3: factors affecting visual acuity .
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
25 Terms
what does VA measure
assesses how well an eye or an individual sees
va taken for distance viewing in every eye exam
factors that affect VA are divided into external and internal factors
external: relate to our equipment and methdology
internal: to the px, eye the optical system of px eye or retina, cognitive ability, cooperation
external factors affecting va
includes chart type, scoring method and chart luminance
full control over external factors eg we can choose what chart to use and how bright it is
internal factors affecting VA
pathology, pupil diameter , cooperation
we have less control over internal factors but still have some control, eg we can take steps to increase the chances of getting a child to co-operate with VA testing
some internal and external factors interact eg pupil dimater and chart luminance interact to determine how much light falls on the retina
more external factors
chart type
scoring methof
chart luminance
chart contrast
termination rule
general lighting conditions
our approach to taking VA eg wat we do to encourage the px avoiding cherry picking
more internal factors
retinal eccentricity- part of retina used to view letters
pupil diamter
refractive error
pathology
age
px cooperation
can change external factors in certain px to increase chances of getting better measurement
eg if texting a toddler, will change the chart to something more age appropriate
eg if px has high refractive error, we increase the letter size
accuracy
reflects how close a measurement is to the true value
precision
reflects how reproducible measurements are even if they are far from the accepted value
repeatability
variation that occurs when repeated measusremnts are made of the same itwm under absolutlely identical conditions
when you measure VA of the same px re and le on separate occasions, in the same room using the same techniwue, lighting and equipmet
gap must be short enough that there has been no actual change to the px VA
so an individuals optometrists VA measures should be repeatabe
same lighting, same practitioner, same room ect
reproductibility
variation that results when diffeent conditions are used to make the measurements, eg diffeent operators, different et ups and measurement systems
when another optometrist or severral take VA measurements in the same px but different room, different charts , the measures should be similar, ideally identical to our measurres
if they are identical or very siimilar then VA measures are reproducible
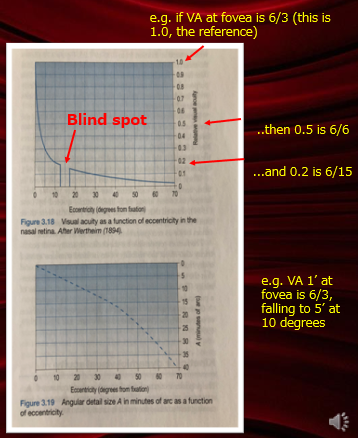
internal: retinal eccentricity
VA is best when the image falls on the centre of the fovea
the fall in VA with eccentricity depends on where image falls on other than centre
its steep if plotted at a ratio, less steep if plotted in MAR
we turn our eyes to recieve the image on the foveal when we eant to see small details
some eyes have poor acuity due to eccentric fixation
some eyes have a damaged fovea and so have to use a non foveal retinal location for fixation
in most px we dont have to worry about whether they are fixating with their fovea as they do this naturally
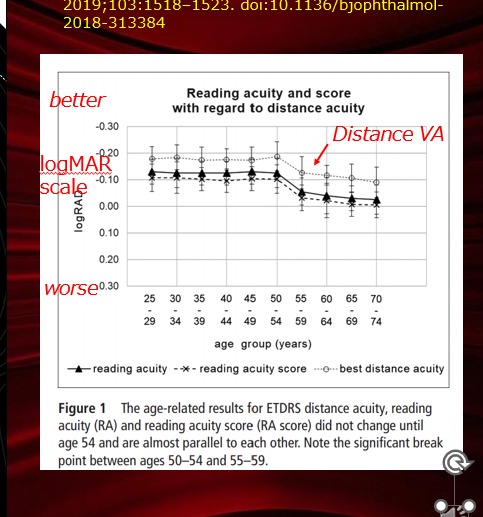
internal: old age
in adults va is constant up to the age of 50
on average VA is considerably better than 6/6 in young adults
VA doesnt approach 6/6 until around the age of 65
after 65 the decline is more rapid
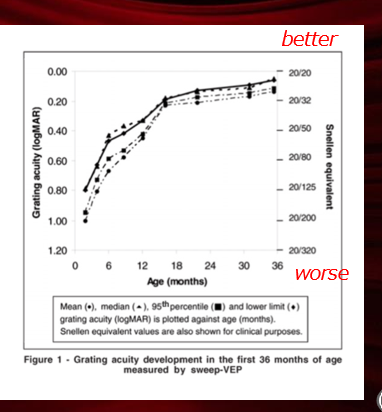
internal: young age
VA in early life is not good eg 6/24 in 6 month old
hard to measure VA in very young and young children
combbination of acuitty that is still developing and an inability to co operate with VA measurement makes VA measures imprecise and innacurate
by age 3 va approaches 6/6
internal; refractive error
uncorrected myopia reduces distance va
uncorrected hyperopia may or may not reduce distance va
uncorrected astigmatism always reducses distance VA
internal: pupil size
the pupil controls the amount of light entering the eye
it dilates in low light and constricts in bright light
