N3TT3 - It's Not Okay
1/291
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
292 Terms
Conflict Prevention & Management - CNO
Conflict
- A power struggle in which a person intends to harass, neutralize, injure or eliminate a rival
- Conflict that is managed effectively by nurses can lead to personal and organizational growth
- If conflict is not managed effectively, it can hinder a nurse's ability to provide quality client care and escalate into violence and abuse
- Conflict among colleagues can lead to antagonistic and passive-aggressive behaviours (such as bullying or horizontal violence) that compromise the therapeutic nurse-client relationship
Factors for Escalation of Conflict from a Patient
The nurse:
- Judges, labels or misunderstands a clients
- Uses a threatening tone of voice or body language (ex. speaks loudly or stands too close)
- Has expectations based on incorrect perceptions of cultural or other differences
- Does not listen to, understand or respect a client's values, opinions, needs and ethnocultural beliefs
- Does not listen to the concerns of the family and significant others, and/or act on those concerns when it is appropriate and consistent with the client's wishes
- Does not provide sufficient health information to satisfy the client or the client's family
- Does not reflect on the impact of her/his behaviour and values on the client
Client Centered Care Strategies
- Continually seek to understand the client's health care needs and perspectives
- Acknowledge the feelings behind the client's behaviour
- Ask open-ended questions to establish the underlying meaning of the client's behaviour
- Engage in active listening (ex. use verbal and nonverbal cues to acknowledge what is being said)
- Use open body language to display a calm, respectful and attentive attitude
- Acknowledge the client's concerns about the health care system and his/her experiences as a client
- Respect and address the client's wishes, concerns, values, priorities and point of view
- Anticipate conflict in situations in which it has previously existed and create a plan of care to prevent its escalation
- Reflect to understand how her/his behaviour and values may negatively affect the client
Conflict Management Strategies
- Implement a critical incident management plan
- Remain calm and encourage the client to express his/her concerns
- Avoid arguing, criticizing, defending or judging
- Focus on the client's behaviour rather than the client personally
- Involve the client, the client's family and the health care team members in assisting with the behaviour and developing solutions to prevent or manage it
- State that abusive language and behaviours are unacceptable, if the nurse believes this will not escalate the client's behaviour
- Step away from the client, if necessary (ex. to regain composure or to set personal space boundaries)
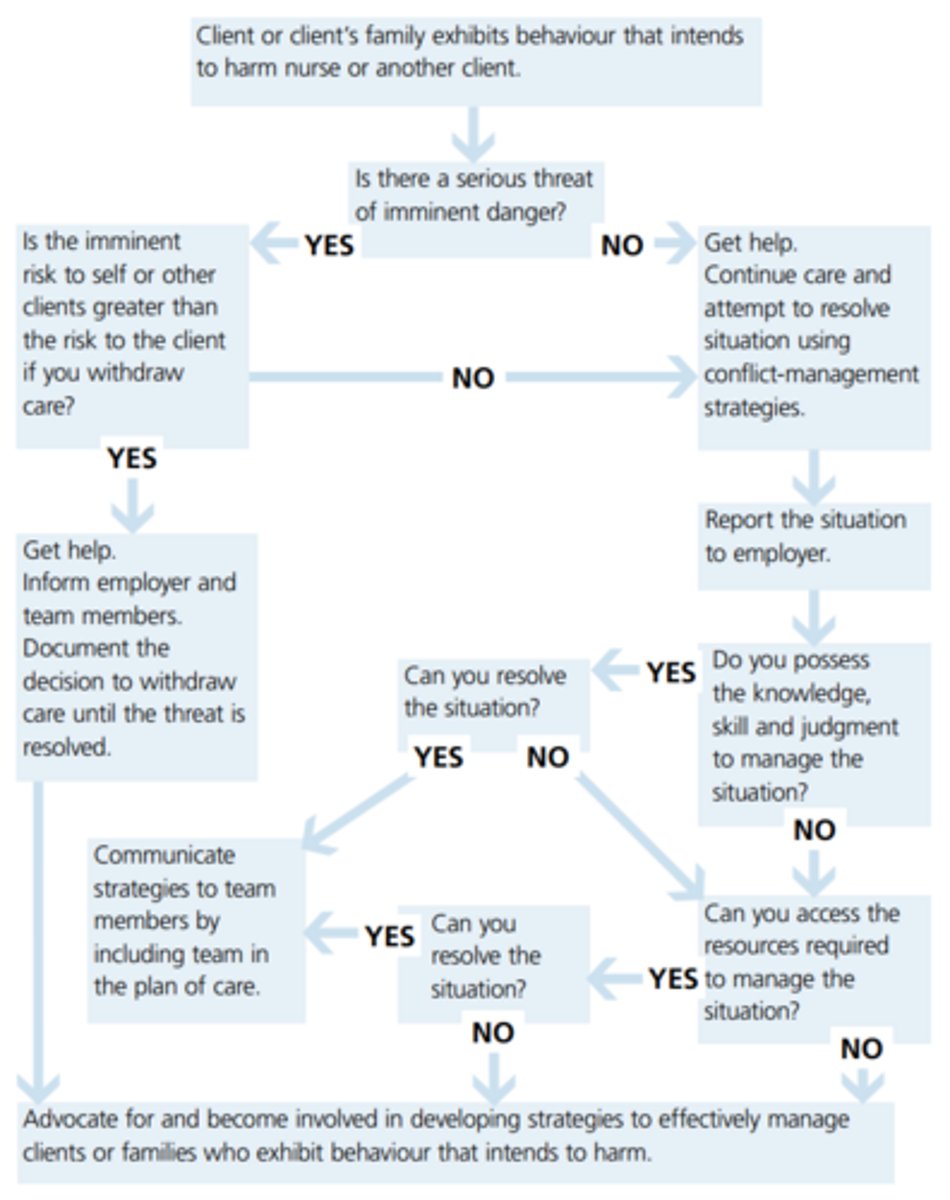
- Leave the situation to develop a plan of care with the assistance of a colleague if the client intends to harm the nurse
- Protect themselves and other clients in abusive situations by withdrawing services
College Conflict Prevention Strategies
- Promote a respectful work environment by modelling professional behaviours
- Mentor, support and integrate new staff members into the practice setting
- Reflect on personal attitudes, motivators, values and beliefs that affect relationships with colleagues, identify personal areas in need of improvement and strive to alter their own behaviour in situations that have previously ended in conflict
- Recognize that personal stress may affect professional relationships and take steps to manage that stress
Positive Collegial Relationships
- Result from good communication, mutual acceptance and understanding, use of persuasion rather than coercion, and a balance of reason and emotion when working with others
- Address conflict directly rather than avoiding or postponing its resolution
- Focus on the behaviours that lead to the conflict rather than on the colleague personally
- Validate assumptions through open dialogue with colleagues rather than acting on misperceptions or assumptions
- Collaborate with colleagues to identify the underlying cause of the conflict
Prevention for Workplace Conflict
- Implement policies that do not tolerate abuse of any kind
- Ensure that policies against workplace conflict are also directed at combating any form of discrimination
- Ensure that managers model professionalism in preventing and managing conflict
- Establish and uphold organizational values, vision and mission that acknowledge the health, safety and well-being of staff
- Educate managers and staff in communication, as well as in conflict prevention and management
- Support effective collaboration and communication among health care team members, especially between nurses and physicians (ex. interprofessional rounds)
- Implement strategies to ease the impact of change and decrease stress among staff
- Identify and address staffing needs as soon as possible, especially at peak times
- Ensure a comfortable and safe physical environment
Management of Workplace Conflict
- Provide a system that promotes the reporting of incidences of workplace conflict, protects nurses from reprisal and deals with reports fairly and efficiently
- Routinely assess the incidence of workplace conflict and implement strategies for corrective action
- Institute clear policies and consequences for those who breach policies aimed at preventing conflict and abuse
Managing Conflict Among Staff Members
- Offer a confidential environment for staff to report episodes of conflict without fear of retribution
- Deal with reports promptly, fairly and confidentially
- Ensure that appropriate follow-up procedures are in place to support nurses who have been abused in the course of their practice
Debriefing After Critical Incident
Nurses can:
- Consult with those involved about the meaning of their experiences during the incident with the intent to heal themselves and the client and family
- Review and reflect on responses and recommend future strategies based on team members' actions
- Reflect on their own behaviour, which may have unintentionally affected the nurse-client relationship
- Help the client understand how his/her behaviour negatively affected the therapeutic nurse-client relationship
- Develop communication strategies with the client so the client can express his/her feelings appropriately
- Use best-practice strategies to develop a care plan for dealing with the client's behaviour
- Use anticipatory planning to develop a consistent approach of addressing the client's behaviour in the future
Abuse
- The misuse of power within a relationship
- Abuse can be emotional, verbal, physical and/or sexual
Anticipatory Planning
- Involving the client in making decisions based on the client's values, beliefs and wishes
Critical Incident
- Any sudden unexpected event that has an emotional impact that can overwhelm the usually effective coping skills of an individual or a group
Horizontal Violence
- Interpersonal conflict among colleagues that includes antagonistic behaviour such as gossiping, criticism, innuendo, scapegoating, undermining, intimidation, passive aggression, withholding information, insubordination, bullying, and verbal and physical aggression
Decision Tree: Withdrawal of Services
Introduction to Motivational Interviewing: An Introduction
Motivation interviewing
- An effective way of talking with people about change
- It is evidenced based
- Require because often change is hard, and people face many decisions that require some sort of change at every stage of life (ex. marriage, career, drugs, medical decisions, accepting help, etc.)
