Week 3
1/36
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
37 Terms
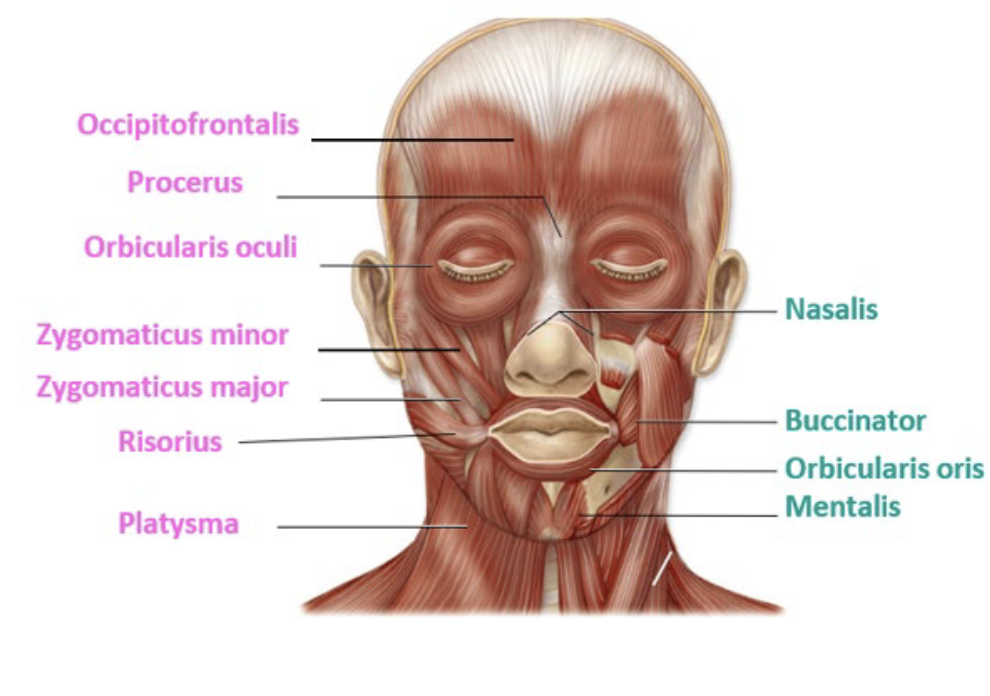
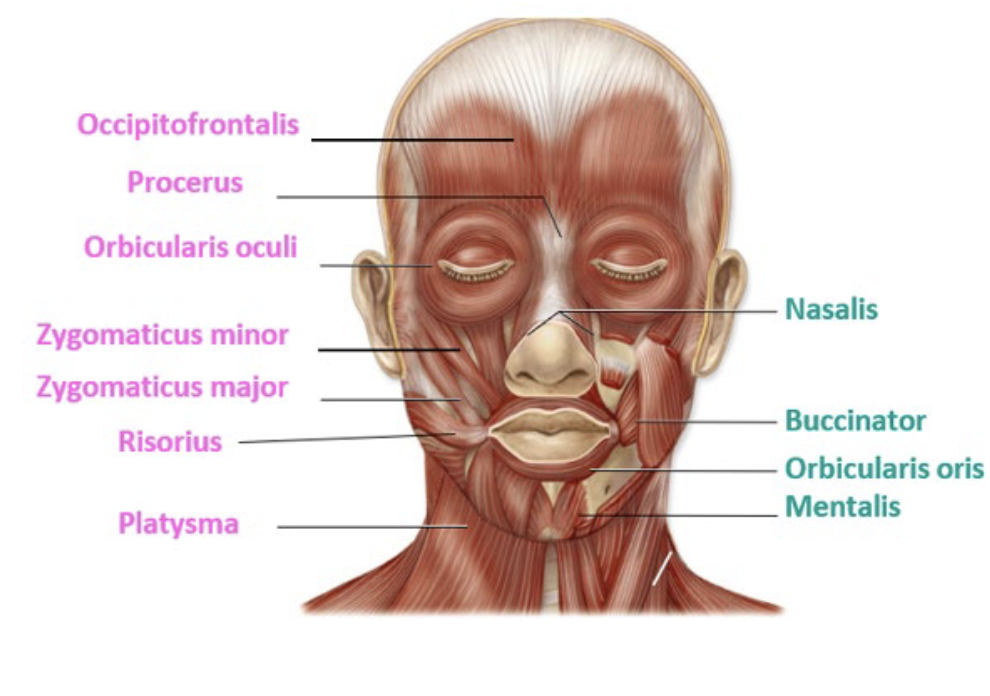
Buccinator + orbicularis oris
Zygotematicus major + minor
Risorius
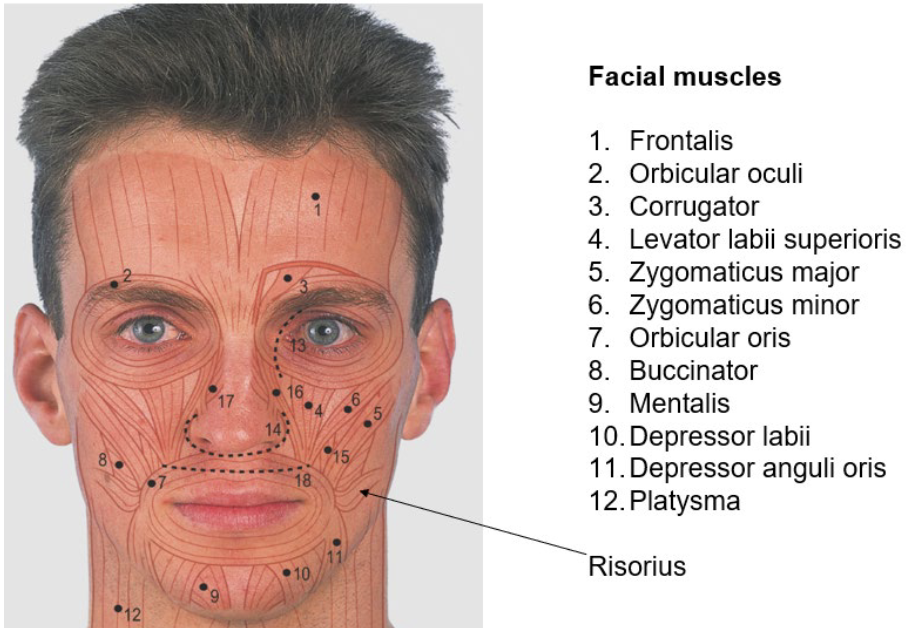
Risorius + depressor labii inferioris
levator labii superioris + depressor labii
dilators of the mouth: risorius plus levator labii superiorirs + depressor labii inferioris
Orbiculris oris
depressor anguli oris
Mentalis
Platysma

