NPB 101 MT3 (Endocrine)
1/168
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
169 Terms
Organs that function specifically for the endocrine system
pituitary
thyroid
parathyroid
adrenal gland
How do endocrine cells communicate?
Endocrine signaling
Hormone
an extracellular signaling molecule that is released into the blood and acts at its receptors in distal tissues in order to elicit a physiological response
Diffusion is “pathetic” but efficient, how?
Strong propulsion causes fast blood flow in the body (makes up for the slow speed of diffusion)
Nervous system
Anatomic Arrangement: A “wired” system: a structural arrangement exists between neurons and their target cells, with structural continuity in the system
Type of chemical messenger: neurotransmitters released into the synaptic cleft
Distance of action of the chemical messenger: short distance (diffuses across the synaptic cleft)
Specificity of action on the target cell: dependent on the close anatomic relationship between neurons and their target cells
Speed of response: rapid (milliseconds)
Duration of action: brief (milliseconds)
Major functions: coordinates rapid, precise responses
Endocrine system
Anatomic Arrangement: A “wireless” system: glands are widely dispersed and not structurally related to one another or to their target cells
Type of chemical messenger: hormones released into the blood
Distance of action of the chemical messenger: long distance (carried by the blood)
Specificity of action on the target cell: dependent on the specificity of target cell binding and responsiveness to a particular hormone
Speed of response: slow (minutes to hours)
Duration of action: long (minutes to days or longer)
Major functions: controls activities that require long duration rather than speed
Hydrophilic hormones
High water solubility: Low lipid solubility (cannot pass through a lipid membrane well
Water-loving
Stored in secretory vesicles post-synthesis until recception of stimulus for secretion
Lipophilic hormones
High lipid solubility: Low water solubility
Lipid-loving
Hydrophilic hormone types
AA derivatives (amines)
Peptide hormones
AA derivative hormones
Amines
Hydrophilic
Include:
dopamine
norepinephrine
epinephrine
melatonin
Peptide hormones
Majority of hormones fit this subcategory
Short to medium length chains of AAs (3 AA to 200AA)
Hydrophilic
Include:
All pancreatic hormones (e.g., insulin, glucagon)
All digestive tract hormones (e.g., secretin, gastrin, CCK, GLP-1, GIP)
All Hypothalamic releasing or inhibiting hormones (except dopamine, see above)
All anterior and posterior pituitary hormones
Various others: angiotensin II, insulin-like growth factor I, erythropoeitin, atrial natriuetic peptide, calcitonin
Amine synthesis benefit
Different hormones derived from each other allows conservation of energy
Dopamine
The only hypothalamic releasing/inhibiting hormone that is not considered to be a peptide hormone
Smaller than an AA, making it the smallest second set of biologically active molecules (compounds) in the body (after gasses)
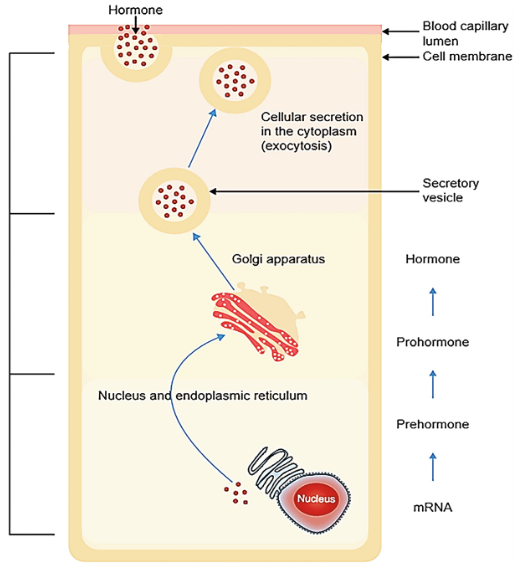
Peptide hormone synthesis
Produced from mRNA, which creates inactive hormones
Activated upon enzyme cutting activity
mRNA → pre-hormone → pro-pre-hormone → hormone
Lipophilic hormone types
Thyroid hormones
Steroid hormones
Thyroid hormones
Derived from 2 tyrosines + iodide (added)
Lipophilic
Note: both lipid and water soluble yet still works like a typical “highly lipid soluble” hormone
Types:
Thyroxine (T4)
Triiodothyronine (T3)
Activate thyroid hormone receptor
Complicated synthesis in thyroid gland
Steroid hormones
Derived from cholesterol
Lipophilic