- Change is hard because it is a motivational issue (wanting to change but can not = ambivalence; often produces anxiety and uncomfort which causes us to continue to procrastinate the decision = often mistaken for resistance)
- Motivational interviewing can help resolve ambivalence and help elicit a person's own motivation to change (in a healthy direction)
Spirit of Motivational Interviewing
- Partnership: Work collaboratively and avoid the "expert" role
- Acceptance: Respecting the clients autonomy, potential, strengths, and perspective
- Compassion: Keep the client's best interests in mind
- Evocation: The best ideas come from the client
Core Skills of Motivational Interviewing (OARS)
- Open questions: Try to ask more open then closed questions to allow client to lead conversation, not interviewer and their own agenda; Ex. How do you feel?
- Affirmations: Ex. You are successful, it took courage to come in today, etc.
- Reflections: Understanding what the client is thinking and feeling and then saying it back to the client
- Summaries: A long reflection of more than one client statements
4 Processes of Motivational interviewing
- Engaging: The process of establishing a trusting and mutually respectful relationship; make the client feel welcome, comfortable, understood, exceeding expectation, mutual goals, and hopeful (ex. attuning, aligning, joining, and connecting with your client) (dis-engaging = assessing you client, telling your client how to fix their problem, power differential, labelling your client)
- Focusing: An ongoing process of seeking and maintaining direction; setting an agenda, setting goals and priorities, clear direction (ex. use OARS skills)
- Evoking: Eliciting a client's own motivation for change (change talk = client speech that favors movement in the direction of change; more they argue for change themselves the more they will want to change)
- Planning: Developing a specific change plan that the client agreed to and is willing to implement (ex. generate SMART goals/plan)
*All in order: start with engaging and then move down
Change Talk Questions
- Why do you want to make a change?
- What are the reasons to change?
- What would some of the benefits be?
- How might you go about making a change?
- What would be your first step?
Palliative Care In Patients with Heart Failure - BMJ
Palliative Care & HF
- The incorporation of palliative care into the management of heart failure has been suboptimal for several reasons: Uncertainty in the disease trajectory, failure to reward communication between healthcare providers and patients, siloed care, lack of knowledge, overlay of comorbidity and frailty, life saving devices with complex trade-offs, and a limited evidence base
HF
- A syndrome of cardiac dysfunction characterized by dyspnea, fatigue, and fluid retention
- Once patients develop chronic symptomatic heart failure, the disease often dominates their overall health and medical care
- Morbidity is high, hospital admission is common, median survival is less than five years, and the disease places great demands on patients, caregivers, and healthcare systems
- Cases are often those >75 yrs; with increasing amount for those >85 yrs
- Most contemporary data from developed nations indicate that the incidence of heart failure has plateaued, or even decreased (patients living longer with symptomatic disease = need for palliative care)
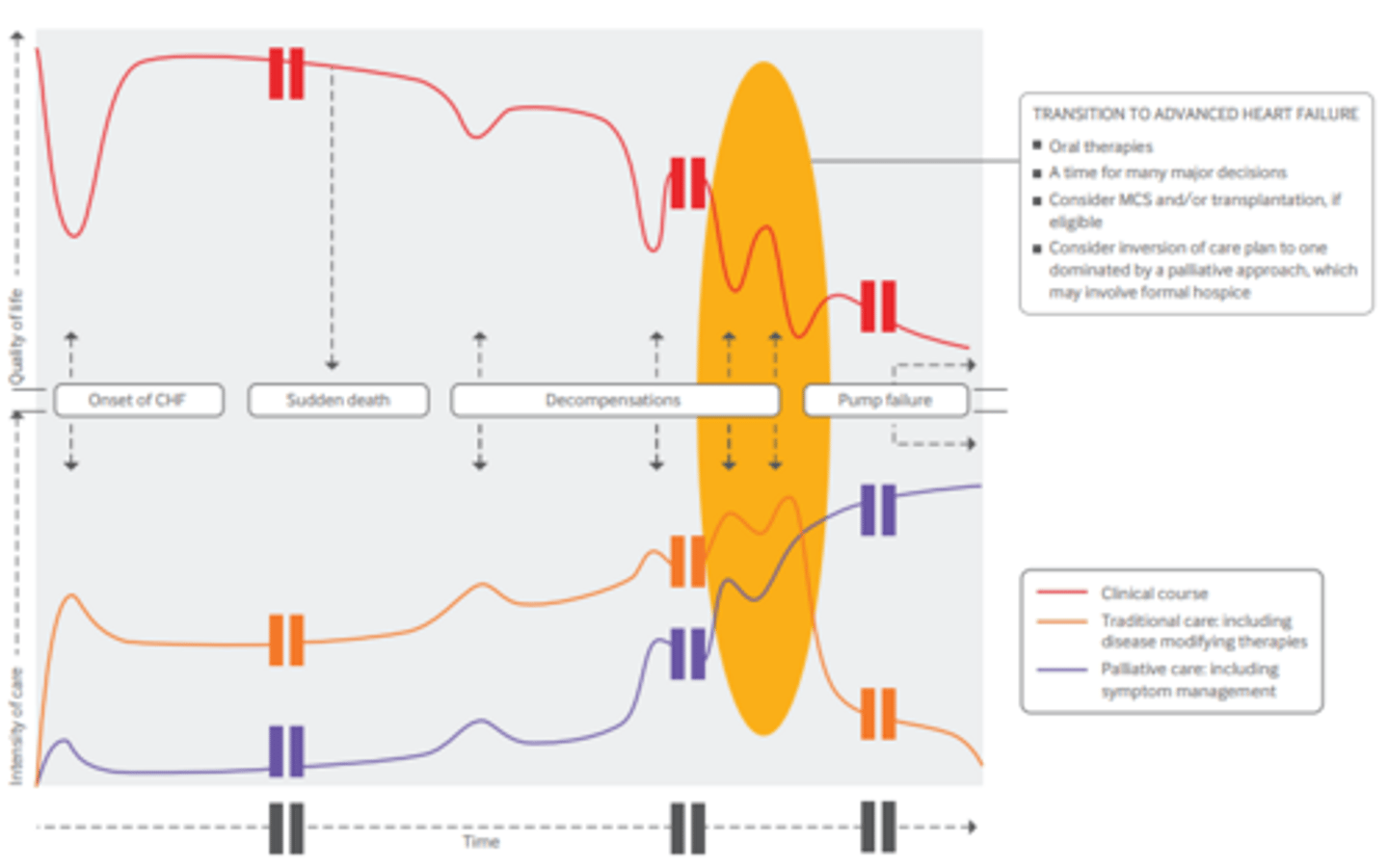
- Although some patients may die suddenly of cardiac arrhythmia, most patients with symptomatic heart failure die of progressive pump failure associated with severe symptoms preceding death
- The most common symptoms of heart failure are pain, breathlessness, fatigue, and depression
- Physical symptom burden was the strongest predictor of health related quality of life
- When heart failure nears end stage, it has one of the largest effects on quality of life of any advanced disease (greater symptom burden and depression)
Palliative Care
- An approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial, and spiritual
- Embodies several principles including relief from pain and other distressing symptoms and the integration of psychological and spiritual aspects of patient care
- It is estimated that only one in every 10 people who needs palliative care currently receives it
- Palliative care has been shown to reduce healthcare spending
Primary Palliative Care
- The basic skills and proficiencies needed by all providers
- Primary care providers and cardiology providers practice primary palliative care to fill the common palliative needs of patients
Secondary Palliative Care
- The specialists and organizations that provide consultation and specialty care
Tertiary Palliative Care
- The academic medical centers where specialist knowledge for the most difficult cases is practiced, researched, and taught
Role of Palliative Care in HF
- The American Heart Association (AHA) developed guiding principles advocating incorporation of palliative care in patients with cardiovascular disease, including providing patients with access to continuous, coordinated, comprehensive, high quality palliative care given simultaneously with specialist care
