PATHO2) W4b- Alterations in Digestion Function in Children
1/37
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
38 Terms
Cleft Lip/Cleft Palate
Syndromic
Occurs as part of chromosomal, mendelian, or teratogenic syndromes
Non-syndromic
Cleft palate occurring alone
Embryonic developmental anomalies that vary in severity
May be caused by genetic or environmental influences
Genetics, B vitamin/Folate deficiency, alcohol, tobacco use, statins, steroids
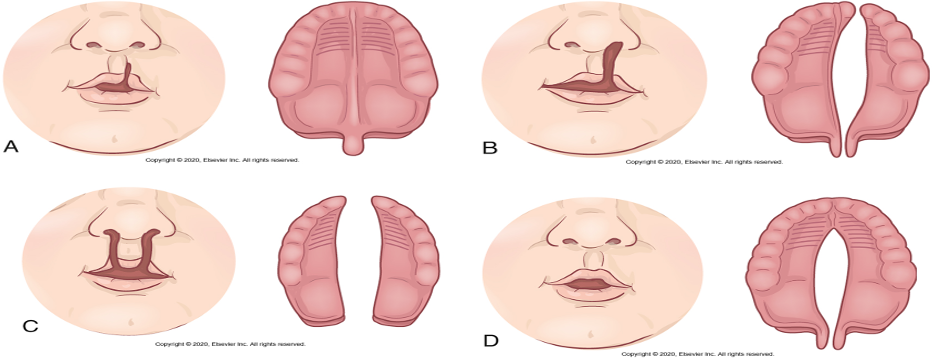
Cleft Lip Cause & Location
-incomplete fusion of the nasomedial process during fourth week of embryonic development
-Period of rapid development
- occurs under one nostril, bilateral , symmetric , asymmetric
Cleft Palate : Where and What
ass. W/ cleft lip but can occur without it
-May affect only the uvula and soft palate or may extend forward to the nostril and involve the hard palate and the maxillary alveolar ridge
CL & CP: clinical manif. & eval.
abnormal facial structure
Feeding difficulties- most significant
Cannot generate negative pressure for normal sucking
Evaluation and treatment
-Ultrasound and postnatal imaging
-Surgical correction
-Speech training
-Prosthodontist and orthodontist follow-up
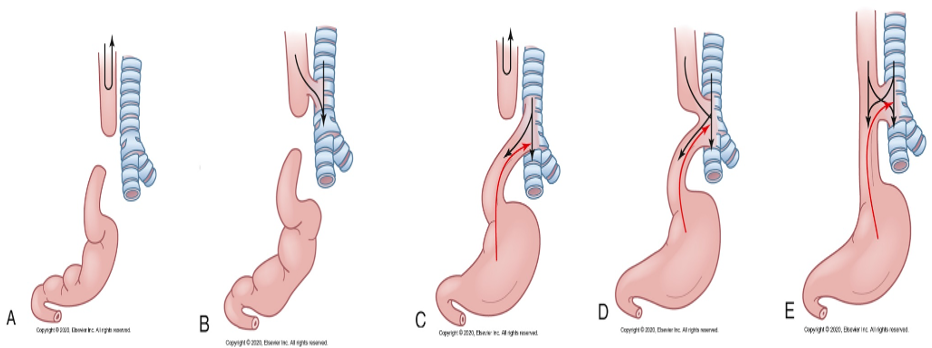
Esophageal Atresia
- blind pouch
-tracheoesophageal fistulas
-Envi. and gen. risk factors
-Antenatal diagnosis = polyhydramnios, inability to pass gastric tube after birth
Signs: drooling, inability to swallow, respiratory distress
Tx: Place tube with suction
HOB elevated
no oral feedings to prevent aspiration
Infantile Hypertrophic Pyloric Stenosis
-Acquired narrowing and distal obstruction of the pylorus
-unknown etiology
-2-3 weeks after birth forceful vomiting with out bilirubin content immediately after feeding
-Vomiting → weight loss, electrolyte imbalances, and dehydration
Infant irritable bc of hunger + esophageal discomfort
Evaluation and treatment
-pylorus is palpable in the RUQ (Olive Sized)
-Tx: pyloromyotomy
-Oversized RUQ Vomiting
Intestinal Malrotation
normally ileum & cecum rotate to RLQ and are fixed by mesentery
-Small intestine lacks normal posterior attachment
-Intestine twists upon itself (volvulus)
- develops during neonatal period (<1year)
Cllinical Manif & Evaluation of Intestinal Malrotation
- bile-stained vomiting
-fluid and electrolyte imbalances
-Fever, pain, scanty stools, diarrhea, and bloody stools
Evaluation and treatment:
x-ray: Laparoscopic, or open surgery to reduce volvulus
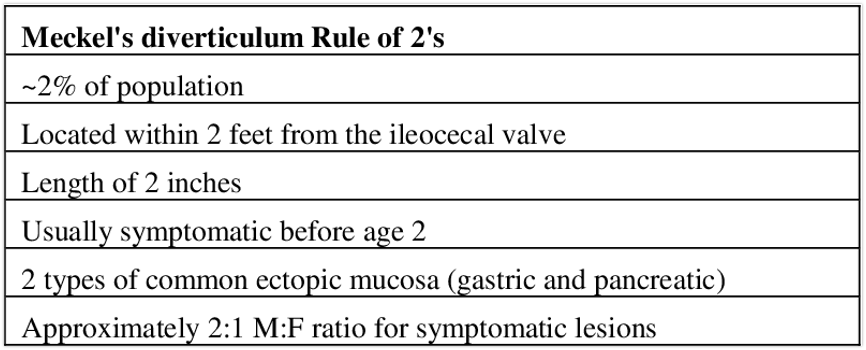
Meckel Diverticulum
Out pocketing of all layers of the small intestinal wall (usually in the ileum)