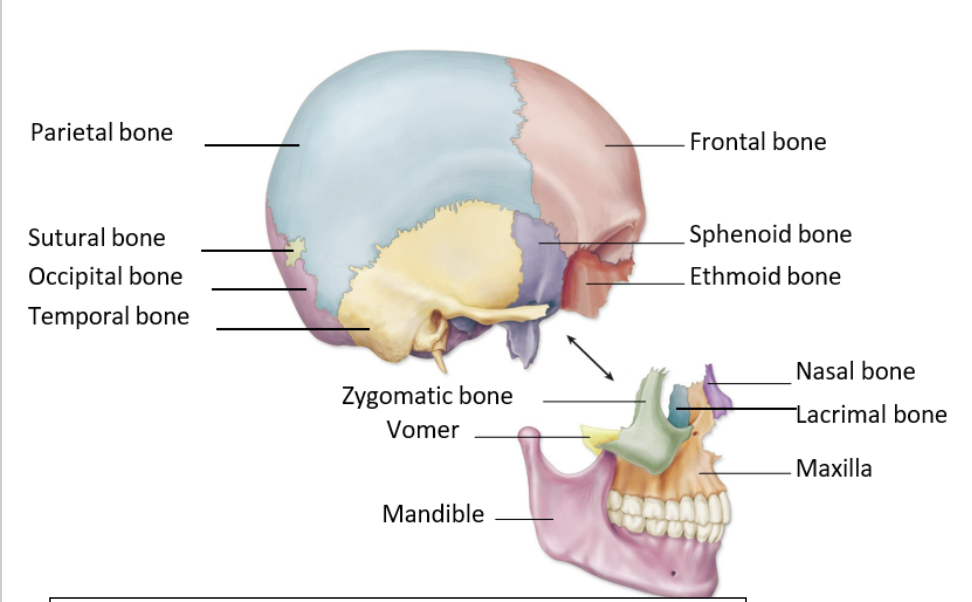
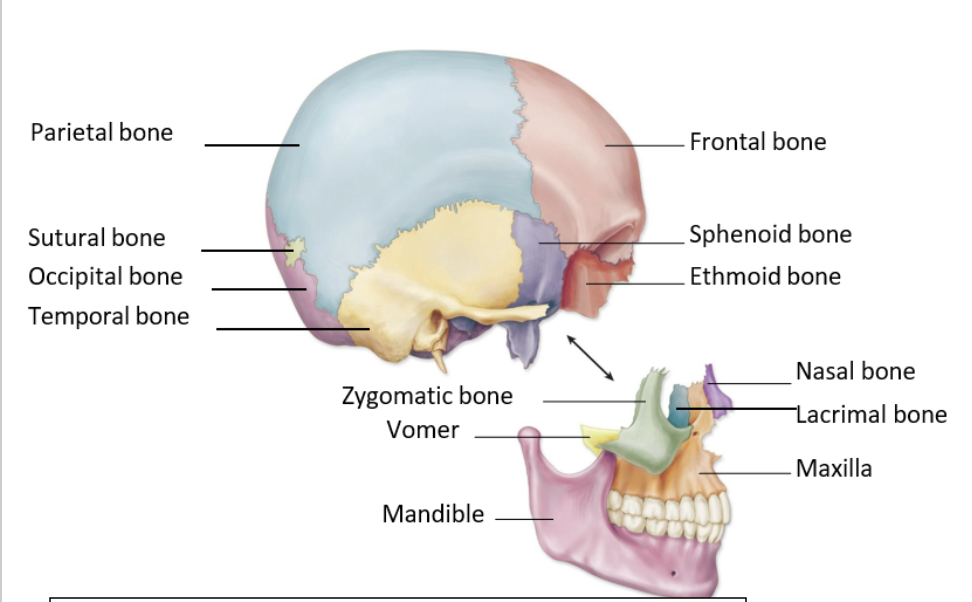
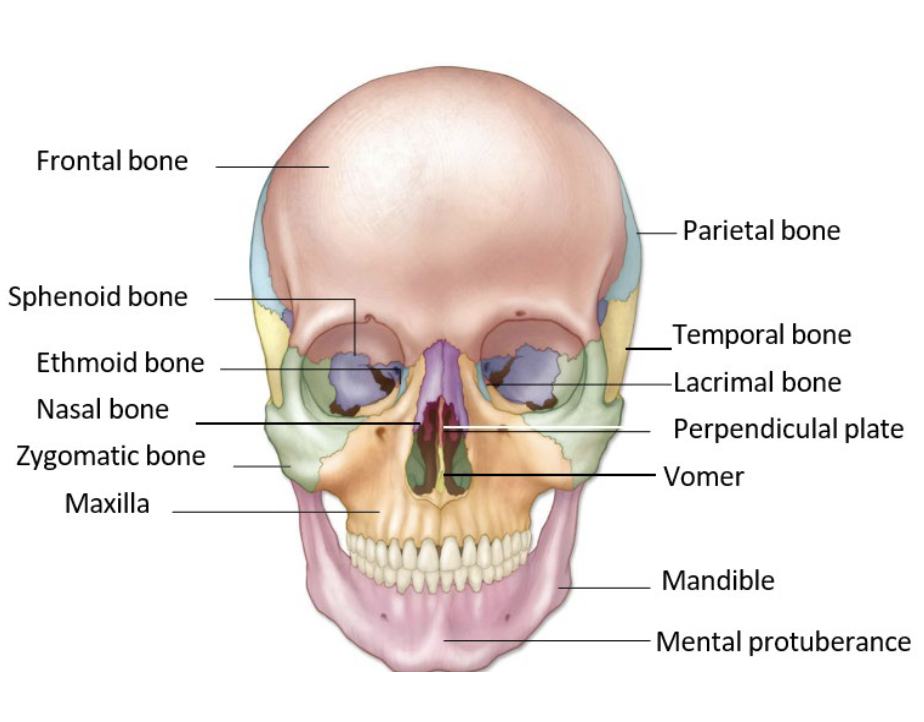
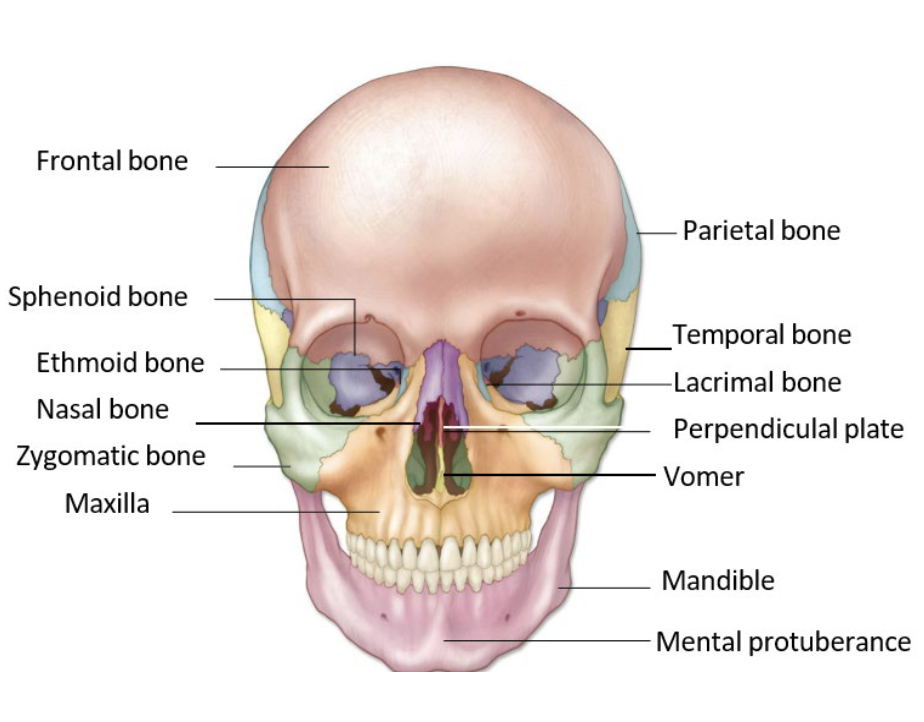
Which of the following bones is classified as a cranial (skull) bone?
frontal bone
Which structure is the only movable bone of the skull and face
mandible
The temporomandibular joint (TMJ) is best classified as which type of joint?
synovial condyloid joint with hinge characteristics or modified synovial hinge joint
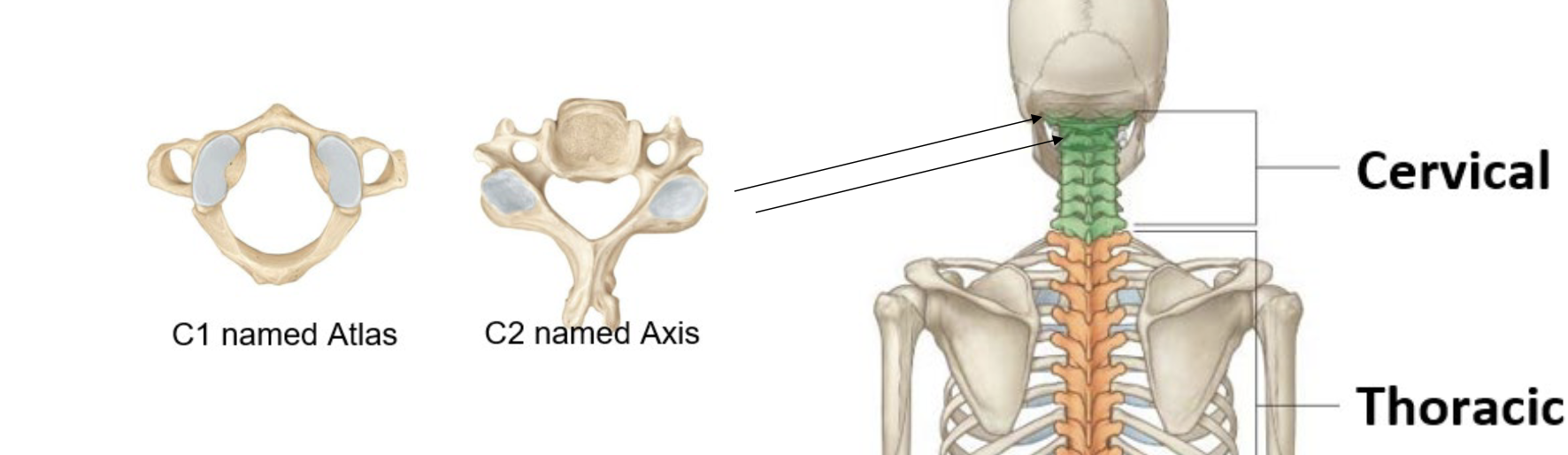