- Because of the progressive, chronic, but unpredictable disease course of heart failure, palliative care can help meet the needs of patients, families, and healthcare providers
- Increase likelihood of death at home
- Palliative care can provide support systems to patients and their families during this time
- Palliative and supportive care is effective for patients with symptomatic advanced disease to improve quality of life
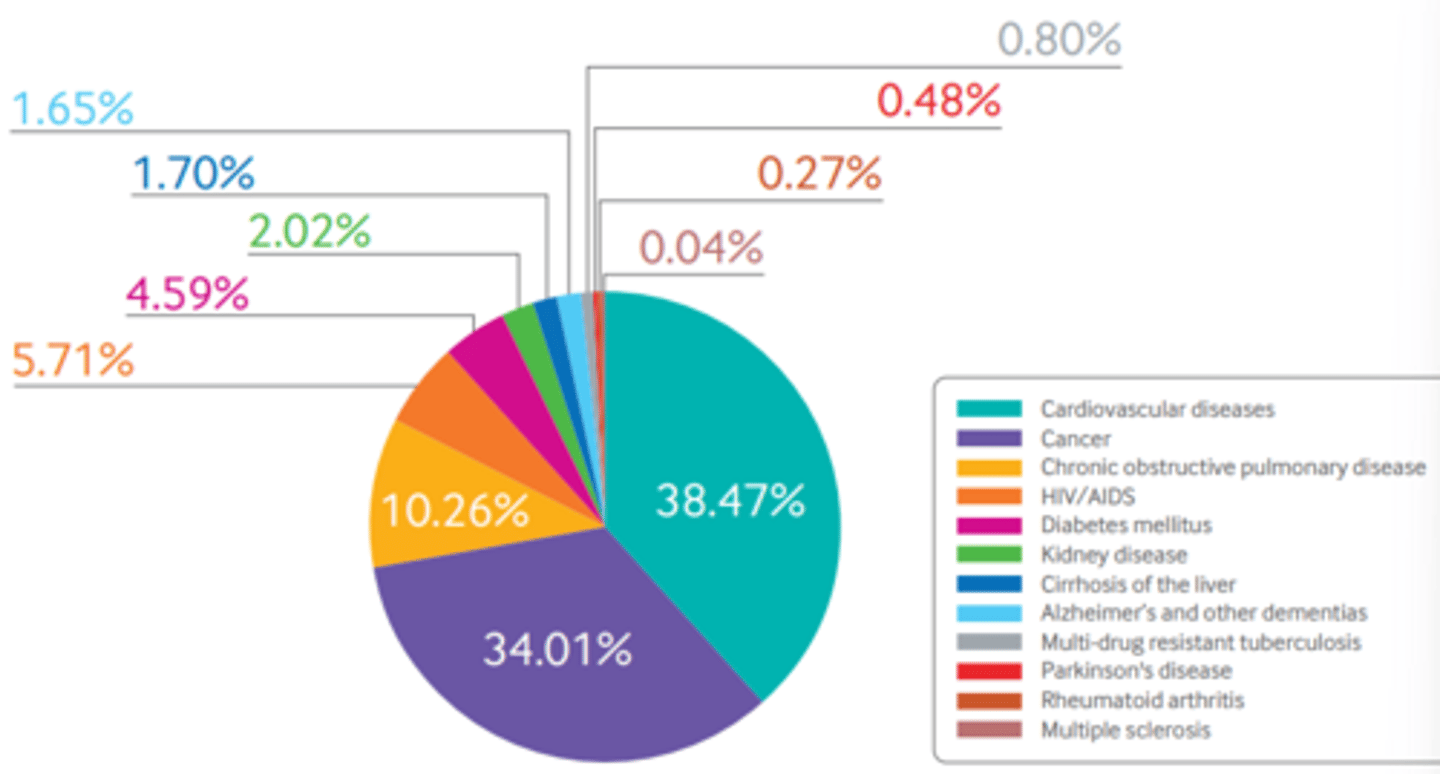
Distribution of Adults in Need of Palliative Care at the End of Life
HF & Multimorbidity
- Heart failure is associated with substantial morbidity and with multiple other comorbidities
- Multimorbidity contributes to the range of symptoms, complicates management, and can alter prognosis
- On average, patients with heart failure have 4.5 comorbidities
HF & Frailty
- Frailty is a biologic syndrome characterized by a decline in overall function and loss of resistance to stressors
- The care needs of patients with heart failure and frailty are often not very amenable to traditional heart failure treatments; palliative care can help with manifestations of frailty by providing a patient centered framework to care grounded in overall values, goals, and preferences
Clinical Course of HF
Palliative Care Interventions for HF
- Opioids are the first line therapy for moderate to severe pain, unless the pain is caused by another condition
- Non-pharmacologic management includes massage, acupuncture, and heat therapy
- Dyspnea refractory to hemodynamic interventions (diuretics, afterload reduction, inotropes) can also be treated with low dose opioids and benzodiazepines
- Non-pharmacologic management includes using a fan to provide cool air to the face, breathing training, and anxiety management
- Selective serotonin reuptake inhibitors are most often used as first line pharmacologic therapy for depression owing to their general effectiveness and limited side effects
- Non-pharmacologic management includes exercise, psychotherapy, and cognitive behavioral therapy
- Sertraline against depression and heart disease showed no significant benefit
- Cognitive behavioral therapy was effective in the treatment of depression in patients with heart failure
Integrating Palliative Care into HF Care
- Acute exacerbation of HF often re resents a temporary reduction in health status but can be a terminal event; at the time of presentation it can be nearly impossible to anticipate the patient's response to therapy and eventual disposition
- s many patients with heart failure overestimate their survival, so it is hard to time and involve palliative care resources
- Effective communication between healthcare providers and patients is essential, especially in chronic diseases, such as heart failure (need early end of life discussions)
- Avoidance of difficult discussions about end of life is probably exacerbated by a lack of training and knowledge in palliative and communication techniques
- Increased education and training must be part of the solution, because integration of palliative care earlier in the disease process requires delivery from a range of providers; the formal palliative care workforce is not large enough to assume all of these responsibilities
- The fact that many providers have false perceptions about palliative care (ex. that it is appropriate only at the end of life or that patients will lose all hope if it is discussed) means that patients are much less likely to be referred to palliative care
- Decision making and patient selection are important components of palliative care, and strategies that provide patients with all medically appropriate options are necessary to help patients navigate these complex decisions
Implanted Cardioverter Defibrillators
- ICDs can prevent death from a lethal arrhythmia but do not improve cardiac function (unless cardiac resynchronization therapy with biventricular pacing is also indicated) and can add to the burden, particularly if the ICD discharges inappropriately
- A discussion should occur with each patient about the risks, benefits, and alternatives of ICD therapy and this discussion should be documented
Left Ventricular Assist Devices
- LVADs are increasingly implanted in carefully selected patients with advanced heart failure who cannot undergo transplantation or for whom a suitable donor organ is not available
- All accredited destination therapy (DT) LVAD programs must have a palliative care specialist as part of the team
- Patients with LVADs are at risk of stroke, bleeding, infection, and other complications that contribute to an average survival after implantation of less than five years
Device Deactivation
- ICDs remain active until, and often during, death; disturbingly, this even happens to patients in hospice
- Deactivating an ICD does not result in almost immediate death as it does with an LVAD
- With DT-LVADs, death will occur with the LVAD in place
- Iterative discussions around device deactivation, starting before implantation, are essential to decrease confusion for providers, patients, and their families
