insufficient, it will result in image _______
More comfortable for the patient
No anatomical limitations
What are 2 advantages of the bisecting angle technique?
No Rinn-type holder: more opportunity for cone cuts and distortions
Film/sensor is more prone to move
What are 2 disadvantages of the bisecting angle technique?
paralleling technique
which radiographic technique is best used for an endo pre-op + post-op eval?
bisecting angle technique
which radiographic technique is best used for an endo intra-op eval?
paralleling technique
which radiographic technique is best used for an endo post-op eval?
bisecting angle technique
which radiographic technique is best used anatomical limitations like small mouth, shallow palate, torus?
Rubber dam must ALWAYS be on for clinical endodontic treatment!!!
What does this photo emphasize the importance of?

- Placement of hemostat on green tab
- Wind sensor cord around hemostat
- Placement under dental dam for maxillary anterior tooth
How can you place the size 2 film to take a radiograph of the maxillary central incisor?
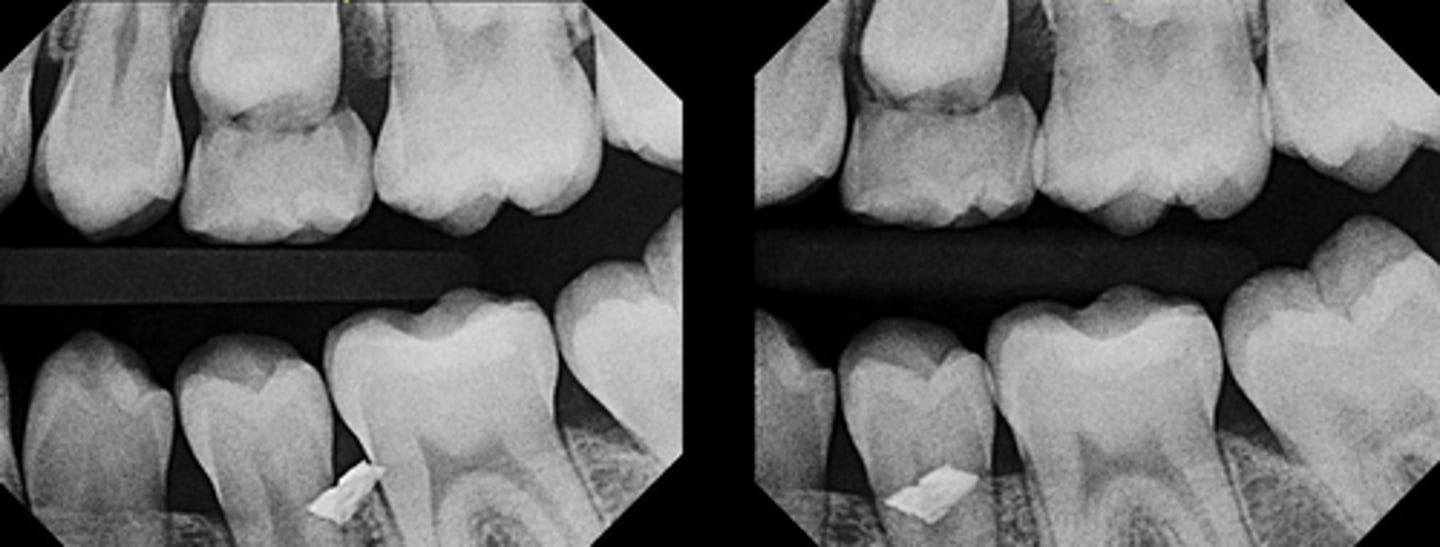
if an object moves in the SAME direction as tube shifts the object is LINGUAL
If the object moves in the OPPOSITE direction the object is BUCCAL
SLOB rule stands for what?
At least 2:
- 1 PA straight on
- 1 PA with x-ray tube shifted from either mesial or distal direction
At least how many PAs do you need for the SLOB rule?
buccal
Is this foreign object lingual or buccal to the teeth?
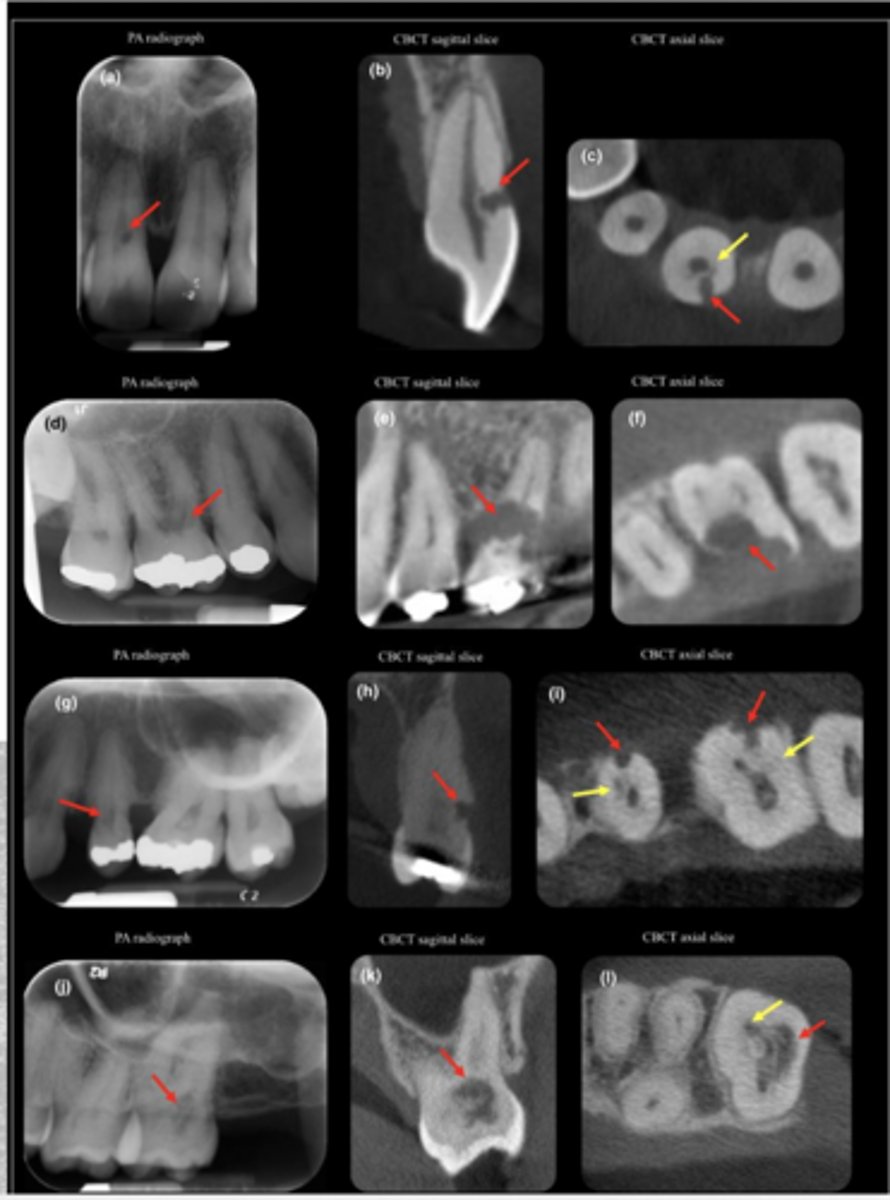
B. Lingual (palatal) to the main mesiobuccal canal
A 35-year-old patient presents with spontaneous pain in the maxillary first molar. The pulpal diagnosis is symptomatic irreversible pulpitis and periapical diagnosis of symptomatic apical periodontitis, and nonsurgical root canal therapy is initiated.
During access preparation, the clinician identifies the mesiobuccal canal but suspects an additional
canal in the same root.