“Rule of 2s”
Most asymptomatic
Most common symptom is painless rectal bleeding
Intestinal obstruction, intussusception, and volvulus can occur
Rule of 2s for Meckel Diverticulum
Meconium Syndromes
Meconium is a substance that fills the intestine before birth
Usually passed within 12-48 hours after birth
Meconium Ileus
Meconium-caused intestinal obstruction in a newborn
Due to thick & sticky meconium
Can be Simple or Complex (medical emergency)
Many complex cases occur with Cystic Fibrosis
Meconium plug syndrome
Characterized by delayed passage of meconium (>24-48 hours) and intestinal dilatation
Distal intestinal obstruction syndrome
Characterized by complete or incomplete intestinal obstruction of viscid fecal accumulation in the terminal ileum and proximal colon
Pathophysiology of Meconium Syndromes
Terminal ileum plugged with thick, sticky meconium resulting from the formation of abnormal mucus
Peristalsis fails to propel this sticky material through the ileum, so it becomes impacted
Manifested by abdominal distention shortly after birth, followed by vomiting
Diagnosed by radiographic examination
Usually relieved by intestinal lavage and laxatives
Hirschsprung Disease
(congenital aganglionic megacolon)
Functional obstruction of the colon
Characterized by absence of parasympathetic nervous system intrinsic ganglion cells
Abnormally innervated colon impairs fecal movements
Causes colon obstruction and distention
CLinical Man and Eval Hirschspring Disease
Clinical manifestations:
-Mild to severe constipation
-Diarrhea
-Enterocolitis, sepsis, death
Surgery: is the definitive treatment
Gastroesophageal reflux vs. GERD
Gastroesophageal reflux
Passage of gastric contents into esophagus separate from swallowing
Normal and non pathologic in healthy infants
GERD
When reflux causes troublesome symptoms or complications
Causes
Transient lower esophageal sphincter relaxations
Inadequate adaptation of sphincter tone to changes in abdominal pressure
GERD CM & EVAL
Clinical manifestations:
Excessive vomiting, food refusal, unexplained crying, choking, gagging
Complications include esophagitis, hemorrhage, stricture, Barrett esophagus
Evaluation and treatment:
Often diagnosed by clinical manifestations
Feeding volume/frequency adjustment, Thickened feedings Medication, surgery, Dietary modifications (caffeine, chocolate, spicy foods)
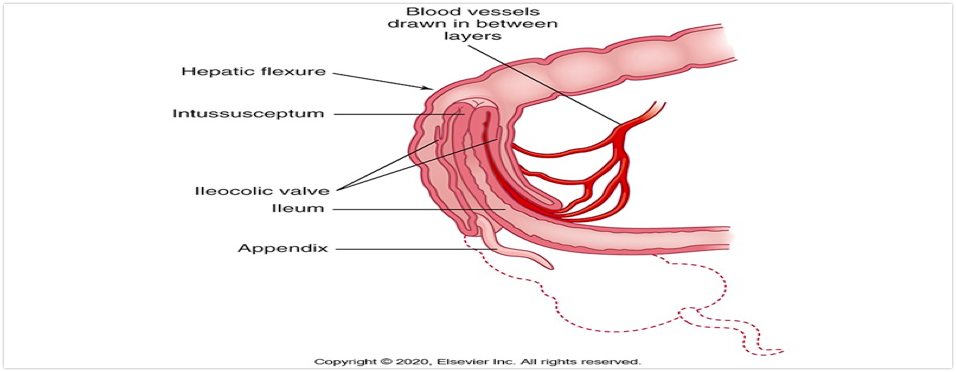
Intussusception
-Telescoping of a proximal segment of intestine into a distal segment, causing an obstruction