Note: highly lipid soluble but have a little bit of water solubility
Types:
Estrogens
Androgens
Progestins
Glucocorticoids
Mineralocorticoids
Vitamin D
Receptors for these hormones are variable in amount with respect to time
Steroidogenesis
The particular steroid hormone produced by a cell depends on the expression and activity of a specific set of “steroidogenic enzymes”
The chemical (soluble) properties of a hormone impact its
Storage: If it can be stored in cells before release into the bloodstream
Transport: How the hormone is carried throughout the bloodstream
Metabolism and Excretion
Mode of action at target cells
Hydrophilic hormone storage
Kept in secretory vesicles after synthesis, thus secretion gets regulated separately from synthesis
Lipophilic hormone storage
None: hormones diffuse out of cells as soon as they are synthesized
Hydrophilic hormone transportation
Completely soluble in plasma; travel where they need to go easily and freely
Lipophilic hormone transportation
Insoluble in plasma, so hormones bind weakly onto carrier proteins circulating in the blood
Weak binding permits them to “jump on and off” [of carrier proteins] at will
Hydrophilic hormone metabolism
Chemical modification to become less active: hormones cleaved by circulating general proteases (enzymes that cut proteins or peptides at many different peptide bonds)
Chemical modification to become more active: hormones cleaved by specific proteolytic enzymes (cut at a specific peptide bond)
these activating enzymes all come from different places in the body to increase efficiency of production
(specifically in reference to peptide hormones)
Lipophilic hormone metabolism
Chemical modification to become less active: hormones modified by liver enzymes to be more water-soluble and therefore can’t enter cells, and are also more easily excreted in urine
Chemical modification to become more active: enzymes in target cells chemically modify one version of a hormone to produce a more active version of the hormone
Hormone receptor properties
Expressed in target tissues and upon hormone binding initiate biochemical chain of events that alters cell function
Hydrophilic hormone mode of action (@ target cells)
Act via receptors in target cell membrane (i.e., membrane receptors) and activate receptor-enzyme complexes, or recruit second-messenger systems to produce their physiological response
Lipophilic hormone mode of action (@ target cells)
Act via intracellular receptors that act in the cell nucleus (i.e. nuclear receptors) to induce gene transcription, producing their long-term physiological response
These hormones can simply pass through the lipid membrane without external help, so getting to the location of action is the easy/fast part
Their function of inducing gene transcription is the natural goal; from there, the time-consuming part (to cause long-term effects)
Time-consuming → high reward
Which signaling strategy might affect cells the fastest?
Hydrophilic
Which signaling strategy might have effects that last the longest?
Lipophilic
Hydrophilic hormones’ Second Messenger Pathway (specific example)
Binding of extra-cellular messenger (hormone) to receptor activates a G protein
G protein α-subunit shuttles to adenylyl cyclase to activate it
Adenyl cyclase converts ATP to cAMP
cAMP activates protein kinase A
Protein kinase A phosphorylates inactive designated protein, activating it. This is done through the targeting of:
Ion channels (& other transporters)
Enzymes
Transcription factors (alter gene transcription, so this response takes longer)
Active designated protein brings about desired response