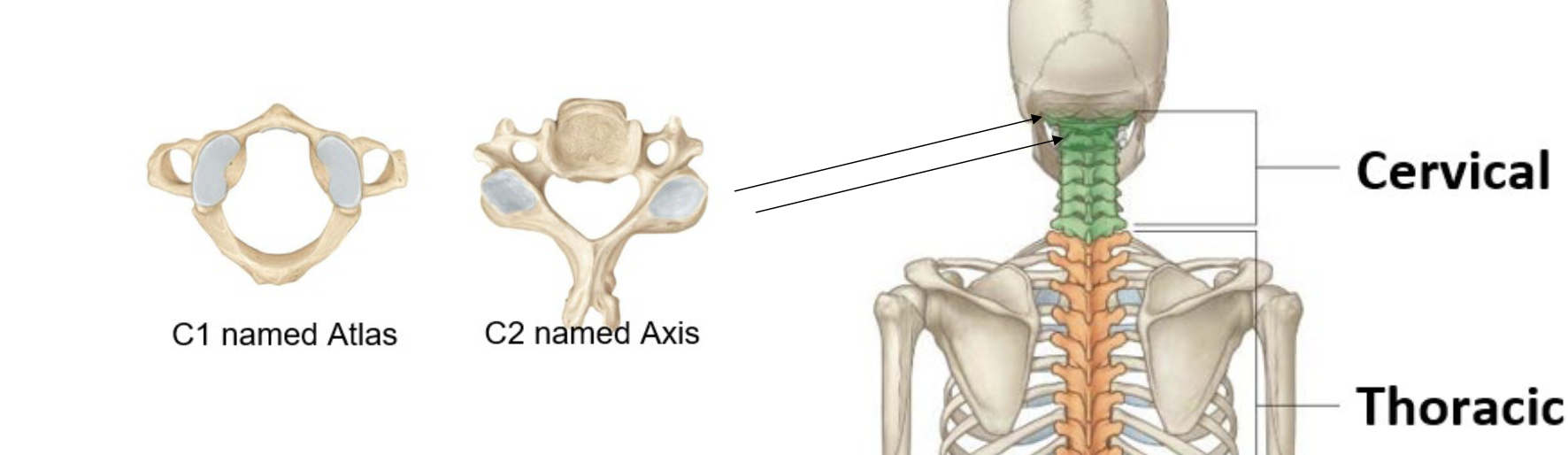
The articulation between C1 (atlas) and the occipital bone primarily allows which movement?
flexion and extension
The articulation between C1 (atlas) and C2 (axis) primarily allows which movement?
lateral rotation
Which muscle when you clench your teeth, can be palpated (felt) contracting at the angle of the mandible
masseter
The hyoid bone is unique because it:
has no bony articulations
Which muscle group primarily stabilises the cervical spine and head?
deep vertical flexors
The sternocleidomastoid muscle produces which action when contracting unilaterally?
oblique rotation
what is a characteristic most associated with older adults
low bone density
What movements can the temporomandibular joint perform?
depression (opening), elevation (closing), protrusion (forward), retrusion (backward), and lateral deviation (side-to-side)
What muscles preform depression (opening), elevation (closing), protrusion (forward), retrusion (backward), and lateral deviation?
masseter, temporalis, medial pterygoid, and lateral pterygoid
Name the muscle group and the function of the muscle group that move the hyoid bone
muscle group: supra hyoid, action: elevate and help swallow food
muscle group: infra hyoid, action: depresses + stabilise
State two functions of the hyoid and the reason why the hyoid bone needs to move:
Swallowing (Deglutition): During swallowing, the hyoid moves upward and forward (anterior-superior) to raise the larynx and open the esophagus for food passage, preventing aspiration.