Two periapical radiographs are obtained:
- The first radiograph is taken with normal horizontal angulation.
- The second radiograph is taken with a distal horizontal tube shift.
On the second image, the suspected canal appears to move distally, in the same direction as the tube shift.
Based on these findings, where is the suspected canal most likely located?
A. Buccal to the main mesiobuccal canal
B. Lingual (palatal) to the main mesiobuccal canal
C. Apical to the main canal
D. Distal to the main canal
The ability to apply the SLOB rule
All of the following require a thorough knowledge of what?
- Distinguish between normal anatomical landmarks and the radiolucent shadows associated with pathosis of the roots of teeth
- Determine the buccal or lingual position of root fractures, perforations and resorptive processes
- Distinguish between internal and external root resorption
- Locate foreign bodies in trauma cases
- Locate anatomical landmarks (i.e. Mandibular canal, maxillary sinus) in relation to the root apex during periapical surgery
- Locate hidden apices prior to periapical surgery by placing a small opaque object (lead foil) on bone near the estimated apex
- Determine the number, location, shape, size, and direction of various roots and root canals during instrumentation and obturation
lamina dura
ID the structure:
A sheet of compact alveolar bone that lies adjacent to the periodontal membrane i.e. lining of the alveolus
lamina dura
ID the structure:
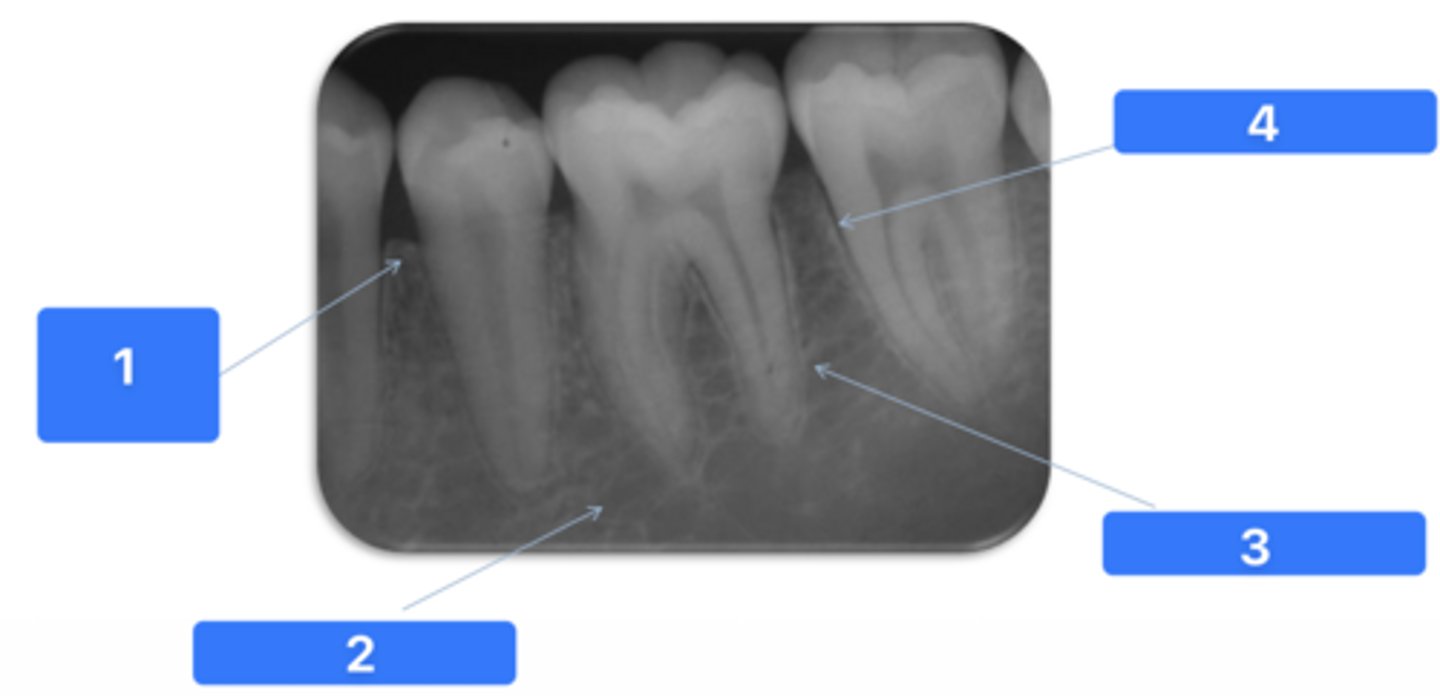
Alveolar crest
medullary bone
lamina dura
PDL space
what are the numbers
intermaxillary suture
ID the structure:
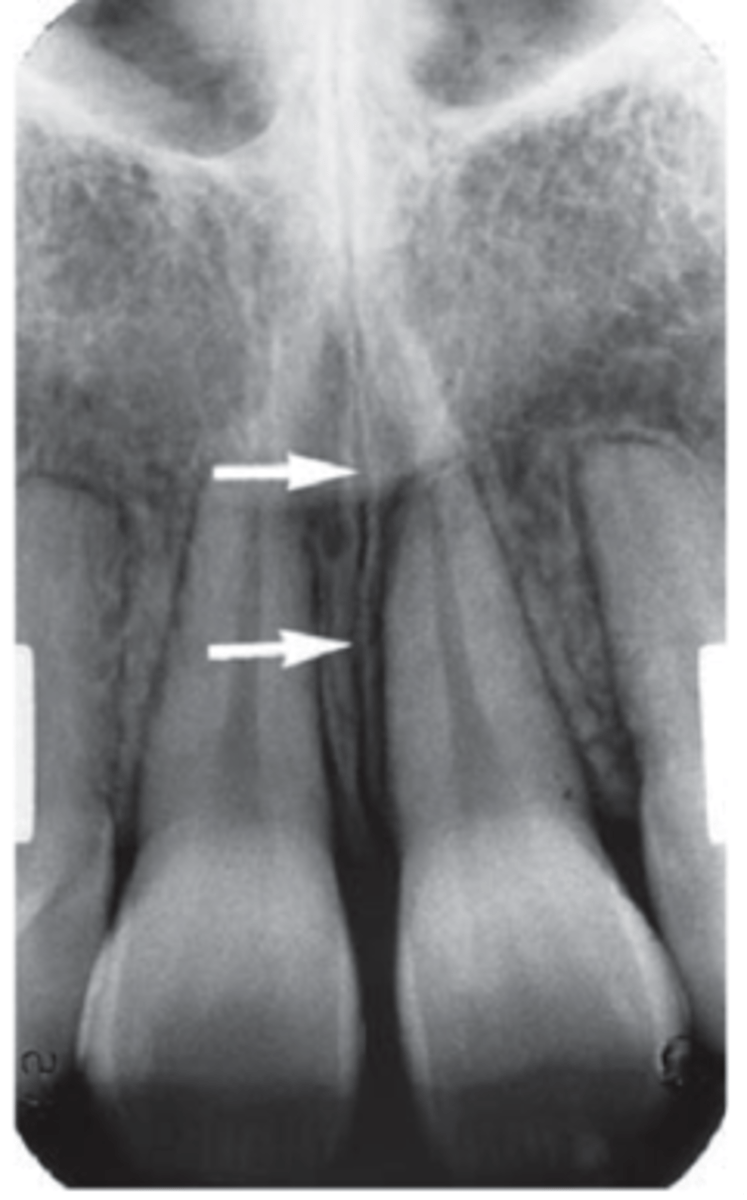
nasopalatine foramen
ID the structure:

