Cardiac cycle
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
pacemaker-capable tissues in order of rate (fast to slow)
-SA node
-AV node
-bundle of His
-Purkinje fibres
what is the pathway of the impulse that travels through the heart
-SA node → atrial muscle → AV node → Bundle of His → left and right bundle branches → purkinje fibres → ventricular muscle
what is the sinoatrial (SA) node
-small cluster of specialised cells
-in top corner of atrium
-provides heart with spontaneous electrical activity to drive beat
what are the key features of SA node
-diastolic depolarisation
-ap fires once membrane potential reaches threshold, doesnt need external input
-depolarises spontaneously faster than any other pace maker region
what is diastolic depolarisation
-unstable resting membrane potential
-slowly depolarises between beats
what makes SA nodes intrinsic rate high
-vagus nerve is constantly applying a slight brake
-req sympathetic stimulation
what is special about SA to AV conduction
-slow
-travels through ordinary atrial muscle
-not specialist tissue
what is special about AV node
-introduces a deliberate delay (AV pause)
-gives ventricle time to fill with blood before contracting
-acts as filter; prevents dangerous high atrial rates from being passed to ventricles
what is special AV node to ventricular muscle
-fast
-Bundle of His and Purkinje fibres are specialist conducting tissue
-speeds the impulse to the apex first
-so the ventricle contracts apex-to-base; pushing blood upward and out through the aorta and pulmonary artery
what does ECG measure
-measures potential difference between 2 electrodes places on body surface
-one is a reference and other is a recording electrode
how can ECG measure electrical activity from surface of body
-wave depolarisation spreading through heart creates a moving electrical dipole
-wave of positivity followed by wave of negativity
-can be detected from surface body using electrodes
-body’s fluid conducts electricity
who pioneered ECG
-Augustus Waller created it
-Willem Einthoven improved it
what are the different electrode positions
-Lead I: right arm to left arm
-Lead II: right arm to left foot
-Lead III: left arm to left foot
what changes when you change electrode positions
-timing of waves stay same
-shape of wave changes
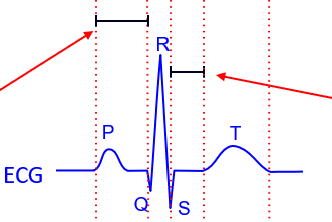
what are the different ECG waves
-P wave
-Q wave
-R wave
-S wave
-T wave
what is the P wave
-atrial depolarisation
-impulse spreads from SA node across both atria
-SA node too small to appear on ECG
-large atrial muscle activating is shown
what is Q wave
-first part of ventricular depolarisation
-septum depolarises first
-wave spreads away form recording electrode
-gives small downward deflection
what is R wave
-main ventricular depolarisation
-spreads towards apex (also towards recording electrode)