Team Based Palliative Care
- Access to formally trained palliative care providers may be limited; therefore, other members of the patient's care team, including primary care providers and cardiologists, should be familiar with available palliative resources and treatment options
- In the early phase of the disease, a general practitioner or cardiology provider can lead the team with formal palliative care consultation only as needed
- In end stage heart failure or at the time of major medical decisions (such as con‑ sideration of LVAD implantation), trained palliative care providers may take on a more central role in coordinating care
- Effective collaborations involving a heart failure nurse or case manager who liaises between the two teams
- Creating incentives for skills training in palliative care principles, such as offering continuing medical education credits, regardless of specialty, can also help bridge the gap

Advance Care Directives & Preparedness Planning
- For patients, advance care directives provide an avenue to express their wishes about life sustaining treatments, usually to withhold or withdraw, in the event of a terminal condition
- For providers, advance care directives can help when assessing patients' values, goals, and preferences to facilitate concordant treatment decisions
- Moving advance care planning upstream involves preparedness planning
- Preparedness planning has been shown to improve attitudes and increase completion of advance care directives in patients with heart failure
- The concept of preparedness planning is often combined with a palliative care visit as the first step to the ultimate completion of advance care directives
- Primary care provider or cardiologist should initiate these discussions
Shared Decision Making & Decision Support
- Patient satisfaction scores, transitional care measures integrating inpatient and out‑ patient settings, and patient reported outcomes are two patient centered initiatives that are particularly applicable to heart failure
- Shared decision making puts patient centered care into practice (it involves both patients and providers, with the ultimate goal of ensuring that a patient's values, goals, and preferences guide informed decisions)
- The tenets of palliative care are fundamentally patient centric, and the specialty places shared decision making and related patient-provider communication at the forefront of management
- Various forms of decisions aids are available, including pamphlets, videos, interactive web based platforms, and books
- Decision aids are increasingly available but have not been widely adopted because of the difficulty of integrating them into clinical practice
- Decision aids have been developed for some heart failure treatments, including ICDs and LVADs
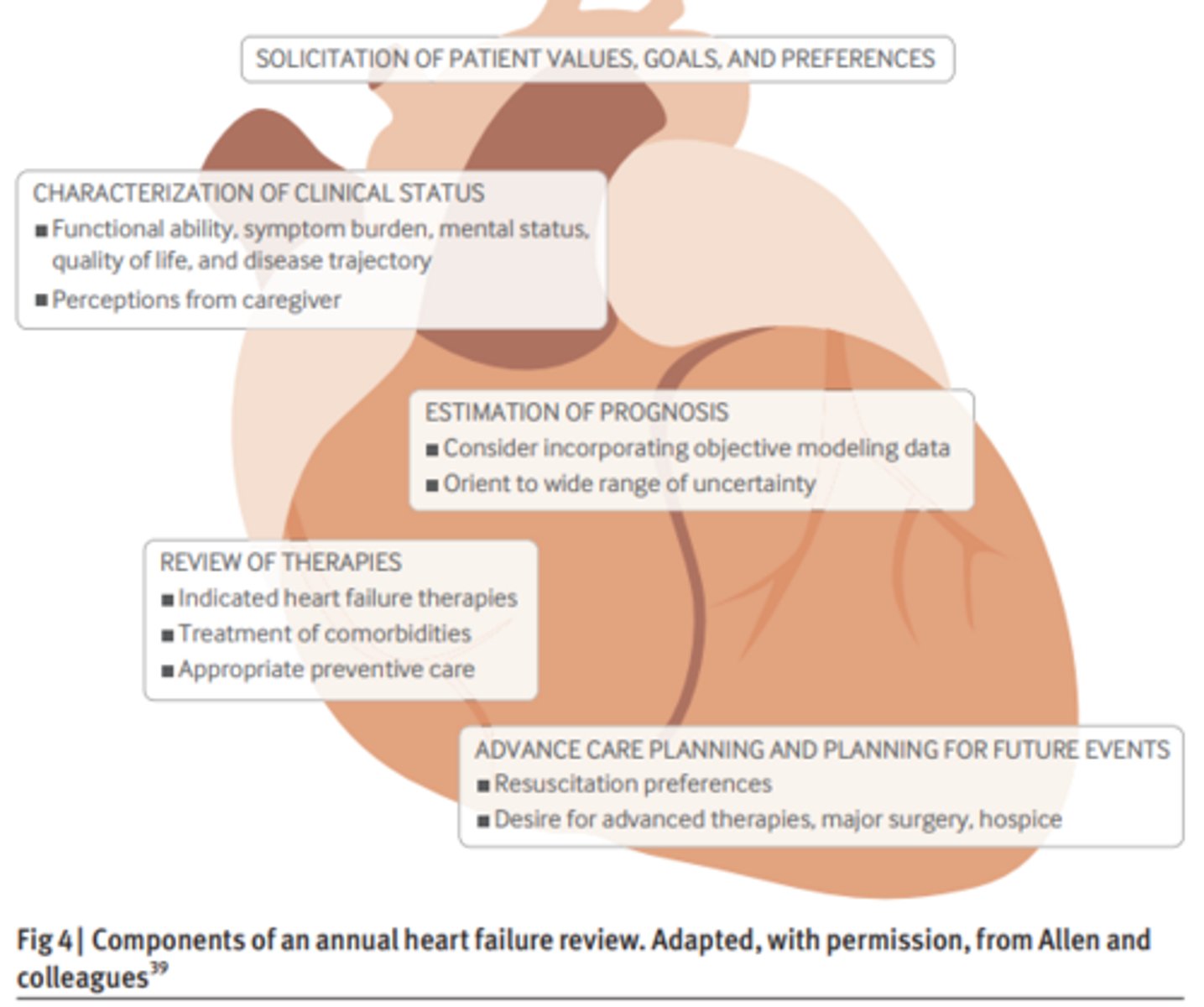
Components of an Annual HF Review
Integration of Palliative Care & HF
Future of Palliative Care & HF
- More frequent, timely, quasi-experimental trials are needed that assess patient centered outcome measures for symptom based and end of life care
- Professional and policy organizations must continue to emphasize and incentivize palliative care, including discussions around end of life (the Affordable Care Act does not explicitly mention palliative care, it does cover some aspects of end of life care = hospice)
- Patients, family members, and healthcare providers must be better informed about palliative care
- The perception of palliative care needs to expand from purely end of life care to care that focuses on symptom burden and stress as a way to improve quality of life throughout disease progression
- If death is consistently viewed as failure rather than an important chapter of life, patients and families are bound to be ill prepared when heart failure becomes unresponsive to therapies
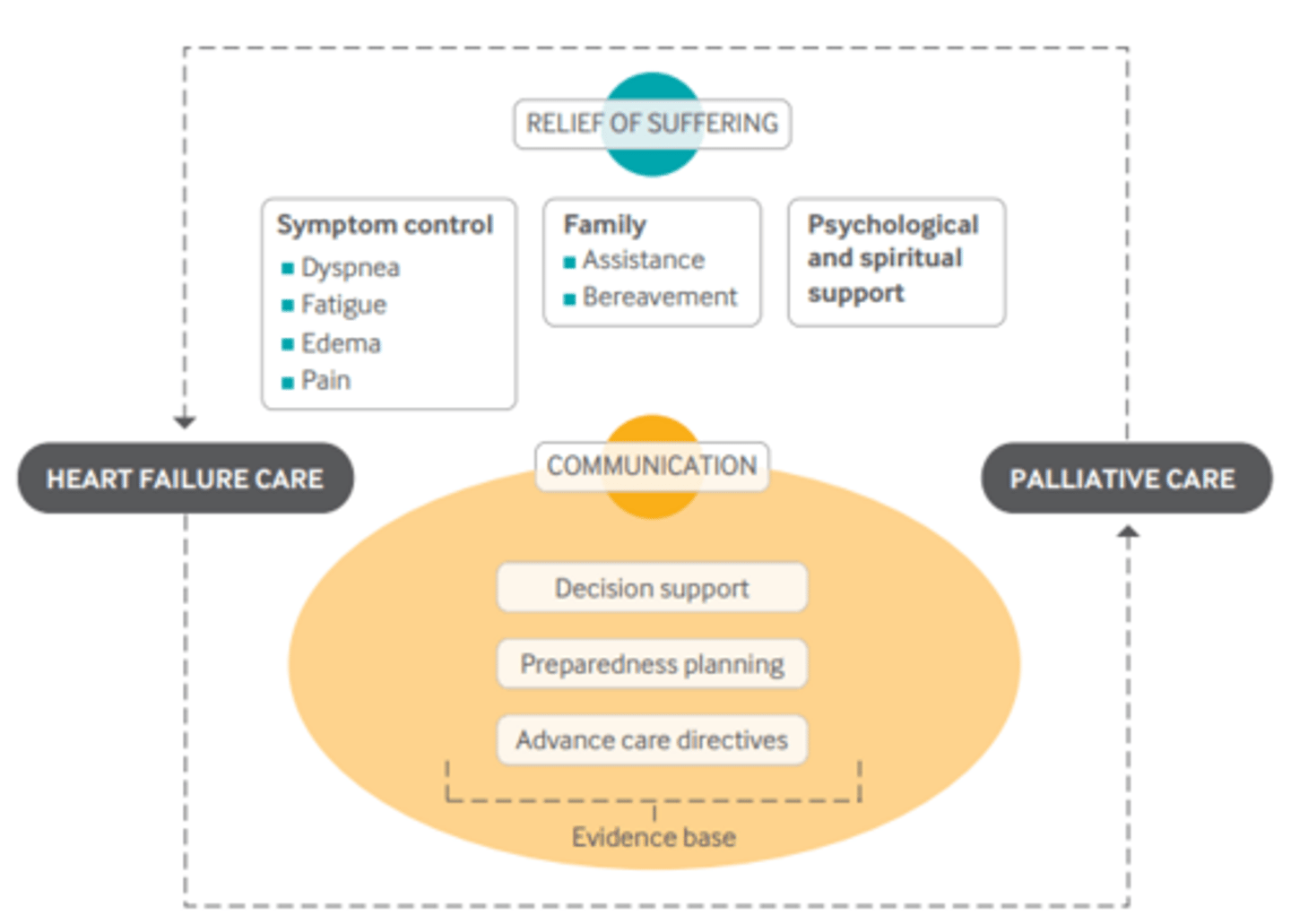
- Palliative care is designed to complement traditional heart failure care through its focus on communication, shared decision making, and advance care planning
- Palliative care strives primarily to reduce suffering through the relief of pain and other distressing symptoms while integrating psychological and spiritual aspects of care
- Palliative care provides a support system to patients loved ones
Respecting Choices Program for Advanced Care Planning & Decision Making
- Patient educational materials are routinely available at local health facilities
- Trained advance care planning facilitators help people with advance care planning when requested
- Practices within the healthcare organizations enable providers to easily obtain, store, and retrieve advance directives when and where they are needed
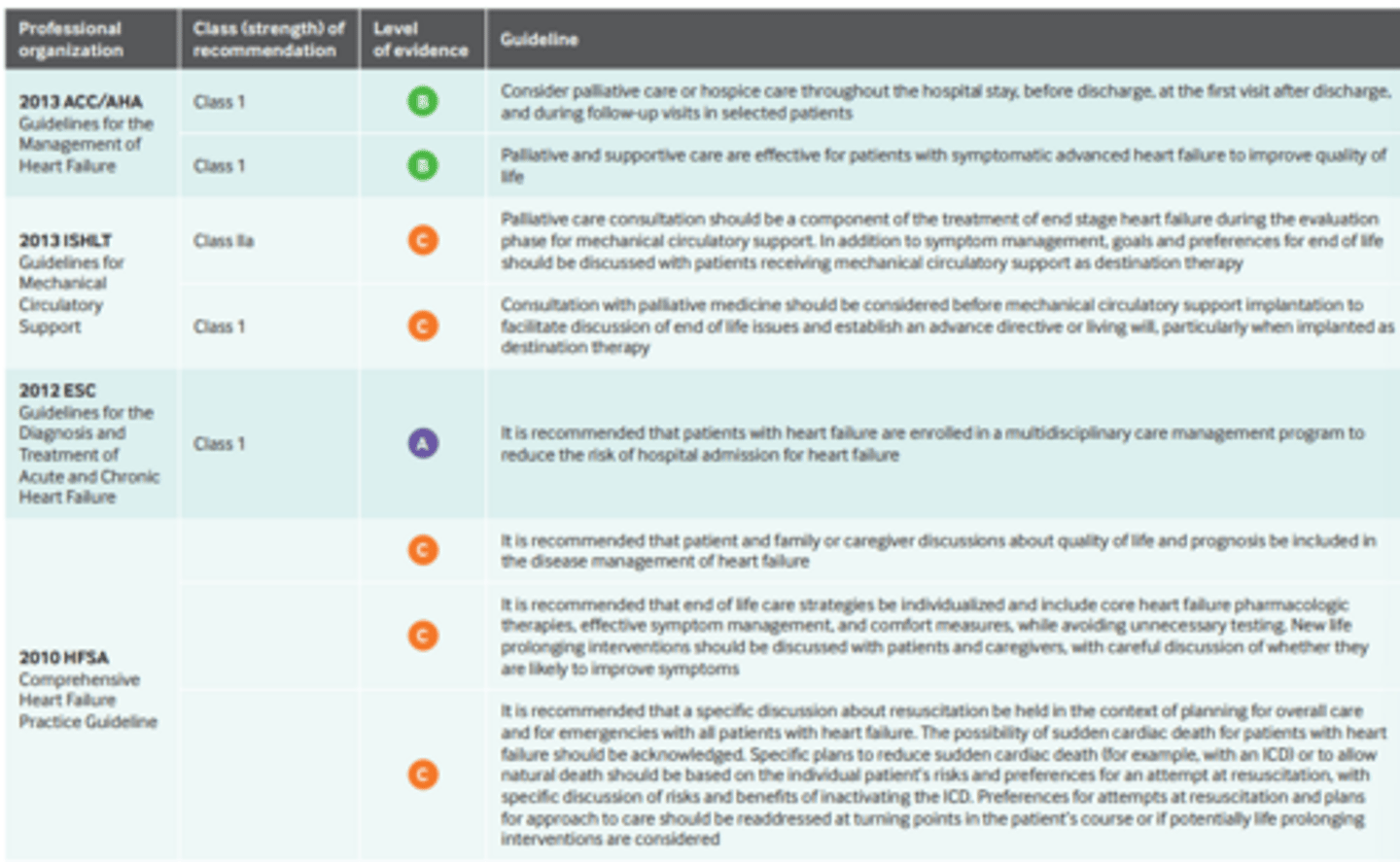
HF Guidelines
Strategies to Support Self-Management in chronic Conditions: Collaboration with Clients - RNAO
Delivering Self-Management Support
- Directly related to studies that have shown interventions involving client self-efficacy, social support, improved coping skills, and certain follow-up plans as having a positive impact on self-management and health outcomes in specific chronic diseases