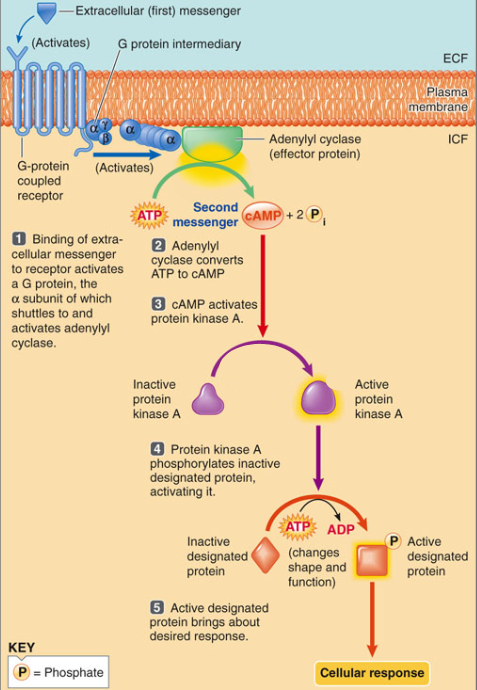
G-receptor role in Hydrophilic second-messenger cascade
Targeted by over 40% of all prescription drugs because they're so frequent in plasma membranes
Hydrophilic hormones’ Second Messenger Pathway (general description)
one hormone molecule binds to the exterior surface of the cells → activation of hundreds or thousands of enzyme molecules inside the cell → catalyze many rounds of reaction → produced amplification of signal
Phosphorylation in Hydrophilic second-messenger cascade
Can either have no effect, increase, or decrease activity — depends on the kinase and protein
A single kinase can act upon thousands of proteins
It's stopped by an esterase eventually
Lipophilic hormones’ Regulation of Gene Transcription Pathway (specific example using a nuclear receptor)
Free lipophilic hormone diffuses through plasma membrane
Hormone binds with its respective specific intracellular receptor
Hormone receptor complex binds with DNA’s hormone response element
Binding activates gene
Activated gene transcribes mRNA
New mRNA leaves nucleus
Ribosomes read "mRNA to synthesize new proteins
New protein is released from ribosome and processed into its final folded form
New protein brings about desired response
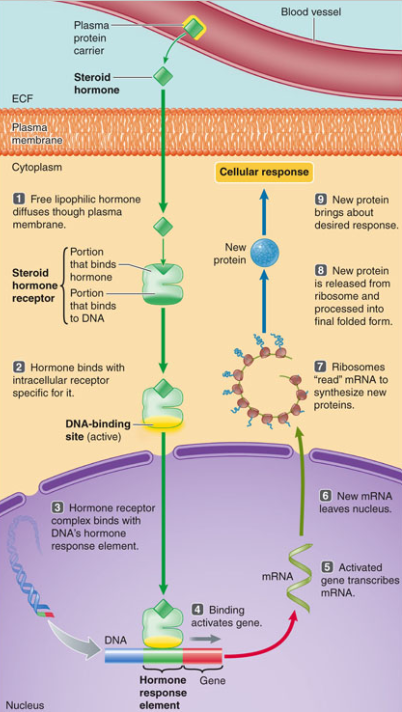
Nuclear receptors in Lipophilic gene-transcription pathway
Intracellular receptors that regulate specific gene transcription
How is endocrine function regulated?
Negative feedback control of hormone secretion
Neuroendocrine reflexes can promote hormone secretion
Circadian rhythms can control hormone secretion
Changes in hormone receptor activity, often by expression or availability
In relation to other hormones: permissiveness, synergy, or antagonism
Endocrine function regulation via Negative feedback control
Can be driven by either:
Direct sensing of changes in the controlled variable (ie: control of blood glucose, Karen can see that the TP is back on the shelf and will stop shouting at the manager)
The endocrine axis itself, where one of the hormones in the control system provides feedback. [ie: hypothalamic-pituitary-(thyroid/adrenal, gonad)- axes, Karen could hear the manager talking to the store clerk]
Endocrine function regulation via Neuroendocrine reflexes
Result in a sudden increase in hormone secretion in response to a specific stimulus
(ie: secretion of epinephrine from the adrenal medulla in response to increased sympathetic nervous system output, or vasopressin secretion from the posterior pituitary when blood pressure drops)
Endocrine function regulation via Circadian rhythms
Rate of secretion of many hormones fluctuates up and down as a function of time.
Most commonly, this is characterized by repetitive oscillations occurring every 24h, responsive to light (and dark).
This is an example of “feed-forward” control.
Advantage: preparation for future events
Ie: one job of cortisol is to increase blood glucose in the morning so we have energy to start the day — making it a glucocorticoid
Endocrine function regulation via Receptor activity (number, availability, or responsiveness)
A target cell’s response to a hormone is correlated to the number of that cell’s receptors that are occupied by the hormone, therefore endocrine function can be regulated by both the concentration of the hormone and the number of available receptors
Endocrine function regulation via other hormones
Permissiveness = one hormone must be present in sufficient amounts to ‘permit’ another hormone to have its full effects (think of E for progesterone)
Synergy = the combined actions of several hormones are greater than the sum of their separate effects.