nasopalatine foramen
ID the structure:
maxillary sinus
ID the structure:

maxillary sinus
ID the structure:

mental foramen (always near mand 2nd premolar)
ID the structure:

mental foramen
ID the structure:

external oblique line
ID the structure with the purple arrow:

inferior alveolar nerve canal
ID the structure with the green arrow:

submandibular gland fossa
ID the structure:
submandibular gland fossa
ID the structure:
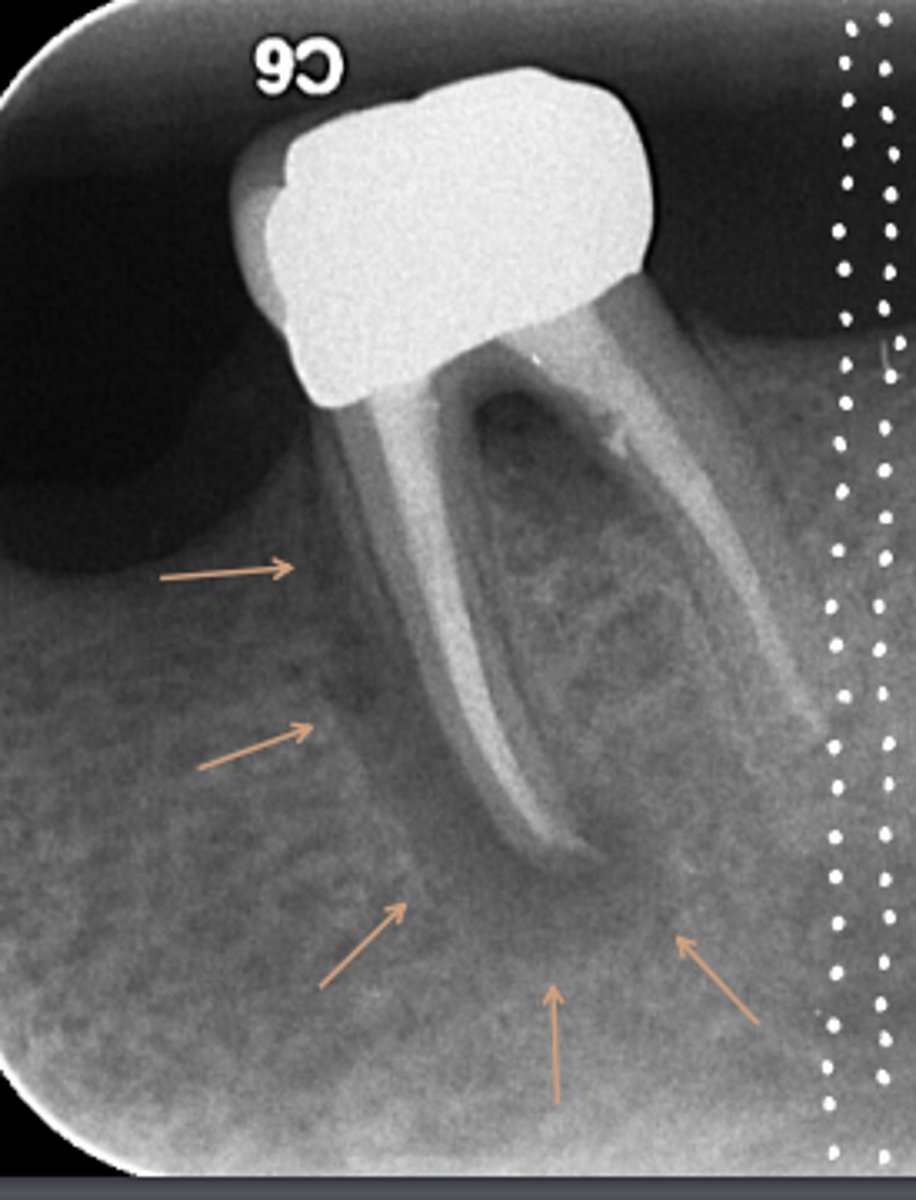
Areas of rarefaction
ID the problems:
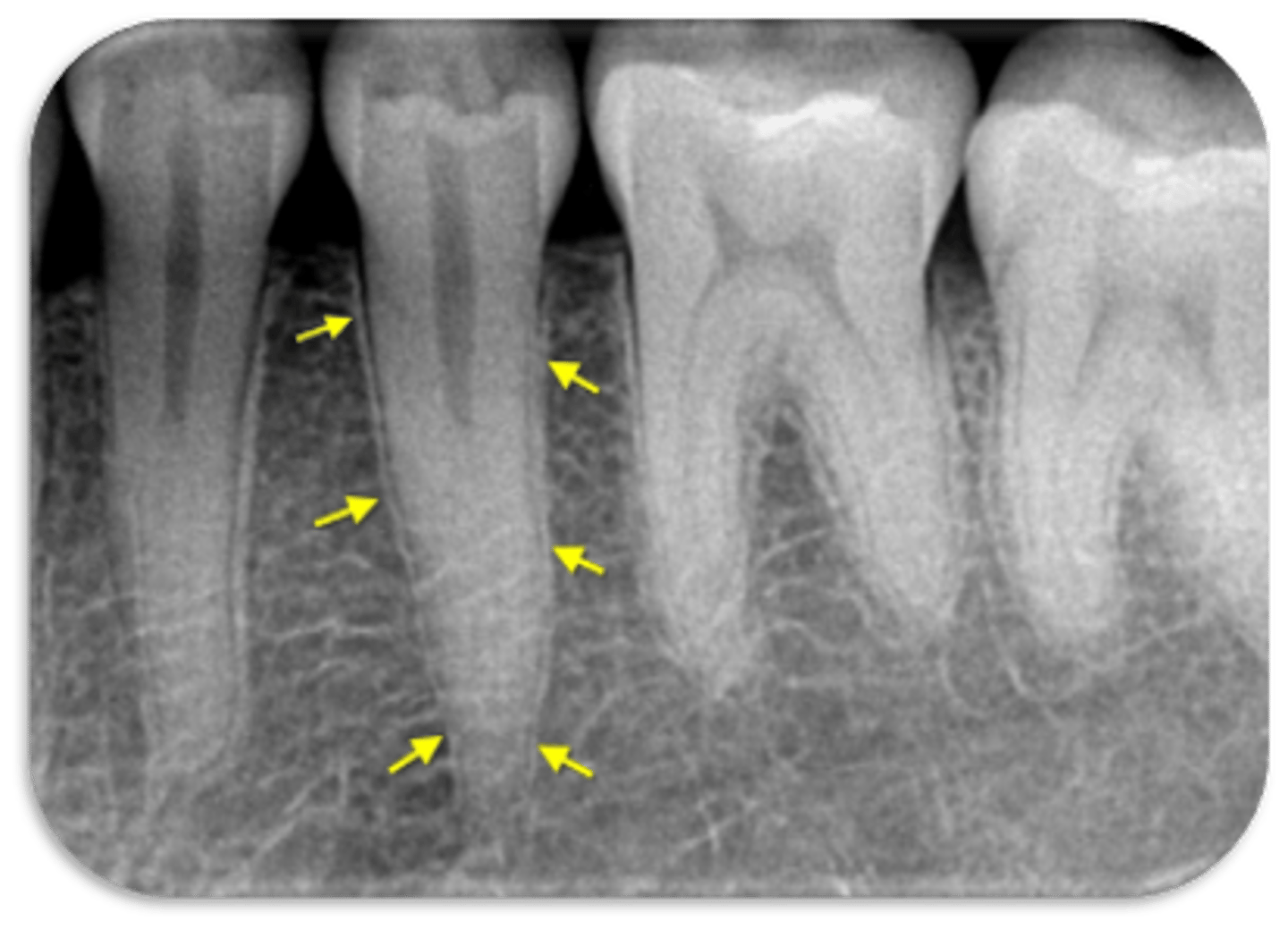