-The most common scenario is the ileum telescopes into the cecum and part of the ascending colon by collapsing through the ileocecal valve
-Causes bleeding, necrosis, and bowel perforation if not treated
Intussusception CM & E
Clinical manifestations:
-Colicky Abdominal pain, irritability, vomiting, “currant jelly”stools, knees drawn into chest
Evaluation and treatment:
-Clinical manifestations and ultrasonography
-Reduction with enema
-Surgical reduction
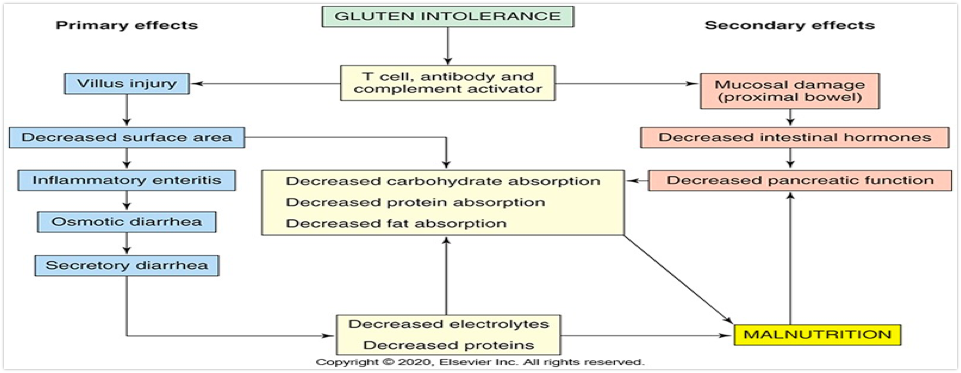
Celiac Disease
-Autoimmune disease that damages small intestinal villous epithelium when gluten is ingested
-Gluten is the protein component in cereal grains (wheat, rye, barley, malt)
-The disease appears to be caused by dietary, genetic, and immunologic factors
Celiac Disease Onset and Severity/ Celiac Crisis
Onset of manifestations depends on the age of the infant when gluten-containing substances are added to the diet
Severity of symptoms varies tremendously
Celiac crisis
Severe diarrhea, dehydration, & hypoproteinemia d/t malabsorption
Diagnosis confirmed with serologic autoantibody measurement
Gluten-free diet for life
Malnutrition and Causes
•Imbalance between nutrient requirements and intake: •Impaired absorption
•Altered nutrient utilization
•Increased nutrient losses
•Increased nutrient requirements
Causes:
•Moderate to severe illnesses
•Lack of access to nutrients
•Behavioral factors
Protein energy malnutrition (PEM)

Types of malnutrition associated with long-term starvation
Kwashiorkor: deficiency in dietary protein
Marasmus: all forms of inadequate nutrient intake
Manifestations
Muscle wasting, diarrhea, dermatosis, low hemoglobin level, infection, generalized edema
Loss of subcutaneous fat
Delays in physical, behavioral, and cognitive development
Faltering Growth
Previously called failure to thrive (FTT)
Physical sign showing that a child has a slower rate of weight gain than expected
Deceleration in weight gain
Low weight/height ratio or BMI ratio
Low weight/height/head circumference ratio
Multifactorial
Biologic
Psychosocial
Environmental
Necrotizing Enterocolitis
Ischemic, inflammatory condition that causes bowel necrosis and perforation
Not a specific diagnosis, but a constellation of symptoms
Most common severe neonatal gastrointestinal emergency
Primarily affects smallest and most premature infants
Etiology unclear
Contributing Factors to Necrotizing Enterocolitis
Contributing factors
Infections
Abnormal bacterial colonization
Intestinal ischemia
Immature immunity
Exaggerated inflammatory responses
Immature intestinal motility
Altered microcirculatory blood flow and barrier function
Perinatal stress