- This shift to self-management is also in response to the need for a more effective and efficient approach to health care as people are living longer lives with complex, ongoing chronic health conditions that cannot be cured but can be managed appropriately to lessen the impact on overall health, quality of life and health system costs
- Self-management support moves away from the traditional model of clients being given instructions that they should adhere to in order to improve their health outcomes, and places the onus on the client to take a more proactive role in their health
- A self-management approach promotes strengthening the self-efficacy of clients, who through their own abilities derive solutions to the problems they face as a result of their chronic health condition
Nurses & Client Self-Management
- Nurses and other health-care professionals will continue to use their knowledge and expertise to inform, activate and assist clients in their care to achieve successful self-management; in addition, there is considerable responsibility for governments, health-care policymakers, health-care organizations, and communities to provide support and resources for this new approach
Client Self-Management Education
- The focus of self-management education is to teaching clients skills that they can use to self-identify problems related to living with a chronic disease and how to address those problems
- The intent is to provide education that enables the client to understand the disease process, acquire skills related to technical management, as well as learn how to live a complete life with the disease
- A client-centred care approach is essential for successful self-management support (client-centred care involves advocacy, empowerment and respecting the client's autonomy, voice, self-determination and participation in decision-making)
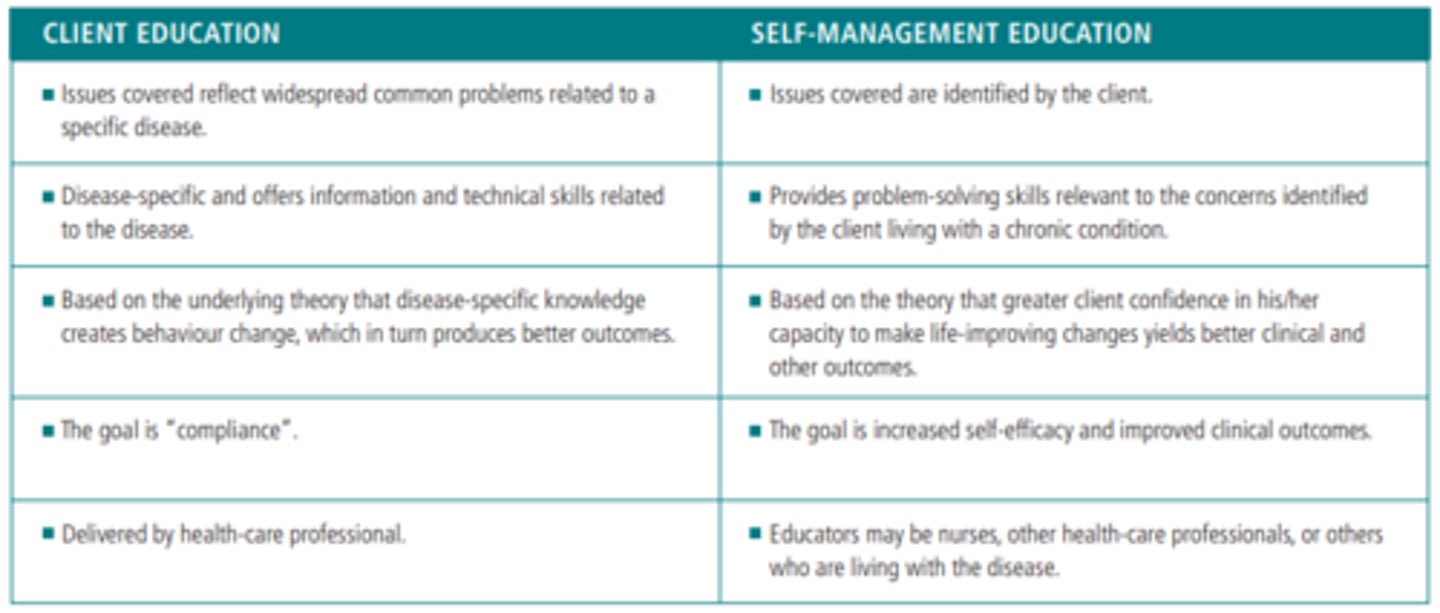
Comparison of Client Education & Self-Management Education
Self-Management Education
- Self-management education has long been considered the essential first step in successfully preparing clients to manage and live with their chronic condition
- Good for short term education
- Traditional client education alone is generally not sufficient for clients to maintain the self-management gains made as a result of education for chronic disease care
- Behavioural strategies are generally considered to be important components of self-management support (self-directed goal-setting, problem-solving, skill-building, action planning, healthy coping, stress management, self-monitoring and providing links to community resources have been effectively used in successful client education programs)
Healthcare Professional Approaches to Providing Self-Management Support
1) By developing and delivering self-management programs
2) By using and providing information to clients about behavioural strategies that enhance their ability to be an effective self-manager. Teaching techniques that assist clients to learn these behavioural strategies include:
- Setting goals, collaboratively, with clients, using templates that can be modified based on the clients context
- Stting goals, collaboratively, with clients, using templates that can be modified based on the client's context
- Assessing clients' readiness for self-management, based on tools that the client can use in the future
- Helping clients to break down goals and tasks into small steps as part of an action plan, using specific tools and templates that can be modified based on the client's context
- Providing personalized feedback and helping the client learn how to ask for, and receive and use feedback
- Teaching self-monitoring, using tools and templates; helping clients obtain social support
- Informing clients of and linking them to community resources
- Helping clients assess their ' commitment to key tasks; and building in follow up processes to help clients measure their progress and milestone attainment
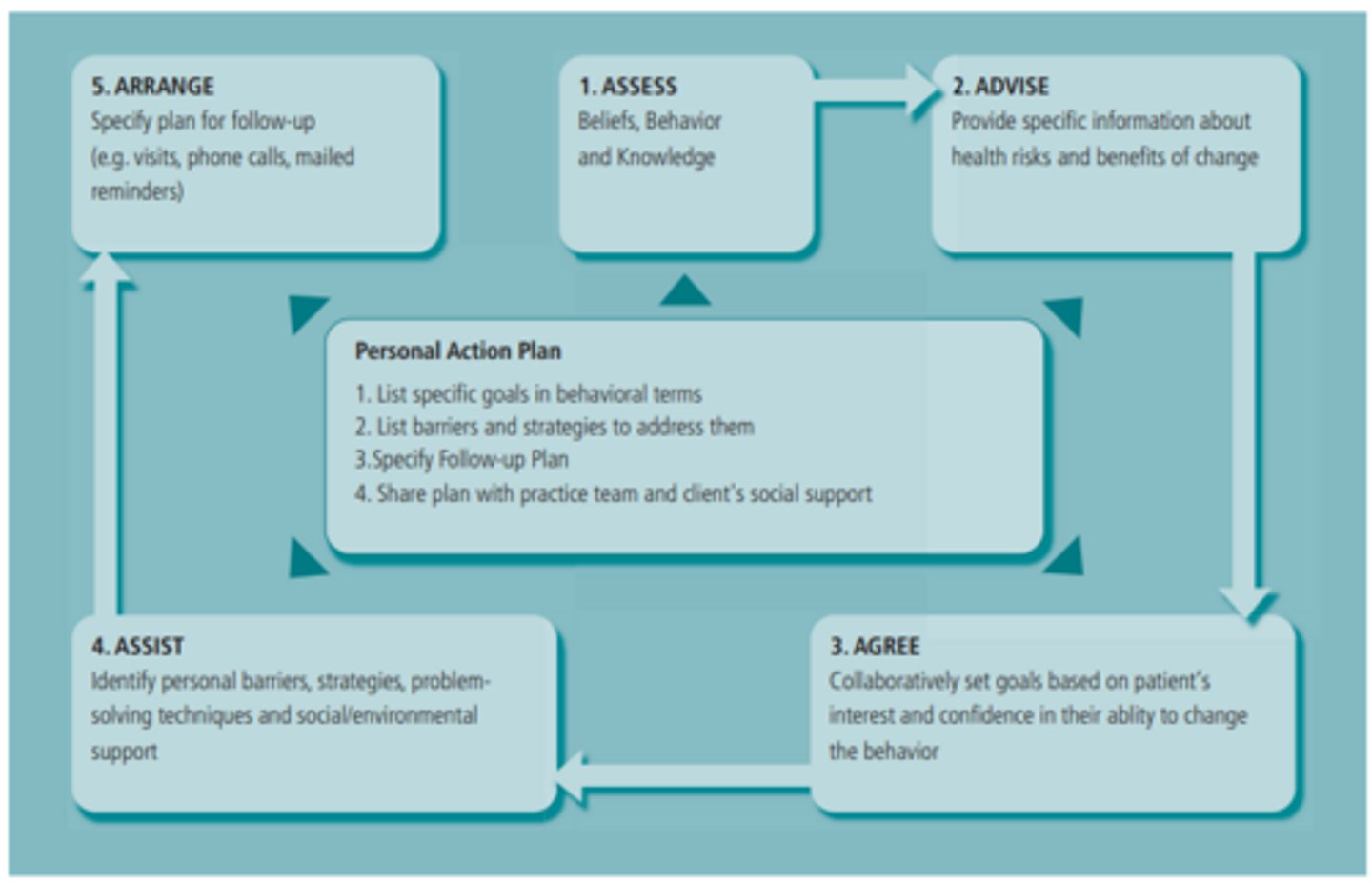
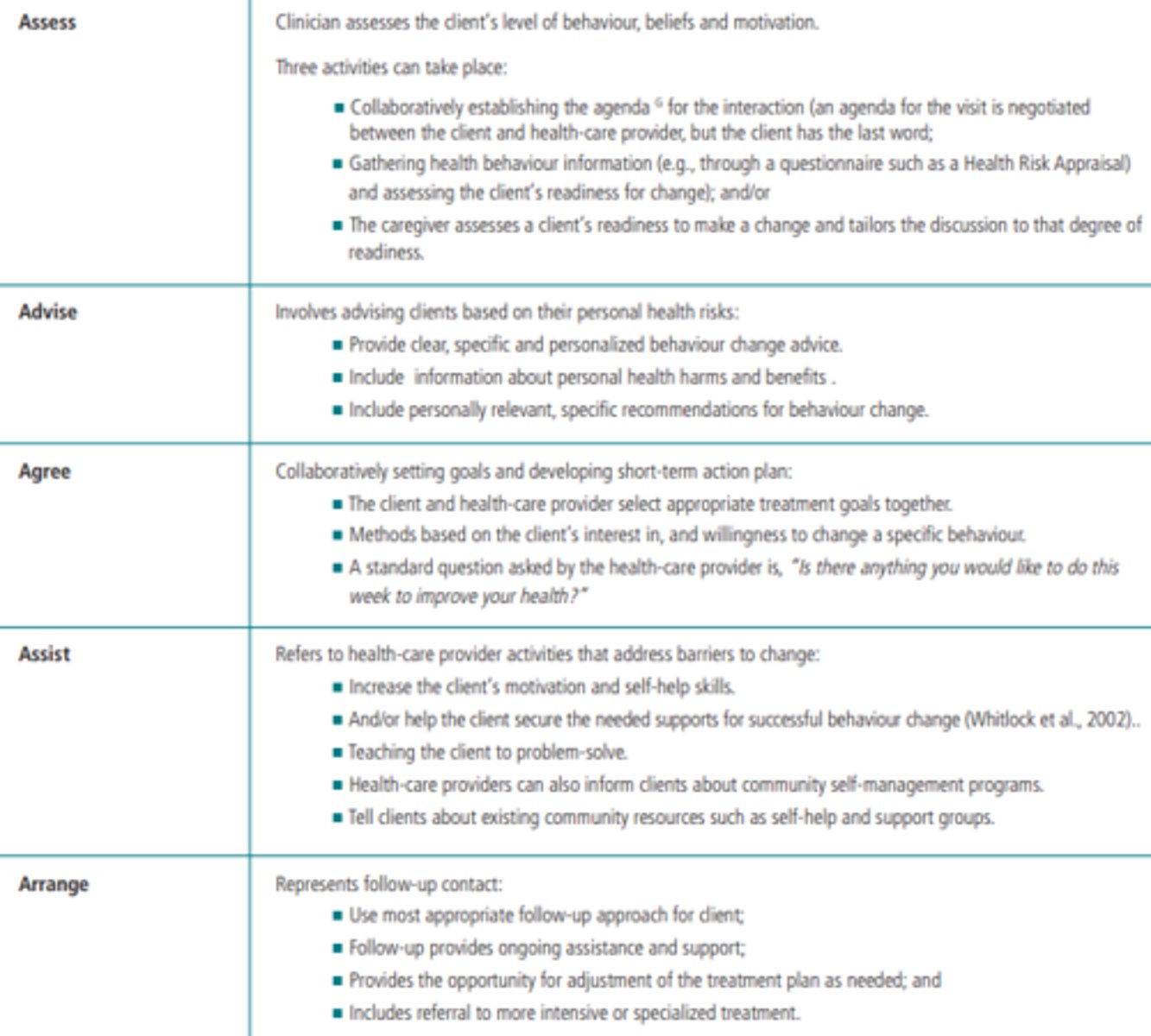
The 5 A's of Behavioural Change
- Nurses utilize the "5 A's" behavioural change approach of assess, advise, agree, assist and arrange, to incorporate multiple self-management strategies when supporting clients with a chronic illness to assist in improved outcomes
- Evidence reinforces an effect of multiple self-management strategies used at once
- The use of education, written action plans and regular reviews improved outcomes, although the impact of each intervention on individual outcomes is unknown
- Systematic reviews and clinical experience have shown that practices that use multifaceted interventions are more effective in promoting healthy behaviours than those that institute isolated measures
- The 5 A's multi-modal approach, which embodies the principles and strategies to successfully deliver behavioural risk factor interventions, provides a unifying conceptual framework for supporting self-management
- The goal of the 5 A's, in the context of self-management support, is to develop a personalized, collaborative action plan that includes specific behavioural goals and a specific plan for overcoming barriers and reaching those goals