Speech and Tongue Movement: The hyoid serves as a stable yet mobile attachment point for the muscles of the tongue, allowing for complex movement required for vocalization and speech articulation
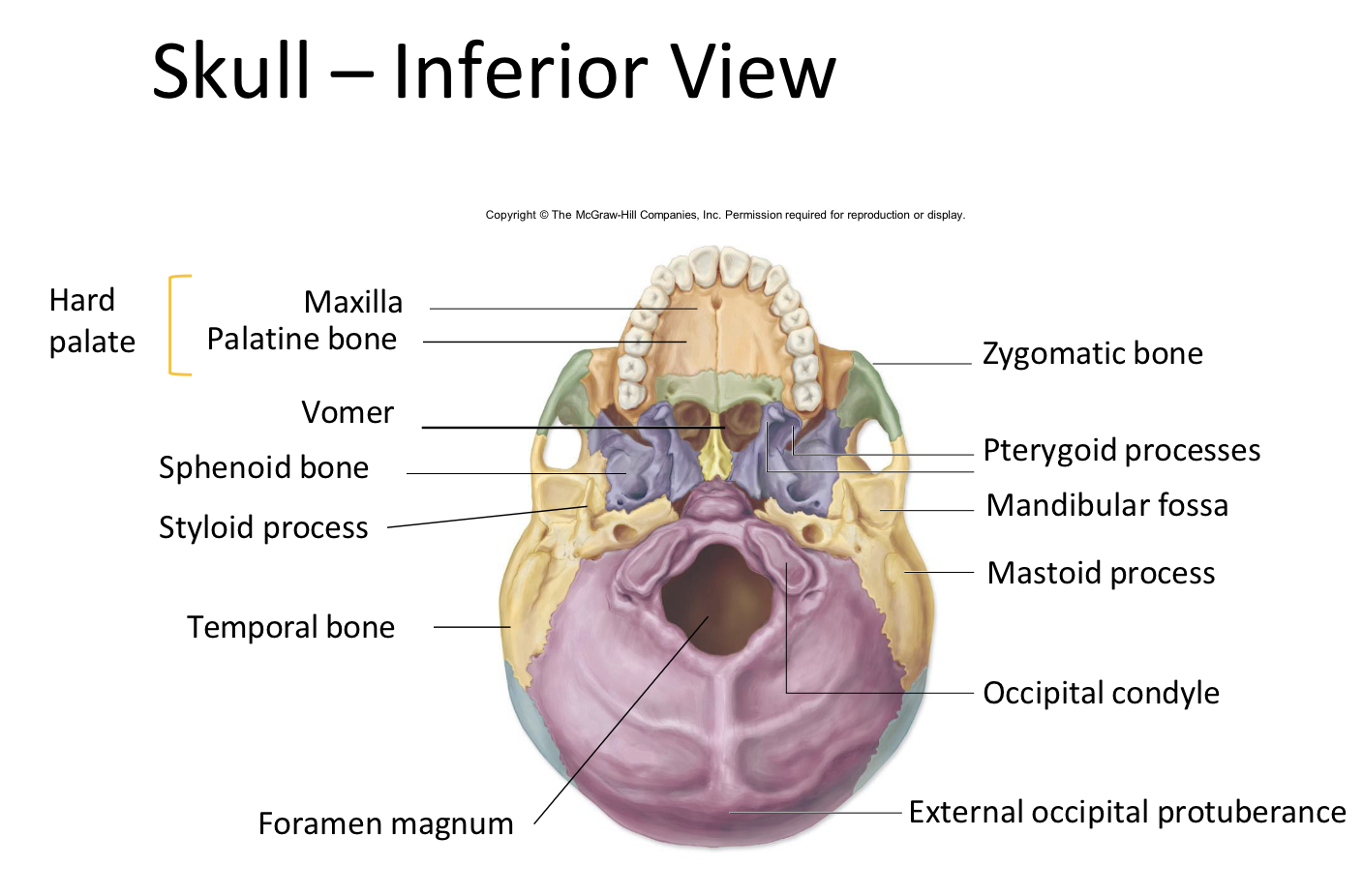
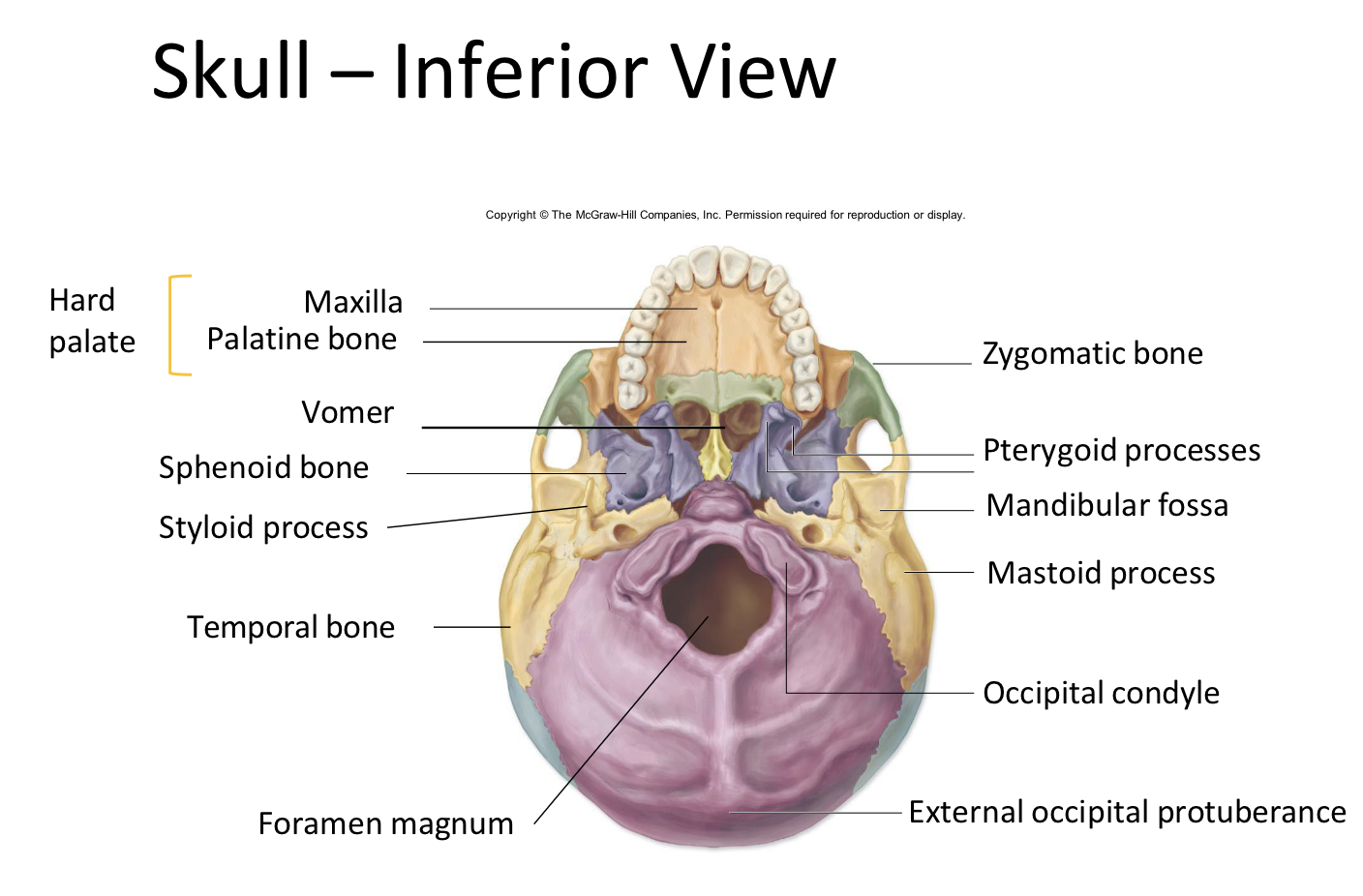
What is the name of the bony landmark and bone the spinal cord leaves the brain stem to travel down the vertebral column?
fortnum magnum of the occipital bone
Describe the discriminating sex characteristics of tendons, ligaments and connective tissue, and the outcomes of these differences
1. Key Sex Characteristics of Connective Tissue
Research indicates that females often have more compliant (less stiff) tendons and greater ligament laxity compared to males, largely influenced by estrogen. [1, 2]
Tendons: Males generally have larger, stiffer tendons (e.g., Achilles, patellar) with a greater cross-sectional area (CSA). Female tendons are more compliant, meaning they deform or stretch more under the same load. [1, 2]
Ligaments: Females possess greater joint laxity (looser joints) and lower collagen cross-linking, which reduces structural stiffness compared to males. [1, 2]
Collagen Turnover: Estrogen levels in females influence collagen synthesis rate; while it helps in recovery, high estrogen can reduce fibrillar cross-linking. Testosterone in males promotes higher collagen turnover and content, contributing to increased tendon stiffness. [1, 2, 3, 4]
2. Outcomes of Differences
These intrinsic differences result in distinct musculoskeletal, biomechanical, and injury profiles:
