exam 1 -part 2
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
54 Terms
preschool aged nutrition
The preschool child requires a well-balanced diet with fat content between 20-30% of calories consumed.
Adequate physical activity and provision of a nutrient-dense diet (rather than foods high in fat and sugar) are the foundation for obesity prevention
Preschoolers are erratic eaters and will eat very well one day and then may eat very little the next day. Food jags are not common in the preschooler but are common in the toddler.
small portions on smaller sized plates and bowls with
appropriately sized utensils
Encourage child to serve self
Allow child to decide when to stop eating (don’t force food)
Snacks should be high quality (lean proteins, whole grain, fruits, veggies, dairy)
Family mealtimes allow parents to model appropriate behaviors at meals and facilitate communication
preschool ages nutrition - levels
500 to 800 mg calcium
10 mg iron
19 mg fiber
Saturated fats less than 10%
Diet high in nutrient-rich foods
Limited amounts of poor-, high-calorie foods (fruit juices)
Regular meals with healthy snacks in between
preschool aged mental processes
Cognitive development moves form an egocentric approach to the world toward a more empathetic understanding of what happened outside of the self
preschool aged mental processes - magical thinking
normal part of preschool development. In magical thinking, the preschooler believes that his or her thoughts are all-powerful. The fantasy experienced through magical thinking allows the preschooler to make room in his or her world for the actual or the real. Through make-believe and magical thinking, preschool-age children satisfy their curiosity about differences in the world around them.
preschooler - animism
The preschooler also attributes life-like qualities to inanimate objects (_animism_) gives further examples illustrating this developmental stage
preschooler - imaginary friends
The imaginary friend is not real and exists only in the child’s imagination. This friend serves as a creative way for the preschooler to sample different activities and behaviors and practice conversational skills. Despite this imagination, the preschooler is able to switch easily between fantasy and reality throughout the day.
preschooler - night terrors
Due to the active imagination of a preschooler nightmares and night terrors may begin during this time
preschooler aged anticipatory guidance for parents
structure, appropriate limit setting, and consistency are the keys for effective discipline during this time, time out is an effective strategy
Masturbation may occur as the preschooler discovers his or her body. If not excessive, it is considered a normal stage
Help teach how to dress themselves
Provide swimming lessons, BUT this does NOT reduce need for supervision
preschooler aged developmental stages - Erikson
Initiative vs. Guilt
Preschoolers enjoy: Exploring, Imagining, Trying new activities
They like to: Help, make choices, Be independent
Positive encouragement develops initiative.
Excessive criticism may cause guilt
preschooler aged developmental stages - Piaget’s
Preoperational Stage
Thinking is: Egocentric (sees world from own perspective) Magical/fantasy-based
Limited understanding of cause and effect
Uses symbols and imagination in play
Improved language and memory skills
preschooler aged developmental stages - Freud’s
Phallic Stage
Increased awareness of body differences
May become curious about genitals
Identification with same-sex parent develops
preschooler aged developmental stages - Kohlberg
Preconventional Level
Behavior guided by:
Rewards
Punishment
Understands “good” and “bad” based on consequences
preschool physical development
Motor Skill Development | ||
Age 3 years | Gross Motor | Fine Motor |
Climbs well | Undresses self | |
Pedals tricycle | Copies circle | |
| Climbs stairs with alternate feet | Builds a tower of nine blocks |
| Bends over with falling | Screws/unscrews lids, nuts, bolts |
5 years | Stands on one foot ≥10 sec | Dresses/undresses self |
Swings and climbs well | Prints some letters | |
May skip | Feeds self well with utensils | |
preschool language development
Vocabulary rapidly increases
Speaks in full sentences
Asks many “why” questions
Can tell simple stories
The vocabulary of a preschooler increases to about 2100 words and the child speaks in full sentences with appropriate use of tense and prepositions.
school ages motor skills
Fine motor: hand usage improves, eye-hand coordination and balance improve, can write, print words, sew, or build models. Takes pride in activities requiring dexterity and fine motor skills, such as playing musical instruments.
With the development of gross motor skills and involvement in sports at school and in the community, safety education practices are required. Also, with participation in cooperative sports, injuries occur.
school aged anticipatory guidance
Nurses should inform child about expected changes in their body to promote self esteem and confidence
Children learn the natural and logical consequences of discipline.
Parents should teach children rules established by the family, values, and social rules of conduct.
Discipline should be consistent, applied fairly, and focus on the development of the child.
Positive acknowledgement of positive behaviors is more likely to encourage those positive behaviors and promote development.
