L4: Equine Esophageal Disorders
1/108
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
109 Terms
left cervical (60% or >2 ft, 39% in thoracic)
A majority of the equine esophagus is located in the _______________ region
Striated or skeletal
The cranial 2/3 of equine esophagus is _____________ muscle
Smooth
The caudal 1/3 of the equine esophagus is _____________ muscle
1. proximal esophageal sphincter
2. cardiac sphincter
what are the two sphincters of the esophagus
conduit for ingesta from mouth to stomach
what is the function of the esophagus
false; no digestive or absorptive role
T/F: the equine esophagus has a minor digestive or absorptive role
Vagus nerve
What nerve provides motor function to the esophagus?
Serosal layer
What layer is missing from the esophagus that causes surgery/healing post injury more complicated?
1. leakage from anastamosis or perforations
2. tension during swallowing or movement
the lack of serosal layer causes..
Dysphagia due to retention of feed, water or saliva
Clinical signs of esophageal disease are consistent with signs of _______________
1. Increased salivation
2. Nasal discharge (feed, water, saliva, mucopurulent)
3. Cough, regurgitation
4. Pain, anxious
5. Dehydration, anorexia
What are the clinical signs of esophageal disease?
Retention of feed, water or saliva in esophagus
Most signs of esophageal disease are secondary to what?
similar
the signs of dysphagia from esophageal disease are (similar/different) from other causes of dysphagia
nursing foals
esophageal obstruction from feed impaction or other primary esophageal disease is uncommon in which types of horses?
1. neuromuscular dysfunction of the palate or dummy foal
2. cleft palate
3. gastric ulcers
differential diagnoses for esophageal diseases or dysphagia in nursing foals
1. Nasogastric intubation
2. Endoscopy/esophagoscopy
3. Imaging: radiography, ultrasound
4. Oral examination
What diagnostics are used for assessing esophageal disease?
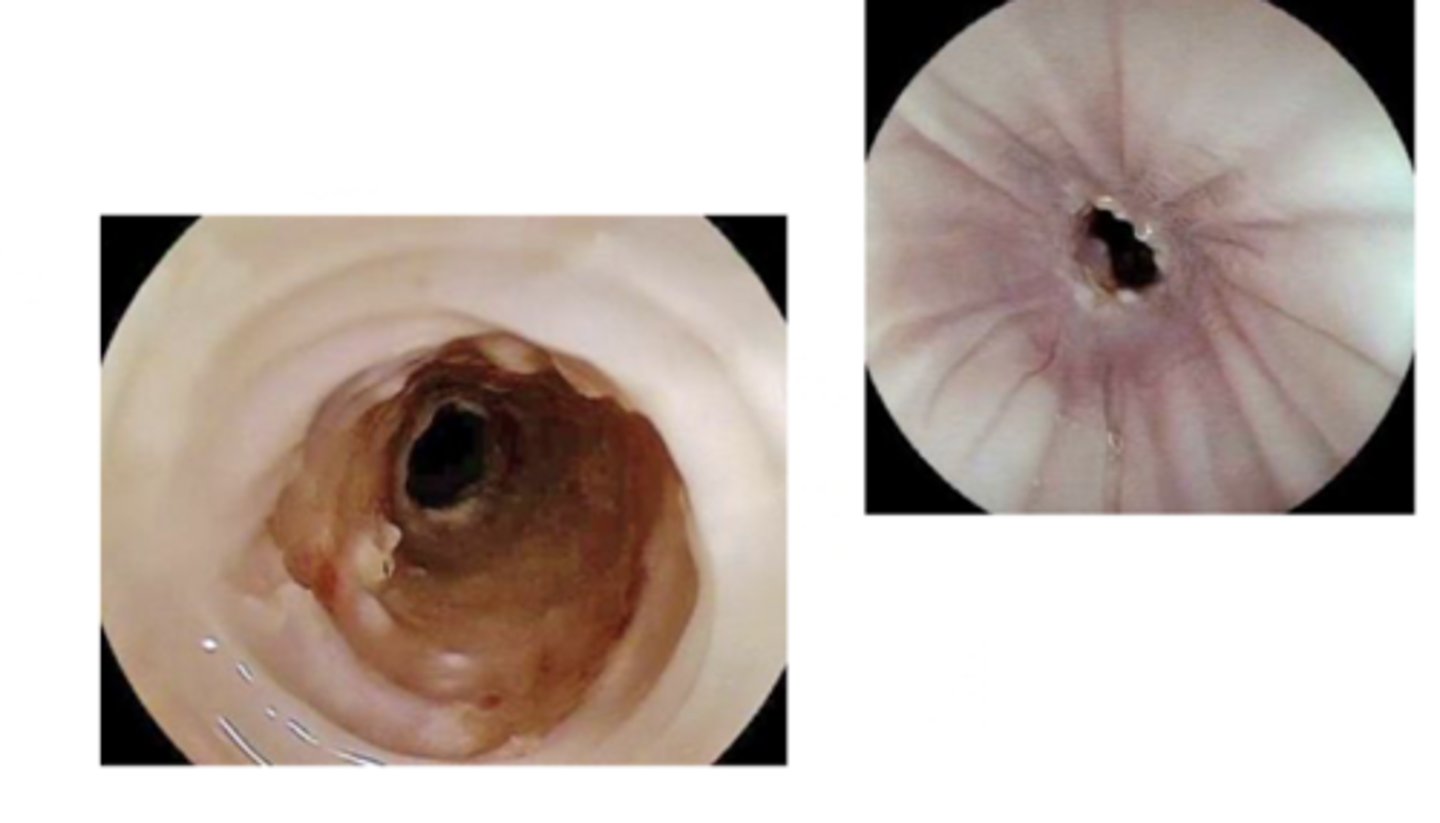
Endoscopy/esophagoscopy
Which diagnostics provide the most information for assessing esophageal diseases?