Increased Female Injury Risk (ACL): Women are 4-6 times more likely to experience non-contact Anterior Cruciate Ligament (ACL) injuries in the knee due to increased ligament laxity and reduced stiffening, which causes lower stability under sudden force. [1, 2, 3, 4, 5]
Increased Male Injury Risk (Achilles): Men are roughly four times more likely to experience Achilles tendon ruptures. While their tendons are stiffer, the higher loads imposed by superior muscle mass, combined with potentially less elastic tissues, make them prone to acute rupture. [1, 2, 3]
Adaptability to Training: Female tendons typically demonstrate lower adaptability (lower stiffness increases) to resistance training compared to male tendons. [1, 2]
Menopause and Aging: As estrogen drops in post-menopausal women, tendon health can decline, leading to increased stiffness, reduced collagen repair, and a higher risk of tendinopathies. [1, 2]
Performance Differences: The higher stiffness in male tendons allows for more direct, efficient force transmission during explosive movements, while the compliance in female tissues can aid in different types of athletic movements
Provide the name and describe the joint type and classification of the only moveable joint of the skull
Name: TMJ
Type and Class of joint: synovial condolyoid with hyinge characteristics (or modified hyinge joint)
When turning head upward to look at the sky, what is this movement called, and which muscle is the primary agonist for this bilateral contraction?