Antagonism = one hormone causes the loss of another hormone’s receptors. Opposite of permissiveness
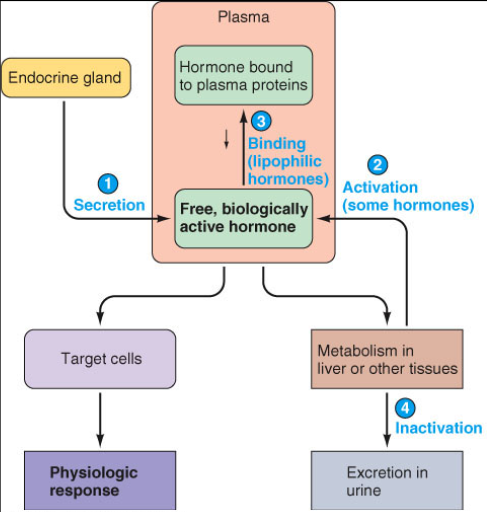
Effective concentration of a hormone in the bloodstream is influenced by:
Primarily, rate of secretion, but also:
Regulated metabolism by conversion or activation– sometimes the secreted hormone needs to be “activated” before it can bind to its receptor.
Transport– lipophilic hormones may circulate mostly in a carrier protein bound form, but only the unbound “free” form can enter cells and activate a receptor.
Metabolic inactivation and excretion (feces and urine) (lowers the amount)
Hyposecretion
Too few hormone secreted by endocrine gland
Hypersecretion
Too much hormone secreted by the endocrine gland
Two major ways of hormone secretion regulation
1) Physiological changes (including reproduction) or developmental cues are sensed within or relayed to the brain (specifically, the hypothalamus), where the information is integrated (which then allows either -/+ feedback)
This results in changes in pituitary hormone secretion that act directly on target cells and/or regulate the secretion of other hormones.
Negative feedback often works here to maintain hormone levels in blood within predetermined high and low set points, but as we will see, positive feedback can occur as well, but that’s mostly involved in reproduction (vs the more common negative feedback in regulating homeostasis)
2) The hormone-secreting cell directly senses a change in a controlled variable and responds by increasing or decreasing the secretion of hormones that correct that change back to a set point, in a classical negative feedback fashion
This is how blood glucose levels are controlled
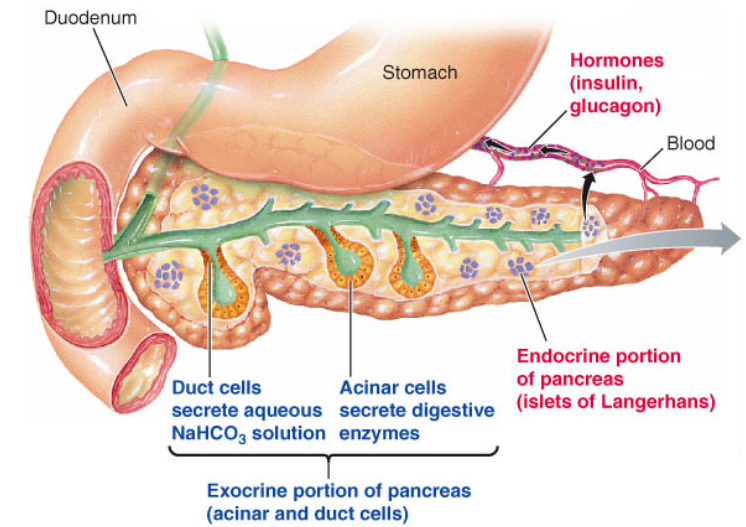
Pancreas Hormones
Don’t receive as much blood supply because they don’t require a lot of energy (not like they need it to incite contractions or anything)
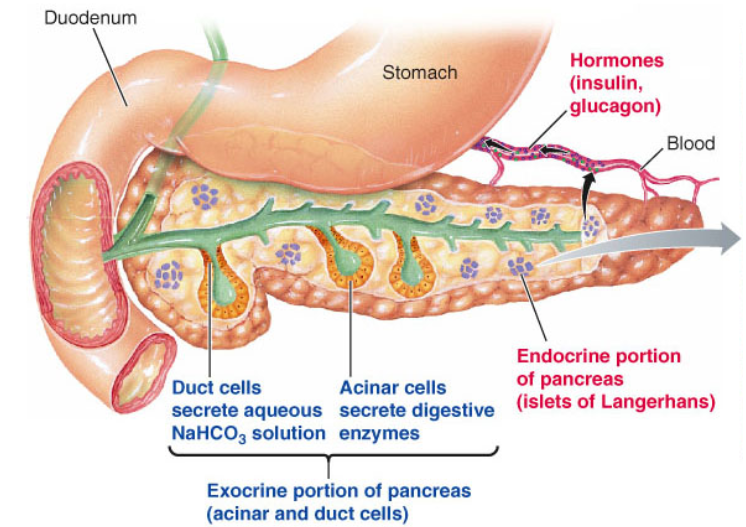