when we read the eyes converge and accomodate and the pupil constricts
older px generally have smaller pupils
pupil size interaction with refractive error
egif theres -5.00 DS of myopia the VA is worse than 6/96 when te pupil diameter is 7mm, but VA i much better if the pupil size is 0.5mm
diffraction and aberrations - interaction with pupil size
these are imperfections of an optical system which mean that the image of a point object is not itself a point
diffraction: deviation in the direction of propgation of a beam of light which occurs when the light passes the edge of an obstacle such as the pupil of the eye. only an issue when pupil is small
aberrations: optical defect in whcih rays from a point object do not form a perfect point passing through an optical system . proble when pupil large
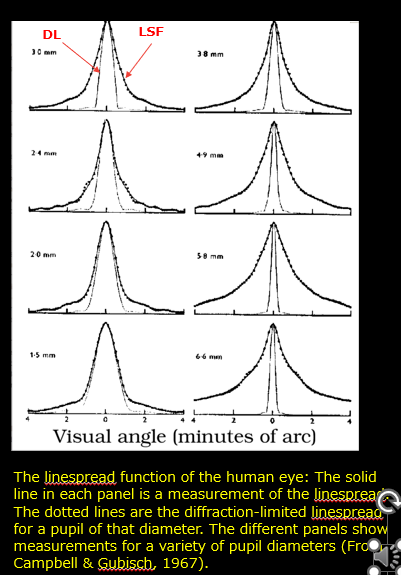
impact on VA of pupil size
line spread function LSF is the image of a thin line formed by an optical system
the system has better optical quality when the LSF is thin , so VA will be better
lsf is thinnest when pupil sizes between 3.4 and 3.8]
if theres a gap between the LSF and diffractionlimit curve this is due to aberraions
when pupil small LSF wide due to diffraction
internal: pathology
many diseases of the beye and visual sstem cause reduced VA
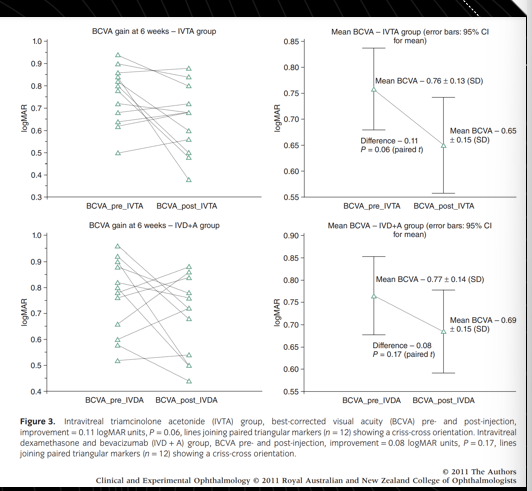
figure shows results from a study about the treatment of diabetic eye disease
each triangle in the 2 panels on the L represents a single eye
the 2 panels on the R show average pre and post treatment VA
va redced in the pre treatment group
internal: px co operation and other cogntive
if px cant eg too young or wont co operate with VA testing it impacts
have to rely on objective means for VA
communication issues can also arise eg px cant speak or dont speak same language
eg by using the umbling e chart rathe than letter chart where the px indicates with their fingers whether the bars of the es are facing up down left or right
external factors: our approach to VA testing
eg dont say what can u read, ask can you read the top line, instruct pc where you want them to start
as they reach their limit point to letters you want them to attempt
no cherry picking
give lots of encouragement
need to reach termination
termination rule
let px stop reading when they want - will intorduce variablility based on how confident the px is
ask every px to attempt every letter on the chart - hugely time efficient anf dispiriting for many px
most common termination rule is stopping when they get 4/5 letters wrong
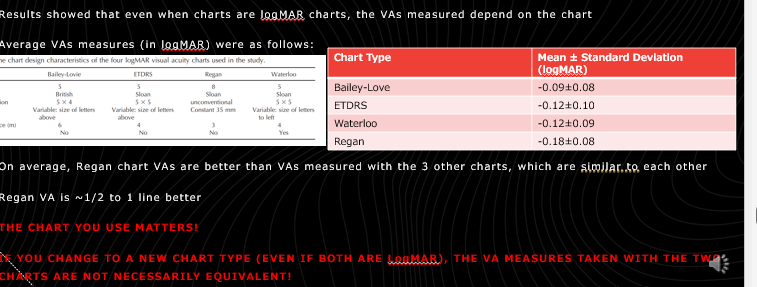
external factors: chart type
crowing: P H N H D or PHNHD
different chart types used to asses VA
on average Regan chart VAs were better than VAs measured with the 3 other charts
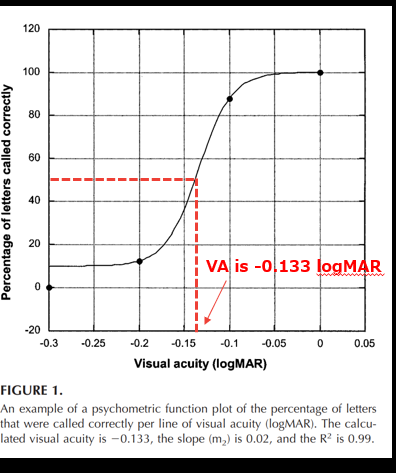
external: scoring method
could score by line eg 6/5 or using per letter scoring system eg VAR
eg
on 0.0 line all letters identified so cooridinates as (0,100)
on 0.3 line, no letters correct so coordinates (-0,3.0)
determine % correct for lines between -0.2 and -0.1
can work out va from this curve
determine logMARA letter size corresponding to 50% correct
external factors : chart luminance and general lighting condtions
retina l luminanceby the pupil size and chart luminance
retinal luminance is measured in trolands where 1 troland is the retinal illuminance for a pupil area of 1mm² viewing a surface that as a luminance of 1 candela per square metra
to ensure adequate retinal illuminance we must ensure chart luminance is high enough
for luminance the permissible range is 80 to 320 cd/m²
internally illuminated charts should have a luminance of not less than 120 cd/m²
to avoid glare the test chart surroundings should be illuminated to a smiliar level
external; chart contrast
like poor luminance, VA is affected by poor contrast
if L1 denotes the luminance of the white background and L2 the luminance of the black letters , the luminance contrast is given by:
( L1- L2 / L1)
VA may be resistance to reduction in contrast to 20% but does not apply to px with opacities of the ocular media