-gives large upward deflection
what is S wave
-depolarisation spreading back up walls of ventricle towards base
-moves away from electrode
-small downwards deflection
what is T wave
-ventricular repolarisation
-atria also repolarises
-but hidden underneath QRS complex
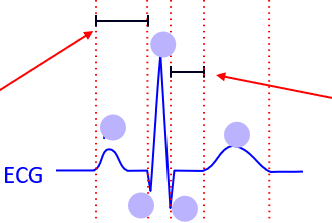
what is the PQ interval
-time from atrial depolarisation to ventricular depolarization
-shows atrial conduction and AV nodal delay
what does it mean if PQ interval is taking too long
-AV is blocked
-impulse is taking too long or failing to get through to AV node
what is QRS duration
-how quickly depolarisation spreads through ventricles via conduction
what does it mean if QRS duration is long
-bundle branch is blocked
-damage to His bundle or bundle branches
what is ST segment
-period when entire ventricle is depolarised
-no dipole is moving so lien is flat on baseline
what does it mean if ST segment is elevated
-part of ventricle has no AP
-sign of myocardial infraction
what is QT interval
-from ventricular depolarization to repolarisation
-equivalent to AP duration
what does it mean if QT interval is long
-long QT syndrome
what are the AV valves
-between atria and ventricles
-mitral valve (bicuspid): left atrium to left ventricle
-tricuspid valve: right atrium to right ventricle
what are semilunar valves
-at outflow tracts
-aortic valve: left ventricle to aorta
-pulmonary valve: right ventricle to pulmonary artery
how do valves open and close
-pressure driven
-if pressure is higher upstream side: valve opens, blood flows through
-if pressure is higher on downstream side: valve snaps shut
pressure volume changes in cardiac cycle
-A pressure is bit higher than V pressure
-mitral valve opens → blood flows into v → vol rises
-P wave fires → a contract → final top up of blood into v → vol inc (EDV)
-QRS fires → v starts contracting → v pressure rises
-a pressure rises → mitral valve shuts
-v pressure less then a pressure ; a valve stays shut
-both valves shut; pressure rises (isovolumic contraction)
-v pressure more than a pressure: a valve opens
-blood ejected into aorta; vol falls
-v relaxes; v pressure less than a pressure
-a valve shuts
-v pressure more than a pressure; mitral valve stays shut
-v pressure falls below a pressure → mitral valve opens -? v refills
what is EDV
-end diastolic volume
what is dicrotic notch
-small bump in a pressure trace
-v pressure less than a pressure
-a valve shuts
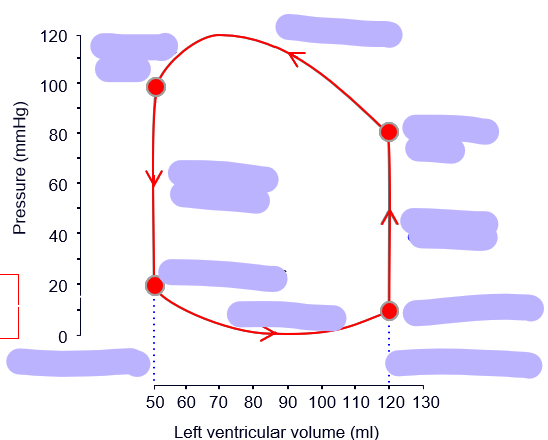
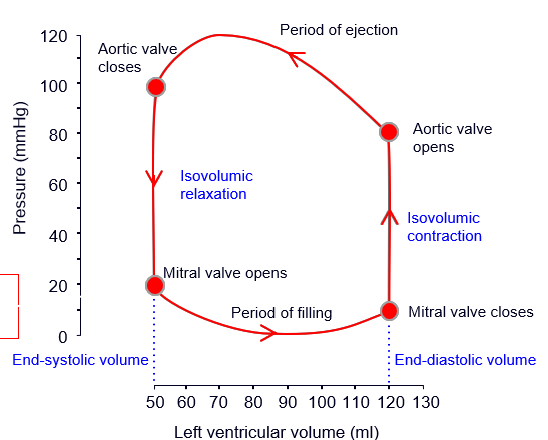
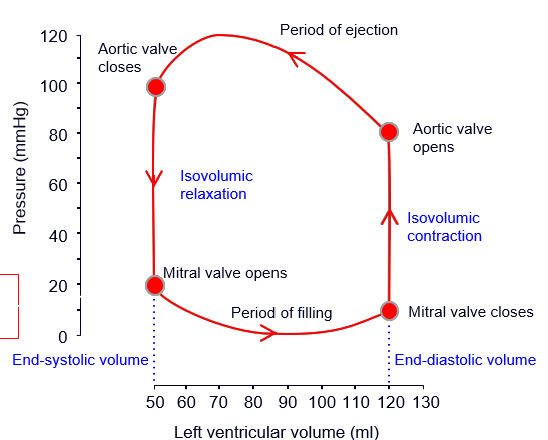
how to find stroke vol from this graph
-EDS - ESV
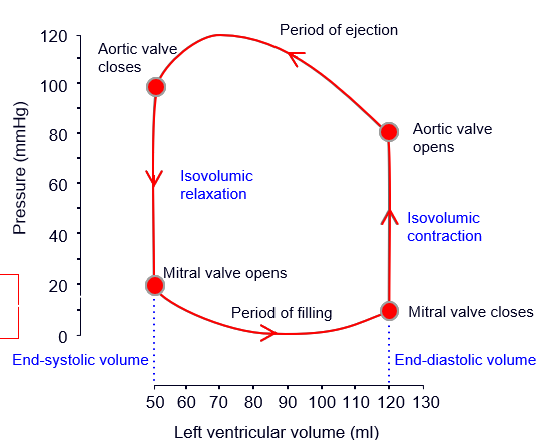
how to find ejection fraction from this graph
-stroke vol / EDV x 100
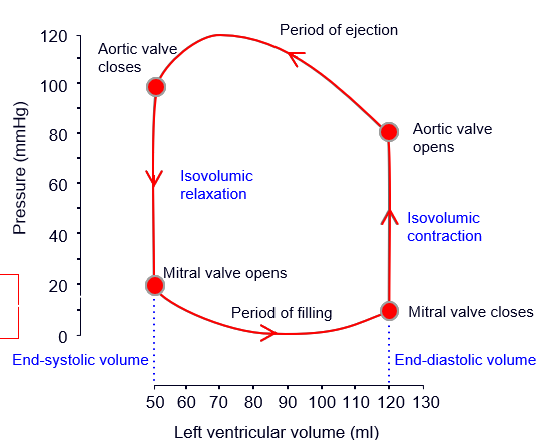
how to find stroke work
-area enclosed by loop