Phonatory Final Exam
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
What is the role of the recurrent laryngeal nerve in voicing?
Supplies the motor control or function to all of the intrinsic laryngeal muscles except for the cricothyroid muscle
abducts (PCA) , adducts, increases and reduces tension of the vocal folds (TA)
What is the role of the superior laryngeal nerve in voicing?
internal - sensory and autonomic (thyrohyoid and supplies sensory fibers to laryngeal mucosa, laryngeal cavity, and superior surface of the VF.
external - motor and supplies the cricothyroid muscle.
laryngeal sensation is important for the reflexive functions of swallow and cough
What is the role of the intrinsic muscles of the larynx?
internal branch provides sensory (autonomic) input to the thyrohyoid, laryngeal mucosa, laryngeal cavity, and superior surface of VF
external branch provides motor input to cricothyroid
What are the layers of the vocal folds?
From top to bottom
Epithelium
SUPERIOR lamina propria
INTERMEDIATE lamina propria
DEEP lamina propria
thyrovocalis (vocalis muscle) AKA ‘the body’
What is the body cover theory?
a theory for how the VF vibrate.
Suggests that the COVER (epithelium and lamina propria) is passive with no neurological input
and that the BODY (thyrovocalis) is active with contractive properties
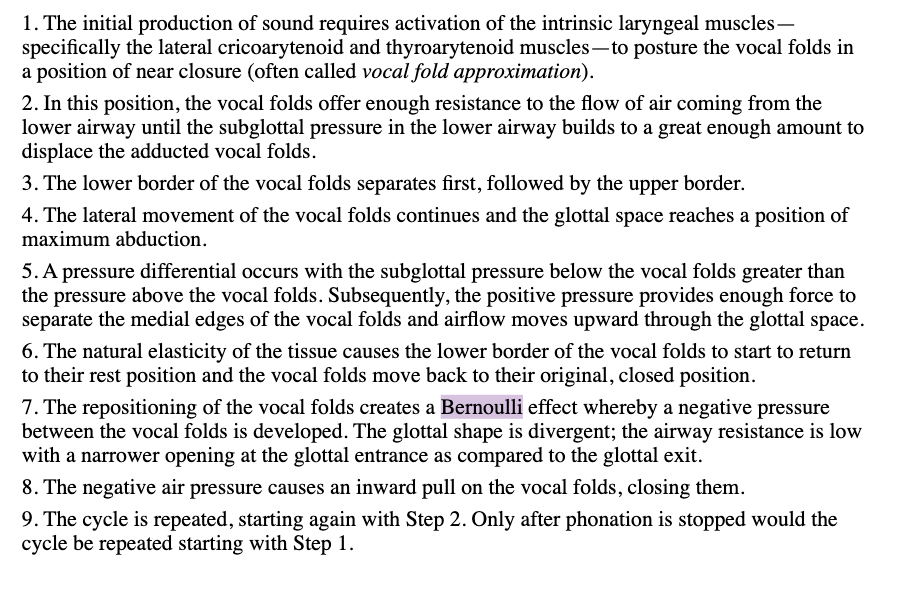
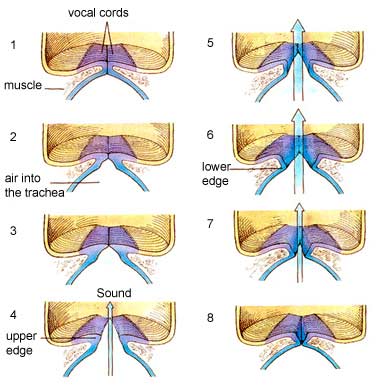
What are the main points of the Bernoulli effect?
the airstream will maintain a constant velocity until a point of glottal constriction - at which point the vocal folds with ‘blow’ apart.
at the point of glottic constriction, the velocity increases as the air passes through which ‘sucks’ the VF back together - due to the negative pressure created
Hirano’s body-cover theory is the _____ component while the Bernoulli effect is the _____ of this theory.
Myoelastic; aerodynamic
How does the Bernoulli effect impact vibration/oscillation of the vocal folds?
the repositioning of the vocal folds creates a Bernoulli effect whereby a negatie pressure between the VF is created causing an inward pull on the vocal folds - closing them.
the cycle repeats itself (vf open due to positive pressure and close due to negative pressure)
with increased resistance (such as mass or tension) greater pressure is necessary to both open and close the VF
What are the factors that affect frequency/pitch?
vocal fold length (affects tension and stiffness)
cricothyroid muscle affects VF length (CONTRACTION INCREASES PITCH)
thyroarytenoid makes VF more rigid (creating a faster rate of VF vibration)
What are the factors that impact amplitude/loudness?
increasing subglottal pressure (lung pressure increases peak glow rate and results in a greater vibratory amplitude of VF).
increased mouth opening and F0
alterations in phase lag between lower and upper margins of VF
What is and how does vocal tract resonance work?
It is how the shape and size of the vocal tract impacts how sound is changed after leaving the VF.
Areas that can influence resonance; larynx, phraynx, oral and nasal cavities, mouth opening, articulators (tongue, lips, cheeks etc).
What are the key components of vocal hygiene?