Endoscopy/esophagoscopy
_________ is essential for complete assessment of esophageal disease lumen and mucosa
1. localize and characterize abnormality
2. evaluate damage and complications
3. guide treatment
how is endoscopy and esophagoscopy used?
Cervical
UItrasound is used to evaluate the __________ esophagus
1. localize the probelm as obstruction, rupture mass etc.
2. evaluate esophageal wall thickness and integrity
3. identify extramural mass
purpose of ultrasound for the cervical esophagus
before
gas foci or gas dilation
survey radiographs should be performed (before/after) contrast studies and use to identify ___ or ___
Contrast esophagram
Radiographic evaluation of motility, complicated obstruction, stricture, diverticula, and masses
1. Positive contrast
2. Negative contrast
3. Double contrast
What types of contrasts can be used for contrast esophagrams?
1. Barium sulfate (liquid or paste)
2. Iodinated contrast
What are examples of positive contrast?
Aspiration
What should you be cautious about when using iodinated contrast for a contrast esophagram?
Negative contrast
Air
Double contrast
Air and barium
Double contrast
Which type of contrast is optimal for mucosal detail?
perforation or aspiration
use caution with contrast when ________ is suspected or when increased risk of _________
Pharyngeal muscles
The proximal esophageal sphincter is formed by ____________
Smooth muscle
The distal esophageal sphincter is comprised of _______________
Primary esophageal obstruction
"Simple choke"; intraluminal obstruction; very common emergency
true
T/F: Primary obstruction can occur in any aged horse
1. Dental problem - older horses
2. Rapid feed ingestion ("wolfing")
3. Sedation/ feeding while sedated
4. recent episode of dysphagia, diverticula, abnormal motility
What are predisposing factors for primary esophageal obstructions?
1. Masses (cervical or mediastinal)
2. Foreign bodies
3. Congenital problems
4. Diverticula
5. Strictures
Secondary esophageal obstructions are less common and typically occur from what?
1. Post pharyngeal
2. Thoracic inlet
3. Base of heart
4. Terminal esophagus
primary obstructions can occur anywhere but are most common at locations of esophageal narrowing, what are they?
1. Bilateral nasal discharge (feed, saliva, +/- mucopurulent)
2. Increased salivation
3. Anxiety, distress, sweating
4. Cough, retching, neck extension
5. Pain
6. Frequent attempts to swallow
7. Focal swelling/edema along neck
What are clinical signs of esophageal obstruction?
1. Sedation and gentle nasogastric intubation
2. Endoscopy (definitive)
What are the initial diagnostics for esophageal obstruction?
Provide NOTHING by mouth until horse is evaluated
If you are worried a horse might have choke based off what an owner describes to you, what should you tell the owner?
true
T/F: Uncomplicated obstructions may resolve without treatment
1. Lower head
2. Reduce anxiety
3. Analgesia
4. Dislodge impaction
What are the treatment goals for esophageal obstructions?
1. Sedation - alpha 2 agonist (xylazine, detomidine)
2. Passage of nasogastric tube +/- gentle lavage
3. Antimicrobials, analgesia (NSAIDs), fluids (if prolonged or complicated)
4. If obstruction does not resolve, consider referral if an option
How do you treat uncomplicated (acute) obstruction?
1. Endoscopy (assess mucosal damage and healing)
2. Continued nasogastric intubation and lavage
3. pharmacologic therapy w/ a-2 and xylazine
4. Supportive care (antimicrobials, NSAIDs, IVF)
5. Surgical correction as last resort
What is involved in management of complicated/prolonged esophageal obstructions?