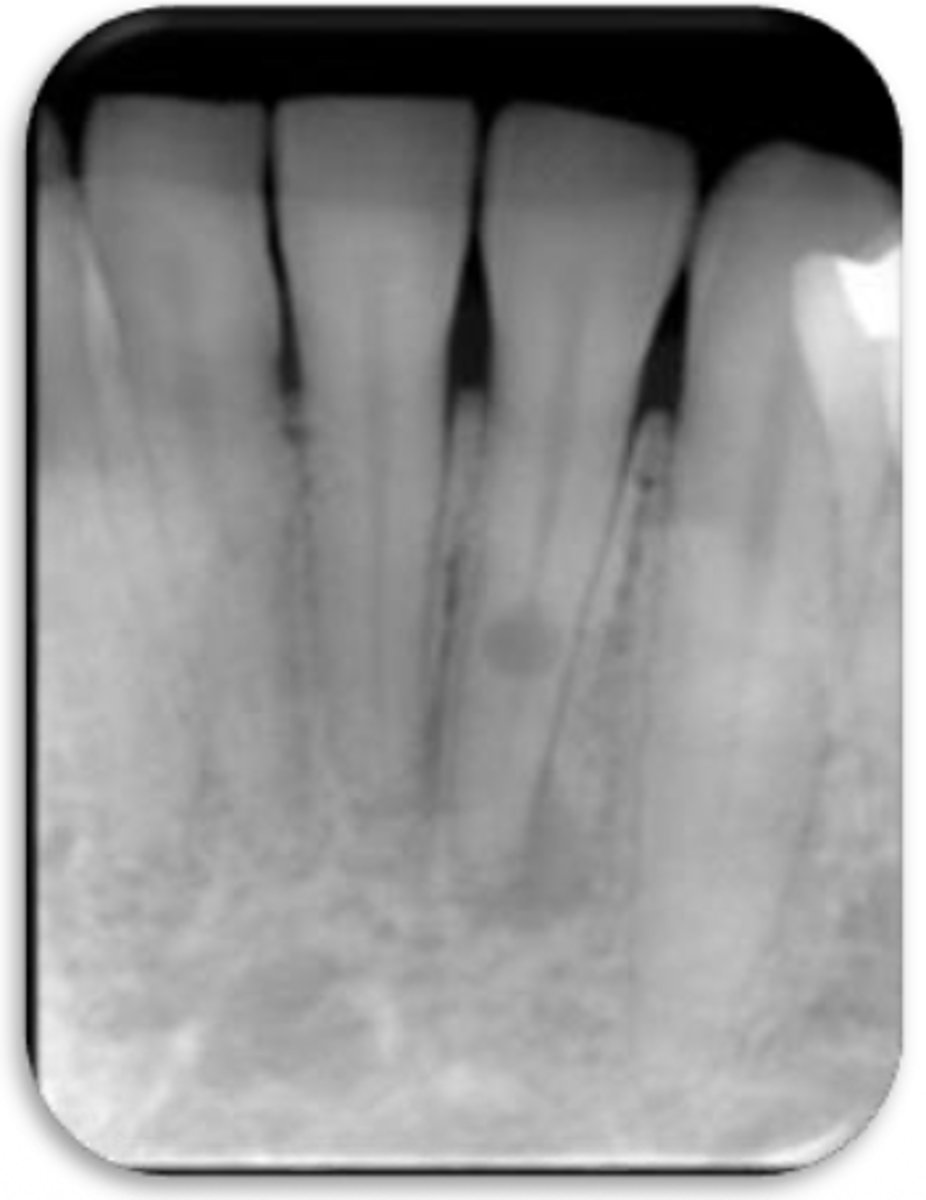
spliting canals
ID the problem:
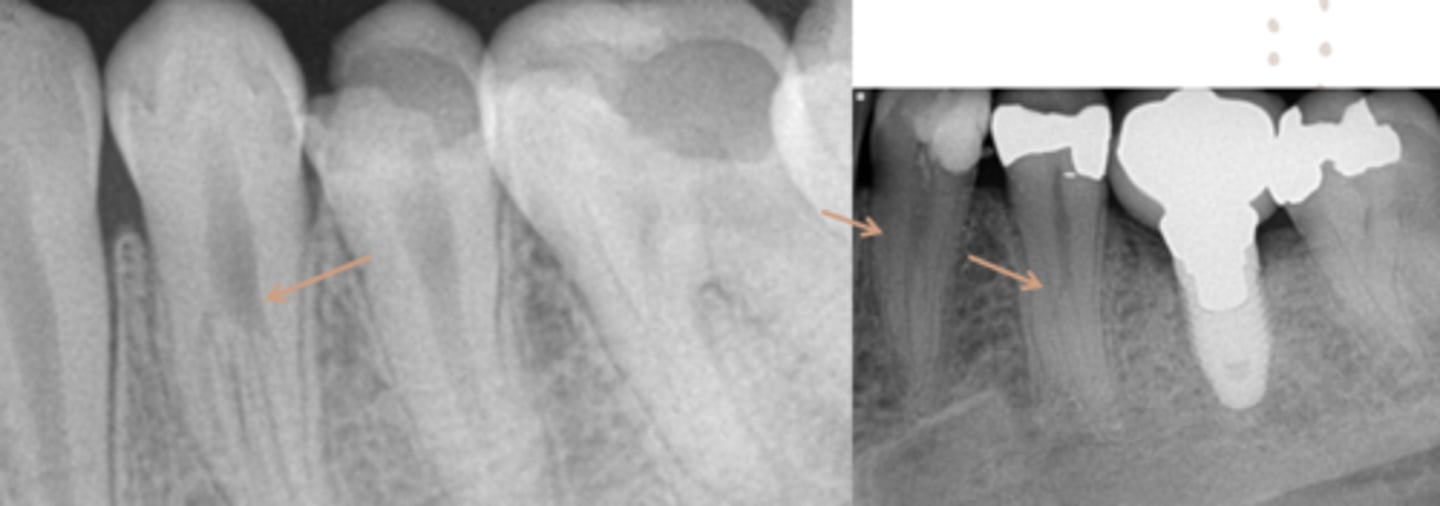
spliting canals
ID the problem:

spliting canals
ID the problem:

spliting canals
ID the problem:
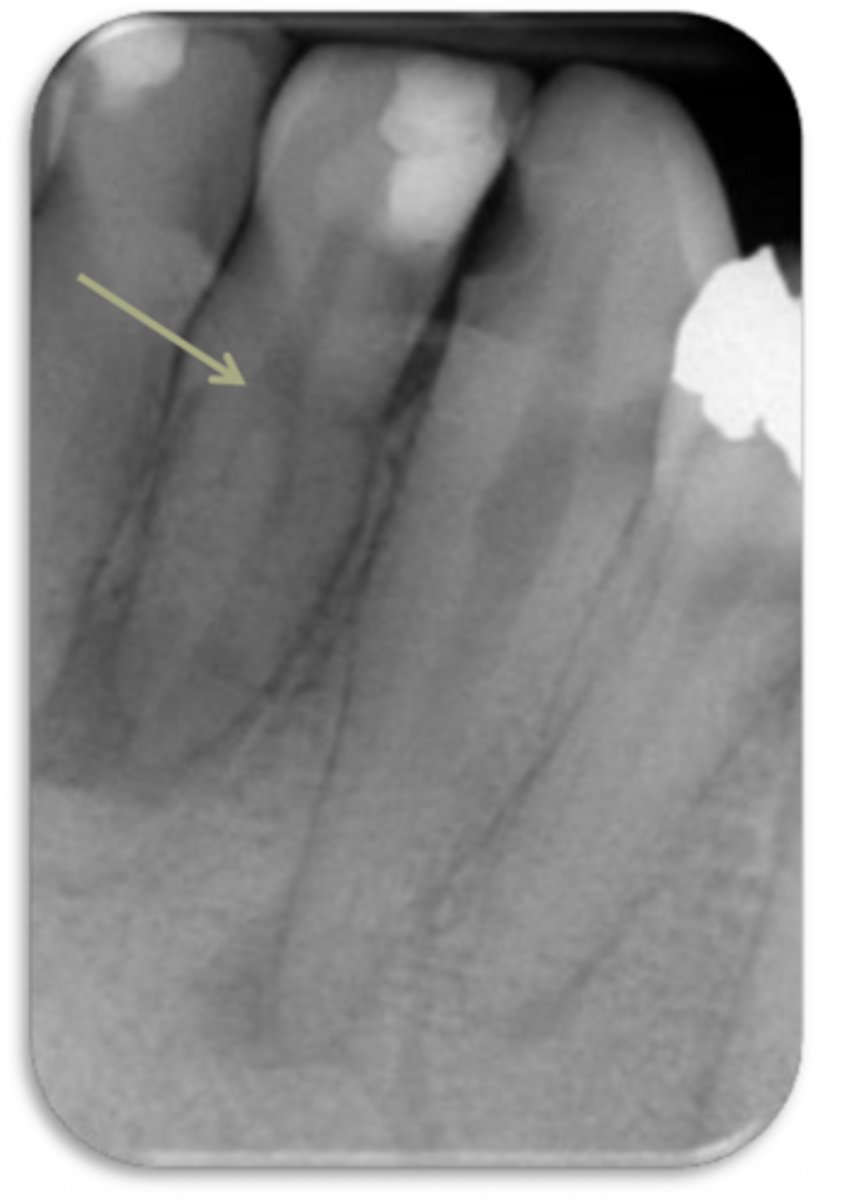
spliting canals
ID the problem:
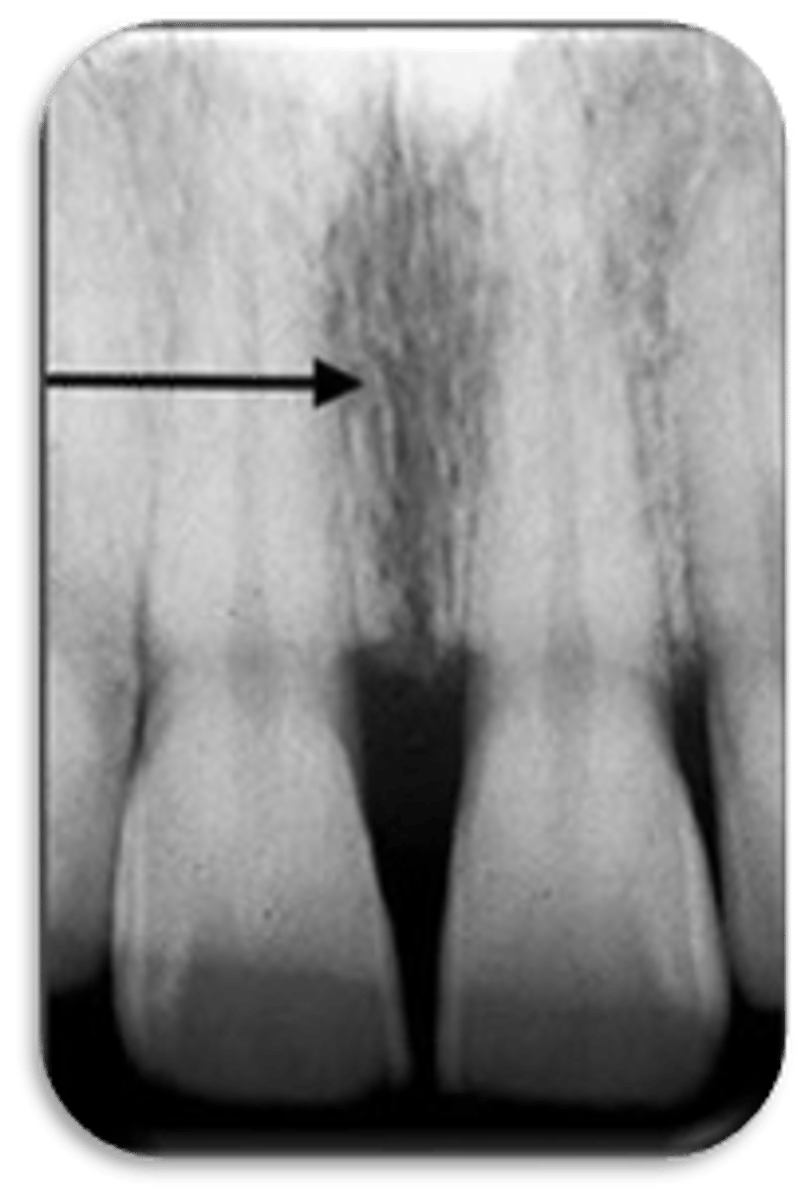
fracture
ID the problem:
fracture
ID the problem:

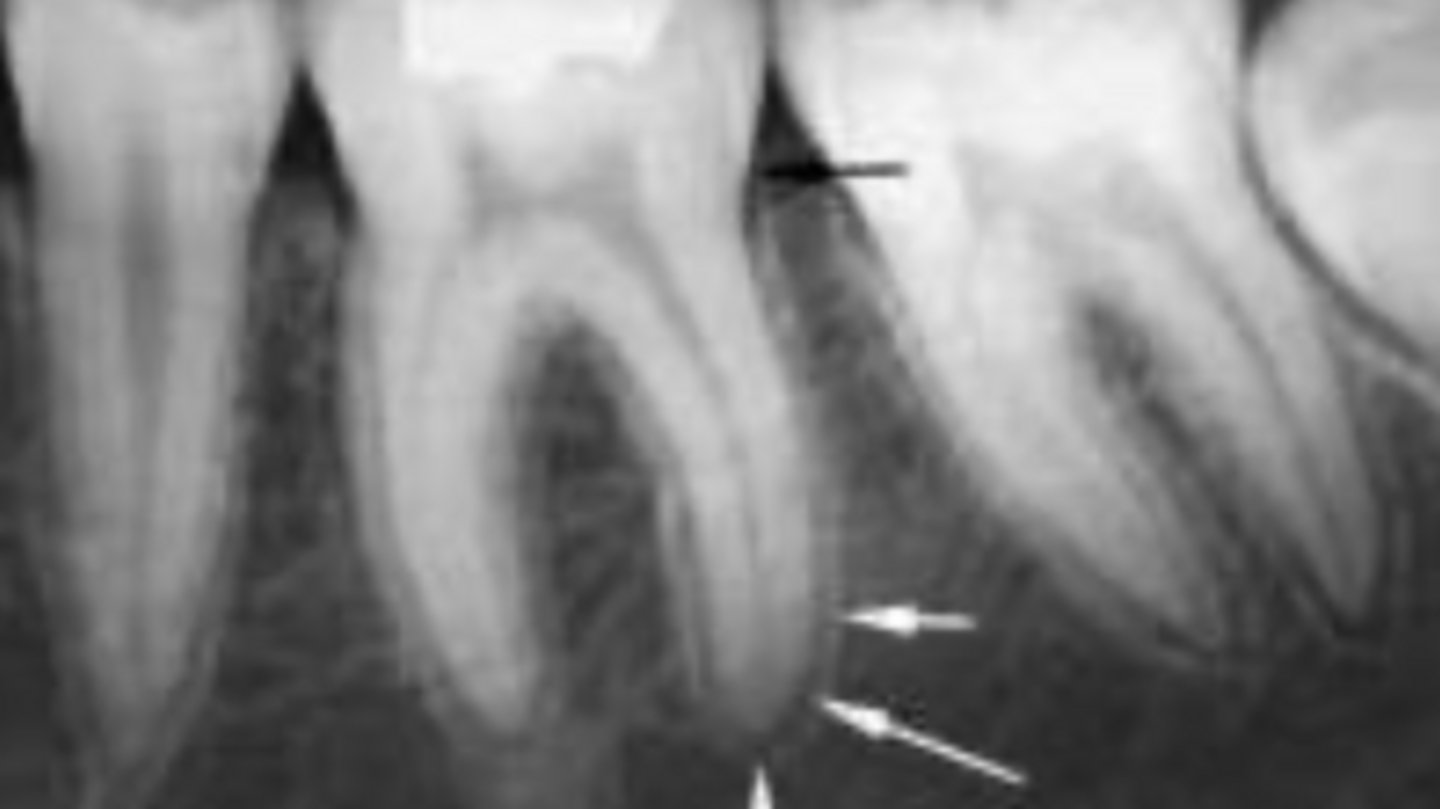
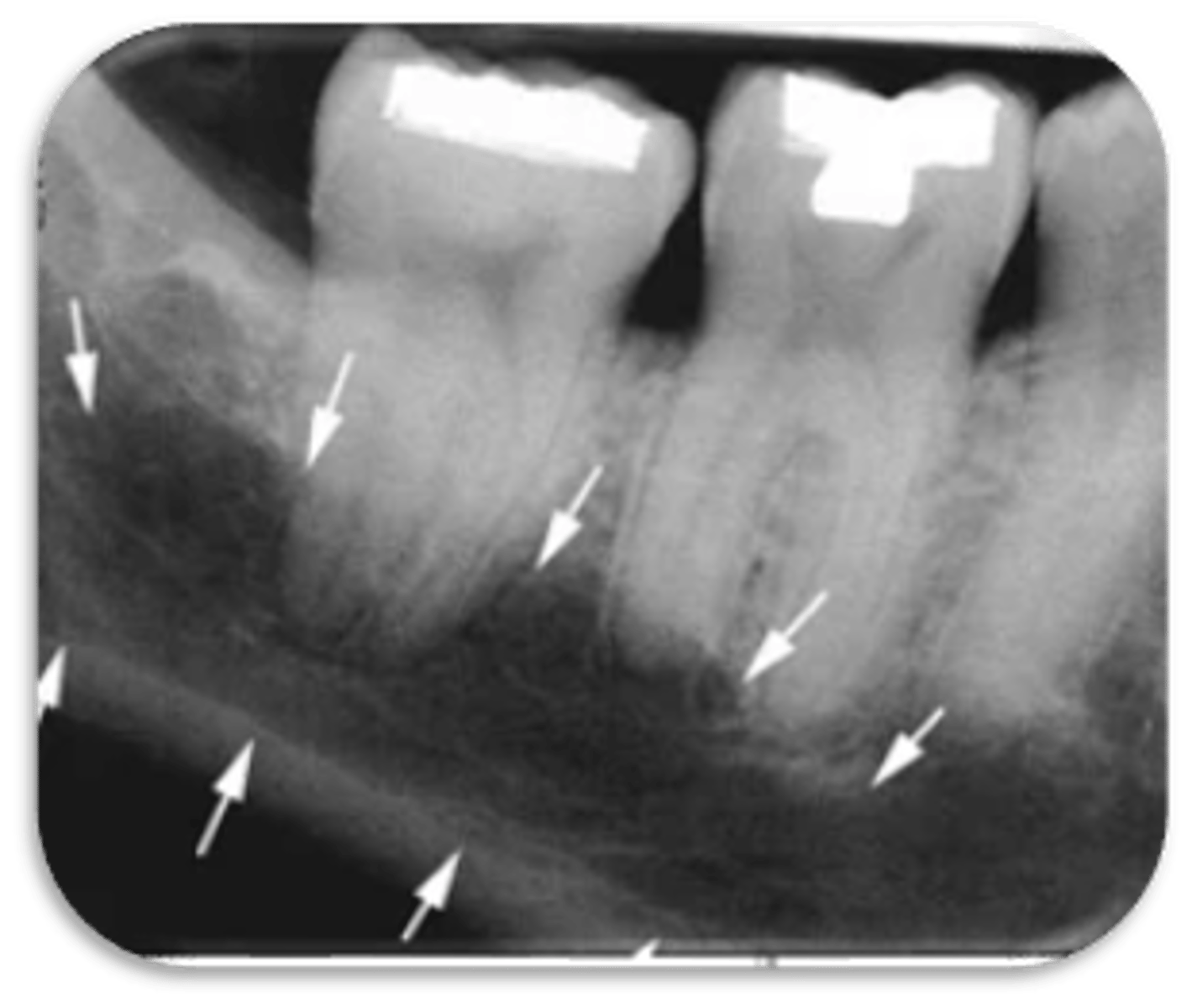
vertical root fracture
ID the problem:
vertical root fracture
ID the problem:
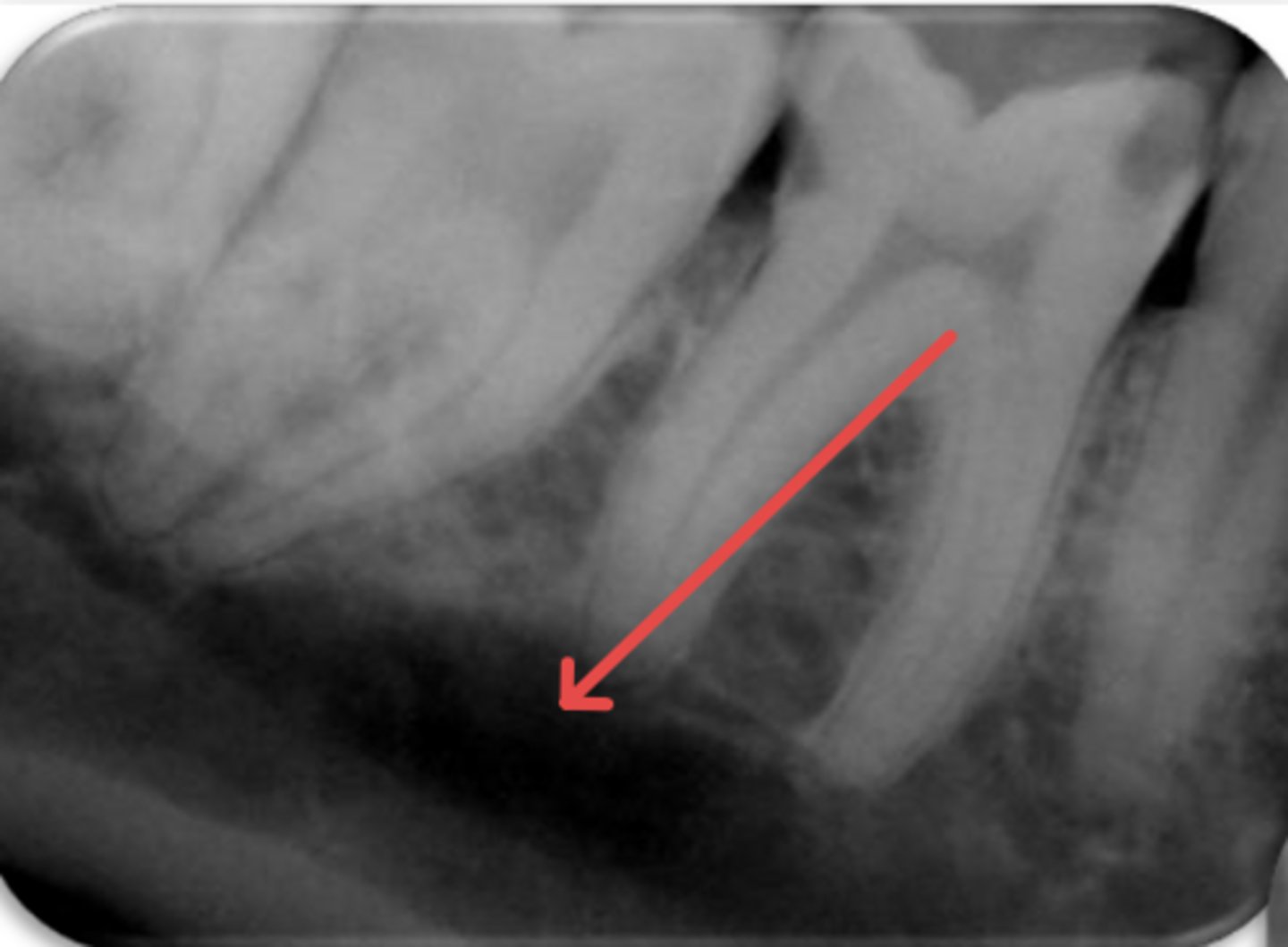