- The 5 A's are elements that are interrelated and are designed to be used in combination to achieve the best results especially when working with clients in complex health and life situations
Health Triad
- The triad of goal setting, action planning, and problem-solving, while not rigorously evidenced based, appear to be important techniques to improve health-related behaviours and clinical outcomes
The Five A's
Care Transitions - RNAO
Summary of Recommendations
- It is good practice that health and social service providers collaborate with persons and their support network before, during and after a transition in care in order to ensure a safe and effective transition
- It is good practice that health and social service providers assess with persons and their support network their care needs and readiness for a transition
- It is good practice that members of the interprofessional team collaborate to develop a transition plan that supports the unique needs of persons and their support network
- Health and social service organizations collaborate to implement a formal interprofessional cross-sectoral approach to support persons encountering transitions in care
- In order to ensure medication safety, it is good practice for health providers to conduct the following in collaboration with the person encountering a transition and their support network: Obtain a best possible medication history; Perform medication reconciliation at all transition points
- It is good practice for health and social service providers to provide persons and their support network with information and support to manage their needs during and after transitions in care
- Navigation support be provided by health or social service providers for persons with complex care needs encountering a transition in care (includes regular follow-up by the provider to assess and respond to the person's current and evolving health and social care needs)
- Peer workers with lived experience offer support to persons with mental health needs who are encountering a transition in care
Best Possible Medication History (BPMH)
- A best possible medication history (BPMH) is a medication history obtained by a health provider using: (1) A systematic process of interviewing the person/and or their support network; and (2) a review of at least one other reliable source of information to obtain and verify all regular medication use
- The BPMH includes the drug name, dose, route and frequency of all medications (prescribed and non-prescribed) that a person is currently taking
Best Practice Guidelines (BPG)
- Best practice guidelines are systematically developed, evidence-based documents that include recommendations for nurses and the interprofessional team, educators, leaders and policy-makers, persons and their families on specific clinical and healthy work environment topics
- BPGs promote consistency and excellence in clinical care, health policies and health education, ultimately leading to optimal health outcomes for people and communities and the health system
Best Practice Spotlight Organization Ontario Health Team (BPSO OHT)
- Ontario Health Teams (OHT) are groups of providers and organizations that are accountable for delivering a full and coordinated continuum of care to a attributed population in Ontario, Canada
Caregiver
- A family member, friend or person of choice who gives unpaid care to someone who has care needs due to a disability, a physical, neurological or mental condition, a chronic illness, frailty or age
Continuity of Care
- Continuity of care is about the quality of the transition in care
- It is the extent to which care is well coordinated and connected as persons move between settings and through the health system
Culturally Safe Care
- People providing culturally safe care are attempting to provide respectful engagement that recognizes and aims to address power imbalances inherent across the health system
- Culturally safe care aims to create and sustain an environment that is free of racism and discrimination, where people feel safe when receiving health care
Discharge Summary
- A summary of what happened during a person's medical stay in a hospital, rehabilitation facilitation or other health-care setting
- It often includes the person's medical diagnosis, test results and pending test results, changes made to treatments or medications (including the reasons why), and follow-up needs
Education Statements
- Organizational approaches to the delivery of education in health service organizations and academic institutions to support evidence-based practice
- Education statements are based on an analysis of educational recommendations across several BPGs on diverse clinical topics and populations
Evidence-Based Practice
- The integration of research evidence with clinical expertise and patient values. It unifies research evidence with clinical expertise and encourages the inclusion of patient preferences
Evidence-to-Decision (EtD) Frameworks
- A table that helps expert panels make decisions when moving from evidence to recommendations