Smoking (cigarettes, vapes, marijuana), chewing tobacco, coughing and throat clearing, alcohol intake, caffeine intake, sleep deprivation, vocal load and vocal fatigue, loud talking, poor nutrition, obsesity, dehydration, allergies.
all of the above can contribute to or exacerbate an existing vocal challenge that a client has.
How is voice treatment different from voice surgery?
Voice treatment is a combination of exercises to, in some cases, strengthen the vocal cords, reduce tension, increase respiration-phonation coordination etc. and does not inherently change the structure of the vocal cords.
Voice surgery, on the other hand, are procedures that clients undergo to change the structure of their vocal cords. This can sometime be shortening or lengthening the cords, adjusting the tension of laryngeal structures, botox injections to increase mass etc.
What are the types of voice disorders?
Functional - disorders with an unknown cause that do not cause structural damage
Organic - disorders with an unknown cause that cause structural or neurological damage
Neurologic - caused or affecting the central or peripheral nervous sustem
What are some functional disorders?
muscle tension dysphonia, vocal fatigue, psychogenic voice loss, puberphonia, hyperfunction, gender affirming voice
What are some organic disorders?
nodules, polyps, cysts, edema, vocal cord paralysis, papilloma, webs, leukoplakia, cancer, sulcus vocalis, presbylaryngis
Can functional disorders lead to organic lesions over time?
yes
What are some neurologic disorders?
dysarthria (flaccid, spastic, ataxic, hypokinetic, hyperkenetic), unilateral true vocal fold paralysis, bilateral abductor true vocal fold paralysis, superior laryngeal nerve paralysis, essential tremor, hypophonia (associated with Parkinson’s), MS, ALS, MSA
What are the components of an evaluation?
Voice history
Patient interview
Case history of the voice problem
Effect of the voice problem
History of the voice problem
Duration of the voice problem
Variability/Consistency of the voice problem
Associated symptoms and sensations
Voice use (vocation, social
Health
Psychological impact (stress)
F0
Phonation range
Vocal Intensity
Perturbation (roughness)
Spectrogram
Air Volumes
Respiratory Movements
Observations and Descriptions (Noninstrumental objective measures (maximum phonation time, s/z ratio)
Recording
Questionnaires (VHI)
What are the main characteristics of hyperfunction?
What are the main characteristics of hypofunction?
Breathy voice caused by atrophy of the vocal folds
Strain and roughness if the patient is trying to copensate for the reduced closure by straining
Incomplete closure of the vocal folds
How do the components of evaluation affect therapy?
What is the difference between direct and indirect therapy?
What are the indications for use of hyperfunction as a therapy technique?
What are the indications for use of hypofunction as a therapy technique?
What therapy techniques work best for hypofunction AND hyperfunction?
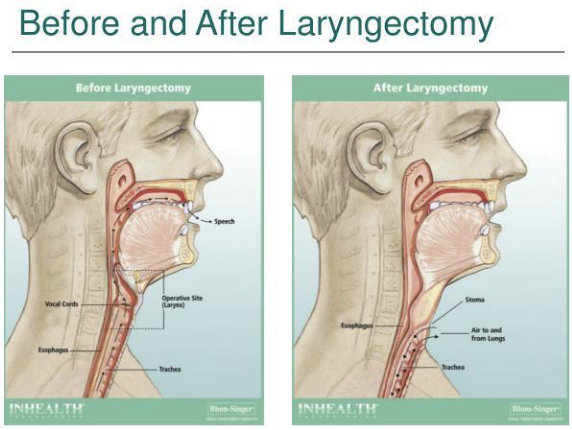
What is the difference between pre and post laryngectomy anatomy?
Trachea is dissociated from the upper airway
Permanent stoma is created in the neck for breathing
What are the types of laryngectomy?
Total Laryngectomy - done with large lesions
Endoscopic excision - carcinoma in situ on the cover of the VF
Cordectomy/Partial Cordectomy - all or part of the VF is surgically removed
Partial laryngecomy - vertical, horizontal, subtotal, near total
What are the alaryngeal communication options post laryngectomy?
Electrolarynx (a device that produces sound electronically and transmits the vibrations to the upper airway, move articulators to create speech sounds)
Esophageal speech (inject air into esophagus and directs is back out vibrating the tissue in the neopharynx - like burping)
Tracheoesophageal Speech (TEP) (small hole between trachea and esophagus to allow for a high-quality ‘voice’)
How do you determine TEP candidacy?
patient must be motivated
patient myst have adequate understanding of post surgical anatomy including TE puncture
patient must have pbasic understanding of function of the prosthesis
patient must demonstrate adequate manual dexterity to manage prosthesis
patient must have adequate visual acuity to manage stoma and prostehsis
patient must exhibit ability to care for prosthesis
patient should not have significatn hypopharyngeal stenosis
patient should demonstrate positive results following esophageal air insufflation test
patient must have adequate pulmonary support for prosthesis use
patient should have stoma of adequate depth and diameter for prosthesis to avoid airway occulsion
patient should be mentally stable
patient must be able to come to clinic in a timely fashion for prosthesis changes or be able and willing to complete changes on their own with patient changeable prosthesis
What are the considerations of a TEP?
What is some important terminology to know for counselling?
What is the SLP role in gender affirming care?
What is metatherapy?
What is the SLP role in trach care?
What is the SLP role in spasmodic dysphonia?