12 hours of sleep is required
adolescent anticipatory guidance
Sports and physical fitness
Learning and participation in school activities
Safety issues
Proper nutrition and healthy eating habits
Healthy sleep hygiene and adequate rest
Personal care
Healthy sexual life
Appropriate discipline
Mental health resources
Discuss alcohol, tobacco, drugs, peer pressure
Discuss driving
Choose words carefully so that message and intent are clear
Clearly express expectations and set limits
adolescents - Erikson
psychosocial: stages: identity vs. role confusion or diffusion → characteristics: focus is on body changes; importance of peer culture becomes primary.
child life specialist roles
To minimize stress experienced by the children and families, pediatric nurses, child life specialists CLS’s), and other health care professionals recommend the use of atraumatic care.
CLS’s are specially trained individuals that are a part of the multidisciplinary team and works with health care providers and parent to create an atmosphere that promotes child’s wellbeing.
The goals of the CLS is to decrease the child’s anxiety and fear while improving and encouraging the child’s understanding and cooperation.
communication techniques
Basics of communicating with children
Introduce yourself to child and explain your role
Position yourself at the child’s level. Never just tower over them (this is intimidating)
Smile and make eye contact if culturally appropriate
Direct questions and explanations to the child
Observe for nonverbal cues
Allow the child to remain with the parents
oral care of children
teach children & adolescents appropriate tooth brushing & flossing techniques
Encourage use of fluoride-containing toothpastes
Encourage routine dental visits
Optimal oral health is not limited to the prevention & tx of dental caries
It includes anticipatory guidance about nonnutritive sucking habits, injury prevention, oral cancer prevention, & tongue & lip piercing
risk assessment screening types
risk assessment is performed by the physician or provider which includes subjective and objective data to see the likely hood of the child
universal screening → an entire population is screened.
selective screening is done when a risk assessment identifies risk factors.
lead poisoning is a problem that affects children mostly younger than 6 years of age the most due to their play habits. They crawl on the ground and put things in their mouth.
screening tests are procedures or laboratory analysis used to identify children with a certain condition (have high false positive, need follow up)
characteristics of immunity
active → acquired when a person’s own immune system generates the immune response. It last for many years or a lifetime
passive → when immunoglobulins of one person are transferred to another (breast feeding, placenta) only last weeks or months
obtaining immunization history
When obtaining an immunization history from the parent, ask, “when and where did your child receive his (or her) last immunization?” The answer will provide more information than simply asking, “Are your child’s immunizations up to date?” The nurse can compare this information with that on the immunization record, discover in what settings the child is getting health care, and use the information as a starting point in a discussion of any reactions to previous immunizations.
blood lead
Lead poisoning is a problem that affects children mostly younger than 6 years of age the most due to their play habits. They crawl on the ground and put things in their mouths.
Elevated blood lead levels (5 μg/dL or higher) remain a preventable environmental health threat
Symptoms: headaches, stomach pain, inattentiveness, irritability, hyperactivity, decreased bone & muscle growth, poor muscle coordination, problems with language and speech, cognitive impairments, hearing problems, & seizures
pediatric assessment - health history
The health history in children includes more than just the chief complaint, history of present illness, and past medical history, it is important to include the perinatal history and developmental milestones
Safety measures are included in the functional history section of the health history.
The parents’ employment status and occupation are important as they may affect the parents’ ability to spend time with the child, as well as determine financial status.
The functional history should include nutrition, physical activity, screen habits, sleep behavior, elimination patters, relationships, adaptive devices and sexual practices
Perform a 3 generation family health history. Asking about the age and health status of the mother, father, siblings, and other family members helps to identify trends and specific health issues that can indicate the need for additional health screening
pediatric assessments - reviewed of systems
inventory of the body systems that is obtained through a series of questions in order to identify signs and/or symptoms which the patient may be experiencing.
Constitutional symptoms (i.e. fever, weight loss, vital signs)
pediatric assessment - physical assessment
The sequence of the physical examination in children should be based on the child’s developmental age, level of cooperation, and severity of illness, obtain heart rate and respiratory while an infant or young child is quiet, perform intrusive procedures such as examination of ears, mouth, and throat last in the infant or young child
The nurse should inspect the infant’s throat during a yawn or cry.
Do exam for school age or adolescent head to toe reserving genitalia and anus for last
The assessment of pain in children is considered to be the “fifth vital sign.” use age appropriate measurement tools to assess pain in children
The FLACC pain scale should be used to measure pain in children who are too young to verbally or conceptually quantify their pain, or when there is a language barrier.
pediatric assessment - temp.