- The purpose of the Evidence-to-Decision framework (EtD) is to summarize the research evidence, outline important factors that can determine the recommendation, inform panel members about the benefits and harms of each intervention considered, and increase transparency about the decision-making process in the development of recommendations
Electronic Health Records
- An electronic health record is a secure, private, lifetime digital record of a person's health and care history that gives authorized health and social service providers real-time access to relevant medical information
Good Practice Statement
- Good practice statements are directed primarily to nurses and the interprofessional teams who provide care to persons and their support network across the continuum of care, including: Primary care; home and community care; acute care; and LTC
- Good practice statements are actionable statements that should be done in practice
- These statements are believed to be so beneficial that summarizing the evidence would be a poor use of the expert panel's time and resources
Health & Social Service Organizations
- Any settings in which a person, together with their support network, receives care or services during a transition in care
- Health service organizations are organizations delivering health-care services to defined communities or populations (ex. family health teams, home care organizations and hospitals)
- Social service organizations are organizations that assist persons with social issues, including housing, domestic violence and substance use
Health & Social Service Providers
- Refers to both regulated health and social service providers (ex. nurses, physicians, pharmacists, social workers, occupational therapists and paramedics) and unregulated health and social service providers (ex. personal support workers, peer workers with lived experience) who are part of the interprofessional team
- Regulated subjected to RHPA, unregulated are not subjected to RHPA
Health Literacy
- The ability of a person to obtain and translate knowledge and information in order to maintain and improve health in a way that is appropriate to the individual and system contexts
- Health literacy covers three broad elements: (1) Knowledge of health, health care and health systems; (2) processing and using information in various formats in relation to health and health care; and (3) ability to maintain health through self-management and working in partnership with health providers
Implementation Science
- The scientific study of methods to promote the systematic uptake of research findings and other evidence-based practices into routine practice, and, hence, to improve the quality and effectiveness of health services and care
Integrated Systems of Care
- Services organized across sectors and organizational boundaries so that persons receiving care receive coordinated and comprehensive services at the right time, from the right provider and in the right place
Interprofessional Cross-Sectoral Approach
- Refers to a collaborative approach where two or more health or social service providers from different disciplines in different sectors work together in a formal way to ensure persons and their support network experience a safe transition in care
Interprofessional Team
- A team composed of multiple health and social service providers (regulated and unregulated) who work collaboratively to deliver comprehensive and quality health services to persons within, between and across health and social care settings
- Key interprofessional team members supporting pediatric and adult persons and their support network during transitions in care include, but are not limited to: nurses, physicians, pharmacists, social workers, occupational therapists and paramedics
Medication Reconciliation
- A formal process in which health providers work together and with persons and their support network to ensure that accurate and comprehensive medication information is communicated consistently during a transition in care
- Medication reconciliation requires a systematic and comprehensive review of all the medications a person is taking (known as a "best possible medication history") to ensure that medications being added, changed or discontinued are carefully evaluated
Medication-Related Harm
- Harms experienced by a person as a result of exposure to a medication that may be preventable (ex. due to a medication error) or non-preventable (ex. an adverse drug reaction)
Navigation Support
- Refers to individualized and coordinated support provided by health or social service providers to help persons and their support network overcome challenges navigating the health and social care system during transitions in care
- This can include providing persons with the information and resources they need to achieve their goals of care, connecting persons with other health and social service providers, helping reduce barriers that prevent persons from accessing timely care, providing social and emotional support, and improving access to culturally safe care
Non-Randomized Study