Pancreas Islets of Langerhans
Endocrine control of nutrient (especially glucose) levels after digestion
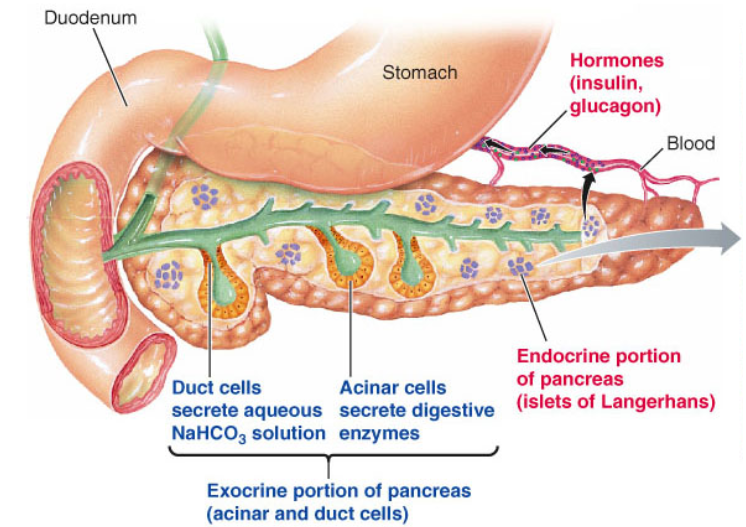
Pancreas Duct Cells
Neutralize the enzymes from the stomach, allowing the pH to increase so they can function better
Pancreas Acinar Cells
Secrete enzymes that break things down
Function best around 7.2 pH → located next to duct cells
Endocrine portion of pancreas
Islets of Langerhans
Exocrine portion of pancreas
Acinar & Duct cells
Homeostatic regulation of blood glucose involves…
The shuttling of energy stores between ingested nutrients and their stored forms to maintain a relatively constant supply of glucose for all the cells of the body — especially for the brain
Anabolic reactions
Build storages of fuel from food
Catabolic reactions
Break down storages of fuel from food
The food we eat is derived from several macronutrient forms:
PRO — protein
CHO — carbohydrates
FAT
AAs are derived from what macronutrient?
Proteins
Simple sugars, including glucose, are derived from what macronutrient?
Carbohydrates
Fatty acids and monoglycerides are derived from what macronutrient?
Fats
Macronutrient derivations
AAs, simple sugars, fatty acids, and monoglycerides can be used immediately as fuel when created or can be stored for future use
Sugars get stored where in the body?
As glycogen in liver and muscle
Fatty acids are stored where in the body?
As triglycerides in adipose tissue
AAs are stored where in the body?
They’re actually used to build structural and functional proteins for the body instead
What fuel is the brain able to use?
Glucose, with the exception of ketoacids produced by the liver during starvation
Why does the brain use ketoacids for fuel during starvation?
It is unable to store glucose reserves for later use
Most abundant metabolic fuel in the body
Adipose tissue (storage site for fat)
If the body wants to access protein for fuel, what has to be done?