Temperature can be tympanic, temporal, oral, axillary, and rectal and for children should be taken in the least invasive method that is accepted by the child, parent, physician, or nurse practitioner. Tympanic can be used in children over 3 but is highly dependent on the user’s technique. Temporal (forehead) can be used for any child over 90 days old except for a child who is ill with a fever
Rectal temperature measurement should be avoided in the neonate and the immunosuppressed child.
Oral for cooperative children over 5 keeping in mind oral intake, oxygen, and nebulized meds may affect it, axillary can be used for children who are uncooperative, neurologically impaired, immunosuppressed, or have injuries or surgery to the oral cavity
Rectal is usually unnecessary but keep in mind to insert no more than 1 inch (2.5cm)
pediatric assessment - vital signs
Heart rate:
infant 80-150
toddler 70-120
preschooler 65-110
school-age 60-100
adolescent 55-95
Respiratory rate:
infant 22-55
toddler 20-30
preschooler 20-25
school-age 14-22
adolescent 12-18
BP: children 3 and up
pediatric assessment - fontanelle
In the infant, always palpate the anterior fontanel to determine size, shape, and whether flat or distended.
Fontanels should be soft and flat, report a bulging fontanel immediately, depressed fontanel can be a sign of dehydration, bulging can be increased intracranial pressure. large fontanels can indicate down syndrome or congenital hypothyroidism, a fontanel that gets larger over time can indicate the development of hydrocephalus especially if they also have an acceleration in head circumference growth. Palpate the skull for asymmetry, overriding or open sutures or deformities. Palpate the jaw joints and palpate lymph nodes looking for size, mobility and consistency
common hospital admissions
Diseases of the respiratory system, such as asthma and pneumonia accounts for the majority of hospitalizations in children under 5.
Older children: respiratory diseases, mental health problems, injuries, & gastrointestinal disorders
Adolescents: Problems related to pregnancy, childbearing, mental health, & injury
reactions to hospitalizations
Hospitalization creates a series of traumatic and stressful events in a climate of uncertainty
Children can experience separation anxiety which is distress related to removal from family and familiar surroundings.
Children have different ways to cope:
magical thinking is a type of thinking in preschool-age children that allows for fantasies and creativity to be part of their cognitive abilities
regression is a defense mechanism used by children to deal with conflict by returning to a previous stage that may be more comfortable for them.
invasive procedures such as a venipuncture should never be performed in the crib, bed, or playroom.
strategies to reduce fear in common hospital situations
EX. Darkness, such as going to MRI or radiology or at night – keep light in the exam room, use a night light in child’s room, allow child to hole care giver’s hand or toy if possible.
Teaching guidelines
read stories to prep kids
talk about going to hospital and what it will be like
be honest and encourage feedback
visit and tour hospital
bring special items from home
include sibling in prep
use of restraints
The nurse should use a clove hitch type of knot to secure restraints with ties to allow quick, easy access and release of the restraint.
Emphasize the restraints are to maintain the child’s safety and that it is not a punishment
rules of a school nurse
Nurses develop health plans for children in the school setting called Individual health plans. They plan support for the child with complex health needs, such as asthmatics, serious allergies, diabetes, physical disabilities, ADD/ADHD, seizure disorders.
caring for a special needs child
The Maternal Child Health Bureau defines children with special health care needs as “those who have or are at risk for a chronic physical, developmental, behavioral, or emotional condition and who also require health and related services…”
Many parents experience grief as a result of losing the perfect child of which they dreamed.
Vulnerable child syndrome refers to a clinical state in which parental reactions to a serious illness or event in the child’s past continue to have long-term psychologically harmful effect on the child and parents for many years.
When familied become exhausted become with home care of their child with special needs, respite care resources may be able to provide relief.
Horseback riding for the child who is handicapped is also called hippotherapy
palliative and hospice care
When a child is receiving palliative care, the focus is on symptom relief rather than curative care.
Nurse management of the dying child.
Focus on the family as a unit of care
communication with families during death of a child
Be attuned to the entire family's needs and emotions in order to foster a holistic connection with the child & family
Listen to the child & family; be still & silent for a time to accomplish this. Foster respect for the whole child by attending to him or her as such.
Acknowledge that parents have diverse needs for information & participation in decision making. Allow & encourage family customs or rituals in relation to death and dying.
Each child & family is individual; discuss their particular fears & anxieties in order to determine the child's & family's needs for education & support
Organ donation
A child that dies unexpectedly is a candidate for organ donation.
Organ donation should be a separate conversation than discussing the impending death.