Movement: head + neck extension
Muscle: splenus capitus
An elderly patient presents with neck pain and headaches following a minor motor
vehicle accident in which their stationary vehicle was struck from behind. (5 marks)
a) Describe the harmful structural movements that occurred to the head and neck during this accident.
Neck hyperflexsion + extension:
These rapid extension and flexion movements can damage cervical muscles, ligaments, facet joints, intervertebral discs, and surrounding soft tissues, resulting in neck pain, stiffness, and headaches commonly associated with whiplash injuries
Using your knowledge of head and neck anatomy, identify TWO lifespan decrements relevant to this patient and explain how each decrement worsens the outcome of this minor acciden
Life Span Decrement | Possible Reasons for Neck Pain and Headaches |
|---|
Neuromuscular coordination decline | Slower muscle activation reduces neck stability during whiplash, causing greater tissue strain and pain. |
Reduced bone density (osteoporosis) | Weaker cervical vertebrae are more susceptible to injury and pain from sudden forces. |
Sarcopenia | Weaker neck muscles provide less support, allowing greater cervical movement and soft tissue injury. |
Loss of ROM and lax ligaments/tendons at cervical spine | Reduced flexibility and support increase the risk of ligament and joint injury during whiplash. |
Slowed central processing and reaction time | Delayed protective responses prevent bracing for impact, increasing neck movement and injury. |
Reduced proprioception | Poor awareness of neck position reduces stability, leading to excessive movement and tissue strain. |
A female rugby league athlete presents complaining of neck pain, tight muscles in her neck. After a
long chat she also tells you that lately she has been suffering from
Headache
Nausea
Sensitivity to light or noise
Difficulty concentrating
Memory problems (especially recent events)
Feeling “slow” or foggy
Mood swings
Sleeping more than usual
Trouble falling asleep
Using your knowledge of head and neck anatomy, explain how anatomical structures, neuromuscular
function, and sex-specific characteristics may contribute to her injury risk of sub concussive trauma.
In your answer, link structure → movement → injury mechanisms
Sub-concussive Trauma in a Female Rugby League Athlete (7 marks)
Structure | Function | Injury Mechanism (Structure → Movement → Injury) |
|---|---|---|
Cervical spine (vertebrae, discs, ligaments) | Supports and stabilises the head while allowing movement. | Repeated tackles and impacts cause rapid flexion, extension, and rotation of the neck. These forces can transmit to the skull and brain, contributing to sub-concussive trauma and neck pain. |
Neck muscles (sternocleidomastoid, trapezius, deep neck flexors) | Stabilise the head and absorb forces during movement. | If neck muscles are tight, fatigued, or relatively weak, they are less able to absorb impact forces. More force is transferred to the brain, increasing injury risk and causing neck pain. |
Brain (especially frontal and temporal lobes) | Responsible for memory, concentration, mood, and cognition. | Repetitive acceleration-deceleration forces cause the brain to move within the skull, producing microscopic neuronal damage. This may result in headaches, memory problems, difficulty concentrating, and feeling "foggy." |
Vestibular system (inner ear and brainstem) | Maintains balance and spatial orientation. | Repeated head impacts can disrupt vestibular function, causing nausea, dizziness, and sensitivity to motion. |
Visual and auditory pathways | Process light and sound stimuli. | Neural irritation following repeated impacts can increase sensitivity to light and noise. |
Neuromuscular function | Coordinates muscle activation to protect the head and neck. | Delayed or inadequate muscle activation reduces the ability to stabilise the head during contact, increasing brain movement inside the skull. |
Female sex-specific characteristics | Females typically have smaller neck circumference, lower neck muscle mass, and lower neck strength than males. | Reduced neck strength may allow greater head acceleration during collisions, increasing the risk of sub-concussive and concussive injuries. Hormonal influences may also affect symptom severity and recovery. |
Summary Link
Smaller/weaker neck structures + reduced force absorption → greater head acceleration during tackles → increased brain movement within the skull → sub-concussive trauma symptoms (headache, nausea, memory and concentration problems, mood and sleep disturbances).