Structural proteins (such as those within our skeletal muscle being used for skeletal muscle things) have to be broken down and removed from their system.
This is so inconvenient that it’s only used for energy as a last resort; death often results long before the capacity is fully used (structural and functional impairment results)
Anabolism
The buildup or synthesis of larger organic molecules from small organic molecular subunits
Dominates the absorptive/fed state
Glucose is plentiful and serves as the major energy source
Catabolism
Breakdown or degradation of large energy-rich molecules within cells
Dominates the post-absorptive/fasting state
“Genesis” root
= building up
“Genolysis” root
= breaking down
Fuel metabolism Anabolic reactions
Glycogenesis: glucose → glycogen → ↓blood glucose
Protein synthesis: AAs → protein → ↓blood AAs
Fat synthesis (lipogenesis or triglyceride synthesis): fatty acids & glycerol → triglycerides → ↓blood fatty acids
Fuel metabolism Catabolic reactions
Glycogenolysis: glycogen → glucose → ↑blood glucose
Gluconeogenesis: glycerol & AAs → glucose → ↑blood glucose
technically just an “interconversion” reaction that is most active in the post-absorptive state
Protein degradation: protein → AAs → ↑blood AAs
Fat breakdown (lipolysis or triglyceride degradation): triglycerides → fatty acids & glycerol → ↑blood fatty acids
Hormone(s) that increase blood glucose
Glucagon – Released by alpha cells in the pancreas when blood glucose is low. It stimulates the liver to break down glycogen into glucose (glycogenolysis) and produce new glucose from non-carbohydrate sources (gluconeogenesis), raising blood sugar
Epinephrine (adrenaline) – Released by the adrenal medulla during stress, exercise, or low blood sugar. It promotes glycogen breakdown in the liver and muscle, and increases glucose production in the liver, thus raising blood glucose
Cortisol – Released by the adrenal cortex in response to stress or low glucose. It increases gluconeogenesis in the liver and reduces glucose uptake by peripheral tissues, elevating blood sugar
Growth hormone (GH) – Secreted by the anterior pituitary. It promotes lipolysis (fat breakdown) and gluconeogenesis, and reduces insulin sensitivity, leading to higher blood glucose
Hormone(s) that decrease blood glucose
Insulin – Released by beta cells in the pancreas when blood glucose is high (e.g., after a meal). It stimulates cells (especially liver, muscle, and fat) to take up glucose from the blood, store it as glycogen, and reduce glucose production by the liver, thereby lowering blood sugar
Insulin
Major absorptive state hormone: It travels through the blood to facilitate uptake and storage of glucose (and storage of other fuels) in target organs
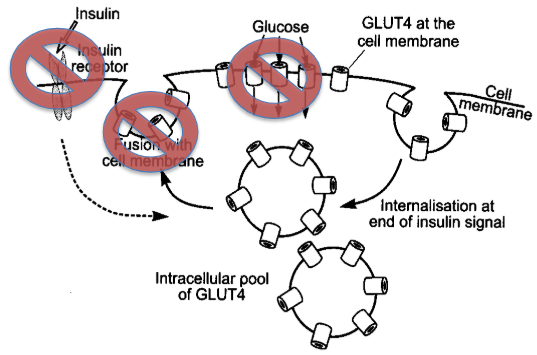
Primary goal: enhance glucose uptake via the transporter protein GLUT4, in many tissues of the body (especially fat cells and resting skeletal muscle)
Released by beta cells in the pancreas’ Islets of Langerhans when blood glucose is high (e.g., after a meal). It stimulates cells (especially liver, muscle, and fat) to take up glucose from the blood, store it as glycogen, and reduce glucose production by the liver, thereby lowering blood sugar
GLP-1
Originally developed to increase insulin secretion in TII Diabetes
+ Parasympathetic stimulation onto Islet β cells for insulin production
Insulin mediated GLUT transportation
To the liver: insulin-independent transport via GLUT2, but insulin is required (dependent!) for glycogenesis
To the skeletal muscles: GLUT4 transport, stored as glycogen
To fat cells: GLUT4 transport, stored as triglycerides (via new triglyceride synthesis)
To the brain: insulin-independent transport via GLUT2, no storage
When is insulin required for glucose uptake in skeletal muscles?