All expenses are paid by the receiving family. The child will still be able to have an open casket if desired. The family’s culture and values will be honored.
infant
Birth to 12 months
play → solitary
gross motor → cephalocaudal
fine motor → proximodistal
milestone → movement; roll, sit, stand
cognitive → trust vs. mistrust
language → 1-2 words
common concept → object permanence
discipline → none
HR → 80-150
RR → 22-55
toddler
1–3 years
play → parallel
gross motor → walking
fine motor → using a spoon
milestone → potty training
cognitive → object permanence
language → 10-50 words, telegraphic speech
common concept → separation/stranger anxiety continues
discipline → timeout
HR → 70-120
RR → 20-30
preschooler
3–5 years
play → co-operative
gross motor → climbing/skipping
fine motor → write letters
milestone → care for themselves
cognitive → kind/generous
language → 200 - 2000 words
common concept → magical thinking
discipline → time out
HR → 60-110
RR → 20-25
school aged
6 - 12 years
play → co-operative
gross motor → riding a bike well
fine motor → writing sentences
milestone → reading/telling time
cognitive → concrete operational
language → reading efficiently, complex words
common concept → loosing teeth, doubles weight
discipline → time out. grounding, taking away privileges
HR → 60-100
RR → 14-26
teen
13 - 18 years
play → team/grown
gross motor → adult-like, riding motor bikes, running races
fine motor → writing paragraphs, papers
milestone → driving
cognitive →formal operational
language → adult language slang
common concept → “it won’t happen to me”
discipline → take away privileges
HR → 55 - 95
RR → 12 - 20
psychosocial development - preschool aged (3-5)
Erikson’s Initiative vs. Guilt
They:
love exploring and learning
feel proud when successful
develop confidence when encouraged
may feel guilty if criticized or unable to succeed
Goal:
Help preschoolers build confidence and independence through encouragement and praise.
cognitive development - preschoolers
Preschoolers are in Piaget’s:
Preoperational Stage
They:
think imaginatively
are egocentric
enjoy pretend play
use magical thinking
may have imaginary friends
do not think logically yet
may not understand death is permanent
moral and spiritual development - preschoolers
the develop
conscience (inner voice, feeling bad after doing something wrong)
understanding of right vs. wrong
morals
spirituality/faith
during ages about 3–6 years.
Kohlberg’s theory:
preconventional morals → preschooler decides good or abd based on punishment, rewards, adult approval. children obey adults because they have authority
infant - trust vs. mistrust
“Can I trust the world?”
toddler - autonomy vs. shame/doubt
“Can I do things myself?”
pre-school - initiative vs. guilt
“Is it okay to try new things?”
school age - industry vs. inferiority
“Can I succeed?”
adolescent - Identity vs. Role Confusion
“Who am I?”
trying to figure out
beliefs
values
career goals
relationships
future identity
DTap vaccine
1st dose at 2 months
2nd dose at 4 months
3rd dose at 6 months
4th dose at 15 - 18 months
5th dose at 4 - 6 years
recommended ages for catch up immunization → 9 months, 12 months, 19 - 23 months, 2 - 3 years
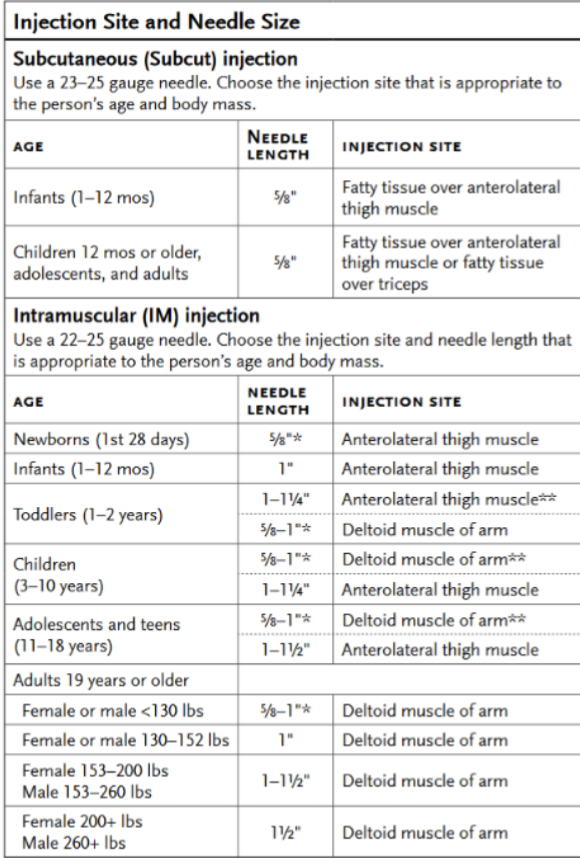
dose → 0.5 mL
route → IM
injections sites and needle sizes