- May not show on PA radiographs
Presents with signs of:
- J-shaped lesion/lateral radiolucency
- Isolated deep pocket
- Coronally located swelling or sinus tract
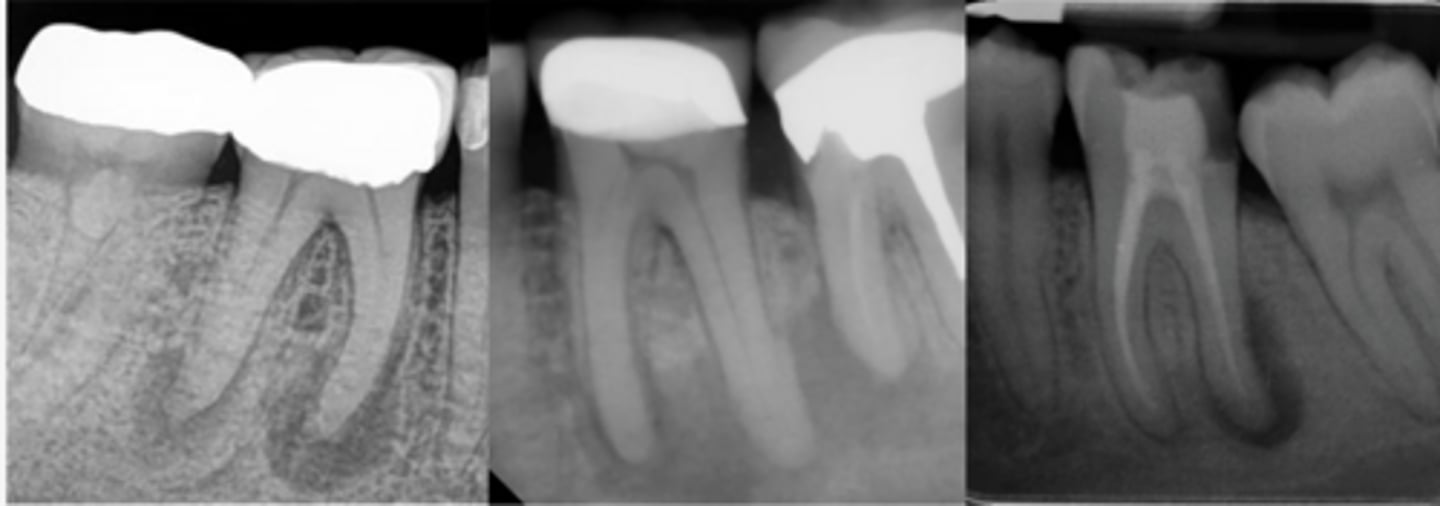
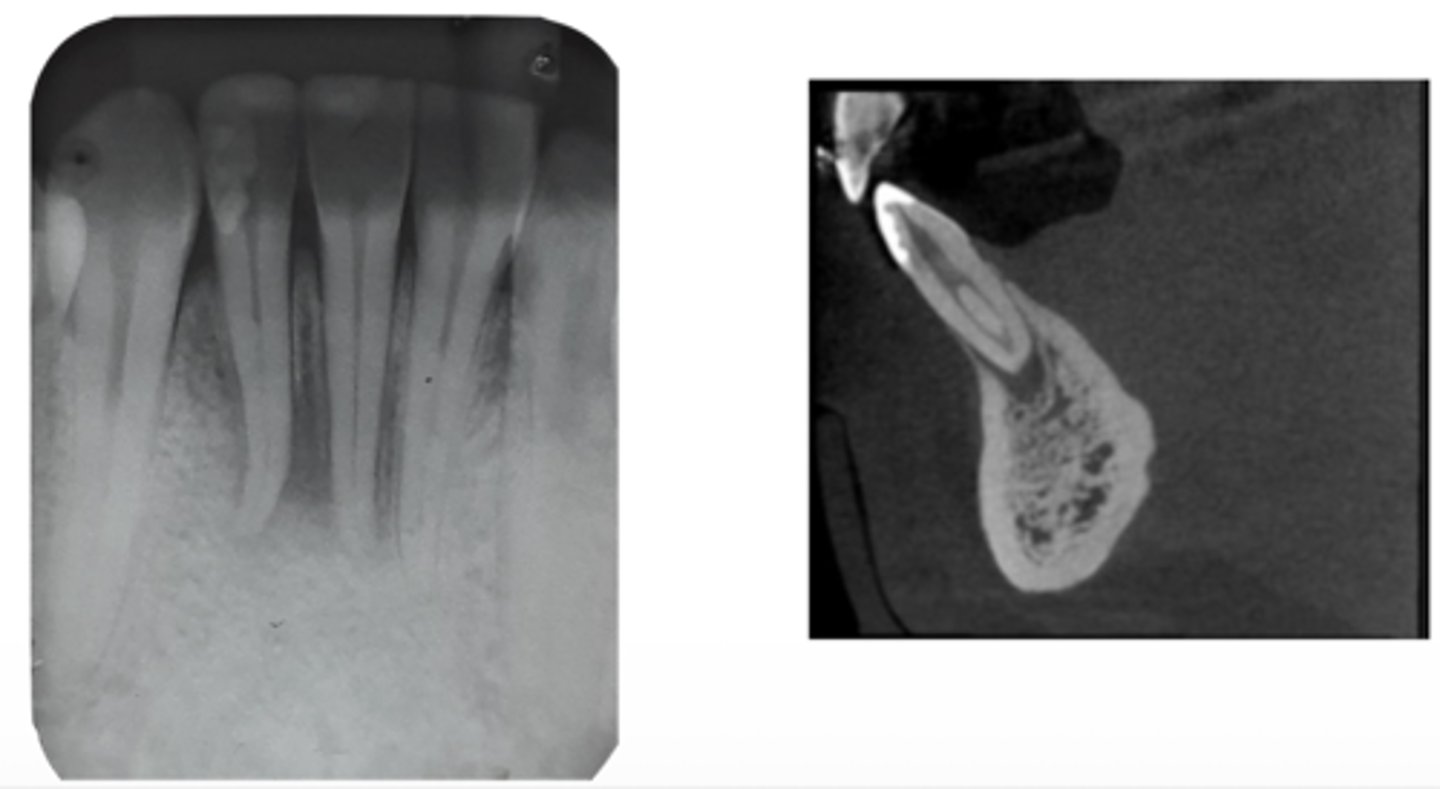
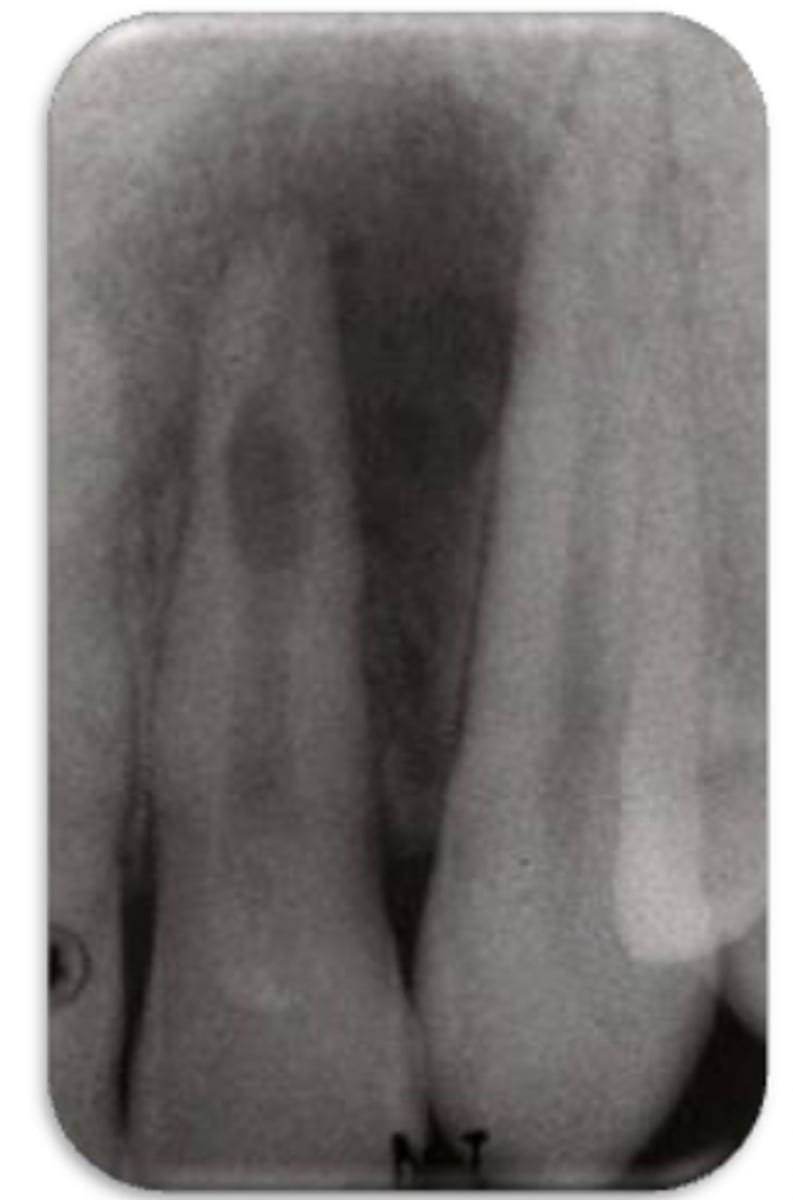
internal resorption
ID the problem:
- Ballooning out of root canal

internal resorption
ID the problem:
internal resorption
ID the problem:
Take a few different angles (SLOB rule)
How can you confirm if a root has internal resorption?
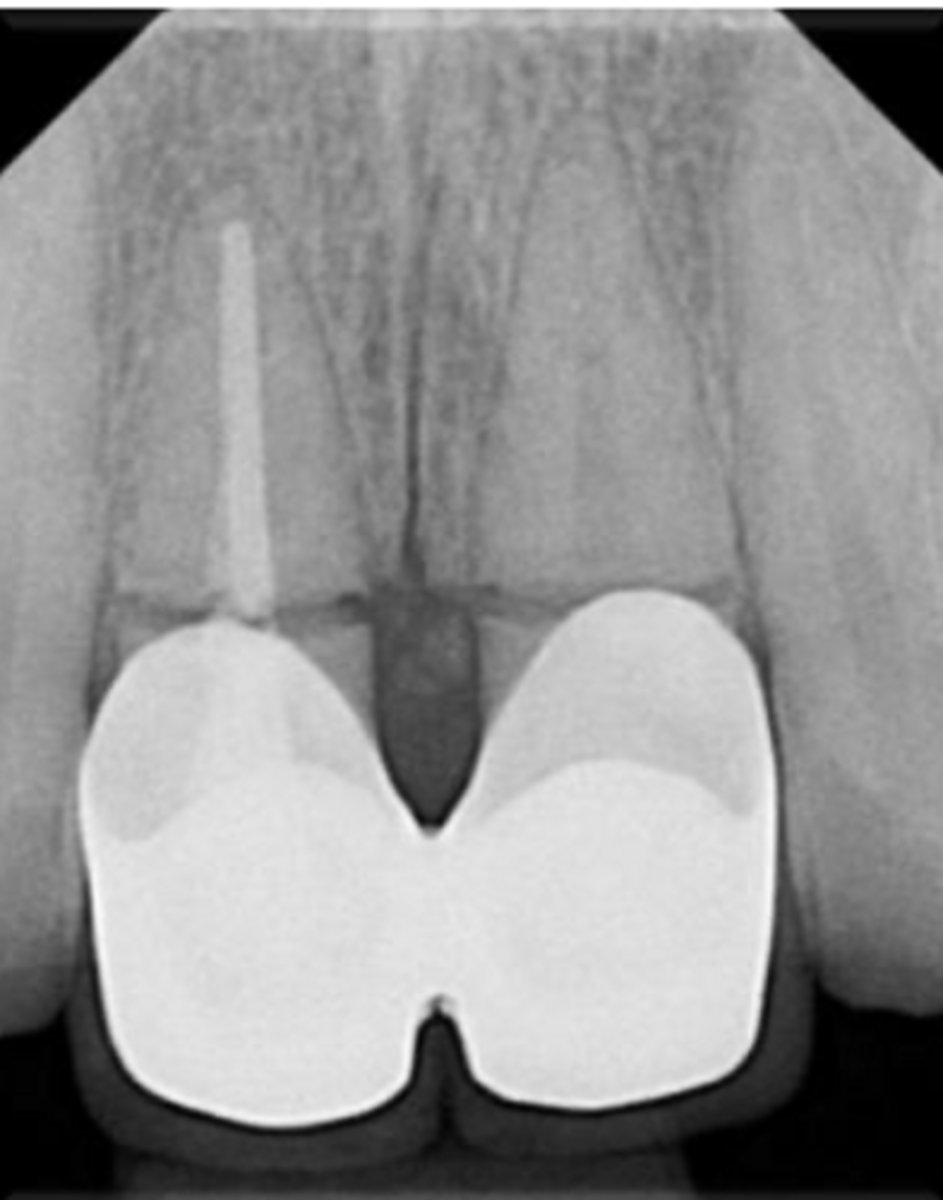
external resorption
ID the problem:
external resorption
ID the problem:

external resorption
ID the problem:
- 1 PA
- 1 BW
Which + how many radiographs should you take pre-op?
Locating canals
Guide file
Final file
Master cone
Sear down/ partial pack
Backfill
When should you take radiographs for intra-op?
PA with restoration and without rubber dam
Follow up
When should you take radiographs for Post-op?
Paralleling technique
What is the preferred radiographic technique in Endo?
Angulated radiographs
What type of radiographs are frequently used to identify superimposed objects or fractures?