Resting skeletal muscles need GLUT4 to be inserted into their membrane
When is insulin not required for glucose uptake in skeletal muscles?
Contracting skeletal muscles already have GLUT4 inserted into their membrane whilst contracting
Insulin effects on Carbohydrate Metabolism
Enhances glucose uptake via GLUT4
Increases liver and skeletal muscle glycogenesis
Inhibits liver and muscle glycogenolysis
Inhibits liver gluconeogenesis
↑ α ↓[Blood Glucose]
Insulin effects on Fat Metabolism
Enhances glucose uptake in adipocytes for triglyceride synthesis
Increases adipocyte triglyceride synthesis
Inhibits adipocyte lipolysis
↑ α ↓[Blood Fatty Acids]
Insulin effects on Protein Metabolism
Enhances AA uptake into muscle and liver
Increases protein synthesis
Inhibits proteolysis
↑ α ↓[Blood AAs]
Which statement about blood glucose levels is TRUE?
It must remain within a normal range because the brain needs a constant supply of glucose.
Which statement is TRUE for insulin but FALSE for glucagon?
It stimulates glucose uptake by resting skeletal muscle
Glucagon
Major post-absorptive state hormone
Facilitates the maintenance of fasting blood glucose
Produced by the Islets of Langerhans’ α-cells
Glucagon in Adipose tissue
Increases lipolysis and inhibits triglyceride synthesis
Glucagon in the Liver
Decreases glycogen synthesis
Increases glycogenolysis
Increases gluconeogenesis (uses amino acids, glycerol)
Mildly increases ketogenesis (byproduct of FA metabolism) (in prep for worst-case scenario where the brain needs ketones for energy)
How to remember the order of Anabolism/Catabolism in the body?
A comes before C
Glucagon in Skeletal muscle
No direct effects of glucagon on skeletal muscle, but: the absence of insulin (or minimal levels) leads to reduced glucose uptake and increased protein degradation
Glucagon in the Brain
No direct effects of glucagon on the brain but: its action in peripheral tissues helps maintain blood glucose to keep the brain happy.
Glucagon effects on Carbohydrate Metabolism
Inhibits liver glycogenesis
Increases liver glycogenolysis
Increases liver glucogenesis
↑ α ↑[Blood Glucose]
Glucagon effects on Fat Metabolism
Decreases triglyceride synthesis
Increases lipolysis
Mildly increases liver ketogenesis
↑ α ↑[Blood Fatty Acids]
Glucagon effects on Protein Metabolism
Minimal/No effect
Stimulation of Glucagon via ↓[Fatty acids]
Recognition that body is “running low on fuel from fat”
Breaks down more glycogen.
Makes more glucose from amino acids and glycerol.
Increases fat breakdown to restore fatty acids in the blood
Stimulation of Glucagon via ↑[AAs]
Prevention of the typical insulin-only response post-meal
Gluconeogenesis performed instead/additionally
Glucose then released into the blood
Diabetes Mellitus
It is a group of metabolic disorders sharing the common underlying feature of hyperglycemia.
In diabetes, hyperglycemia results from
Defects in insulin secretion
Defects in insulin action
Defects in both insulin action and secretion
Chronic hyperglycemia can result in multiple organ damage
11-12% of the population in the US suffers from diabetes (2021) (it is the most common of all endocrine system related diseases).
3X that number suffers from “pre-diabetes” (some evidence for dysregulated glucose homeostasis)
Hyperglycemia in diabetics results from
Defects in insulin secretion
Defects in insulin action
Defects in both insulin action and secretion
RBC Glycosylation
When glucose concentration in the blood becomes excessive, glucose molecules stick to the hemoglobin of the blood
The attachment of glucose to hemoglobin is permanent; the two remain stuck until the end of the 3-4 blood cell lifespan
Thus, remains unaffected by whether or not someone is fasting when blood glucose is tested
What makes the A1C such an efficient test for diabetes?
It’s not affected by fasting vs. non‑fasting — results reflect long term patterns instead of short-term ones.
The score specifically represents the average blood glucose over the past 3–4 months [which is also lifespan of RBCs (with glycosylated hemoglobin)]