1. protect airway
2. sedation, head below thoracic inlet
3. general anesthesia is needed in rare cases
when passing a NG tube with complicated obstructions. ..
Esophagotomy
What is considered a last resort for treating complicated/prolonged esophageal obstructions?
1. Dehiscence
2. Laryngeal hemiplegia
3. Other (horners syndrome, chronic esophageal obstruction, aspiration pneumonia)
What are the surgical complications associated with esophagotomy?
1. 2% lidocaine via NG tube about 50 mL
2. Oxytocin
3. Buscopan
What are the pharmacologic treatment options for obstruction?
esophageal spasm
lidocain is use to alleviate __ __
Skeletal
Oxytocin reduces ___________ muscle tone in proximal 2/3
anticholinergic parasympatholytic agent
MOA of bucospan
Smooth
Buscopan causes __________ muscle relaxation
true
T/F: There is mixed to little evidence that pharmacological treatment options are successful
1. Dehydration
2. Electrolyte or acid base abnormalities
3. Aspiration pneumonia
4. Reobstruction
5. mucosal ulceration
(Also: failure to resolve/prolonged, esophageal trauma, esophageal rupture)
What are the most common complications from prolonged or recurrent obstruction?
Alkalosis
Electrolyte loss due to esophageal obstruction leads to metabolic (acidosis or alkalosis)
usually due to mixed bacterial infection that is treated with broad spectrum antimicrobial
aspiration pneumonia/pleuroneumonia as a complication
loss of free water with hyponatremia, hypocholremia, hypokalemia leading to metabolic alkalosis with treatment via IV fluids
fluid/salivary and electrolyte loss as a complication
Duration of obstruction and presence of mucosal damage with greatest risk 24-48 hours post resolution
Acute reobstruction risk increases with what?
24 to 72 hours
To avoid acute reobstruction, reintroduce soft feed gradually ___________ post resolution
true
T/F: It may take up to 3 weeks to return to normal diet when preventing acute reobstruction
1. Severe mucosal injury
2. Impaired motility, dilation
3. Strictures, diverticulum, perforation
4. Esophagitis
What are risks for recurrent obstructions?
1. Dental care (especially for older horses)
2. Diet (hay quality, pre soak feed)
3. Do NOT feed a sedated horse
4. Prevent rapid feed ingestion
How do you prevent esophageal obstruction?
Post obstruction due to pressure necrosis and circumferential ulceration
What is the most common cause for esophageal stricture?
1. History of recurrent obstructions
2. Endoscopy
3. Double contrast esophagram
How do you diagnose esophageal stricture?
Medical management
___________ should always occur first, especially if acute, for treating esophageal stricture
1. Soft diet
2. Antimicrobials
3. NSAIDs
What is involved in medical management of esophageal strictures?
2 months
What is the treatment duration for medical management of esophageal strictures?
1. Balloon dilation
2. Surgical resection and anastomosis
What is included in treatment of chronic strictures or those that do not respond to medical therapy?
false; chronic
T/F: acute strictures have a less favorable prognosis
Cervical
Esophageal perforation typically involves the __________ esophagus
1. Prolonged/severe obstruction
2. Trauma (external - kick, NG intubation, severe obstruction)
What are causes for esophageal perforation?
1. Draining fistula
2. Tissue necrosis
3. Cellulitis
4. Edema
5. SQ emphysema
6. Abscess
What are clinical signs of esophageal perforation?
Grave to poor
The prognosis of esophageal perforation is what?
Primary
A _____________ surgical closure should only be done if an esophageal perforation is acute (<12 h) and no contamination
Secondary
A (primary/secondary) closure for esophageal perforation is most typical due to contamination and/or duration on presentation
1. indwelling feeding tube
2. longterm broad spec antimicrobial
3. addressing extensive salivary/electrolyte loss
4. septicemia and cellulitis common findings
secondary closure of esophageal perforation involve?
Cervical
Esophageal diverticula typically localize to the ____________ esophagus
1. Congenital - Friesian horses
2. Trauma
What are causes for esophageal diverticula?
Recurrent obstruction but can be asymptomatic
Signs of esophageal diverticula are often similar to what?
Contrast radiography (could also do endoscopy but sedation can mask it so it can be hard to diagnose this method)
What is the ideal way to diagnosis esophageal diverticula?
1. Dietary management
2. Surgical repair (of small diverticula rare)
What is the treatment for esophageal diverticula?