- A quantitative study estimating the effectiveness of an intervention, where people are allocated to different interventions using methods that are not random
Outcomes
- A dependent variable or the clinical and/or functional status of a patient or population used to assess if an intervention is successful
- In GRADE, outcomes are prioritized based on if they: (a) are critical for decision making; (b) important but not critical for decision making; or (c) not important. Use of these outcomes helps make literature searches and systematic reviews more focused
Peer Worker with Lived Experience
- A person who has lived through similar experiences to their peers, such as a mental health challenge or illness, and who is trained to support others in their journey by providing practical and emotional support
Person
- An individual with whom a health or social service provider has established a therapeutic relationship for the purpose of partnering for health
Person-Centered
- An approach to care in which the person is viewed as whole
- The process of coming to know the whole person is nurtured through the formation of a therapeutic relationship between the person, those who are significant to them, and health and social service providers
- This approach to care involves advocacy, empowerment, mutual respect and an understanding of the person's right to be autonomous, to self-determine and to participate actively in decisions about their health
Person with Lived Experience
- Members of the community who have first-hand experience and knowledge of the topic of interest as a person, unpaid caregiver or advocate
- Persons with lived experience are a diverse group with an array of backgrounds and experiences
PICO Research Question
A framework to outline a focused question. It specifies four components:
- The patient or population that is being studied
- The intervention to be investigated
- The alternative or comparison intervention
- The outcome that is of interest
Preferred Reporting Items for Systemic Reviews & Meta-Analyses (PRISMA) Diagram
- A diagram that depicts the flow of information through the different phases of a systematic review
- It maps out the number of articles identified, included and excluded
Quadruple Aim
- An internationally-recognized framework for the delivery of health care that is centred around four overarching goals: (1) enhanced experiences for persons receiving care; (2) enhanced experiences for health and social service providers delivering care; (3) improved health outcomes for persons receiving care; and (4) reduced health care costs
Quantitative Research
- An approach to research that investigates phenomena with tools that produce statistical measurements/numerical data
Randomized Controlled Trial (RCT)
- An experiment in which the investigator assigns one or more interventions to participants who are randomly allocated to either the experimental group (receives intervention) and the comparison (conventional treatment) or control group (no intervention or placebo)
Recommendation Question
- A priority research area of practice, policy or education identified by expert panel members that requires evidence to answer
- The recommendation question may also aim to answer a topic area around which there is ambiguity or controversy
Responsive Behaviours
- Words, actions or gestures presented by persons with dementia or other neurological conditions in response to something frustrating, confusing or important in their social or physical environment
Self-Management
- Often associated with self-care and includes an array of activities that persons undertake to live well with one or more chronic conditions
SDoH
- Non-medical factors that influence health outcomes
- They are the conditions in which people are born, grow, work, live and age, and the wider set of forces and systems shaping the conditions of daily life
- These forces and systems include economic policies and systems, development agendas, social norms, social policies and political systems
Social Movement for Knowledge Uptake & Sustainability
- Individuals, groups and/or organizations who, as voluntary and intrinsically motivated change agents, mobilize to transform health outcomes
Stakeholder
- An individual, group or organization that has a vested interest in the decisions and actions of organizations, and which may attempt to influence decisions and actions
- Stakeholders include all of the individuals and groups that will be directly or indirectly affected by the change or solution to the problem
Strength-Based Approach
- Strength-based approaches focus on identifying and supporting the various strengths, motivations, and ways of thinking and behaving, as well as the protective factors, within the person or the environment, that support people in their journeys towards health and well-being
Support Network
- Individuals identified by a person as being significant in their life
- The network can include individuals who are related (biologically, emotionally or legally) and/or those with close bonds (friendships, commitments, shared household and child-rearing responsibilities, and romantic attachment)