Effects of medications and feeding practices
Genetic predisposition
Necrotizing Enterocolitis: CM & E
Clinical manifestations
Feeding intolerance. abdominal distention, & bloody stools.
Septicemia with elevated WBCs& low platelets
Evaluation and treatment
Clinical manifestations, laboratory results, and plain films of abdomen
Cessation of feeding, maintain fluids/electrolytes, gastric suction to decompress intestines, antibiotics to manage sepsis, and surgery
Primary Lactose Intolerance
The inability to digest lactose due to inadequate production of lactase (the enzyme that catabolizes lactose)
Malabsorbed lactose causes
Osmotic diarrhea
Abdominal pain
Bloating
Flatulence
Neonatal Jaundice
Yellow pigmentation of the skin caused by an increased level of bilirubin in the bloodstream
Usually becomes clinically apparent when the serum bilirubin concentration is greater than 2 mg/dL
Physiologic Jaundice
-Common in healthy newborns
-improper bilirubin uptake and conjugation
-poor intake or dehydration
-Ass. With hemolytic disease, metabolic and endocrine disorders, liver abnormalities, infections
-Tx: phototherapy.

Pathologic Jaundice
Bilirubin concentration >20 mg/dl in newborn period
Associated with severe illness
Risk factors include:
Fetal-maternal blood type incompatibility, premature birth, exclusive breast feeding, maternal age >25 years, male sex, delayed meconium passage, glucose-6-phosphate dehydrogenase deficiency, and excessive birth trauma
Treated with exchange transfusion and treatment of underlying cause
Biliary Atresia
Congenital malformation characterized by the absence or obstruction of extrahepatic bile ducts leading to neonatal cholestasis
Can lead to Biliary cirrhosis, Portal Hypertension, & Liver failure
Jaundice is the primary clinical manifestation
Fat absorption may be impaired
Liver transplant long-term therapy
Metabolic Disorders
Wilsons, Galactosemia, Fructosemia
Early diagnosis is critical to:
Prevent damage to organs
Provide further genetic counseling
Minimize complications
Wilson’s Disease
•Autosomal recessive defect of copper metabolism
•Causes toxic levels of copper to accumulate in the liver, brain, kidneys, and corneas
Galactosemia
•Autosomal recessive trait of deficient galactose-1-phosphate uridyl transferase
•Causes toxic levels of galactose in body tissues, liver, and brain
•Autosomal recessive trait of deficient fructose-1-phosphate aldolase
•Causes toxic levels of fructose to accumulate in body tissues
•Autosomal recessive trait of deficient fructose-1-phosphate aldolase
•Causes toxic levels of fructose to accumulate in body tissues