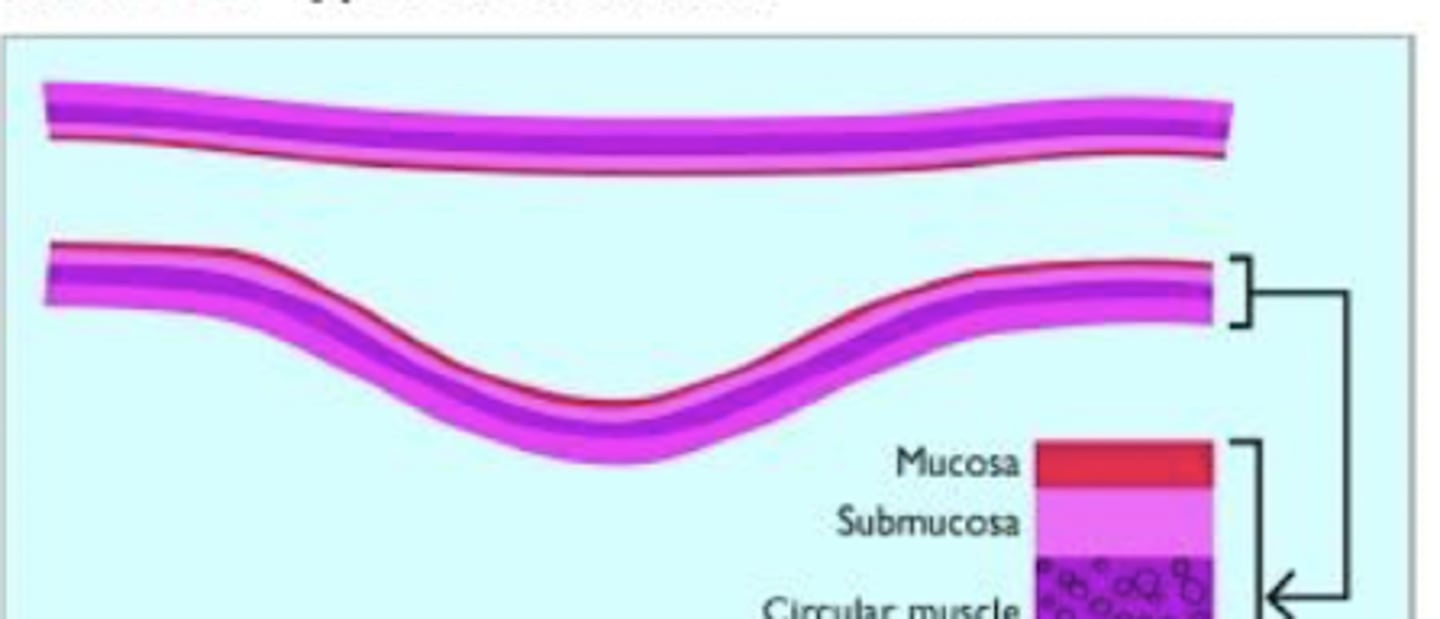
Traction and pulsion/hernial
What are the two types of diverticula?
Traction diverticula
A true diverticula of the mid-esophagus that is usually asymptomatic associated with post trauma, rarely feed entrapment
Pulsion diverticula
A hernial diverticula of the esophagus that is associated with feed entrapment and therefore increased risk of obstruction or rupture
traction
ID type of diverticulum
pulsion
ID type of diverticulum

Esophagitis
Inflammation and ulceration to mucosa of esophagus
1. salivary and food buffers
2. peristalsis
3. gastroesophageal/cardiac sphincter
normal esophageal mucosal protection involves...
1. increased salivation or retching
2. inappetence and weight loss if chronic
clinical signs of esophagitis may mimic recurrent obstructions like
Reflux
___________ esophagitis is most common
1. Chemical injury from gastric acid and bile salts (most common)
2. Prolonged intubation
3. Trauma
4. Neoplasia
5. Toxin
What are causes for esophagitis?
1. Gastric emptying or motility disorder (pyloric outflow obstruction)
2. Lower esophageal sphincter dysfunction
3. Severe intestinal ileus
4. Severe equine gastric ulcer syndrome (EGUS)
What are causes for reflux/chemical esophagitis?
1. Full gastroscopy
2. Abdominal ultrasound
3. +/- assessment of motility with contrast radiography
What should you always perform if you identify esophagitis?
address the primary cause if possible
what should you do first when managing a case of esophagitis
1. Sulcralfate
2. Control gastric acidity
3. Bethanechol (prokinetic; if you suspect motility disorder)
4. Dietary management and supportive care
How do you manage esophagitis?
sucralfate
what drug acts as a mucosal protectant
PPIs like omeprazole
H2 antagonists like famotidine
what drugs act to control gastric acidity
Megaesophagus
Chronic dilation and hypomotility of esophagus
Friesian horses
Congenital megaesophagus is common in what breed of horse?
Acquired
(Congenital or acquired) megaesophagus is more common